
Abstract
22q11.2 deletion syndrome is a rare multisystem genetic disorder with over 200 associated characteristics, occurring in various combinations and severity. Extensive biomedical research has been undertaken on 22q11.2 deletion syndrome, however, there is a dearth of research on families’ experiences of managing a family member with this condition. The complex and at times serious phenotypical presentation of the syndrome can make the management of the condition difficult for families. The aim of this mixed method explanatory sequential study was to investigate family hardiness as a resilience factor for adaptation in families of children with 22q11.2 deletion syndrome from parents’ perspectives. We found that adaptation scores increased by 0.57 points (95% CI: 0.19–0.94) for every one-point increase in family hardiness score. Qualitative results indicated that acceptance of the child’s diagnosis and support positively influenced hardiness whereas fears about the future and their experiences of loss negatively influenced hardiness.
Background
22q11.2 deletion syndrome is a multisystem genetic disorder associated with chromosome 22q11.2 interstitial deletions (Bassett et al. 2005). The syndrome is associated with more than 200 characteristics which can occur in various combinations and severity (Michaelovsky et al. 2012). The worldwide incidence of 22q11.2 deletion syndrome has been estimated to be 1 in 2,000 live births (Blagojevic et al., 2021). The phenotype of the syndrome and its symptoms vary widely from person to person. It is a complex disorder that can affect every system in the body and in most severe cases can be life threatening (Swillen and McDonald-McGinn, 2015). As clinical problems evolve over time, clinical management of the syndrome may require input from a range of specialists such as cardiologists, immunologists, endocrinologists and others. Some specialists may not have a full understanding of the complexity of the disorder which has a rare disease status (Palmer et al., 2018; Rizzo et al., 2020), thereby presenting challenges for the early detection, recognition, and medical management of 22q11.2 deletion syndrome (Genetic and Rare Diseases Information Centre, 2023).
Families, particularly parents of children with rare diseases can experience unique challenges (Pelentsov et al. 2016). Challenges may include lengthy delays in obtaining a diagnosis (Black et al. 2015), difficulty in sourcing information about the condition and identifying experienced health specialists with knowledge of the condition (Pelentsov et al. 2016). Parents have also reported experiencing no clear pathway of care and experiencing difficulties in accessing appropriate care (Pelentsov et al. 2016; Rizzo et al., 2020).
As a condition, 22q11.2 deletion syndrome has been the focus of a vast body of biomedical research in recent years (e.g. Martin et al. 2014; Gul et al., 2015; Fleming et al. 2021; Zhang et al., 2021). Recent research that has investigated experiences of people with the syndrome and/or their families has focused on daily life stress for people with 22q11.2 deletion syndrome (Schneider et al., 2020), the impact of COVID-19 on worry and medical disruptions (White et al., 2022), and resilience and quality of life of young adults with the syndrome (Van de Woestyne et al., 2021). However, there is little research to date documenting their experiences of resilience or adaptation. The complex and at times serious phenotypical presentation of the syndrome can make the management of the condition difficult for families. When a person is faced with adversity, it is inevitable that adversity extends to the family unit. Hence, there is a need to consider family resilience.
Theoretical Framework
The theoretical framework used to guide this study was the Resiliency Model of Family, Stress, Adjustment and Adaptation (from herein; the Resiliency Model) (McCubbin et al., 1996). Previous researchers who have examined family resilience have used the Resiliency Model e.g. families who have a family member with autism (Greeff and van der Walt, 2010), mental illness (Jonker and Greeff, 2009), physical disability (Greeff et al., 2012), mental illness (Puasiri et al., 2011) and Down syndrome (Caples et al. 2018). Family resilience is described as a multilevel process of interaction between families and other systems in challenging environments that help a family’s capacity to cope with adversity over time (Ungar, 2016). The Resiliency Model asserts that family resources can be called upon to meet the demands families face during crisis or adverse situations. One such resource is family hardiness, which has been identified as a protective factor and an adaptation resource that focuses on the internal strengths and durability of the family unit.
According to McCubbin et al. (1996), family hardiness can be seen as a buffer in alleviating the negative effects of both stressors and demands. Family hardiness as a resilience resource associated with family adaptation has been studied in the past with various population groups including people with schizophrenia (Bishop and Greeff, 2015; Hsaio and Tsai, 2014), autism (Greeff and van der Walt, 2010), physical disabilities (Greeff et al., 2012) and developmental disabilities (Greeff and Nolting 2013). This research has found family hardiness to be a vital indicator of strength and resistance resources that families draw on to lessen the effects of demands and a key element that facilitates both individual and family adaptation. Although family hardiness has been researched across a range of complex conditions, there remains little research on the experiences of parents and families of children with 22q11.2 deletion syndrome.
According to Ungar (2011), there is a need for an understanding of resilience from multiple contexts and realities and recommended mixed methods research drawing on both qualitative and qualitative methods. McCubbin et al. (1996) recognised that whilst their model adopts a quantitative approach to resilience, it does not preclude the use of qualitative data to complement quantitative findings. Given that family hardiness is an important family resilience resource that influences family adaptation, the aim of this study was to investigate the relationship between family hardiness and adaptation for families of children with 22q11.2 deletion syndrome using a mixed methods approach to inquiry.
