
Abstract
HIV clinicians today need to move from focusing on viral suppression to a chronic disease model in which comorbid conditions and risk factors are comprehensively identified and addressed to reduce rates of serious non-AIDS-related morbidity and mortality. This study aimed to determine the prevalence of comorbid conditions in an Australian HIV-positive population. Of 180 patients included, there was a median CD4 count of 0.520 cells/mm3. The majority (88%) of patients were currently receiving highly active antiretroviral therapy (HAART). There were high rates of failure to attend clinical appointments (30%), current smoking (42%), hypertension (16%), and dyslipidemia (17%). Significant rates of dipstick-positive proteinuria (16%) and elevated blood glucose (15%) were recorded. Risk factors were commonly not addressed by the treating clinician. There is an urgent need to systematize detection and management of high-prevalence comorbid conditions to prevent premature mortality associated with serious non-AIDS events.
Introduction
Medical management of patients with HIV has been transformed since the introduction of highly active antiretroviral therapy (HAART). HIV-positive patients with access to HAART should now have a life expectancy approaching that of HIV-negative individuals. 1 With the prevention of opportunistic infections by maintenance of immune function through HAART, we have entered a new era of HIV management as a chronic disease. HIV-infected individuals have significant comorbid conditions which include high rates of smoking and smoking-related diseases, 2 –4 antiretroviral side effects such as dyslipidemia, 5 elevated rates of cardiovascular and cerebrovascular disease, 6,7 significant mental health issues including substance abuse and affective disorders, 8 increased rates of early cognitive impairment, 9 liver dysfunction related to both hepatotoxicity of antiretroviral medications and coinfection with hepatitis B and C, 10,11 osteoporosis, 12 diabetes, 13 chronic kidney disease, 14,15 and many other complex and interrelated conditions. The aim of this study was to identify the prevalence of comorbid conditions and health risk factors in HIV-positive individuals in Australia, and where these conditions were present to assess whether the risk factors were addressed by the treating clinician.
Methods
A retrospective study was performed of all HIV-1-infected patients who attended an outpatient Sexual Health and HIV Clinic in Nambour, Queensland, Australia, in 2009. All 180 patients attending the clinic were included in this study. Data were collected by review of patient records and the institution pathology database. The study was approved by the institutional human research ethics committee.
Two types of data were collected on each patient (Table 1):
