
Abstract
Keywords
Introduction
There are an estimated 2.4 million HIV-positive individuals in India, and the majority of them seek care and support from government institutions. There are more than 300 antiretroviral therapy (ART) centers in India providing care, support, and treatment services to people living with HIV/AIDS (PLWHA) apart from other health facilities like Community Care Centers, Link ART Centers, and Centers of Excellence. Technology-based communication and information sharing have been used frequently in the Western world to provide health-based advice and education. Warmlines, hotlines, perinatal lines, Post-Exposure Prophylaxis (PEP) lines, and so on, were practiced consistently and reliably in many parts of the world to provide technical and programmatic support to the new, trained but less experienced health care providers in areas of patient care. 1,2
In India, the medical officers with a basic degree in medicine were selected and were provided a short-term (12 days) induction training based on a standard national curriculum and they were posted at government ART centers (around 300 ART centers) to provide clinical care, support, and treatment. As of today, there were over 400 000 PLWHA getting ART services from ART centers in India. 3 The International Training and Education Center for Health, India (I-TECH India), established a warmline pilot process in the year 2008 to provide remote, mobile-based technical support to the ART medical officers.
Methods
The I-TECH India established a mobile telephone consultation service, called warmline, and it was supplemented with e-mail communications whenever necessary. Two senior clinicians from I-TECH India were provided training at National Clinicians Consultation Center, University of California San Francisco (UCSF) General Hospital, San Francisco, California, and they in turn trained 3 clinicians in India on the various aspects of warmline service.
The warmline was operated between 9:00
The data were collected using the standard forms. The forms were adapted from National Clinicians Consultation Center and separate forms were used for calls related to (1) OIs, (2) ART, (3) perinatal calls, and (4) post-exposure prophylaxis calls. The Epi Info database was used to capture and collect the data. The hardware used was a single mobile phone with a dedicated number. The calls and the answers were checked for quality using external evaluators.
The warmline marketing strategy was mainly passive through (1) a formal announcement at National and State AIDS Control Organization (NACO) trainings (only those who took their training at Government Hospital of Thoracic Medicine [GHTM], Chennai) on the last day of their induction training and (2) by word of mouth. The ART medical officers were provided with a telephone facility and computer with broadband Internet connection, at their ART centers through the national program. In addition, e-mails (roughly 800) were sent to all trained NACO medical officers and specialists to announce and describe the service. No formal marketing materials were developed.