Method
Research design
This study was conducted using a mixed method explanatory sequential design comprising two phases (Creswell and Plano-Clark, 2018) underpinned by pragmatism as the philosophical worldview of choice (Mackenzie and Knipe, 2006). The search for practical answers is a major characteristic of pragmatism (Teddlie and Tashakkori, 2009). Pragmatism gives researchers a middle ground both philosophically and methodologically and is an outcome-oriented method of inquiry (Burke Johnson and Onwuegbuzie, 2004). Guba and Lincoln (1988) argue that differing research designs are not compatible. However, Howe (1988) suggested different research methods should be viewed as being “compatible” and the mixing of both qualitative and quantitative methods should be seen as a good thing and the combination of methods should not only be encouraged but should also be required. Such an approach, consistent with the explanatory sequential design used in this study, can provide an in-depth understanding of the research problem, and an explanation of findings from one method to another; each approach offsetting the weaknesses of the other (Creswell and Plano Clark, 2018). Therefore, mixed methods research can help to answer research questions more comprehensively than one method alone (Creswell and Plano Clark, 2011). Hence a mixed methods design was chosen for this study.
Using a mixed methods approach, quantitative and qualitative data were collected sequentially, with quantitative data collection being the first phase taking priority. A connecting data approach was used which involved the collection and analysis of the quantitative data and then using the results to inform 1) the qualitative second phase of the study, 2) the development of the qualitative interview schedule and 3) the identification of research participants for the qualitative phase. Additionally, at the interpretation and reporting level, a segregated approach was used whereby quantitative and qualitative findings were reported separately and integration between the components takes place through the discussion section (O’Cathain, 2009; Leech and Onwuegbuzie, 2009).
Prior to the commencement of the study, ethical approval was sought and gained for both phases of the study from the Social Research Ethics Committee, University College Cork (ref: 2016-080).
Participants and Sampling
The target population for this study was families of children who had a diagnosis of 22q11.2 deletion syndrome and were living in Ireland. For the quantitative phase, non-probability convenience sampling was used to recruit families from the 22q11 Ireland support group (n=141). One questionnaire was administered to each participating family with the invitation for it to completed on behalf of the family. Survey respondents were given the opportunity to indicate if they were willing to participate in an individual interview. Participants from the quantitative phase who indicated they were willing to participate in an individual interview (n=59) became the sampling frame for the qualitative phase. In the qualitative phase, maximum variation sampling was used to achieve heterogeneity of the sample and to highlight different perspectives of the phenomenon being explored, thus providing a more complex picture of the phenomenon (Creswell and Plano Clark, 2011).
Participants (n=9) selected from the sampling frame were contacted by telephone to enquire if they were still willing to be interviewed and were informed of the purpose of the interview, the topics to be discussed and the processes involved. A letter confirming the date and time of the interview and an information leaflet was sent to each participant providing further detail on the qualitative phase of the study. Individual face-to-face interviews were scheduled at times and locations convenient to each participant and they ranged in duration from sixty to seventy-five minutes. The interviewer, the lead author, received informed consent from each participant prior to the commencement of each interview.
Quantitative Data Collection
The first phase of this study was quantitative using a postal cross-sectional survey. A research pack was sent to all families (n=141) of the 22q11 Ireland Support Group with the support of the Group’s chairperson. A detailed information leaflet and a prepaid envelope to return the questionnaire was included in the research pack. Two reminder emails were sent (via the Chairperson) at two separate time points.
Measures
This paper reports on the results of a subset of data from a larger study. In the larger study, 16 scales were used to operationally measure adaptation and resilience variables. These included (i) a demographic questionnaire, (ii) the FIRA-G which has 7 subscales namely: Family Stressors Index, Family Strains Index, Relative and Friend Support Index, Social Support Index, Family Coping-Coherence Index, Family Hardiness Index and the Family Distress Index, (iii) Family Problem Solving Communication Index, (iv) Family Member Well-Being Index, and (v) Family Management Measure. In this paper, the results relating to family hardiness and adaptation are presented.
In this study the measure used to measure family hardiness was the Family Hardiness Index (McCubbin et al., 1987). This scale measures the characteristic of hardiness as a stress resistance and adaptation resource in families, which would function as a buffer in mitigating the effects of stressors and demands. The Family Hardiness Index is a 20-item scale that measures commitment, challenge and control and reflects a “we” rather than “I” orientation. The scale has a possible range of 0 to 60 based on the degree to which each statement within the scale describes their current family situation. A higher score reflects higher family hardiness. The internal reliability Cronbach’s alpha for the Family Hardiness Index is reported as 0.82. When tested the Cronbach’s alpha for this study was 0.81.
The scale used to measure family adaptation was the Family Member Well-being Index (McCubbin and Patterson, 1982). This 8-item scale was developed to measure the degree to which a family member is adjusted in terms of concern about health, tension, energy, cheerfulness, fear, anger, sadness and general concern. Internal reliability Cronbach’s alpha of the Family Member Well-Being Index is reported as 0.85. When tested the Cronbach’s alpha for this study was 0.80.
