
Abstract
Parental stress increased during the COVID-19 pandemic. Families with children with an intellectual or developmental disability (IDD) and extensive support needs—such as complex communication needs—experienced additional challenges, including service loss and difficulties accessing virtual learning. The purpose of this study was to understand the experiences of parents (N = 37) with children with IDD and complex communication needs related to parental stress and family resilience. Qualitative interview and quantitative survey data were collected within a convergent parallel mixed-methods design, with interviews occurring three times across the 2020–2021 school year. The two sets of data were analyzed separately and then integrated using back-and-forth exchanges and a joint display. Findings indicated that families showed resilience through family adaptation and cohesion—creating rhythms and routines that fostered togetherness—and by growing in advocacy and empowerment related to their child’s learning. But, many parents worried that they were not able to do enough for their child. Social support predicted lowered parental stress and stronger family resilience; yet, perceived social support varied widely across families—particularly support from teachers and service providers. This study provides important insight into family experiences during a unique time with the COVID-19 pandemic while pointing to important ways to strengthen family resilience long into a postpandemic future.
Substantive literature focuses on how families adjust to having a child with an intellectual and developmental disability (IDD; Miodrag & Hodapp, 2010; Pastor-Cerezuela et al., 2016; Peer & Hillman, 2014), including specifically when the child has extensive support needs (i.e., needing significant support across settings, such as for daily living, communication, behavior, social skills, and relationships). Much written about family adjustment seems to be built on the same premise—that caring for a child with a disability who has extensive support needs adds stress and can cause strain for the parent and family (e.g., Hayes & Watson, 2013). Indeed, parents of children with disabilities do report higher rates of stress, anxiety, and depression than parents of children without disabilities (Hayes & Watson, 2013; Lievore et al., 2023), especially when children have complex communication or behavior support needs (e.g., Rivard et al., 2014). But, standing somewhat in tension to this premise, McConnell et al. (2015) found that two-thirds of parents agreed or strongly agreed with the statement “Overall having a child with disabilities has been positive for our family.” In addition, parents often talk about benefits coming from parenting a child with a disability—including personal development, increased spirituality, seeing the child as a source of happiness and fulfillment, and expanded relationships (Beighton & Wills, 2019; McConnell et al., 2015).
Instead of starting from the premise that caring for a child with a disability is a stressor, other researchers have used ecocultural theory to emphasize the role of social-ecological factors that impact family functioning and resilience (McConnell & Savage, 2015; Ungar, 2011). Ecocultural theory asserts that (a) societal and other factors outside the family influence family functioning and (b) all families—not just families of children with disabilities—face the same task: constructing a stable routine that allows them to attain their goals for their family, in light of their values, and given the demands and circumstances they face (Gallimore et al., 1989; McConnell & Savage, 2015; Peer & Hillman, 2014). In other words, ecocultural theory recognizes that families are affected by social and societal forces around them, but also that families are more than “hapless victims” to these forces (Gallimore et al., 1989, p. 217). Family members, both individually and collectively, take action to accommodate to achieve the type of life they want to have (Gallimore et al., 1989; McConnell & Savage, 2015). Therefore, these outside forces shape families’ internal characteristics and actions, which then mix together to form each family’s unique social-ecology, called the family “niche” (Gallimore et al., 1989).
Examining aspects of the family niche can lead to important insight about supporting stronger outcomes for families of children with IDD who have extensive support needs, such as decreasing parental stress and promoting family resilience. Although it is important to understand family stress and resilience under any circumstance, this need grew during the COVID-19 pandemic. Schools and clinics closed their doors to slow the spread of the novel coronavirus. Even with the use of virtual schooling and telepractice-based services, the abrupt and severe disruption of routines had profound effects on families with children with disabilities: increasing caregiving responsibilities, limiting access to therapies and educational services, creating social isolation, and amplifying uncertainty about the future (Neece et al., 2020; Rossetti et al., 2023; Spann et al., 2023). Therefore, it is critical to understand family stress and resilience during this period—not only to increase awareness and empathy for families’ lived experiences, but also to inform future efforts that might help ensure that all families have what they need to flourish.
Parental Stress for Parents of Children With IDD
Parenting any child—with or without a disability—can be stressful. When parents experience distress from the demands associated with parenting, that distress is typically called parental or parenting stress (Berry & Jones, 1995; Louie et al., 2017). Too much parental stress impacts family functioning for many reasons, including because parents who are stressed may have more difficulties caring for and relating to their children (Miodrag & Hodapp, 2010). Importantly, social-ecological factors (e.g., service access, social support) can mitigate or worsen parental stress for families of children with disabilities. Access to both formal and informal supports was disrupted during the COVID-19 pandemic. Parents often reported that their children did not have the individualized accommodations, services, and supports they needed during the emergency use of virtual instruction (Navas et al., 2022; Spann et al., 2023). Meeting children’s educational needs at home—with the loss of services—was often an incredible source of stress (Neece et al., 2020; Rossetti et al., 2023).
In the midst of these challenges, social support may be one of the greatest protective factors (Drogomyretska et al., 2020; Robinson & Weiss, 2020). Social support is multidimensional and includes different types of resources, including physical or tangible assistance, information sharing, and emotional support. Families can receive social support from both formal and informal sources. Formal social support typically refers to support from professionals (e.g., educators, service providers), whereas informal social support refers to support through relationships with friends and family (McIntyre & Brown, 2018). In particular, perceived social support seems to play a greater role in reducing stress than actual received support (Robinson & Weiss, 2020). Received social support refers to the helping behaviors that are actually exchanged within a person’s social network, whereas perceived social support is related to satisfaction—the belief about whether support is adequately available.
Parents of children with disabilities differ widely in their satisfaction with their social support networks, but many families report difficulties accessing the formal and informal social support they want and need (Resch et al., 2010). One explanation for this gap is that access to social support can be tied to complex and intersecting factors, including child-related, family-related, and systems-related factors (McIntyre & Brown, 2018). For example, some parents of children with extensive support needs may be more likely than other parents to seek support from professionals, family members, or friends to care for their child (e.g., information, emotional support, tangible help). Yet, at the same time, these families might not feel satisfied with their social support networks for a variety of reasons. Service providers may struggle to meet child and family needs well if resources, time, or expertise to work with students with extensive support needs are limited (Andzik et al., 2023). Or, with regard to informal support, families of children with extensive support needs may feel they have to pull back from pursuing activities or relationships outside the home to have time to care for their child (Boyd, 2002).
Family Resilience for Families With Children With IDD
Family resilience is important to consider alongside parental stress. Family resilience is more than simply avoiding being negatively impacted by difficult circumstances (e.g., absence of family dysfunction or psychological distress). Instead, resilience is marked by families’ capacity to adapt positively and flourish in the midst of many different circumstances. Walsh (2021) calls resilience “the potential for personal and relational transformation and positive growth that can be forged out of adversity” (p. 256). In other words, resilience can produce positive outcomes at the personal and relational-family level such as optimism, self-efficacy, acceptance of change, and strong family relationships (McCubbin & McCubbin, 1996; Pastor-Cerezuela et al., 2016).
Resilience involves meeting stressors with adaptation, aided by protective factors that buffer stress and empower families (McCubbin & McCubbin, 1996). Importantly, stress and resilience appear to impact one another transactionally; family resilience can protect against parental stress, but high stress levels may also negatively impact family resilience (Pastor-Cerezuela et al., 2016; Zhao et al., 2021). Beyond this relationship, families can build resilience by mobilizing strengths and resources through dynamic processes of accommodation and adaptation such as making meaning of adversity, having positive outlook, turning to faith and spirituality, being flexible, communicating and prioritizing connectedness, and problem-solving (Walsh, 2021). Social-ecological factors such as families’ social and ecological resources are also important parts of family resilience (Fong et al., 2021; Peer & Hillman, 2014).