Data Collected on Each Patient Included in the Audit a
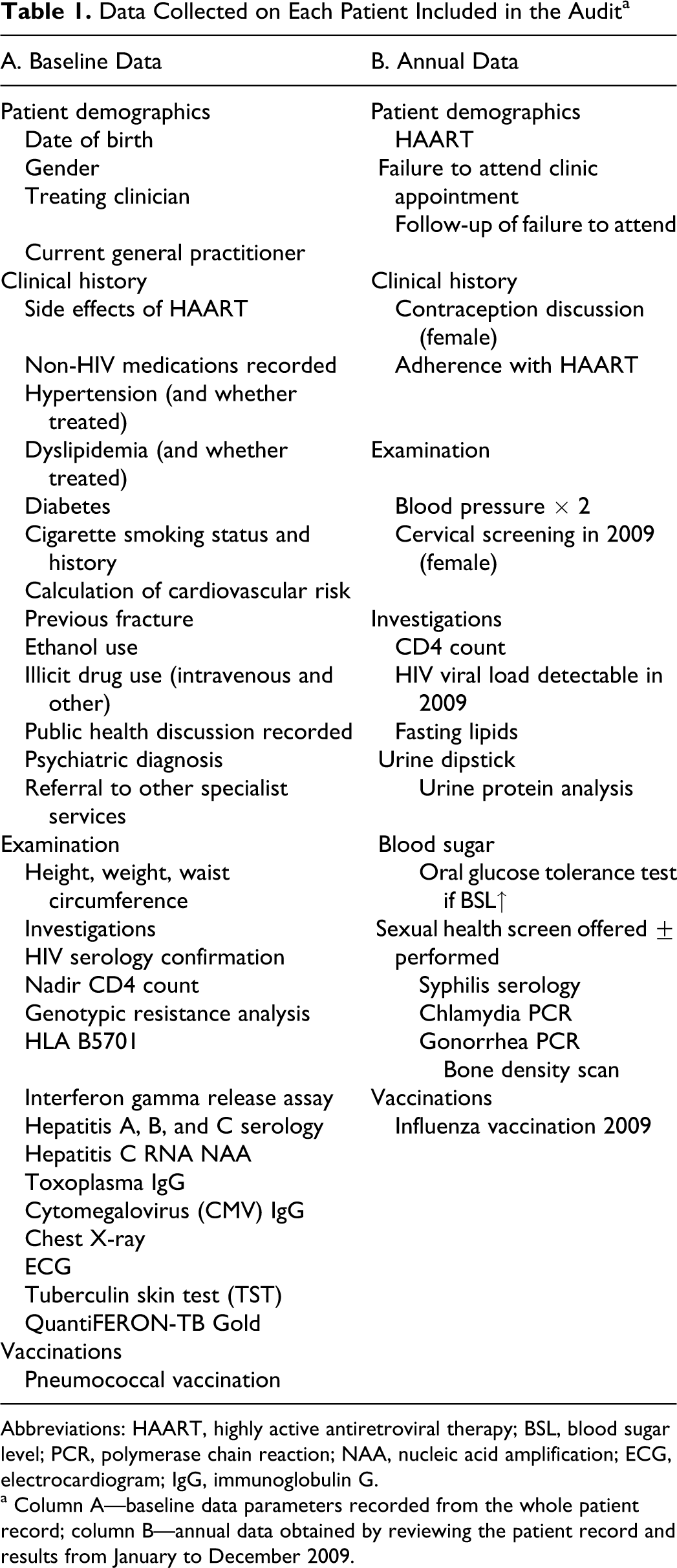
Abbreviations: HAART, highly active antiretroviral therapy; BSL, blood sugar level; PCR, polymerase chain reaction; NAA, nucleic acid amplification; ECG, electrocardiogram; IgG, immunoglobulin G.
aColumn A—baseline data parameters recorded from the whole patient record; column B—annual data obtained by reviewing the patient record and results from January to December 2009.
Baseline data: clinical assessments, tests, and examination findings that were done at initial patient assessment or irregularly in HIV care were assessed from the whole patient record.
Annual data: clinical assessments, tests, and examination findings that were considered routine at least on an annual basis in HIV care were only assessed for 2009.
Definitions
Hypertension
The definitions of hypertension and dyslipidemia were defined by the Australian Therapeutic Guidelines (eTG complete [Internet]. Melbourne: Therapeutic Guidelines Limited; Accessed 2010, February<https://online-tg-org-au.cknservices.dotsec.com/ip/>). Normal blood pressure was <120/80 mm Hg and target treated blood pressure levels were <125/75 for patients with proteinuria, <130/80 for patients with any associated conditions or end-organ damage, and <140/90 for other patients. Treatment and target lipid levels were defined according to patient risk per Australian Therapeutic Guidelines.
Proteinuria
Proteinuria was assessed by urinary dipstick analysis. An algorithm guiding the investigation of abnormal dipstick results was used by the clinic, and compliance with this algorithm was assessed in the study. The algorithm recommends repeat testing of all patients with trace protein on urinary dipstick in 3 months and further investigation of all patients who have more than trace protein in their urine. In patients with greater than trace protein, a protein–creatinine ratio is performed and referral to a specialist nephrology service is indicated if >100 mg/mmol is detected.
Australian Alcohol Guidelines
Current Australian guidelines for alcohol consumption were taken from the Australian Government Department of Health and Ageing Web site, www.alcohol. gov.au, which recommends no more than 2 standard drinks on any day and no more than 4 standard drinks on a single occasion.
Interpretation of Hepatitis B Serologic Test Results
The interpretation of hepatitis B serology as susceptible, immune due to natural infection, immune due to hepatitis B vaccination, acutely infected, chronically infected or unclear, followed the US Department of Health and Human Services (DHHS) Centers for Disease Control and Prevention guide for the interpretation of hepatitis B serologic test results (www.cdc.gov/hepatitis).