Qualitative Data Collection
For the qualitative phase of the study, semi-structured individual interviews (n=9) were conducted at times and locations convenient to each participant, ranging in duration from sixty to seventy-five minutes. Informed consent was received from each participant prior to the commencement of each interview Interviews were audio-recorded and transcribed verbatim. Following quantitative data analysis, a semi-structured interview guide was developed based on statistically significant findings from the quantitative phase of the study, in keeping with a connecting data approach as part of an explanatory sequential design (Liem, 2018). Questions were designed to be clear, easy to understand and open ended. The interview schedule of questions followed the same sequence for each participant, although with flexibility to allow participants share their experiences in terms of what was important to them. The researcher (MC) used probing questions for elaboration, and/or explore new issues that arose. The participants were asked the following questions: • I have found that family hardiness is something that has an effect on family well-being. [families who felt they were hardy actually experienced better well-being. So, if you were strong and tolerant of difficult situations your well-being was better]. So firstly I want to ask you what is your understanding of what hardiness is? • Is there anything that you find has a positive effect on your hardiness? • Is there anything that you find has a negative effect on your hardiness? • Have you become more or less hardy over time?
Data Analyses
Survey data were analysed using statistics package SPSS, version 18. Quantitative data analyses involved the use of both descriptive and inferential statistics. Descriptive statistics were then used to describe, compare and summarise data. Bivariate and multivariate analysis was undertaken in the larger study to investigate the relationships between the variables. Stepwise linear regression was also performed in the data analysis of the larger study to determine which combination of independent variables best explained adaptation.
For the qualitative data analysis, a deductive content analysis approach was used guided by Elo and Kyngäs (2008). For this study, the transcribed texts were analysed deductively. Initially, transcripts were read several times to become familiar with the content and to develop a sense of each transcript. Following this, manual coding of the data was undertaken using a content analysis matrix that was developed using the statistically significant findings from the quantitative phase. Using these content areas, subcategories were created within the matrix and codes were applied to the transcripts, with segments of data being selected to represent these codes. Each content area was coded for subcategories. For example, subcategories for the content area family hardiness were factors that positively influenced family hardiness and factors that negatively influenced family hardiness. This process was repeated for each transcript and similarities and differences across the data were sought (Holloway and Wheeler, 2010). The researchers met during the coding process to establish inter-rater reliability in the identification of categories and sub-categories. To increase the trustworthiness of the data, transcript citations were provided to identify where and how the categories were formulated (Elo et al., 2014).
Results
Survey
Characteristics of respondents, n = 64.*
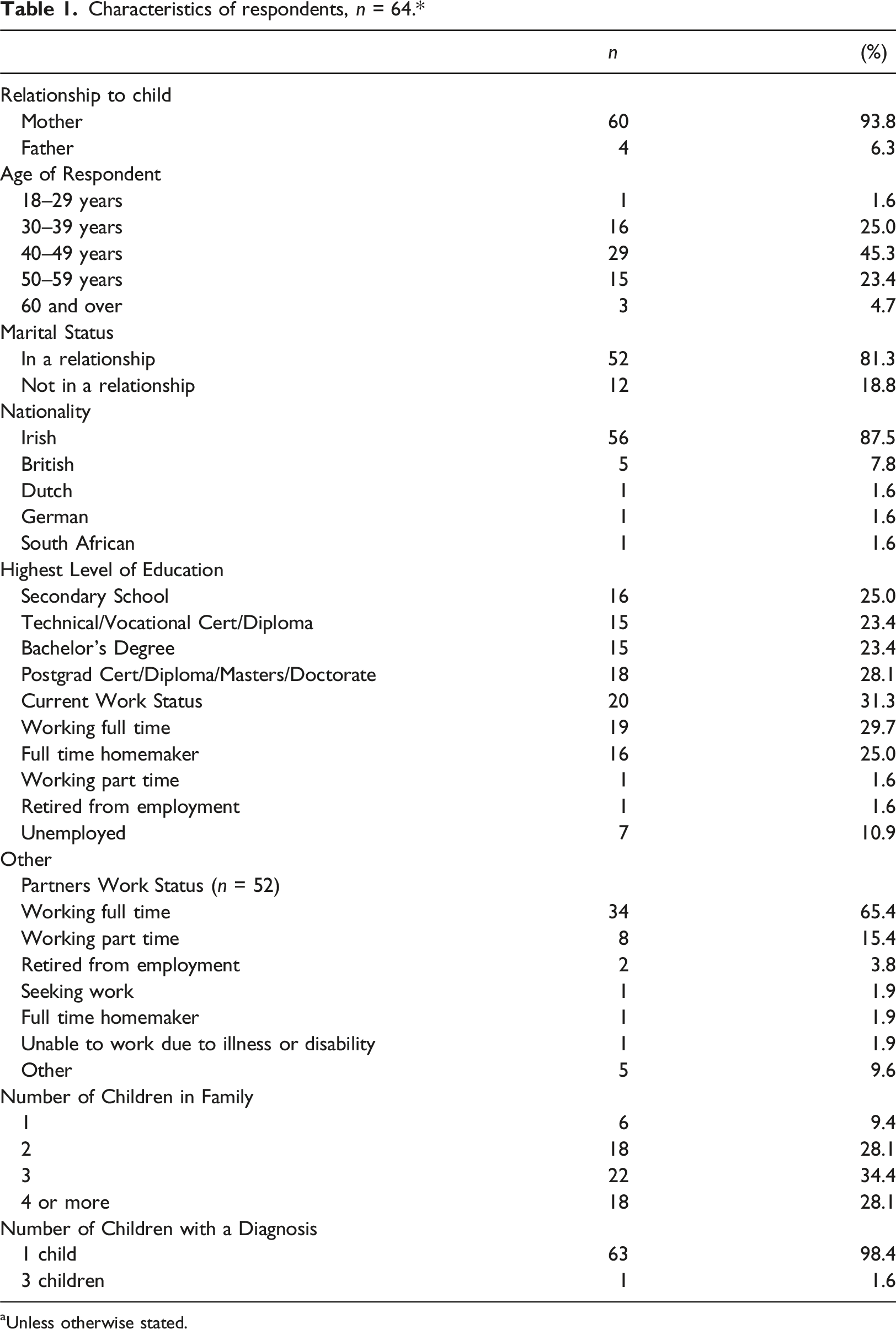
aUnless otherwise stated.
