
Abstract
Keywords
Introduction
Cervical cancer, a leading cause of mortality worldwide, kills nearly 300 000 women annually. 1 The vast majority of these deaths occur in developing countries, few of which have global cervical cancer screening programs. Human papillomavirus (HPV) infection of the anogenital tract is strongly associated with cervical neoplasia and cervical cancer. HIV seropositivity is a known risk factor for HPV infection. 2–6 HIV-infected women have 4 to 6 times greater chance of developing invasive cervical cancer than HIV-seronegative women. 3,7–10
Systematic cytologic screening programs using routine Papanicolaou (Pap) testing, with effective follow-up biopsy and treatment, have dramatically decreased the morbidity and mortality of cervical cancer in developed countries. 11 Such programs require (a) reliable health care infrastructure; (b) significant political support; (c) adequate numbers of highly trained specialists and technicians to collect and evaluate specimens; and (d) access to costly supplies and equipment. The absence of these components makes such programs difficult to implement in developing countries. Furthermore, Pap smears require multiple clinic visits. Patients with abnormal Pap smears must return first for confirmatory biopsy and again for treatment. Unfortunately, local conditions in many developing countries render follow-up for abnormal Pap smears difficult. Recent attention has thus focused on alternative methods of cervical cancer screening in resource-poor nations.
One promising method is direct visual inspection with acetic acid (VIA), a technique in which 3% to 5% acetic acid (household vinegar) is applied to the cervix, which is then assessed for characteristic acetowhite changes suggestive of cervical neoplasia. Although it is possible to view these lesions with the naked eye, magnification is sometimes used in detection. The technical and procedural advantages of VIA over cytology-based screening programs in low-resource areas are numerous. Visual inspection with acetic acid is inexpensive, requires minimal equipment that can be easily obtained in most developing countries, and can be performed by nonphysicians with appropriate training. Furthermore, this technique yields immediate results, making it possible to both screen and treat women in a single visit. Recent data have shown the screen-and-treat approach by VIA to be safe, effective, and cost-effective. 12,13
Although evidence exists supporting the potential utility of VIA as an alternative to cytologic screening in resource-poor countries, limited experience exists examining its usefulness in HIV-infected women. The correlation between HIV, HPV, and the development of cervical neoplasia indicates that screening programs in developing countries with high HIV prevalence are an important public health intervention.
We sought to assess the degree of correlation between Pap smear and VIA findings among a group of HIV-infected women in Phnom Penh, Cambodia.
Methods
Study Population
A total of 304 HIV-infected women receiving care at the Community Resource Center in Phnom Penh, Cambodia, between January 2005 and February 2006 were referred to the women’s clinic for routine gynecological care including Pap smear and VIA screening. This retrospective study by chart review was approved by the Institutional Review Boards of Brown University and of Sihanouk Hospital Center of HOPE, Phnom Penh, Cambodia. All women were screened for cervical cancer simultaneously by Pap smear and VIA. Pregnant women were excluded. Because no routine gynecologic screening program exists, and patient records are incomplete, we believe that no women had had previous Pap smears.
Procedures
Pap smears were obtained using a plastic or wooden spatula and an endocervical cytobrush and were fixed on a glass slide with cytological fixative. Visual inspection with acetic acid was then performed. A cotton swab was soaked in 3% to 5% acetic acid and applied to the cervix for 30 seconds. The cervix was visualized under 4× magnification by a digital camera and examined for the presence of acetowhite lesions. VIA was classified as negative, positive or cancer based on criteria from the International Agency for Research on Cancer.14 With the use of 4x magnification visible lesions could be further differentiated as low grade or high grade based on lesion characteristics using criteria established by the American Society for Colposcopy and Cervical Pathology. 15 All VIA screenings were performed by 1 of 2 physicians trained in VIA technique. Digital images of 75% of abnormal VIA tests were sent to Women and Infants Hospital in Rhode Island for quality assurance (QA), with good concordance between abnormal readings. A subset of normal VIA images were included in the QA process as well.
All Pap smears were read at the Sihanouk Hospital by a Cambodian physician trained in cytopathology. In addition to the standard Bethesda classifications, “Inflammation” was added, which described a cytologic pattern of increased inflammatory cells without cellular neoplasia (Table 2 ). 16 Digital images of 25% of the slides were sent via telepathology to pathologists at the University of Basel, Switzerland, for QA purposes. The results of the 2 tests were then compared. All Pap smears read as atypical squamous cells of undetermined significance (ASCUS) or higher were considered positive. Those classified as “inflammation” were considered negative. All abnormal VIAs were considered positive.