Results
Patient Demographics
One hundred and eighty HIV-positive patients attended Clinic 87 from January to December 2009 for HIV care (Table 2). The majority of patients (89%) were male. The most common risk factor for transmission was homosexual sexual activity. A significant proportion (34%) of patients did not list a current general practitioner (GP). If a GP was listed, letters were sent to the GP in 83% of cases.
Characteristics of HIV-Positive Patients Audited

Abbreviations: IQR, interquartile range; IVDU, intravenous drug use; GP, general practitioner.
HIV-Specific Results
In all, 88% of patients (n = 158) studied were currently receiving HAART. Median CD4 counts were good with a median value of 0.520 cells/mm3 (27%) and an interquartile range (IQR) of 0.400 to 0.700 cells/mm3, and only 13 patients had a CD4 count less than 0.200 cells/mm3. The median nadir CD4 count was 0.228 cells/mm3. Twenty-eight percent of patients receiving HAART had a detectable HIV viral load during 2009. To avoid detecting “viral blips” that have been observed with the recent introduction of the highly sensitive Roche Cobas Amplicor assay, a detectable viral load was defined as >200 copies/mL. The presence or absence of side effects related to HAART was documented in 42% patients receiving HAART. The clinician’s impression of adherence was reported in 85% patients, with 72% of patients recording adherence with HAART and nonadherence recorded in 13%. A genotypic resistance analysis (GRA) had been performed (at any time) in 32% of patients.
Screening for Infections
Latent Tuberculosis
Fourteen percent of patients attending Clinic 87 have been screened for latent tuberculosis either by a tuberculin skin test (TST) or by an interferon-γ release assay (Table 3). Tuberculin skin test is not available locally in Nambour. Ten percent of patients had been screened for latent tuberculosis (TB) by interferon-γ release assay which is currently available.
Screening for Infections
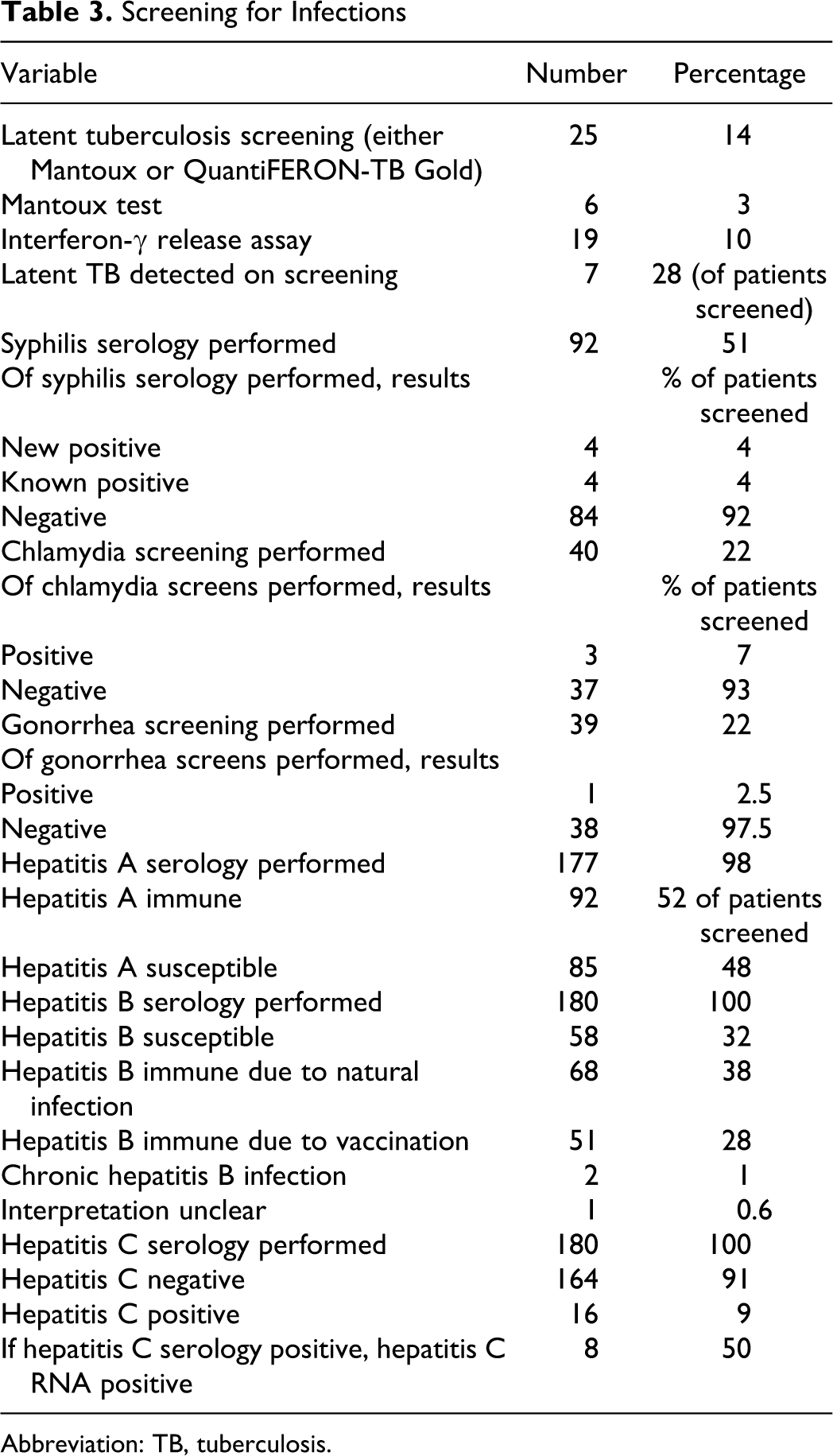
Abbreviation: TB, tuberculosis.
Sexually Transmitted Infections