Characteristics of child with 22q11.2 deletion syndrome, n = 66.*
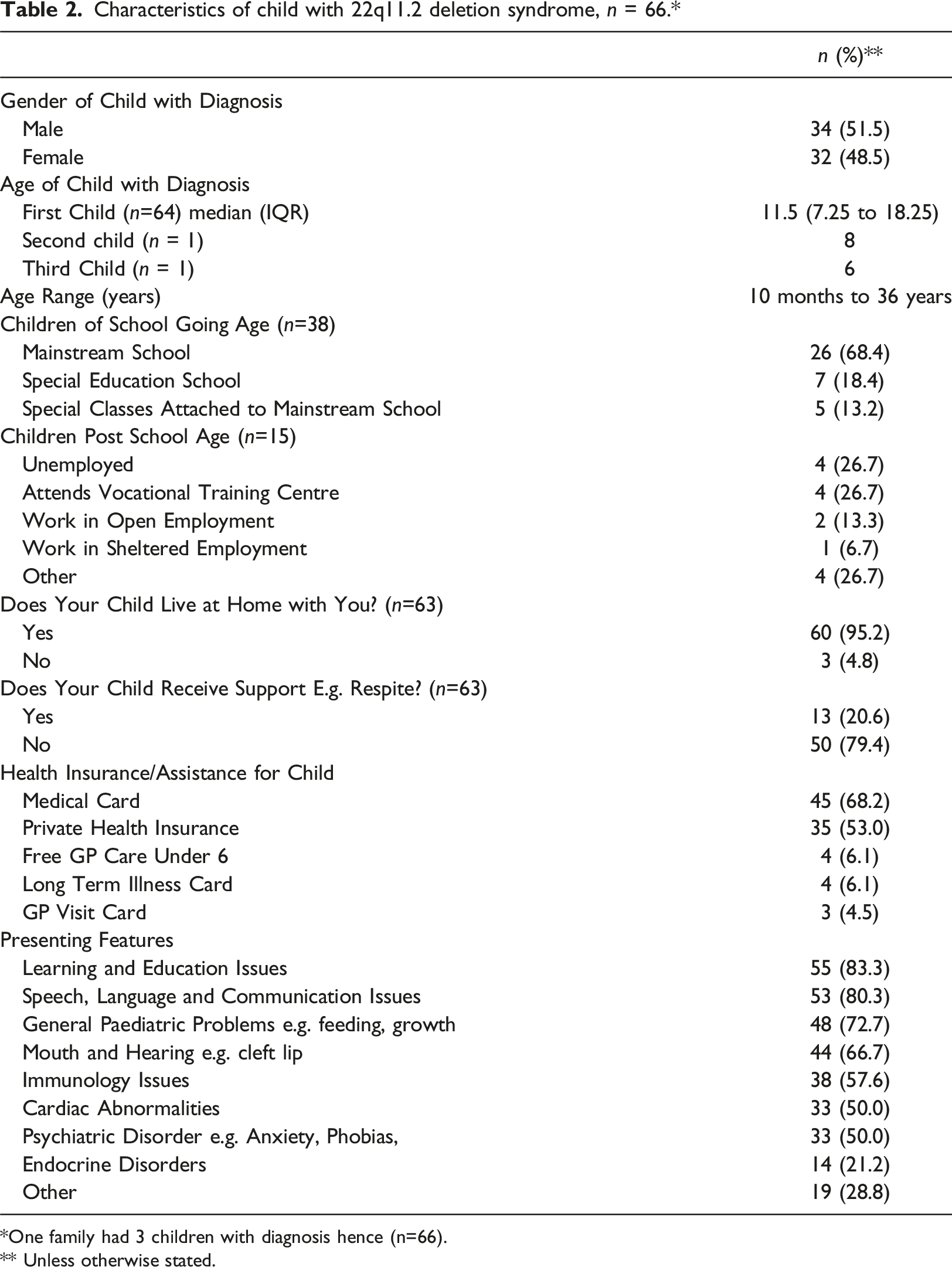
*One family had 3 children with diagnosis hence (n=66).
** Unless otherwise stated.
The mean score for hardiness was 43.75 (SD: 7.44) based on 59 respondents, indicating that the sample typically had good family hardiness at the time of data collection. A moderate, positive, relationship was found between adaptation and family hardiness (r=0.339, p=0.011, n=56), indicating that those with greater hardiness had better adaptation. Adaptation score increased by 0.62 points (95% CI: 0.15 to 1.08) for each one-point increase in family hardiness score. R2 was 11.5%, indicating that family hardiness explains 11.5% of the variance in adaptation. In the multivariate analyses, family hardiness was associated with adaptation (p=0.047). A positive linear relationship was found between the two variables, indicating that when family hardiness increases, adaptation increases. Family hardiness uniquely accounted for 6.8% of the variance in adaptation. The adjusted R2 for the model was 12.0%. The quantitative results revealed that family hardiness was a significant predictor of family adaption.
