
Abstract
There is a paucity of research demonstrating how HIV-funded services in Africa have improved equity and access to non-HIV services for both HIV-infected and uninfected patients. In this short communication, we describe the impact of an airborne outreach program to provide HIV services to high-HIV burden health facilities in rural Botswana. The analysis demonstrates how this HIV-funded program enhanced access to essential subspecialist services at several rural health facilities across Botswana.
Background
Despite considerable investment in HIV programs in Africa over the last decade, little is known about whether funding for HIV care and treatment services has influenced access to and quality of other health services across the continent. 1 Notably, there is a paucity of research describing whether HIV funding has improved access to non-HIV specialty services for rural communities. Although evidence from high-income countries has demonstrated that rural outreach programs can improve health coverage and outcomes of non-HIV-related diseases, 2,3 it is less clear whether HIV-specific outreach programs have affected access to non-HIV services in rural settings in Africa.
Botswana has established one of Africa’s most progressive programs for dealing with HIV despite having the second highest HIV prevalence in the world. By 2010, Botswana achieved near universal access: 93% of all eligible patients had been initiated on antiretroviral (ARV) medications. The speed and scope of Botswana’s ARV medication scale up has been attributed to a number of factors, such as significant donor investment, good governance, high-quality HIV-specific training, 4 and effective mentorship programs to facilities. 5
To support scale up, HIV specialists from the 2 tertiary referral centers, in Gaborone and Francistown, provide regular outreach support to HIV clinics across Botswana. These specialists are available to see complicated patients, including those failing second-line ARV medications, patients with complex comorbid diseases, and those with concurrent tuberculosis, especially complicated or drug-resistant tuberculosis. Although general medical practioners and nurse prescribers manage most of these HIV-infected patients, they have little formal HIV training, and mismanagement of complicated patients is not uncommon. The outreach specialist referral service provides mentorship to these health care workers as well as high-quality care even to the busiest clinics. Since 2007, this program has been facilitated by Airborne Lifeline Foundation (ALF, www.airbornelifeline.org) transporting specialists to several of the most remote, high-burden facilities. The ALF is funded by the US government through the President’s Emergency Plan for AIDS Relief (PEPFAR), 6 in collaboration with the Botswana Ministry of Health, to provide specialized HIV care and treatment services in remote, high-volume health facilities.
Apart from providing HIV specialist support, ALF’s program also facilitates provision of non-HIV subspecialty services, such as orthopedics and otolaryngology, to the same facilities. Facilities supported through airborne outreach are all sites that had limited access to any of these services before introduction of the flying outreach service and instead referred patients to 1 of the 2 tertiary referral centers, 700 km away.
In this analysis, we describe how airborne outreach to high-HIV burden facilities ensured access to both HIV and non-HIV services in rural Botswana.
Methods
This was a retrospective analysis of all outreach flights flown between July 2011 and June 2012. Specialist outreach flights were defined as planned visits by specialist-trained medical practitioners to government-determined high-volume hospitals in rural locations. Supported facilities were all assigned by the Ministry of Health and determined to be high HIV-burden sites, too remote to be supported by car-based outreach services. Supported facilities serve communities with HIV prevalence estimated at between 13.5% (Ghanzi) and 23.0% (Kasane). 7 Facilities were between 509 km (Hukuntsi) and 933 km (Kasane) away from the supporting tertiary referral center, in Gaborone.
Recorded details from flights to these facilities included the number of health care providers participating on each visit and the number of individual patient encounters, as reported by outreach clinicians, on each trip. From March 2012 onward, information on HIV status of all the patients seen on outreach was also reported.
Access to care was described in terms of subspecialist clinical services rendered at these sites, and the number of clinical encounters performed by subspecialty clinicians. These outcomes have been used widely as metrics to assess impact of outreach programs. 8 Since the analysis included only routinely collected data, institutional review board approval was not required. Descriptive statistical analysis was performed using Microsoft Excel (Microsoft, 2011).
Results
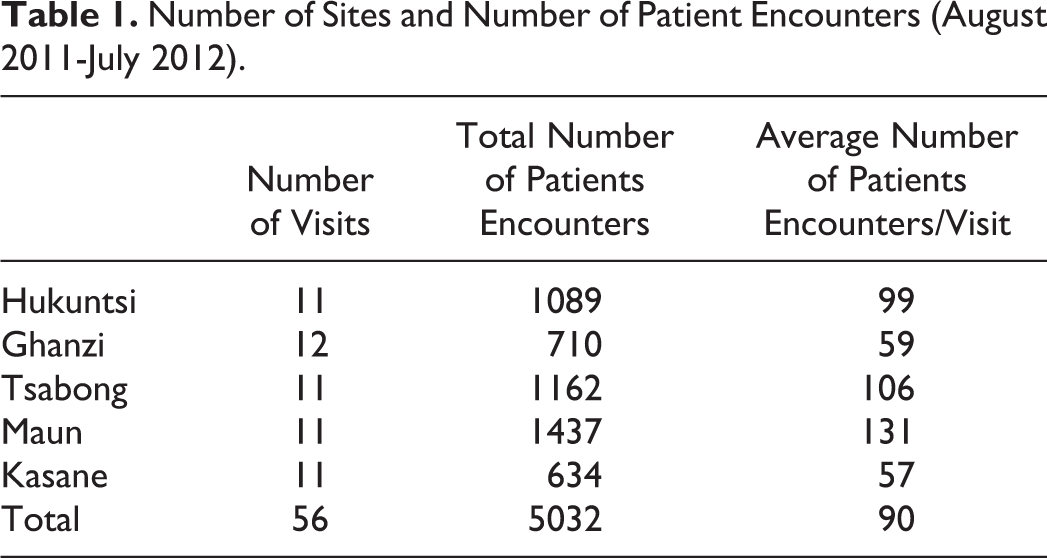
During the 12 months, between July 2011 and June 2012, airborne outreach provided essential clinical services to 5 high-volume, rural health facilities: Ghanzi, Hukuntsi, Kasane, Maun, and Tsabong (Table 1). A total of 5032 patients were seen on 56 outreach flights. An average of 90 patient encounters occurred at each site per visit. Between April and June 2012, 20% (n = 390) of the patient encounters involved HIV-positive patients (Table 2).