In 2009, in 51% of patients syphilis serology was performed, and in 22%, chlamydia and gonorrhea polymerase chain reaction (PCR) was performed. From this testing, there was 1 new diagnosis of syphilis, 3 cases of chlamydia, and 1 case of gonorrhea.
Viral Hepatitis
Screening for hepatitis was comprehensive, with 98% patients tested for hepatitis A, and 100% patients tested for hepatitis B and hepatitis C. Of patients tested for hepatitis A, 52% were immune. Of patients tested for hepatitis B, 66% were immune either from immunization or from natural infection. Chronic hepatitis B infection occurred in 1% patients, and 32% were susceptible to hepatitis B infection. Nine percent (n = 16) of patients screened for hepatitis C had positive serological tests, and of those, 50% (4.4% of all patients) had detectable hepatitis C RNA.
Screening for Noninfectious Comorbid Conditions and Risk Factors
Cardiovascular Risk
Smoking
Smoking status was documented in 80% patients. Of these patients, 42% were current smokers (Table 3). Twenty-one percent of patients were ex-smokers, giving a total of 63% of patients with a previous or current smoking history (of the patients in whom this was recorded). A discussion of smoking cessation was documented for 53% of current smokers.
Hypertension
Sixty-five percent of patients had their blood pressure measured on at least 2 occasions in 2009. Of these patients, 16% were hypertensive (eTG complete [Internet]. Melbourne: Therapeutic Guidelines Limited; Accessed 2010, February <https://online-tg-org-au.cknservices.dotsec.com/ip/>). Of the hypertensive patients, 42% were receiving antihypertensive treatment; and of those treated, only 2 patients (25%) were reaching blood pressure targets defined by Therapeutic Guidelines.
Dyslipidemia
Fasting lipids were measured in 69% patients, in 2009. Treatment was indicated in 17% patients in whom lipids were measured (eTG complete [Internet]. Melbourne: Therapeutic Guidelines Limited; Accessed 2010, February <https://online-tg-org-au.cknservices.dotsec.com/ip/>). Treatment was prescribed in 42% patients in whom lipid therapy was indicated; and of those treated, 63% reached target lipid levels on treatment.