Semi-Structured Interviews
A total of nine parents were interviewed ranging from 30-59 years of age. The ages of their children with 22q11.2 deletion syndrome ranged from 3 years to 33 years. The length of time since their child’s diagnosis varied with some diagnosed in utero, others at birth and some experiencing late diagnoses.
The meaning of hardiness
The qualitative data provided deeper insights, explaining what hardiness meant for participants. Some participants believed that hardiness was innate such as having strength, determination and stubbornness. For some, characteristics were described as innate and in their DNA: “I think I’m quite stubborn person…think it’s the way I’m made, it’s in my DNA to be hardy, tough, stubborn, I’m quite stubborn I am…” P2
This sentiment was echoed by another participant who also held the belief that hardiness was just in your being, your character, an “in-built” characteristic: “I just think the hardiness is … I would just think it’s in-built in you…it’s either there or it’s not…I do think it’s your personality, regardless of…what you’re facing in life. So, it’s the characteristics of your personality” P11
For others, hardiness was not seen as innate, rather developed over time as a consequence of having a child with a disability. There was no choice but to be hardy since it was not possible to change the situation of having a child with a disability: “You know when you don’t have an option…you get on with it. They say there is certain things you can’t change, so there is no point kind of dwelling on them. You can’t change it, you can’t change it, you just have to get on with it” P10
Hardiness as strength was described not only on an individual level, but also in terms of strength as a family and for the family. It was described as a “toughness”, an ability to endure what life throws at you.
Strength, as a characteristic of hardiness took them through this process of “getting on with it”. One participant described herself as “mentally strong”: “So, mentally I would be quite strong, and I suppose because I keep busy, I don’t spend too much time thinking about it…” P9
However, even in the presence of characteristics such as strength, determination and stubbornness, the process of “getting on with it” was not easy. Participants described the toll that having a child with 22q11.2 deletion syndrome had on them. For example, one participant commented as follows: “I’d say yes, you probably sort of worry, cry, worry, cry, probably for many days, weeks months, years and then you have to sort of get up and keep it up, because you have to get up and keep going” P9
There was also a sense of hardiness because of personal growth; personal growth that stemmed from having a child in the first instance, but more specifically from having a child with 22q11.2 deletion syndrome. They viewed hardiness as being “in us all”, but when faced with adversity it grew and came to the fore. Whilst most participants described themselves as hardy, they were also of the view that hardiness was not static rather it was fluid and fluctuated from time to time: “It’s not an all defining type of thing you know; I don’t think you can be hardy a hundred per cent of the time” P3
Factors that Positively Influenced Hardiness
Participants revealed factors that they believed influenced their hardiness. Participants’ own parents and upbringing were spoken of as having a positive influence on their hardiness. Family values and one’s upbringing contributed to an inner strength within the family unit. One participant spoke of how her dad’s innate value of “respect” and his own hard upbringing contributed to her “toughness”: “Like I think it was my upbringing as well. He [Dad] brought us up to be respectful. He had a hard upbringing himself……. Yeah, he made us tough” P2
Learning from what was seen and experienced as a child shaped their approach to life as an adult. Participants spoke of how hardiness was embedded in one’s own family context with reference to their upbringing. For some, there was a sense that hardship led to hardiness. One participant described how family hardships and values as a child positively influenced her hardiness as an adult: “We are all set in our own family context, so my own parents would have had a hard-enough life and would endured hardships and you know, gotten through them. So, I suppose if you don’t have things easy all the time you do learn a certain resilience you know...Whatever it is you decide your values are, if you stand firm on them, that’s what makes you hardy” P3
Another positive influence on hardiness for participants was acceptance. The acceptance of the child’s diagnosis and its relative importance to hardiness was highlighted by participants. For some, acceptance was seen as “huge” and without it, the development of hardiness would be difficult: “…acceptance is huge it really is. I mean if you can’t accept something, it is difficult to be hardy…” P3
For some, acceptance did not come easy; it was a struggle and only came because of having no choice but to accept their child’s diagnosis. The struggle to accept the child’s diagnosis was poignantly portrayed by one participant who described herself as “reluctantly” but not fully accepting of her child’s diagnosis: “I don’t know, I wouldn’t say one hundred per cent, no. I have accepted it because obviously I have to. I still hate you know the thoughts that she has it. I suppose obviously I haven’t fully accepted it then… so I would say, I wouldn’t say no, and I don’t know whether I ever will. I mean, I accept it in as much as I have to” P11
Support was identified by many as a factor that contributed to their hardiness. Support was received in many forms and from a variety of sources such as spouse/partner, their siblings and support groups. An account from one participant identified that spousal support often provided a balance when she was having a bad day: “We do get it[support] from each other. Like myself and [husband] we would both be on the same wave length and if I have a bad day thinking you know, this is going really bad or I am really worried about this, he would be look she is doing really well in this and this and looking at the positive side of it” P11
The immediateness of the support received from spouses was recognised as important, however, the support received for the extended family unit was also seen as integral to hardiness. Family were relied upon at times when feeling “less hardy” and was described as a “fantastic” support. At times, the support required was more than their families could sometimes provide, which led to participants seeking support elsewhere. Participants described the value of a shared experience. The shared experience of having a child with a disability and/or 22q11.2 deletion syndrome was found to be a good source of support described as almost being part of a “club”: “I suppose you also look around you even at work and there are other people as well with children with disabilities and it just you are in that club as well…. so, you realise there are lots of people with children with disabilities” P9