Purpose of the Study
This mixed-methods study aimed to examine the experiences of parents with children with IDD and extensive support needs related to parental stress and family resilience during the COVID-19 pandemic. We focused on families with elementary-aged children who had complex communication needs (i.e., children who were nonspeaking or who had limited use of speech for communication). Children with complex communication needs often use augmentative and alternative communication (AAC) instead of or alongside speech to communicate, such as picture symbols or speech-generating devices (Beukelman & Light, 2020). Understanding the experiences of this group of families is important. During the pandemic, having a child with complex support needs was associated with families experiencing greater challenges because of the disruption and loss to services (Navas et al., 2022; Spann et al., 2023; Therrien et al., 2022). Additionally, many children with complex communication needs have co-occurring behavior support and/or medical needs, which increase the level of support and care they need (Andzik et al., 2018; Beukelman & Light, 2020).
A mixed-methods approach was especially appropriate for our interest in studying parental stress and family resilience through the lens of ecocultural theory. Qualitatively, we aimed to understand and describe families’ firsthand perspectives about their own resilience and stress. Strengths of the qualitative component included facilitating depth of understanding, allowing for unanticipated findings, and ensuring findings about lived experiences were humanized. Quantitatively, we aimed to pinpoint factors within the family niche that were associated with stronger family outcomes, and we were especially interested in the role of social support. We hypothesized that (a) parent satisfaction with social support would predict family resilience and (b) satisfaction with social support and family resilience would each act as unique predictors of lowered parental stress. Therefore, by merging the qualitative and quantitative findings, we aimed to generate mixed-methods meta-inferences (Creswell & Plano Clark, 2018) that could answer our research question with greater depth of understanding than any single method alone. Our research question was: What are families’ experiences related to stress and resilience during the COVID-19 pandemic, and how are these experiences shaped by aspects of the family niche?
Method
This study was part of a larger longitudinal mixed-methods project focused on the experiences of families with elementary-aged children with complex communication needs during the COVID-19 pandemic (Leroux et al., 2024; Spann et al., 2023). For this study, we used a subset of data focused on stress, resilience, and social support. We collected data across three time points during the 2020–2021 school year (fall, winter, spring).
Participants
After receiving Institutional Review Board approval, we recruited families by distributing emails through school districts, service providers, and community disability associations. Recruitment materials directed interested families to complete an electronic interest form, and then potential participants were screened for eligibility by telephone. To participate, families had to reside in Tennessee and have a child with IDD who: (a) received special education services in kindergarten through fourth grade in a public school and (b) had complex communication needs, which was defined as using prelinguistic (e.g., gestures, nonword vocalizations) or early linguistic communication (e.g., single words and/or some short 2–3 word phrases), measured through parent report using the Communication Matrix (Rowland & Fried-Oken, 2010).
A total of 37 families participated (see Table 1). Most were biological mothers (n = 31, 83.8%); five were biological fathers (13.5%) and one was an adoptive mother (2.7%). The majority were White and non-Hispanic (89.2%). Two participants (5.4%) reported speaking both Spanish and English in their homes. Family income ranged (see Table 1); 14 participants (37.8%) reported their child was eligible for free or reduced-price school lunch based on family income. Families resided in suburban (56.8%), rural (29.7%), and urban settings (13.5%).
Characteristics of Parents and Their Children With Complex Communication Needs.
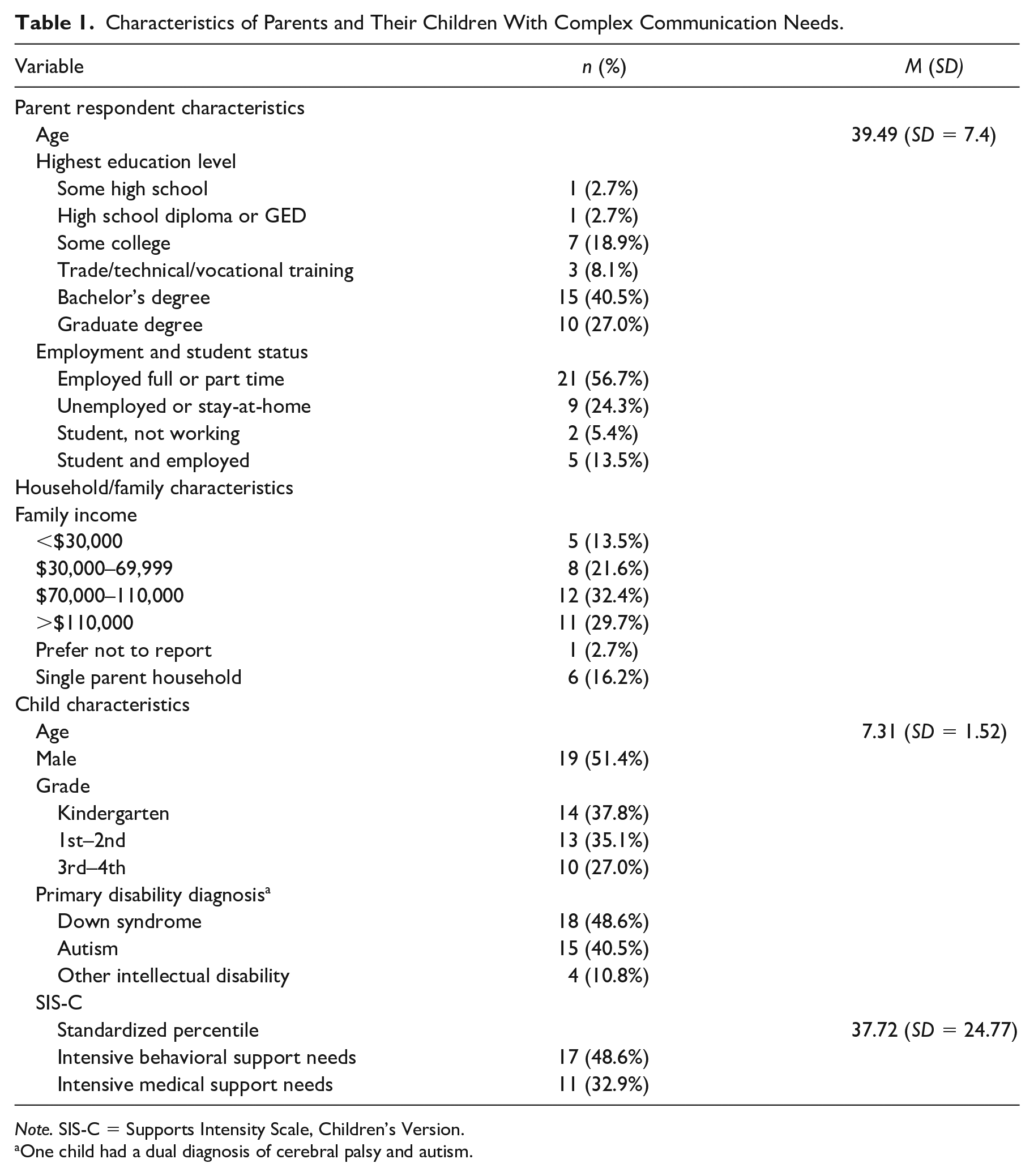
Note. SIS-C = Supports Intensity Scale, Children’s Version.
One child had a dual diagnosis of cerebral palsy and autism.