Over a 4-month period, from May 11, 2008 to August 14, 2008, the telephonic consultation was provided to ART medical officers who have undergone 12 days of induction training at GHTM. Standardized warmline call records were reviewed and analyzed to determine basic call details (Table 1) and indicators. The data analyzed were limited to calls made between May 11, 2008 and August 14, 2008, which was the designated pilot period. Statistical analyses were performed using SPSS version 11.5 (SPSS Inc, Chicago, Illinois). We used t tests to evaluate normally distributed continuous variables, chi-square tests to evaluate differences in proportions, and Mann-Whitney test to evaluate differences in variables that were non-normally distributed. In addition, selected program staff were interviewed as a focus group using a semi-structured questionnaire to provide qualitative feedback on the program that is not available on the recording and reporting forms (ie, background/rationale, operational issues and processes, future vision of the program, etc).
Warmline Assessment Data a
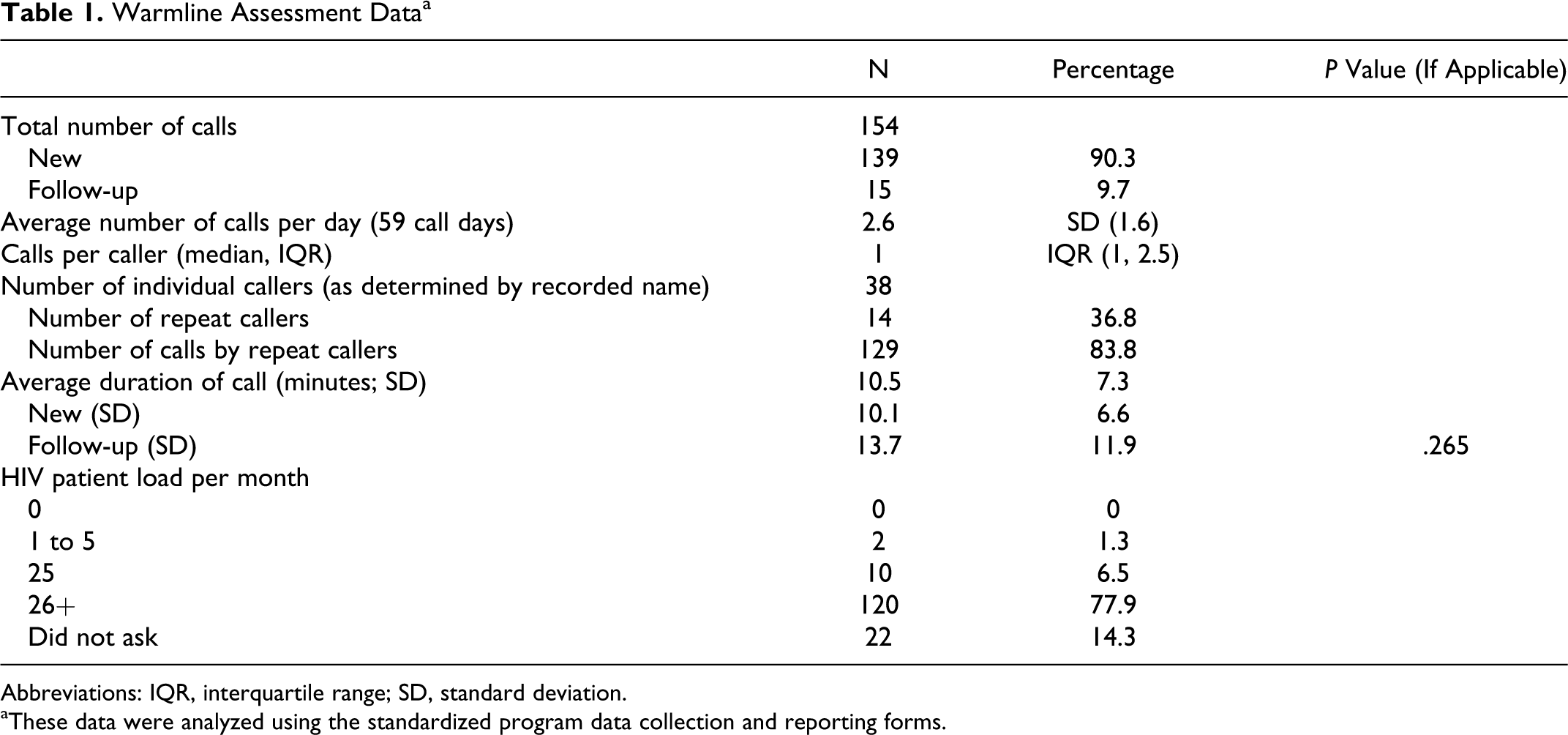
Abbreviations: IQR, interquartile range; SD, standard deviation.
aThese data were analyzed using the standardized program data collection and reporting forms.
Results
Between May 11, 2008 and August 14, 2008, the I-TECH India warmline received 154 calls (Table 1), of which 139 (90.3%) were new calls and 15 were follow-up calls. Using only the days (59 of 95 days) that calls were taken, an average of 2.6 (standard deviation [SD], 1.6) calls were taken each day during the pilot period. There were no calls on the other 36 days. A total of 38 individual doctors utilized the warmline services during the pilot period. Of these, 14 (36.8%) doctors utilized the warmline services more than once but the overall median number of calls was 1 (interquartile range [IQR] 1, 2.5); the repeat callers made 129 (83.8%) of the total calls and 1 doctor had made 67 (43%) of the total calls.
Each call took an average of 10.5 (SD 7.3) minutes to complete, and the total amount of time spent by a single consultant on the call was 27.3 minutes per day; this is the amount of time on the phone only and does not include time for documentation. Follow-up calls (13.7 minutes) appeared to take longer time than new-issue calls (10.1 minutes), but the difference was not statistically significant (P = .265).
The majority (81%) of calls were made by physicians who see a relatively high number of PLWHA (more than 26) each month (78%). Most callers (73%) came to know about the warmline through the NACO trainings conducted at our hospital, where the warmline was announced (Figure 1). The vast majority of calls (>90%) came from doctors in Tamil Nadu, with most of those (>60%) coming from the city where our hospital is located, that is, the city of Chennai (Figure 2).