Diabetes
Blood glucose (fasting or random) was measured in 98% of patients, and 27 patients (15%) had an elevated blood glucose. Six patients had known diabetes, and oral glucose tolerance tests were performed in further 2 patients. The remaining 19 patients did not have further assessment for their elevated blood glucose.
Calculating cardiovascular risk
Cardiovascular risk was calculated in 2 patients (1%).
Renal Disease
A total of 96 patients (53%) had a urine dipstick analysis performed in 2009. Of the 96 patients who underwent urine testing, 54 (56%) had protein detected in their urine. Trace protein was detected in 39 (41%), 1+ protein in 13 (14%), and 3+ protein in 2 (2%) patients. Current clinical practice at Clinic 87 is to follow a renal algorithm that recommends repeat testing of all patients with trace protein in 3 months and further investigation of all patients who have more than trace protein in their urine. In patients with greater than trace protein, a protein–creatinine ratio is performed and referral to a specialist nephrology service is indicated if >100 mg/mmol is detected. The renal algorithm was followed in 19 (35%) patients with protein detected on urine dipstick.
Osteoporosis
Twenty-two (12%) patients had a history of a fracture, 5 of which had been identified as an osteoporotic fracture and 3 had bone mineral density assessed.
Female Patients
Of 20 female patients included in this study, 17 had undergone cervical screening in 2009. A discussion about contraception was documented for 15% female patients.
Substance Use
Of 63% patients in whom ethanol use was recorded, 19% drank greater than the Australian guidelines (www.alcohol.gov.au, Department of Health and Ageing). Active intravenous drug use (IVDU) was documented in 3 patients (1.7%) and 16% patients had a history of past IVDU. Thirty patients (17%) had documented the use of nonintravenous illicit drug.
Psychiatric Diagnoses or Symptoms
Psychiatric diagnoses or symptoms included documentation of depression and anxiety by medical practitioners. Thirty-six percent of patients had an active diagnosis (the majority, 80%, documented depression or anxiety symptoms).
Public Health Discussion
Eighty-two percent of patients had a documented discussion on the legal implications of HIV transmission recorded in their records.
Failure to Attend an Appointment
Thirty percent of patients failed to attend at least 1 appointment in 2009.
Discussion
Identifying high rates of psychiatric symptoms, failure to attend clinic appointments, substance abuse, and risk factors for serious non-AIDS-related conditions such as cardiovascular disease, this study clearly demonstrates the challenges of providing comprehensive care to HIV-positive patients in Australia, today. In addition to multiple pathologies, the focus of the clinician is often on multidrug antiretroviral regimens with complex drug interactions, reducing attention on preventative approaches for comorbid conditions. Few HIV clinicians in Australia are experienced in the management of chronic disease and aging populations, which in combination with a lack of engagement of HIV-positive patients with general practitioners, may lead to the underinvestigation and treatment of risk factors for long-term non-AIDS–related conditions.
It is of concern that a viral load was detectable in 28% patient on HAART. As the study recorded data over a 1-year period, it is likely that some patients with a detectable viral load were initiating HAART and therefore not fully suppressed, resulting in a detectable viral load on treatment. Future studies will record the date of HAART initiation for patients with a detectable viral load.
This study revealed comprehensive screening for coinfection with viral hepatitis but inadequate screening for sexually transmitted infections (STIs) and latent TB. Vaccination rates should be increased to reduce the number of patients that remain susceptible to hepatitis A and B. Screening of men who have sex with men (MSM), which constitutes a large majority of the study population, for STIs including syphilis, gonorrhea, and chlamydia is recommended annually, with increased screening for patients who are at increased risk (STI testing guidelines for MSM, www.racp.edu.au, Australasian Chapter of Sexual Health Medicine). This study demonstrated 3 new cases of chlamydia diagnosed in 40 patients screened in 2009. It is likely the low screening rate would have missed other cases of chlamydia. Screening for syphilis and gonorrhea was also low.