Children ranged in age from 5;2 (years;months) to 10;1 (M = 7;4). About half were male (51.4%), and most had the medical diagnoses of Down syndrome (48.6%) or autism (37.8%). However, 78.5% of children had multiple diagnoses, which included intellectual disability (48.6%), developmental delay (40.5%), chronic health conditions (27.0%), attention-deficient/hyperactivity disorder (10.8%), visual impairment (2.7%), cerebral palsy (2.7%), hearing impairment (2.7%), apraxia (2.7%), and anxiety/mood disorder (2.7%). All of the children could be classified as having extensive support needs, which we evaluated by having parents complete the Supports Intensity Scale—Children’s Version (SIS-C; Thompson et al., 2014). SIS-C scores are standardized and address the level of support that a child needs relative to other same-age children with IDD. On average, children in the sample had more extensive support needs than 37.7% of other same-age children with IDD (SD = 24.8). Furthermore, nearly half of children had behavioral support needs considered exceptional on the SIS-C (48.6%) and roughly one-third had exceptional medical support needs (32.9%). All children were described by their parents to use prelinguistic communication such as gestures or nonword vocalizations (100%); in addition, parents reported their children communicated through single spoken words (64.8%), short-spoken phrases (45.9%), manual signs (45.9%), and aided AAC (40.5%). Of note, approximately two-thirds of children (64.9%) had access to aided AAC such as a speech-generating device, but not all of these children used it at home.
Because this study took place during the pandemic, children’s educational services changed frequently. We collected data at three time points—Time 1 (September 2020), Time 2 (January 2021), and Time 3 (May 2021). At Time 1, children were divided between attending school in-person (43.2%), virtually (25.1%), and in a hybrid arrangement (21.6%; i.e., combination of in-person and virtual learning). Fewer children attended school in-person at Time 2 (24.2%), with 45.9% in a hybrid arrangement and 29.7% virtual. By the end of the school year (Time 3), more than half were attending school in-person (56.8%); 35.1% were in a hybrid arrangement, and only 8.1% (n = 3) were virtual.
Study Design
We utilized a convergent parallel mixed-methods design (Creswell & Plano Clark, 2018), which involves concurrently conducting qualitative and quantitative methods, weighing the methods equally, analyzing the two components independently, and then integrating results to interpret them together. Figure 1 shows a procedural design diagram for the study. Merging qualitative and quantitative data allowed us to enhance and corroborate our findings while leveraging unique strengths of each method (Fetters et al., 2013). We used quantitative data to examine models predicting stress and resilience, with a specific interest in understanding the role of satisfaction with social support. We used interviews with families across the school year to provide an in-depth understanding of families’ experiences, which helped humanize, contextualize, and interpret the results of the quantitative analysis. Importantly, we attended to Leko and colleagues’ (2023) framework for quality indicators in special education mixed-methods research and to the American Psychological Association’s Journal Article Reporting Standards (JARS) for mixed-methods research (Levitt et al., 2018).
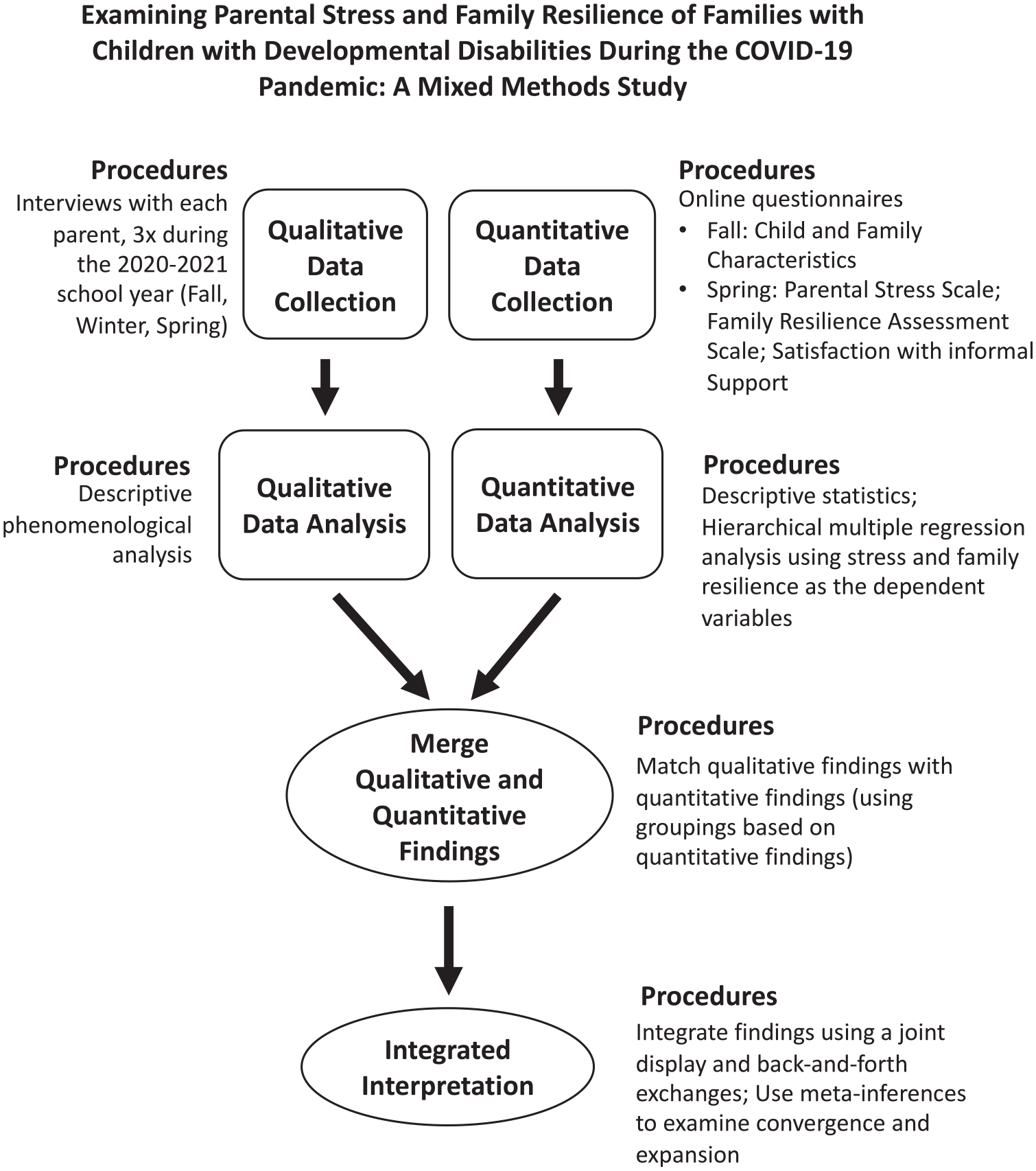
A Procedural Design Diagram for the Convergent Parallel Mixed-Methods Design.
Research Paradigm and Positionality
The three study authors were a White, female special education faculty member and two Asian, female undergraduate students. We operated out of a pragmatic research paradigm, which uses a combination of research methods to conduct practical research with human benefit (Kivunja & Kuyini, 2017). The three researchers had varying experiences with students with complex communication needs and their families, including the first author having served as a special education teacher to elementary-aged students with complex communication needs. The diversity of perspectives and collaboration within our team strengthened opportunities for checking bias through collaboration and critical discussion (Patton, 2015). We as researchers shared some experiences and identities with participants (e.g., all were impacted by the COVID-19 pandemic including the first author who was parenting an elementary-aged child with autism at the time of the pandemic), but we were also outsiders in other ways (i.e., no research team member was a parent of a child with complex communication needs). Because of this, we felt it was important to attempt to relate to families in ways that felt comfortable to them, using strategies such as having participants choose interview times and using a conversational interview style. We also addressed potential researcher bias by using reflexive practices such as critical discussion and memoing throughout all stages of the study (Patton, 2015).