Number of Sites and Number of Patient Encounters (August 2011-July 2012).
Number of Patients Encounters Disaggregated by HIV Status (April-June 2012).

HIV specialists, providing pediatric and adult services, attended every flight. Available data from the 3-month period between April and June 2012 demonstrated that oncologists, orthopedic surgeons, otolaryngologists, neurosurgeons, and psychiatrists also participated regularly in the outreach visits (Table 3). During the same period, otolaryngologists and orthopedic specialists performed over a one-third of all outreach clinical encounters, seeing an average of 48 and 59 patients per outreach visit, respectively. Allied health professionals, including nurses, physiotherapists, dieticians, radiology technicians, and psychologists, were regularly present on outreach trips.
Number of Patient Encounters Disaggregated by Subspecialty Service (April-June 2012).

Abbreviation: ENT, ear, nose, and throat.
Discussion
The findings of this report are important for a number of reasons. First, the analysis demonstrates that airborne outreach is an effective and expedient strategy for providing HIV specialist care in remote, high HIV prevalent settings. Over a 3-month period, the specialists were able to undertake over 1000 HIV-specific clinical encounters. Because of the remoteness of the clinics visited, it is unlikely that many of these encounters would have otherwise occurred; patients who would have had to travel long distances to see HIV specialists at tertiary referral centers could be seen locally. Outreach visits also facilitated HIV-specific training and mentorship for doctors and nurses working at the rural clinics.
Second, the report demonstrates how HIV-specific outreach can enhance health equity, access, and outcomes across the spectrum of care, by increasing access to other subspecialty services in the rural communities. Despite the enormous investment in HIV programming in Africa, there has been considerable debate about whether HIV-specific funding has strengthened health care systems at large. 1,9,10 Given that ALF is funded by PEPFAR, this study provides a concrete example of how HIV funding has been a catalyst for strengthening delivery platforms for non-HIV programs.
Third, our data demonstrates that when resources are available, airborne outreach is feasible in an African setting. Although there is existing data from high-income countries that airborne outreach is an effective intervention, 11–13 there has been minimal operational research describing the feasibility of airborne programs in sub-Saharan African settings. Although there are reports that airborne outreach by surgical teams have been successful in Kenya, 13 Zimbabwe, 14 and Uganda, 15 we believe this is the first report describing how multidisciplinary outreach is feasible and effective in an African context.
Given that the program is funded entirely through donor support and in light of the significant constraints on health care systems in many parts of Africa, there is considerable debate about whether airborne programs are a viable solution to the challenges of inequitable access in rural African settings. Other outreach interventions, including web-based mentorship 16 and m-health programs, 17 offer alternative, effective, low-cost alternatives for providing mentorship to clinicians in remote settings. Such solutions are particularly advantageous given increasing Internet access via cellular networks across the continent. 18 Although airborne outreach offers clear benefits for in-person mentorship and patient contact, it is a far more expensive program than low-cost web- or phone-based support programs. A multifaceted outreach program, combining remote support via web-based platforms and airborne support, may represent a viable long-term option, as external funding for outreach diminishes. However, we believe that airborne outreach will remain an important facet of a sustainable long-term model of care, when expensive transport costs are weighed against the direct and indirect costs of not providing specialist clinical services to remote, high-volume facilities, especially given the large numbers of patients seen by specialists on outreach. Our research certainly suggests that airborne outreach is time saving for specialist physicians, when compared with road-based outreach to remote facilities. Nevertheless, further research is necessary to determine the cost effectiveness of airborne outreach programs.
We acknowledge that there are potential harms associated with establishing an airborne specialist outreach programs. These include extra costs and additional resources required to provide the clinics, inefficient use of specialists’ time when they could be consulting in their primary practice, and the opportunity costs associated with additional investment in the specialist sector. Nevertheless, although outreach does require additional investment on the part of the health care system when compared with traditional hospital-based care, these extra costs may be partly offset by reduced costs for the patient and the greater cost effectiveness of multifaceted interventions.
This report is limited by the fact that the data collected give little insight into the complexity of patients seen or the quality of care provided by specialists on outreach. Furthermore, it is limited by the quality of the data, since patient encounters were recorded for programmatic nonresearch purposes. Nevertheless, it is likely that the numbers reported represent an underestimate of total number of patient encounters because of underreporting of patient numbers by clinicians on outreach flights.
Conclusion
Airborne outreach to rural facilities in Botswana is necessary to support continuing HIV care at these remote, high-burden facilities. Since multidisciplinary non-HIV specialist services were also provided, the program illustrates how HIV-funded interventions can be effectively leveraged to improve access and equity to health care in remote settings in Africa. Furthermore, by fostering strong links between rural facilities and tertiary referral services, airborne outreach is an important tool for building clinical capacity. More research is warranted to determine the clinical impact and the cost effectiveness of this service.
Footnotes
Acknowledgments
We acknowledge the Botswana Ministry of Health for kindly granting us access to programmatic data. In addition, this publication was made possible through support for Airborne program from the US President's Emergency Fund for AIDS Relief.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.