The 22q11 Ireland support group was viewed by most as a great source of support and gave them strength: “When you have a whole group a community of people [22q11 Ireland support group] who are kind of reflecting back to you, your issues and your concerns, it does give a great strength that you wouldn’t have otherwise you know. I think back to prior pre 22q Ireland days and now there is no comparison, it just makes you stronger, it makes your hardier” P3
Factors that Negatively Affected Hardiness
Participants readily identified factors that had a negative influence on their hardiness. For many, the future for their children was of concern. Participants described how “anticipating” the future, “the unknown” challenged and negatively impacted their hardiness: “I think I can be hardy on terms of getting through the stuff, the daily day to day stuff and the therapies and that kind of stuff. But when it comes to the unknown and the future then you know I find it very hard to be [hardy]” P11
There was a resounding sense of fear amongst the participants with regards to the mental health phenotype of 22q11.2 deletion syndrome. This fear was palpable and evident in all participants regardless of the age of the child. Fear for the future was not centred in its entirety on the child with 22q11.2 deletion syndrome. Many spoke candidly of the fear of their own mortality and what that would mean for their child: “We are not going to be around forever and I don’t even think about that, cos I’d start freaking” P1
The experience of loss was recounted by many participants and like fear it was evident across a multitude of levels. Participants described a loss of personal identity, a loss of their pre-diagnosis self and the personal sacrifices a diagnosis brought. For some, loss was spoken about in terms of “grief” or “mourning”. Grief that was experienced because of having a child with a disability and that for some resulted in a certain vulnerability. One participant described how the grief never goes away and of being constantly in mourning.
Having a child with 22q11.2 deletion syndrome impacts everyone in the family unit. One participant in particular described how the worry within the family becomes cyclical between everyone. Everyone worrying about everyone else. In addition, many participants felt guilt was a challenge to their hardiness. For many this guilt was longstanding and usually centered around their other children: “I think once there is a disability within a home, no matter what it is, it impacts on everybody in the home and the siblings. Because my daughter [non affected] would worry about daughter [with 22q], she would worry about her dad, needless to say the dad would worry about daughter [with 22q11.2 deletion syndrome] then they would worry about me and they would worry about dad because…” P7
One participant described that life can get more difficult over time due to the new challenges brought about by the condition and this can have a negative impact on hardiness. This brings to the fore the sustainability of hardiness over time with recognition for the life-long impact of the syndrome and how that can negatively affect families over time.
Hardiness was viewed not only in response to a child’s diagnosis but also in terms of dealing with health care professionals. Participants described how negative interactions with professionals can have a negative impact one’s hardiness. One participant described the feeling of being dismissed as “only the mother” and how that had a negative impact on her: “You can get knocked back so easily by professionals that don’t understand. From the teacher to the nurse to the consultant, who will say you know “well actually I know better”…and if you have a particular concern about your child and it is dismissed and you are not feeling strong enough or confident enough to challenge that, that can be a real clamp back again do you know” P3
Discussion
This study investigated hardiness as a predictor of adaptation in families of children with 22q11.2 deletion syndrome. From the larger study from which this paper is drawn, family hardiness was found to be one of the most influential resilience factors of family adaptation. The quantitative results showed that when family hardiness increased, so too did family adaptation. Whilst these findings are new in the context of families of children with 22q11.2 deletion syndrome, they echo results from previous work in differing cohorts such as families of children with Down syndrome (Pruktarat et al., 2021; Caples et al. 2018), adverse life conditions (Dunst, 2021) and developmental disabilities (Greeff and Nolting, 2013). In addition, at the time of data collection, the parents of children with 22q11.2 deletion syndrome were found to have above average levels of family hardiness. This finding is also not unique to these families as previous research with families of children with chronic illnesses (Woodson et al. 2015) and mental illness (Puasiri et al. 2011) have also reported similar findings.
The identification of family hardiness as a predictor factor of family adaptation for families of children with 22q11.2 deletion syndrome is important. Whilst previous research has attempted to glean qualitative perspectives on factors that contribute to family adaptation, the findings were scant due to the reliance of open-ended questions in surveys which limits the in-depth exploration of family experiences. In addition to the specific focus on 22q11.2 deletion syndrome, this study therefore makes an important contribution to understanding family adaptation in the broader context of disability in that the qualitative perspective on family hardiness was included.
As revealed in the qualitative findings, participants perceived hardiness to be about “strength and determination”. The intrinsic nature of hardiness was described by some in terms of being an “in-built characteristic” to be “mentally strong” that served as a resource to endure the challenges of having a child with 22q11.2 deletion syndrome in the family. The focus on strength and endurance as a resource for families in adverse situations is consistent with the concept of family hardiness for resilience in that internal strengths and durability of the family unit serve as a buffer in alleviating the negative effects of stressors and demands (McCubbin et al. 1996).