Measures
Dependent Variables
Parental Stress Scale
Parental stress was measured at Time 3 with the Parental Stress Scale (PSS; Berry & Jones, 1995). The PSS is an 18-item self-report measure, which we selected because it specifically addresses stress related to parenting and has strong reliability and validity (Berry & Jones, 1995). Participants used a 5-point rating scale (1 = Strongly disagree to 5 = Strongly agree), and a final sum score was calculated by totaling all scores after reverse scoring appropriate items. Potential sum scores could range from 18 to 90, with lower scores indicating lower levels of parental stress. The scale demonstrated strong reliability within the study sample (Cronbach’s a = 0.89).
Family Resilience Assessment Scale-Autism Spectrum Disorder
Family resilience was measured at Time 3 with the Family Resilience Assessment Scale-Autism Spectrum Disorder (FRAS-ASD; Gardiner et al., 2019) which is an adapted version of the Family Resilience Assessment Scale (Sixbey, 2006). The FRAS-ASD includes three subscales: Family Communication and Problem-Solving, Utilizing Social and Economic Resources, and Family Spirituality; and it has strong reliability and validity (Gardiner et al., 2019). Participants provided ratings on a 4-point scale (1 = Strongly disagree to 4 = Strongly agree). In accordance with scoring guidelines, we calculated mean scores for each subscale and for the overall scale; higher scores reflect higher levels of resilience. The scale had strong reliability within the study sample (Cronbach’s a = 0.92).
Predictor Variables
Child and Family Characteristics
We examined two child and family characteristics: (a) household income (self-report in $10,000 increments from $0 to 9,999 to more than $120,000) and (b) whether a child’s behavioral support needs met the threshold on the SIS-C (Thompson et al., 2014) to be considered exceptional (1 = behavioral support needs, 0 = no).
Satisfaction With Social Support
Satisfaction with social support was measured using the emotional well-being subscale from the Beach Family Quality of Life Scale (Hoffman et al., 2006). Although this subscale is titled emotional well-being, the four statements focus on perceived social support (e.g., “My family has friends or others who provide support”). Importantly, this subscale has been used by several other research groups to assess satisfaction with social support (e.g., Fong et al., 2021). Parents provided ratings using 5-point rating scale (1 = very dissatisfied to 5 = very satisfied). Reliability was strong in our sample (Cronbach’s a = .88).
Semistructured Interviews
Semistructured interviews were conducted on Zoom with each participating parent at each of the three time points. We conducted a total of 115 interviews (two participants did not complete the first interview, and one did not complete the final interview), using semistructured interview guides that were developed by our team for this study through an iterative process involving review of the literature, consideration of the research questions, and piloting work with several families not participating in the study. The interview guide can be accessed through Supplementary Materials posted on the Open Science Framework (OSF): https://osf.io/esbth/?view_only=150c842ca80e4ae1b244acb835f9ed4f.
Four people conducted the interviews—the first author and three research assistants. We assigned each family to one interviewer to (a) build rapport across the school year (Grinyer & Thomas, 2012) and (b) allow for conducting informal member checks by revisiting participant statements from earlier interviews (Motulsky, 2021). Interviews averaged 84 min in length at the first time point (range = 51–119 min), 33 min at the second time point (10–56 min), and 51 min at the third time point (19–81 min). Variability in length was because of the number of questions asked, and sometimes additional data were collected for the larger project. After each interview was conducted, the interviewer completed a written reflection and shared it with other team members, which promoted reflexivity (Patton, 2015).
Quantitative Data Analysis
Preliminary analysis (i.e., examining histograms and Shapiro–Wilks’s tests) determined that each dependent variable was normally distributed. Therefore, we used frequencies, means, and standard deviations as descriptive statistics. We also conducted multiple hierarchical regressions to examine factors associated with stronger family outcomes. Hierarchical regression allowed us to determine if the variable of interest (i.e., satisfaction with social support) explained a significant amount of variance in the dependent variable(s) (i.e., stress, family resilience) after accounting for other variables (i.e., other child- and family-related factors). The correlation matrix in the OSF Supplemental Materials displays bivariate correlations between all variables, which we also used to determine there were not issues of multicollinearity.
Qualitative Data Analysis
Within the qualitative component of the mixed-method design, we relied on thematic analysis based on descriptive phenomenology (Sundler et al., 2019), which aims to explore and describe people’s lived experiences. Specifically, we used Colaizzi’s (1978) method, consisting of four main steps: (a) reading transcripts, (b) extracting significant statements that pertain to the phenomenon of interest (i.e., stress and resilience during the COVID-19 pandemic), (c) formulating meanings for each significant statements, and (d) organizing formulated meanings into clusters and themes.
Interviews were first transcribed verbatim, checked for accuracy, de-identified, and imported into Dedoose (Version 9.0.46) for analysis. After re-reading transcripts, the third author and two research assistants collaboratively identified significant statements that pertained to the research question using structural coding (Saldaña, 2021), which involves labeling and indexing excerpts so they can be further analyzed. The next step was to formulate meanings for each significant statement, which involves re-stating the underlying intent of participant’s statement in a clear, simple way (Colaizzi, 1978). The second and third authors collaboratively wrote the formulated meanings, which supported trustworthiness by using critical dialog to help the researchers set aside their own beliefs and focus on the participants’ views themselves (Sundler et al., 2019). For the final step, the three authors independently read through the formulated meanings to identify themes that grouped ideas based on common patterns, then met to achieve consensus on the themes. Afterwards, the third author conducted a final round of analysis focused on searching for evidence confirming and disconfirming the themes. No significant disconfirming evidence was found (i.e., nothing contradicted the interpretation of the themes), but this analysis step was important for generating analytical memos about each theme that deepened and added nuance to understanding of the themes. The memos were reviewed and edited by the first and second author before analysis was complete.
Mixed-Methods Integration
The quantitative and qualitative results were merged, which involved (a) comparing the results to evaluate how they confirmed and/or expanded one another, and then (b) drawing meta-inferences (i.e., new insights about the research question which can only be gained by the integration of the two sets of data; Creswell & Plano Clark, 2018). We merged the findings through a process of back and forth exchanges (Bazeley, 2012), which involved iteratively relating the qualitative and quantitative findings to one another through memoing, diagramming, and critical conversation. We created multiple versions of joint displays to aid in this integration process, and then we focused on refining the formatting of one of these joint displays to support clear communication of the findings (Guetterman & Fetters, 2022).
Results
Results are presented using a contiguous approach to mixed-methods integration (Fetters et al., 2013), which means we first separately report the findings of each component—qualitative and then quantitative—followed by reporting the integrated findings.
Qualitative Findings
Three themes captured families’ experiences with stress and resilience during the COVID-19 pandemic: (a) Navigating many challenges, (b) Coping and finding support, and (c) Showing resilience. Quotes are attributed to participants using pseudonyms.
Navigating Many Challenges
Families’ stressors encompassed concerns about: (a) their families’ physical health, (b) their families’ social-emotional well-being, and (c) the education and care of their child. Related to their health, many families shared that their worries about COVID-19 were heightened because their children had complex medical needs and were immunocompromised. They also worried about who would care for their child if they got sick themselves. Diana explained: “I can’t be sick . . . I have stuff to do. I have to take care of my child . . . I can’t be sick because I can’t just call in anybody to take care of [my child].” Lockdowns and quarantining were also emotionally challenging for many parents and their children. Some parents described their children as “restless” (Diana), “confused” (Genevieve), and “frustrated” (Matthew), because they would normally “thrive on routine” of going to school, therapy, and other activities. Children often experienced increases in challenging behavior, requiring greater support and patience from their parents—who already felt stretched thin. Hannah explained: Him and I both, we feed off each other a lot. So if he’s having a bad day, it kind of like seeps into me too . . . If I’m having a bad day, it’s like he knows it, too. So he’s grouchy.