Comparison of VIA to Pap
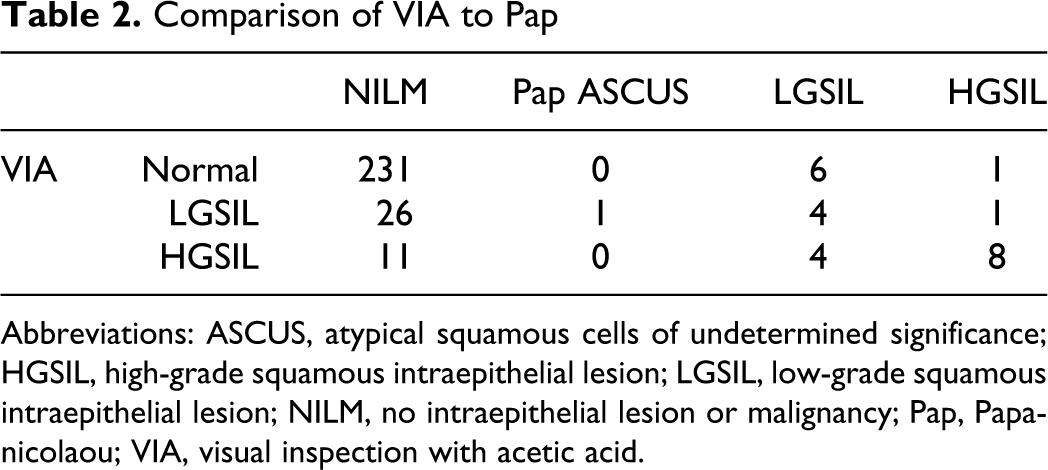
Abbreviations: ASCUS, atypical squamous cells of undetermined significance; HGSIL, high-grade squamous intraepithelial lesion; LGSIL, low-grade squamous intraepithelial lesion; NILM, no intraepithelial lesion or malignancy; Pap, Papanicolaou; VIA, visual inspection with acetic acid.
Statistical Methods
McNemar chi-square test was used to assess for equality of proportions of positive cases between the Pap smear and VIA groups. Chi-square and descriptive statistics were performed using Stata v.9 (Stata Corporation, College Station, Texas). We used an α probability of .05 as the threshold for statistical significance.
Results
Complete data were available on 293 of 304 women screened. Eight women were missing Pap smear results. Three were missing VIA results. Demographic information is shown in Table 1 . Visual inspection with acetic acid readings between the research site and the blinded reviewer were in agreement 70% of the time overall, with 75% agreement for normal, 75% for LGSIL, and 63% for HGSIL. There was a slight tendency for the research site to classify a finding as low grade, which the blinded reviewer felt was of high grade. Pap results between the research site and the blinded reviewer were in agreement overall at a rate of 93%, with 98% agreement for no intraepithelial lesion or malignancy (NILM), 90% for LGSIL, 95% for HGSIL, and 90% for ASCUS.
Demographics

Abbreviation: HAART, highly active antiretroviral therapy.
Of the 293 women, 55 (19%) screened positive on VIA. Of the 293 Pap smear cytologic specimens collected, 25 (8.5%) were positive. Among these 25 with abnormal cytology, 1 had ASCUS, 14 had LGSIL, and 10 had HGSIL. Visual inspection with acetic acid detected 18 of the 25 patients who were positive by cytology, and was negative in 231 of the 268 who were negative by cytology. Of the women who screened positive on VIA, 37 (67%) had a negative Pap smear. McNemar chi-square test demonstrated significant differences in the proportion of positive diagnoses between the Pap smear and VIA methods (P < .001).
Of the 55 women with positive VIA, 32 (11%) were recorded as LGSIL and 23 (8%) as HGSIL. Of the 23 women with high-grade VIA, 8 (35%) also had HGSIL by Pap, 4 (17.3%) showed LGSIL by Pap, and 11 (48%) were negative by Pap. Of the 238 examinations that were normal by VIA, 7 (3%) showed abnormalities by Pap smear—1 showing HGSIL and 6 LGSIL (Table 2).
Discussion
Cambodia is a poor country with a paucity of health care resources and no routine gynecologic care. Cambodia has an estimated HIV seroprevalence of 0.7%; women comprise nearly 50% of adults living with HIV/AIDS. 17 The International Agency for Research on Cancer’s 2008 GLOBOCAN statistics report an annual cervical cancer age standardized rate of 27.4, which is significantly higher than in any other country in the region. 1 An effective alternative to cytology-based cervical cancer screening encompassing the unique association between HIV and HPV is needed.