At the time of quantitative data collection in this study, the participants were found to have above average levels of family hardiness, similar to studies on families of children with a range of chronic illnesses (Woodson et al. 2015) and with mental illness (Puasiri et al. 2011). Although hardiness was viewed as innate regardless of life circumstances, participants believed that this characteristic grew stronger in the case of having a child with a disability. While this qualitative finding suggests that families of children with disabilities have greater hardiness than those without disabilities, comparative research on parents with and without congenital defects have found higher levels of hardiness among those of typically developing children (Golpich et al. 2012). However, the findings from a review of evidence on family hardiness as a resource in coping with stress were inconclusive regarding the differences between families of typically developing children and of children with disabilities (Dervishaliaj, 2015). Although evidence on differences across families remains inconclusive, a consensus drawn from the work of previous researchers is the need for ongoing research on family hardiness among families of children with disabilities. In particular, these researchers called for a better understanding of protective factors that contribute to family hardiness (Weiss et al. 2013; Woodson et al. 2015; Dervishaliaj, 2015). According to Weiss et al. (2013), without understanding what contributes to family hardiness, developing resilience in families faced with chronic stressors in caring for children with long term conditions such as autistic spectrum disorders is not possible.
The qualitative phase also explored factors that positively or negatively influenced family hardiness in relation to having a child with 22q11.2 deletion syndrome. The findings offer a depth of insight into family hardiness influences compared to qualitative components of previous studies on family resilience which were typically limited to an open-ended question on surveys, none of which explicitly focused on the meaning of hardiness or influencing factors (e.g. Greeff and van der Walt, 2010; Greeff and Nolting, 2013; Bishop and Greeff, 2015). One insight was the “acceptance of the child’s diagnosis” and its importance to family hardiness. The earliest adverse event for families as described by parents was receiving their child’s diagnosis. Although a shock at the time, parents believed that acceptance of their child’s diagnosis had a positively “huge” influence on their hardiness. Acceptance has been reported as a protective resiliency factor against stressors and higher levels of acceptance have been associated with lower psychological distress and increased adaptation in mothers of children with autism (Da Paz et al. 2018).
Participants believed they had little choice but to become hardy since they could not change the situation of having a child with 22q11.2 deletion syndrome. They spoke of “getting on with it” as indicative of their acceptance, which seemed to reflect commitment as a component of family hardiness in the Resiliency Model concerning interdependence and an ability to work together as a family (McCubbin et al. 1996). For some participants, getting on with it as a family was described as a mechanism for survival especially in the earlier years, similar to comments expressed by families of adults with schizophrenia with reference to families working together to embrace the problem in order to survive (Bishop and Greeff, 2015). Acceptance and thus hardiness was also described by some parents as taking years to develop. This is important to note because time alone is considered insufficient for parents or families to come to terms with having a child with a long-term condition (Barnett et al. 2006).
Participants accounts of the fears they experienced offered insights into factors that threatened their hardiness, fears which were largely future oriented. Fears included fear for future, fear of the unknown, fear of the mental health phenotype associated with the syndrome and fear concerning their own mortality as parents. Some participants feared a decline in their hardiness as their children got older because protecting them was perceived to be a greater challenge than when younger. There is some evidence to support this fear in that parents of older children with chronic illnesses have been found to have lower levels of hardiness compared to their younger counterparts (Woodson et al. 2015). Given that these fears were found to have a negative impact of family hardiness and ultimately family adaptation, they need to be both acknowledged and addressed. There is a need for psychoeducational programmes to be developed to help parents better understand and cope with their fears and particularly the management of anticipatory anxiety associated with the fear of psychosis. To best support these parents, such programmes will require a level of flexibility to be adapted to the specific needs of the parents who are most in distress (Mahendran et al., 2017). With regards to fears of their own mortality, this is a fear common to many parents of children with disabilities (Walker and Hutchinson, 2018a; Deville et al. 2019; Walker and Hutchinson, 2018b). Assisting parents through the provision of both formal and informal supports to start future planning for their child may help alleviate some of the fears they are experiencing regarding their future mortality and their child’s future (Walker and Hutchinson, 2018a; Marsack-Topolewski and Graves, 2020).
In addition to fears, some participants spoke of their sense of loss and grief for a child without disabilities as negatively impacting their hardiness. The “constant mourning” described by one participant suggests that families can experience a chronic sorrow characterised by loss and a longing for their desired child on realising their child with disability may not reach the full potential of typically developing children (Coughlin and Sethares, 2017). According to Kandel and Merrick (2007), parents’ responses to children with disabilities can vary with mourning and acceptance at opposite ends. The role of acceptance of a child’s disability and its potential towards helping families offset or manage their fears and sense of loss has received little research to date. Although some studies have explored how parents come to terms with their child’s disability (Altiere and Von Kluge, 2009; Da Paz et al. 2018; di Renzo et al. 2020) and have developed interventions supporting their acceptance (Blackledge and Hayes, 2006; Reid et al. 2015), there has been little family research in this regard.