Uncertainty compounded families’ stress, particularly with the seemingly constant transitions from virtual to in-person and back to virtual schooling. Emily explained: I think the negative part has just been the uncertainty of everybody’s schedule. What are we doing today? Where in the past, five days a week, everybody’s doing the same thing. You know what to expect, so now the unexpected I think causes a little bit more stress in the family. I feel overwhelmed sometimes that I have more on my plate when they’re home, that I don’t maybe get as much done.
Although families’ experiences varied, many grieved losing out on social support and relationships from people they would usually see in-person such as extended family, friends, and special education support staff. Flora explained how this impacted her daughter: “Not seeing her friends is driving her nuts. Not going to church. We can’t even drive by the church because she, she gets very upset that she can’t go.”
Families’ greatest challenges were often pertaining to their children’s education and care. Many parents felt their child was not getting what they needed from their school, but they also felt they themselves could not necessarily provide what their child needed. Stephanie explained, “I don’t know what to do with [my daughter]. I don’t know how to help [her]. I’m not the teacher—what do you want me to do?” Many (but not all) parents were concerned about their children regressing, particularly when they saw their children and their teachers both struggling with virtual instruction. Some parents described being “completely overwhelmed” and “hopeless” trying to support their children in virtual classes when they were juggling so many other responsibilities (e.g., virtual school for other school-age children, care for younger children, work responsibilities). Constance explained: I was trained to implement ABA [applied behavior analysis] at home. But to do it with a therapist on a computer screen, and have to keep that computer screen in front of me so that the therapist can count is dehumanizing. And if you’ve ever tried to do anything, do one-to-one ABA, and keep an eloping kid from eloping, and then do that in an open floor plan house with three kids with a therapist that wants to count on a computer that your kid keeps closing. It was exhausting and not beneficial.
Some parents had good experiences with their child’s educational team, but many felt unsupported by the schools, explaining that the schools were not providing the individualized education their child needed. Hannah, for example, shared, “I feel like anytime I say something, it’s just brushed under the rug.” Valentina explained: The lack of consideration towards these children in the education system is just beyond what I’ve ever experienced [before the pandemic]. There’s no accommodation at all for them. Everything is for the regular typical child, but anybody who has those needs, like being nonverbal, it’s like, “Tough luck.”
Coping and Finding Support
Families needed to cope. They sometimes described self-care (e.g., exercising, reframing thoughts, making time for oneself), but more often they emphasized how their family supported and helped one another through their relationships and connectedness: communicating and listening, sharing in problem-solving, and creating new rhythms that allowed them to spend enjoyable time together as a family. Sherry explained: “not to say we didn’t have bumpy days. . . . [But] we’ve been able to manage it. I don’t know that there was any owner’s manual for that. We just made sure we talked things out.” Megan explained: I think that it was a time where our family unit just grew stronger, you know really through everything, really. Being unsure of what was to come and just holding onto each other. And then the time spent together and getting back down to basics, doing a lot more cooking and just spending time together.
Some families felt isolated in facing their challenges, but many families were able to maintain or build new relationships (e.g., extended family, other parents of children with disabilities, friends, people from their faith communities). Kylie explained: Being together [as a family] so much has been good and bad. And we also need [other] relationships. I guess finding ways to stay connected to relationships outside of my family has helped my family be resilient.
Conversely, Mia lacked support from her family members: I don’t have any family that can help me with her. . . . And we used to, we could take her over to mom’s so we can clean house or do stuff around the house without having to worry about her. I don’t have that support now; we can’t take her over there. So it’s just a lot. It’s stressful because I don’t have that help. . . . It’s just more 24/7 with her. It’s hard.
Families also varied in whether they felt supported by their children’s teachers and service providers. Matthew explained: “We’re frustrated at that school because it feels as though his special education teacher has just pretty much given up.” Matthew and other families described feeling they were constantly “fighting” with the school but still not getting what their child needed. Conversely, Olivia talked about how her relationship with her daughter’s special education teacher was strengthened. She explained: “I feel I can call her anytime of the day or night, and just have a conversation or cry or just show her a great picture of [child] doing a puzzle. So that’s been great.” Audrey also felt deeply supported by her child’s educational team: Her teachers, her therapist, her paraeducators, even the learning center she goes to after school are great. Everyone is just all amazed at her progress. And I’m amazed at the whole team effort to get her where she is . . . I think we’ve just all worked together to get her where she is today.
Showing Resilience
When asked about what resilience means to them in the context of their family, parents explained that resilience was not something they just had, but rather something they worked for: “not giving up” (Madilyn), “pushing forth through the times” (Molly), “overcoming challenges” (Ryan), “adapting” (Todd), doing what “needs to be done” (Shelby), and “not letting hard things keep us stuck” (Kylie). Audrey explained: We got to keep moving. We power through, we get through and we power through with the mentality that things are going to be kind of okay. We’re going to work through anything that’s kind of just thrown our way, to make sure that [our child] succeeds, that her brother succeeds, that we succeed as a family together.
One of the things that families emphasized most was working to find family rhythms and routines. Several families described this process of adapting as being intertwined with finding out what was really important to them as a family. Jordyn explained: When you are in a tough season and there’s a necessity for resilience, [it’s about] your ability to be aligned as a family unit. “Here is what’s important to us right now. Here’s what we’re just going to let go of.”
For many families, what was really important was “togetherness” (Katie). Many families described their “together” routines as being an important part of supporting their well-being as a family: “spending more time with one another” (Shelby), “having dinner together” (Rianna), “sharing more in responsibilities” (Kayla), and “playing together” (Audrey). Shelby explained that having a child with a disability had already taught their family to slow down, but the pandemic “taught [them] to slow down even more.” Genevieve described the good things that came for their family from this process of adapting together and finding new routines: We have just spent, obviously, so much time together that we’ve been able to see our kids’ relationships change and blossom. We’ve been outside so much and we’ve been swimming all the time and just having family adventures. So, I feel like our quality time as a family really improved because of the pandemic. So, it’s been a blessing for our family, I feel like.
Another aspect of resilience that many families mentioned related to resilience was the “good side” (Audrey) of having to advocate more for, and be more involved in, their child’s educational supports. This “good side” (for some families, when they felt supported by their child’s educational team) was that they felt more empowered as an advocate and to support their child’s learning at home. Audrey explained how her feelings of empowerment grew: I feel more confident, being able to support her. . . better, [and being] a better parent and teacher through this which is kind of crazy. . . being pushed into a situation that I don’t really have much control of having to do it. And being okay with having to do it. I think was huge. So my confidence level has grown tremendously.