Screening for the presence of latent TB by TST is recommended at initial patient assessment for all HIV-positive patients by the DHHS) Guidelines for the use of antiretroviral agents in HIV-1-infected adults and adolescents. Concerns among HIV clinicians regarding the use of interferon-γ release assays in screening HIV-positive patients are reduced with recent evidence supporting the sensitivity of this test in HIV patients. 16 –18 Of the 25 patients who were screened, the positive screen rate of 28% indicates that there are likely to be a significant number of patients who have not been screened and who do have latent TB. Therefore, the introduction of routine QuantiFERON-TB Gold testing of all patients attending Clinic 87 in the future will be one outcome from this study.
The prevalence of current cigarette smoking in this study (42%) is dramatically higher than that of the general Australian population (15.6%). 19 This study documented a record of smoking status in 79% patients, but a formal discussion on smoking cessation was only recorded in 53% smokers. HIV clinicians may not feel confident in their ability to provide smoking cessation advice. 20 The development of resources and clinical algorithms to guide HIV clinicians in smoking cessation interventions is currently underway in Queensland.
A significant proportion of patients in this study did not have screening for hypertension and dyslipidemia in 2009. Of those that were hypertensive or had dyslipidemia documented, treatment was not always initiated, and treatment targets were not met in a significant proportion who were treated. Cardiovascular risk calculation was underutilized. Sixteen percent of patients that had their blood pressure measured had documented hypertension. This is consistent with the documented rates of hypertension in the Australian population of similar median age, and the proportion untreated are also consistent with Australian data. 21 In a patient group with a high prevalence of cardiac risk factors, modifiable risk factors require increased attention to reduce future cardiovascular morbidity.
Of the 53% patients who had urine dipstick analysis performed, an extremely high number (56%) had protein detected by dipstick testing in their urine. The majority (41%) had only trace protein, but 16% had 1+ or greater protein detected. Even trace protein on urinary dipstick has been identified as a significant hazard for the development of end-stage renal disease, although this has not been assessed in HIV-positive cohorts. 22 Previous studies have documented microalbuminuria or proteinuria in 31% HIV-infected patients, but the value of microalbuminuria in predicting progression to overt proteinuria requires longitudinal studies. At this point, progression does appear to occur in at least a proportion of patients with microalbuminuria and HIV, but the value of interventions is not clear. 23 Smoking is identified as a risk factor for renal impairment and proteinuria and may contribute significantly to the high rates of proteinuria in the HIV-positive population. 19 Mineral bone disease occurs at increased rates in HIV-positive populations, and a progressive reduction in bone mineral density related to the duration of HIV infection has been observed. 12,25 Bone disease occurs at an earlier age than in the HIV-negative population and is multifactorial in origin. 26 The European AIDS Clinical Society (EACS) recommends risk stratification for osteoporosis screening based on conventional risk factors and the World Health Organization Fracture Risk Assessment Tool. Patients in this study group have risk factors for mineral bone disease including high alcohol use and smoking. It is likely that HIV infection is also a secondary risk factor although the quantification of this risk is not validated at this point. 27 Screening for osteoporosis was performed only in 3 patients, despite 12% patients having a documented fracture, 5 of which were identified as osteoporotic. As the HIV population ages, screening and treatment for osteoporosis needs to be addressed, with the development of consensus guidelines for clinicians to follow. From the deficiencies in clinical care of HIV-positive patients identified by this study, a care plan has been developed to facilitate comprehensive nursing and medical assessment of all relevant clinical parameters and risk factors. This care plan will be used at each HIV clinical visit. HIV clinics need to institute regular auditing to identify areas of deficiency in their current clinical practice and to ensure that their clinical practice is improving. A further study will be performed at this clinic in 12 months after the introduction of the care plan to assess changes in the parameters assessed in this study.
Conclusions
Systematization of HIV clinical care by the development of clinical care plans and HIV-specific algorithms for the investigation and management of comorbid conditions and risk factors would be expected to lead to more rigorous and comprehensive patient assessment and management and allow for the development of auditable standards and benchmarking between HIV clinics. As the HIV population in Australia ages, there will be a need for multidisciplinary HIV care and increased engagement and communication with primary care providers. Whole patient care is both an organizational and clinical challenge for HIV clinicians today.
Footnotes
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) received no financial support for the research, authorship, and/or publication of this article.