The positive influence of support on family hardiness came to the fore in this study in particular, the support received from immediate and extended family. In addition, the national 22q11.2 deletion syndrome support group was described as providing families with great strength. Families were acknowledged as an important and valued “support system” especially at times when feeling “less hardy”. Family as a “support system” calls to mind Ungar’s (2016) perspective on family resilience with reference to various members interacting at multiple levels when faced with challenging situations. Within the context of the Resiliency Model, the ability of families to work together to combat stressors influences family hardiness (McCubbin et al. 1996). To date, there is a paucity of research on the influence of social support on hardiness within the context of the family as a unit. Similar to the current study, both social support and hardiness have been measured in previous family resiliency research (Jonker and Greeff, 2009; Greeff and van der Walt, 2010; Greeff et al. 2012; Greeff and Nolting, 2013; Bishop and Greeff, 2015; Caples et al. 2018). However, none have investigated the relationship between these variables and whether social support might be a mediator explaining the relationship between hardiness and adaptation for families of children with disabilities. While this gap in knowledge has not been addressed in the quantitative phase of the current study, the qualitative findings contribute to knowledge in this regard given the emphasis that participants placed on the importance of support as a positive influence on their hardiness with reference to their immediate and extended family and the social support network of the national 22q11.2 deletion syndrome group.
The importance of family support identified in the current study lends support to Smith et al.’s (2020) recommendation for multicomponent family focused interventions that provide skills training, psychosocial and educational support. It is recommended that family hardiness be considered as a component within interventions, given that in this study it was the resilience factor that best explained family adaptation. While multicomponent interventions are more likely to have positive outcomes, they are complex and need to follow guidelines available for rigorous development and evaluation (O’Cathain et al. 2019). Such interventions need to target individual family members and the family unit.
Future studies need to increase family representation beyond one individual, typically mothers reporting on behalf of the family, to include other family members such as fathers and siblings, and children affected by the syndrome. This is important to better understand the family perspective on resiliency so that interventions are developed and tailored to their specific needs. The consequences of proxy reports on resiliency from key family informants, as has been the case in most previous research and in this study, are that individual rather than family level data are captured (De Haan et al. 2002). However, there are difficulties with obtaining and analysing family level research data (Eggenberger and Nelms, 2007) because family research requires an understanding of family processes, meaning making among different members, diverse family contexts, and family interactions (Roy et al. 2015).
For the purpose of developing family focused interventions, qualitative research is an important first area of inquiry in order to gain a deep understanding of family experiences (Eggenberger and Nelms, 2007). Further qualitative research is recommended with families of children with 22q11.2 deletion syndrome given the limitations noted for the current study regarding sample size and proxy accounts. In addition to individual interviews with various family members, suggestions for providing a richer sample include interviewing two or more family members at the same time, for example, family group interviews, couple interviews, and sibling interviews (Roy et al. 2015). Further qualitative research also has implications for advancing the theory of family resiliency by drawing out the richness and paradoxes of the totality of family life (Hutcheon and Lashewicz, 2015).
In contrast to the emphasis that participants placed on the positive influence of informal supports on family hardiness, the data referred to mixed levels of support from health care professionals in this regard. Negative interactions with various professionals in the health and education sectors were described by some participants as negatively influencing their hardiness. This study has highlighted the need for an integrated family focused approach to service delivery and practice in caring for people with 22q11.2 deletion syndrome. Health care professionals supporting families of children with 22q11.2 deletion syndrome need to shift from an individual approach to care to a family focused model of care. Adopting a family focused model of care could help identify the needs of each family member and address the current tensions that exist between some parents and professionals. A shift to integrated family focused models of care has the potential to improve services for families of children with 22q11.2 deletion syndrome, especially given the multisystem nature of this syndrome and requirement for health services from many specialities and services.
Limitations
The aim of this study was to investigate the relationship between family hardiness and adaptation therefore, the study of the family should encompass all family members. Only one questionnaire was administered to each participating family with the invitation for one parent to complete on behalf of the family. Most participants were mothers, and it is unclear if family members conferred in completing the questionnaire. Therefore, a limitation of the study is that the perspectives of individual family members and the whole family were not gleaned. Consequently, the individual, rather than family unit, become the primary source of data (De Haan et al. 2002). This is not unusual as previous studies concerning families have reported experiencing similar difficulties (Bayat, 2007; Greeff and Nolting, 2013; McConnell et al. 2014). Whilst the primary caregiver is often aware of their family’s needs and has unique insight into family life (McConnell et al. 2014), responses may have differed if different family members were sampled. For example, there is evidence that siblings of children with chronic disability are at heightened risk of psychosocial difficulties (Emerson and Giallo 2014; Giallo et al. 2012). Future studies need to increase family representation beyond mothers to include other family members such as fathers and siblings.
Conclusion
This study contributes to an understanding of family hardiness for families of children with 22q11.2 deletion syndrome. The findings provide insights into perspectives on family hardiness and adaptation at different times across the lifespan. The quantitative phase of this study was cross-sectional and so the findings on resilience and adaptation for families of children with 22q11.2 deletion syndrome relate to one time point in their lives. Insights gleaned from the qualitative findings revealed that family hardiness was not static; it can and does change over time according to various circumstances such as transition to school, unanticipated medical treatments such a surgery, or transition into adulthood. Therefore, it is recommended that future studies consider a longitudinal approach such as experience sampling methodology to appraise their experiences in daily life over time to elicit a comprehensive view of their experiences. Longitudinal research will also help to identify changes in the phenotypical presentation of the syndrome (e.g. development of a psychosis in adolescence/young adulthood), and how this might impact on family hardiness and adaptation. In addition, in order to better understand the family perspective on resiliency, future studies need to put in additional efforts to recruit and increase family representation beyond mothers to include other family members such as fathers and siblings, and children affected by the syndrome.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.