Quantitative Findings
Family Resilience
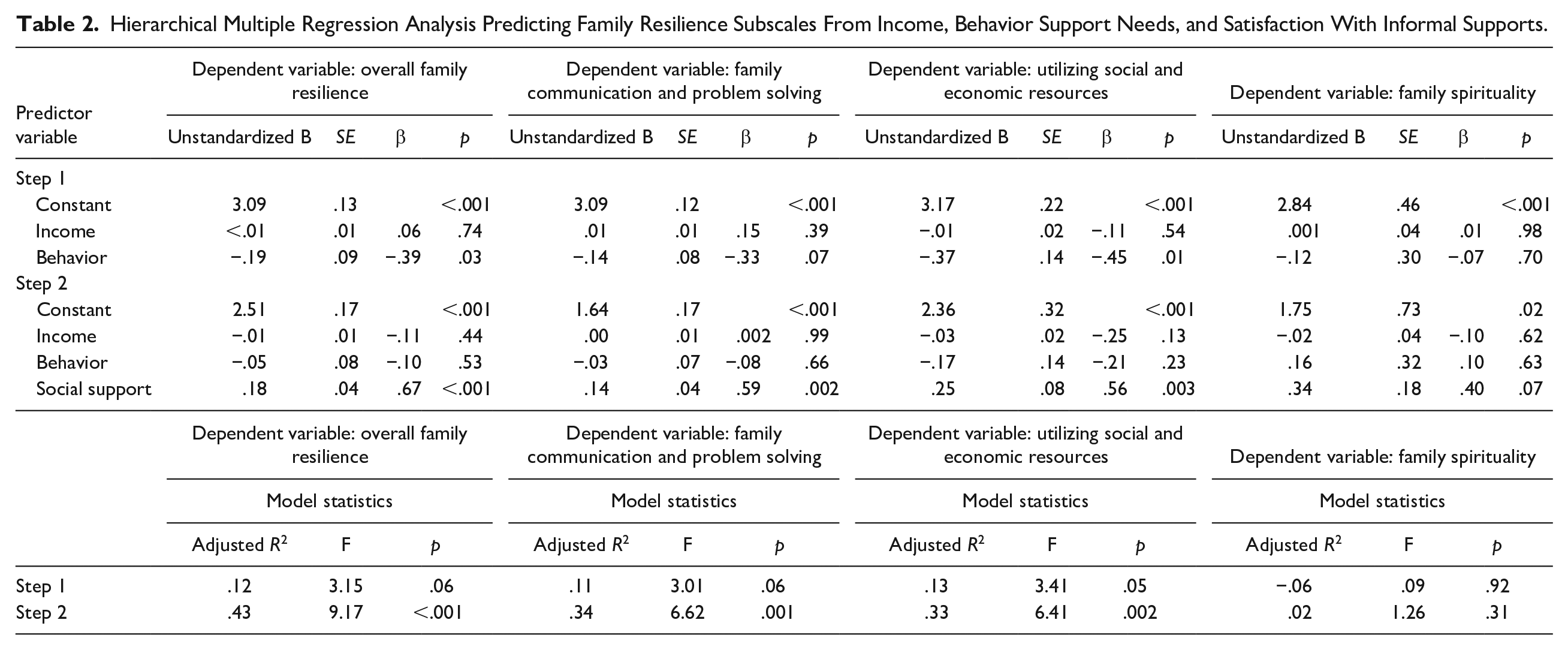
FRAS-ASD results are shown in the Supplementary Materials on OSF. Of the three subscales, parents’ ratings were highest for Family Communication and Problem-Solving (M = 3.09, SD = 0.22), such as for items like “The things we do for each other makes us feel a part of the family” (M = 3.33, SD = 0.48) and “We show love and affection for family members” (M = 3.33, SD = 1.14). Ratings for Utilizing Social and Economic Resources were slightly lower (M = 2.84, SD = 0.44), followed by Family Spirituality (M = 2.75, SD = 0.80). Of note, these two subscales (i.e., Utilizing Social and Economic Resources, Family Spirituality) also showed greater variability in the sample compared to Family Communication and Problem-Solving.
Table 2 summarizes results from hierarchical regression models for overall resilience and each subscale. The first step of the hierarchical regression included family income and the presence of exceptional behavioral support needs for the child as control variables. For overall regression, this model accounted for only 12% of the variance (F [2, 31] = 3.15, p = .06). Behavior support needs significantly and negatively predicted family resilience (p = .03), but income was not a significant predictor (p = .74). The second step of the hierarchical regression involved adding satisfaction with social support, which led to an improved model (adjusted R2 = .43; F [3, 30] = 9.17, p = < .001). Neither income nor behavior support needs predicted family resilience in this improved model, but satisfaction with social support was a strong, positive predictor (p < .001, β = .67). As shown in Table 2, social support was a significant, positive predictor of the Family Communication and Problem-Solving subscale (p = .002; β = .59) and Utilizing Social and Economic Resources (p = .003; β = .56), but not Family Spirituality.
Hierarchical Multiple Regression Analysis Predicting Family Resilience Subscales From Income, Behavior Support Needs, and Satisfaction With Informal Supports.
Parental Stress
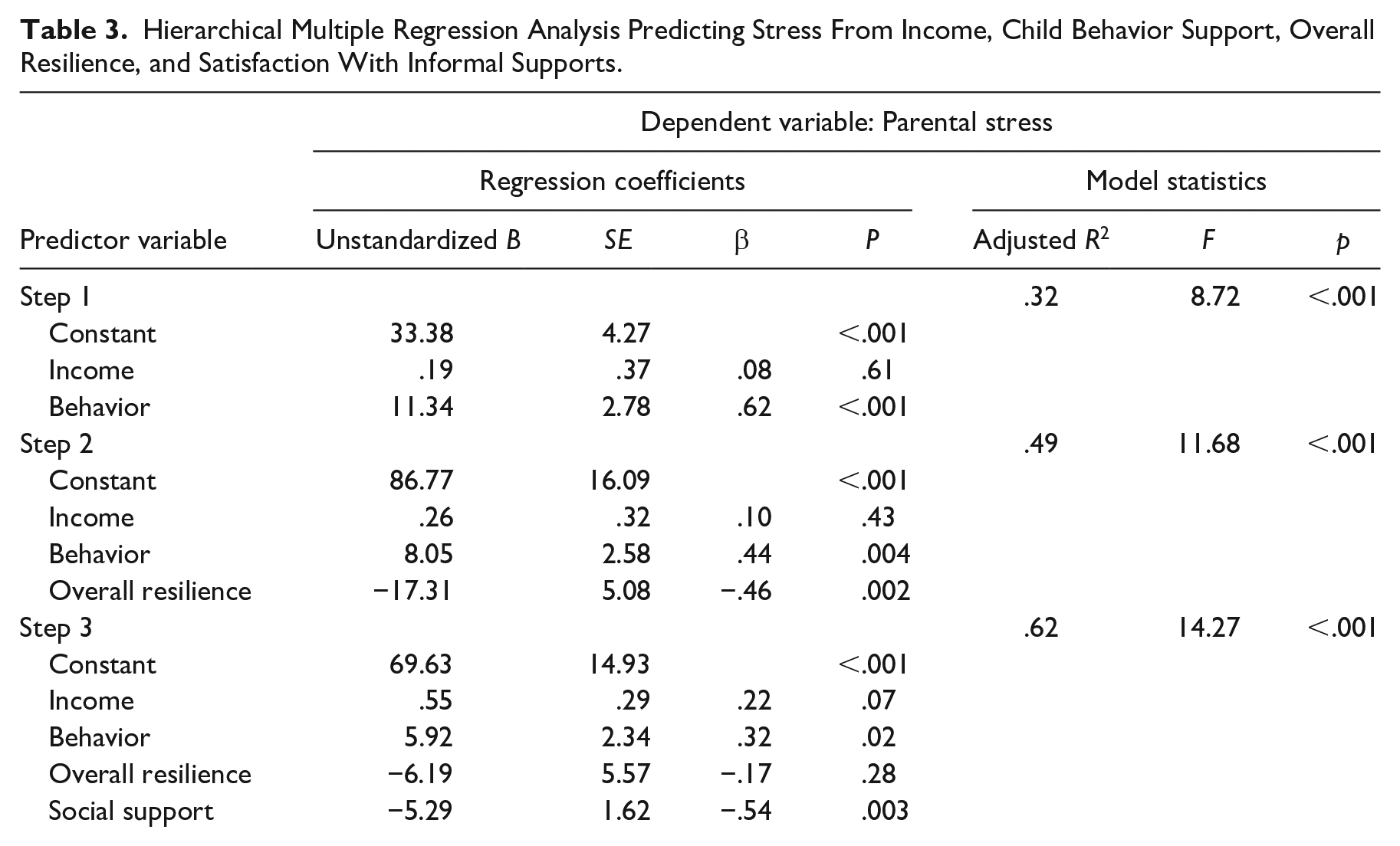
Results of the PSS are shown in the Supplementary Materials posted on OSF. Parental stress ratings were moderate but variable across the sample and across items on the scale. Parents reported the highest stress levels on items related to feeling they had to give more energy than they had to care for their child, and worrying about whether these efforts were enough (i.e., “I sometimes worry whether I am doing enough for my child” [M = 4.17, SD = .74]; “Caring for my child sometimes takes more energy than I have to give” [M = 3.58, SD = .94]).