Referral source of warmline callers

Warmline calls (%) by warmline callers
The majority of the warmline calls (Table 2) were related to antiretroviral (ARV) toxicities, ART initiation, and diagnosis and management of OIs. There were 14 calls related to HIV–tuberculosis (TB) coinfection. The other categories were related to PEP, perinatal-related questions, HIV-1 and HIV-2, and drug interactions, and there were few programmatic queries also. The majority (102) of calls were a related to adult treatment (Figure 3). All the calls (100%) came from the ART centers. The majority (72%) of calls came from the ART centers located at medical college hospitals of Tamil Nadu (Table 3).
Call Categories

Abbreviations: ART, antiretroviral therapy; ARV, antiretroviral; TB, tuberculosis; OI, opportunistic infection; PPTCT, Prevention of Parent to Child Transmission; WHO, World Health Organization; CME, Continuing Medical Education.

Warmline call classification
Warmline Calls by Facilitya

Abbreviation: ART, antiretroviral therapy.
Discussion
The warmline pilot in South India for a period of 95 days demonstrated the frequency of calls and also the nature of clinical and programmatic questions raised by the ART medical officers in the national program. The number of calls seems to be higher during the pilot phase when compared with National perinatal HIV Consultation Service provided by the National Clinicians Consultation Center at San Francisco General Hospital, UCSF. There were 430 calls from January 1, 2005 to June 30, 2006, but the study included calls related to perinatal issues only and the same center received calls related to PEP, and other categories of calls related to OIs, ART, and resistance issues. 1
The types of calls project the clinical issues faced by the ART medical officers in their day-to-day clinical practice in the national program. Most of the questions were related to ARV toxicities, ART initiation, and management of OI, HIV-TB coinfection, and treatment failure. Many of the questions were related to Non Nucleoside Reverse Transcriptase Inhibitor (NNRTI) toxicities, and the medical officers were mainly interested in knowing appropriate ARV substitutions. Few questions were related to diagnosis and management of lactic acidosis.
There were also few questions related to programmatic aspects, drug–drug interactions, PEP, and pregnancy. The more challenging questions were related to ART initiation in patients with HIV-1/HIV-2 dual infection. The program-related questions were mainly restricted to State AIDS Clinical Expert Panel (SACEP) referrals regarding the first-line ART treatment failure. The presence of 1 clinician, who is also an SACEP member, was an advantage to the warmline pilot activity. There were questions related to adherence also.
There were very few questions related to ARV resistance mutations. Although the resistance mutations were not practiced in the national program, few ART medical officers came across patients with resistance mutation studies and they have utilized the warmline to get appropriate answers. Most of the questions related to resistance mutations were answered by the team, but on selected occasions, the team requested assistance from National Clinicians Consultation Center at San Francisco General Hospital, UCSF. Most of the questions were related to adults and adolescents and a few questions were related to pregnancy and children. There were many repeated calls indicating the value of the warmline service as perceived by the callers. The majority of the calls were made by the ART medical officers working from health facilities with high volume patient load, indicating that the physicians with more case load came across more day-to-day issues related to case management. The medical officers requested for options despite their busy schedule.
Most of the calls came from the State where the warmline service is provided, indicating the proximity of the warmline facility and the callers’ convenience. There were few calls from outside the State, probably indicating mild marketing strategy.
Conclusion
The warmline pilot in South India demonstrated a potential model of ongoing technical assistance to ART medical officers at times of need, particularly in the areas of ART care, clinical, and programmatic issues of patients with HIV/AIDS. It also provides HIV physicians with easy and timely access to up-to-date HIV clinical information and case-specific expert consultation. The NACO may consider expanding this model of expert distance mentoring clinical support as a resource for HIV/AIDS clinical officers in India and other countries.
Footnotes
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This document was developed by the International Training and Education Center for Health (I-TECH)/University of Washington with funding from Cooperative Agreement U91HA06801-06-00 from the US Department of Health and Human Services, Health Resources and Services Administration (HRSA), and with support from the US Centers for Disease Control and Prevention (CDC). Its contents are solely the responsibilty of the authors and do not necessarily represent the views of CDC or HRSA.