Visual inspection with acetic acid has found a place as an alternative, low-cost method of cervical cancer screening in other low-resource countries. 18 Previous studies comparing VIA to Pap smear in women with no HIV infection, using histology as the gold standard, have reported sensitivities and specificities ranging from 64% to 98% and 66% to 96%, respectively. 18 Despite the relatively high sensitivities and specificities, studies have consistently shown that VIA yields falsely abnormal results more often than does Pap smear, resulting in low positive predictive values.
Most developing countries are burdened with numerous health care problems all competing for limited resources. The usefulness of this technique thus remains controversial, and the adoption of universal screening with VIA continues to be considered on a country-by-country basis.
As women now make up half of all people living with HIV/AIDS (PLWHA), the VIA debate must take into consideration HIV-infected women. To date, little has been published on the usefulness of this technique within this population. Our study serves as a preliminary evaluation of VIA as a cervical cancer screening tool in HIV-infected women. Our data show a reasonable correlation between VIA and Pap smear. Visual inspection with acetic acid was abnormal in a significantly higher number of patients than was Pap smear (19% vs 8.5%, respectively). This finding is consistent with data from previous studies comparing VIA to Pap smear in women with no HIV infection. 19–21 Visual inspection with acetic acid detected abnormalities in 18 of the 25 women who were abnormal by Pap smear. It is of significant concern that 7 women who were positive by Pap smear (1 HGSIL and 6 LGSIL) were normal by VIA.
If used as an alternative to cytology, our results indicate that VIA screening could result in a high rate of referral for colposcopy compared to cytology, a result that may be burdensome in many developing countries that lack necessary equipment and trained professionals. However, because of the significantly increased risk of HPV infection, and the accelerated progression from cervical neoplasia to invasive cancer in HIV-infected patients, the dangers of failure to diagnose a potential dysplatic lesion may outweigh the burden of increased numbers of colposcopy among HIV-infected women.
Visual inspection with acetic acid may be a suitable alternative to Pap smear in HIV-infected women in low-resource areas with the caveat that it may increase the need for colposcopy. More studies on VIA and Pap with histologic confirmation among HIV-infected women in developing countries are needed. Our center is currently in the process of implementing a colposcopy program that will allow us to further evaluate VIA, Pap, and biopsy in our setting.
There were several limitations to this study. First, we did not have the resources to perform cervical biopsies and histology, the gold standard for diagnosis of cervical neoplasia, on all study participants. We were, therefore, unable to determine the test characteristics of VIA and Pap, and thus limited in the conclusions that we could make regarding the accuracy of VIA compared to Pap smear in HIV-infected women. Our hospital has recently acquired a colposcope and further follow-up with histology is now possible. Second, we were limited by a small sample size and limited budget. In a larger trial, it would thus be more appropriate to perform biopsies on all women. It should be noted, however, that even colposcopy with biopsy has limitations in sensitivity. One study found that increasing the number of biopsies performed increased the sensitivity of diagnosing cervical neoplasia from 68% using 1 biopsy to 82% using 2 biopsies. 22 Third, VIA examinations were performed by 1 of 2 physicians. Given the subjectivity in reading VIA, it would be more appropriate had all patients been examined by the same physician. Our QA process did involve reading by a single clinician with good agreement. While there were some discrepancies in the opinions of the clinicians, our overall agreement compares favorably to that of expert colposcopists from the United States in 1 published study, where agreement was only 57%. 23 Visual inspection with acetic acid seems best suited as a screening test to identify normal findings that need no further workup. The best strategy for management of patients with abnormal findings on VIA should be investigated. Should such patients have close follow-up with repeat VIA, undergo biopsy, or proceed directly to treatment, as some have advocated? 12 Finally, some investigators have found a relationship between cervical neoplasia and CD4 count. 24 This association seems most significant in relation to nadir CD4. 25 One study found no association between CD4 and cervical intraepithelial neoplasia (CIN), although nadir CD4 was associated with CIN recurrence. 26 Others have determined that the use of antiretroviral therapy (ART) facilitates clearance of HPV but not to a regression in neoplasia. 27 This retrospective analysis did not include CD4 or antiretroviral use as variables. A further analysis of a larger data set is currently underway to evaluate the impact of CD4 and antiretroviral use on cervical neoplasia in this cohort.
Footnotes
The author(s) declared no potential conflicts of interests with respect to the authorship and/or publication of this article.
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: This project was supported by the National Institutes of Health Fogarty International Research Collaboration Award [R03 TW006981]; Fogarty AIDS International Training and Research Program [NIAID TW000237]; World AIDS Foundation [320 (03-038)]; National Institutes of Health BIRCWH Scholars Program [K12 HD043447]; National Institutes of Health [NIAID RO1AI40350, K24 AI066884] and Brown/Tufts/ Lifespan Center for AIDS Research [NIHP30AI42853].