Table 3 summarizes the results of the hierarchical regression model for parental stress. The first step of the hierarchical regression included the control variables of family income and behavioral support needs, which together accounted for 32% of the variance in parental stress (F [2, 31] = 8.72, p = < .001). Having a child with exceptional behavioral support needs was a significant predictor (p < .001; β = .62), but income was not. In the second step, we added overall family resilience as a predictor, which accounted for an additional 17% of variance (adjusted R2 = .49; F [3, 30] = 11.68, p = < .001). Exceptional behavioral support needs still significantly predicted higher stress (p = .004; β = .44), and resilience predicted lower stress (p = .002; β = −.46). In the final step, we added satisfaction with social support to explore whether resilience and social support were unique predictors. The fit of the model was improved (F [4, 29] = 14.27, p = < .001; adjusted R2 = .62). Exceptional behavioral support needs still significantly predicted higher stress (p = .02; β = .32) and satisfaction with social support significantly predicted lower stress (p = .003; β = −.54), but resilience was no longer a unique, significant predictor (p = .28).
Hierarchical Multiple Regression Analysis Predicting Stress From Income, Child Behavior Support, Overall Resilience, and Satisfaction With Informal Supports.
Integrated Findings
The results of the merged quantitative and qualitative analysis are presented in a joint display on Table 4. We arranged quantitative and qualitative data side by side by grouping participants into three roughly quartile-based groups using parents’ social support ratings (i.e., average of the four ratings on the 5-point rating scale): high satisfaction (roughly the top 25%, n = 13), middle satisfaction (middle 50%, n = 14), and low satisfaction (bottom 25%, n = 9). These divisions created meaningfully different groups based on satisfaction with social support, as demonstrated by the standard deviations within each group being small while differences in mean values across the groups were large (greater than one point difference; see Table 4).
Joint Display of Merged Quantitative and Qualitative Data About Families’ Experiences With Stress and Resilience During the COVID-19 Pandemic.
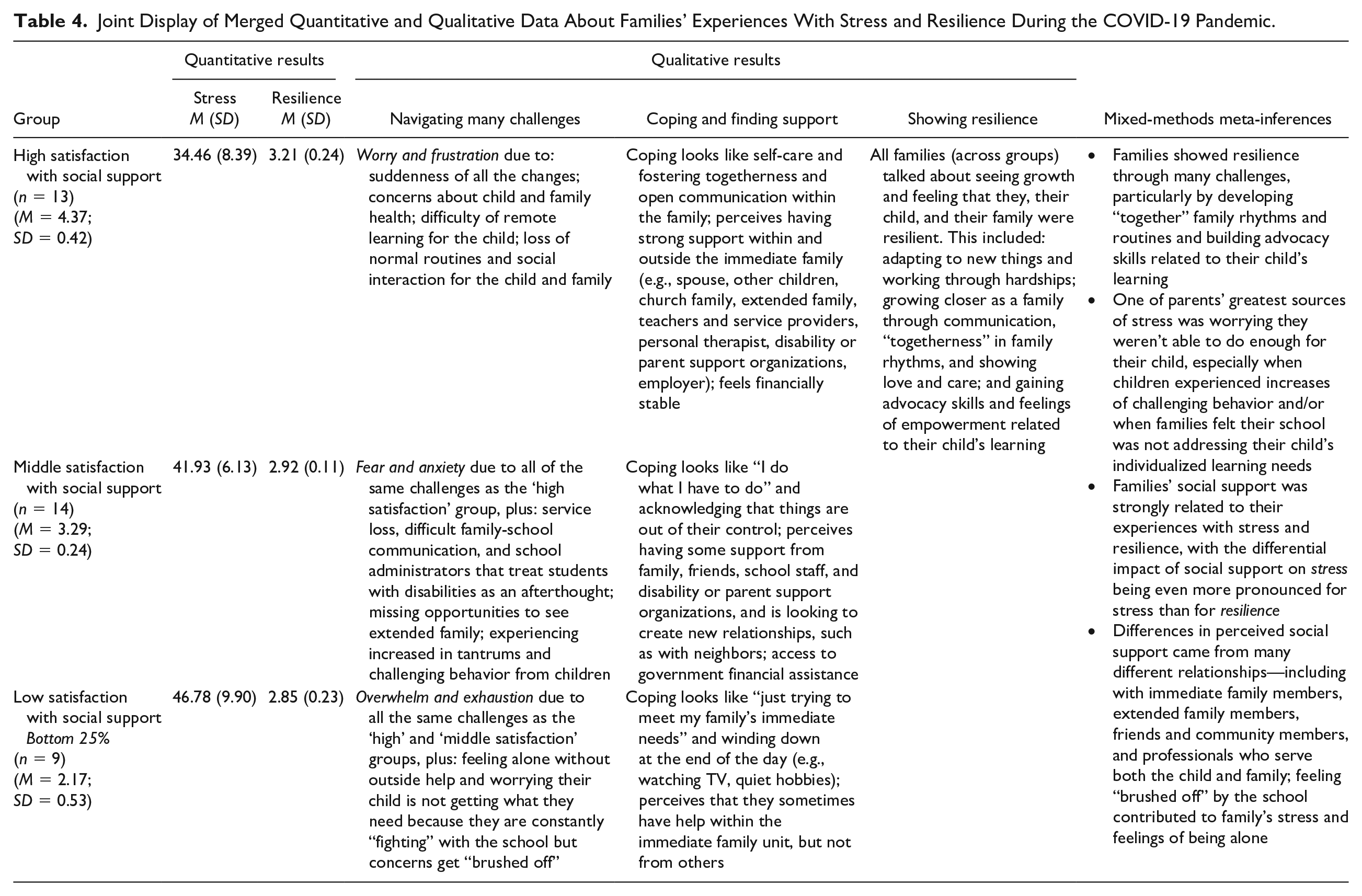
Based on the integrated findings, qualitative and quantitative findings converged related to stress and social support, revealing that parental stress grew from resembling worry and frustration (in the group highly satisfied with their social support), to fear and anxiety (middle satisfaction), to feeling entirely overwhelmed and exhausted (low satisfaction). Qualitative findings further expanded the quantitative findings by revealing that for the parents who were the least satisfied with their social support, the biggest source of stress was how poorly they felt supported by educators and service providers at their child’s school. These parents described “fighting” with the school, but still feeling “brushed off” by teachers, service providers, and administrators. Conversely, parents in the high satisfaction group described teachers and service providers among the people in their lives who offered them support.
Related to resilience, quantitative and qualitative findings converged to demonstrate the role of social support in increasing family resilience. Qualitative findings expanded understanding by illustrating what this resilience actually looked like: families created rhythms and routines within their family niche that fostered communication and togetherness. One of the products of resilience for some families involved growing in their empowerment and advocacy, particularly when they felt supported by their child’s educational team at school.
Discussion
The COVID-19 pandemic disrupted daily routines and provided challenges for all families, but parenting a child with complex communication needs could be especially difficult because of the service loss and change and resulting impact on children and families (Spann et al., 2023; Therrien et al., 2022). We aimed to understand family experiences with stress and resilience and were especially interested in how aspects of the family niche shaped family outcomes during the pandemic (Gallimore et al., 1989; McConnell et al., 2015). Our findings extend prior knowledge in several ways, offering important implications for practice and illustrating the value of mixed-methods research to learn about the lived experiences of children with IDD and their families.
First, our findings indicated that, as a group, families reported a moderate level of parental stress, but this varied widely across the sample. Parental stress was the highest related to (a) worrying they were not doing enough for their children and (b) feeling that caring for their children took more energy than they had to give. Importantly, parents who reported the highest levels of parental stress felt the least satisfied with their social support network. Social support within and outside of the family minimized parental stress, but not all families benefited from this protective factor. Although some families felt well-supported by their family, friends, and community (e.g., church family)—and by professionals such as their child’s teachers and service providers—many other families felt alone and exhausted. Although previous research has demonstrated the role of social support to promote family flourishing and to mitigate things like parental stress (Drogomyretska et al., 2020; Robinson & Weiss, 2020), this research has not focused specifically on children with complex communication needs or examined these issues within the context of the COVID-19 pandemic.
Second, our findings add in novel ways to previous research examining how parenting a child with challenging behaviors might be associated with increased parental stress (Burke & Hodapp, 2014; Lievore et al., 2023; Rivard et al., 2014). We found not only that children’s behavioral support needs predicted increased parental stress, but also that parents of children with extensive behavioral support needs reported being less satisfied with their social support networks— as demonstrated by the moderate negative correlation between these two factors (see the correlation matrix within the OSF Supplementary Materials) and that the strength of the relation between behavioral support needs and parental stress decreased when social support was added to the model (see Table 3). Therefore, our findings suggest children’s behavioral challenges may relate to parental stress by impacting how parents access and perceive their family’s social support. Our study did not have a large-enough sample to explore whether social support acts as a mediator between children’s behavioral challenges and parental stress, but it will be important for future researchers to investigate intricate relations between social-ecological factors and child characteristics (McConnell & Savage, 2015). Although future research is needed, our findings suggest that families of children with extensive behavioral support needs may find it harder to have the social support they need to flourish, not just from their informal social networks, but also from professionals.
Third, findings provide important insight into family resilience as an aspect of the family niche. Families shared stories about how they adapted to the challenges and uncertainty of the pandemic by creating rhythms and routines that fostered communication and togetherness. Importantly, these routines often brought forth positive outcomes, and many parents described feeling more confident to tackle hardships, more empowered to advocate for their children, and more connected as a family. Yet, these experiences were not consistent across families. Like previous researchers who have studied family resilience in other groups of families and in contexts outside the pandemic (e.g., Beighton & Wills, 2019; Fong et al., 2021; Peer & Hillman, 2014), we found that parents’ satisfaction social support influenced family outcomes not only by being associated with lower stress, but also by being associated with increased resilience.
Finally, we strengthened the insight gained in this study by using a mixed-methods approach. Although both quantitative and qualitative findings independently provided unique insight into families’ experiences with stress and experience, only by integrating these results did we discover that the biggest difference for families who felt more satisfied with their social support was feeling supported by their child’s teachers and service providers. Families with quantitatively lower stress and higher social support satisfaction talked at length about their relationships with their children’s teachers and service providers, describing them as “great listeners,” “a sounding board,” “always encouraging,” and “my go-to person.” Conversely, for the families who were dissatisfied with their social support, everything with the school felt like a “fight.” Educators and service providers should be important members of families’ support networks, but for some of these families, these professionals were actually part of the problem; they became one of the stressors. In previous literature, Burke and Hodapp (2014) found that family-school partnerships, specifically strong partnerships (rather than poor or even adequate partnerships) seemed to lessen levels of maternal stress for children with IDD. This study builds on this previous work in important ways by (a) offering firsthand accounts from families of their experiences working with and relating to their child’s providers during a unique time, and (b) illustrating the valued role that mixed-methods research can serve in investigating family outcomes like stress and resilience.
Limitations
This study had limitations that are important to consider when interpreting results. First, we aimed to describe the experiences of a fairly small group of families in a single state. The value of this approach was that it allowed us to conduct repeated, in-depth interviews that were crucial for humanizing, contextualizing, and meaningfully interpreting the results of the quantitative analysis. But, such a small sample from within a single geographic region means the findings should not be assumed to generalize to the larger population. Beyond this, another concern is that the sample over-represented White, middle- and upper-class families who were monolingual English-speaking thus underrepresenting families from diverse racial/ethnic, linguistic, and socioeconomic backgrounds. We attempted to utilize strategies to recruit a diverse sample, including by targeting school districts with diverse student populations for recruitment, reducing the time required for participation whenever possible, and offering financial compensation. However, these efforts still did not yield the diverse sample we aimed to have. Increasing sample diversity in the future is critical so that researchers can address how the experiences of families from historically marginalized groups—including related to race, ethnicity, linguistic diversity, and socio-economic status—may align or differ from the experiences of the families in this study. Previous research has shown how barriers to accessing educational, health, and other services often lead to poorer outcomes for children and families from marginalized backgrounds compared to their White, middle- and upper-class counterparts (Harrington & Kang, 2008). In addition, researchers should consider how cultural differences may play a role in experiences related to family stress and resilience (e.g., disability stigma and perceptions of disability, cultures that may be more individualistic or more collectivistic; e.g., Babik & Gardner, 2021). Finally, although we strengthened the qualitative component of the mixed-methods design by using repeated interviews, this study is not longitudinal because we did not focus on analyzing changing patterns over time.
Implications for Practice
Families’ mental health and well-being should be considered a core aspect of supporting children with IDD, including children with complex communication needs. Attention on families, and their flourishing, is clearly needed during crisis situations like the COVID-19 pandemic, but it should not be limited only to unprecedented times. Special education law through the Individuals with Disabilities Education Improvement Act (IDEA) has long-emphasized the importance of family-school partnerships, but IDEA has tended to almost exclusively focus on the importance of family-school partnerships for student outcomes, not for parents or families themselves (Burke & Hodapp, 2014). The findings of this study underscore that teachers and service providers can either mitigate or increase parental stress for the families of the children they serve. Strong partnerships with teachers and service providers—the kind in which parents described professionals as being “always encouraging,” and “my go-to person”—decreased parental stress and supported family resilience. Conversely, other parents perceived their children’s teachers, service providers, and school administrators as being significant sources of parenting stress. These parents knew their children were not getting what they needed, and they felt disrespected, overlooked, and dismissed when they attempted to advocate.
Family-centered partnerships are multidimensional. For instance, family-professional partnerships include how families perceive communication and trust both in how the teacher or provider (a) works with and supports the child directly and (b) supports the family at large (Summers et al., 2005). Findings from this study demonstrated the importance of both of these dimensions. With all the challenges that the COVID-19 pandemic brought, parental stress was minimized and family resilience was bolstered when parents perceived that their child was getting what they needed from their educational team, and when parents perceived that their child’s teachers and service providers were there to support them as a family. Therefore, teachers and service providers need to recognize the power they have to influence not just child outcomes, but also whole-family outcomes. Family–school partnerships matter deeply, not just during unprecedented times, but always.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was made possible by a special COVID-19 grant from the Spencer Foundation (#202100017).
Editor-in-Charge: Esther Lindström