
Abstract
The COVID-19 pandemic profoundly impacted daily life, including the educational experiences of school-age children with and without disabilities and their families who supported them. This descriptive qualitative study examined the experiences of families with children with extensive support needs and complex communication needs during the COVID-19 pandemic, specifically in relation to their (a) supports and (b) feelings of empowerment related to their child. Participants were 37 parents of children with disabilities who had extensive support needs and complex communication needs, with most families having a child with either autism or Down syndrome. Interviews were conducted with each family at three time points during the 2020–2021 school year. Results indicated that the supports families received varied widely, as did their feelings of empowerment— including empowerment related to advocacy and to supporting their child’s learning and well-being at home. The supports that families received from providers (e.g., teachers, service providers) impacted their feelings of empowerment, sometimes acting as facilitators and sometimes as barriers. Implications for future research and practice are discussed related to how teachers and other providers might better partner with families during crises like the COVID-19 pandemic and beyond.
Beginning in March 2020, the COVID-19 pandemic impacted 50.8 million students in the United States through school closures (Education Week, 2020). Remote learning ranged widely across schools, with variations both in expectations for student engagement and in format (e.g., take-home packets, online assignments, live instruction through videoconferencing; Marshall et al., 2020; Oster et al., 2021). Learning access and outcomes continued to be impacted through the 2020–2021 school year, playing out differentially across students, and posing the greatest challenge for those already at risk for educational disparities such as students with disabilities, especially who have extensive support needs (Colvin et al., 2022; Oster et al., 2021).
Students with extensive supports needs have intellectual and developmental disabilities (IDD) and need substantial support across domains (e.g., communication, academics, behavior, daily living, health, relationships); they are also students who are generally eligible for their state’s alternate assessment (Kurth et al., 2019). Many students with extensive support needs also have complex communication needs, meaning they are mostly or entirely nonspeaking and use aided or unaided augmentative and alternative communication (AAC) instead of or alongside verbal speech—including gestures, nonword vocalizations, manual signs, picture symbols, and/or speech-generating devices (Beukelman & Light, 2020). The pandemic greatly affected students with complex communication needs, as they often lost not only access to in-person academic instruction but also other needed services (e.g., speech therapy/AAC services, occupational and physical therapy; Neece et al., 2020; Therrien et al., 2022).
Teachers and families alike reported challenges with remote learning for students with extensive support needs and complex communication needs (Averett, 2021; Hanreddy, 2022; Navas et al., 2022). The emergency use of remote teaching meant children often did not receive needed accommodations, services, and support (Averett, 2021; Navas et al., 2022), and so families were often left to navigate educational services that required substantial involvement from them but still did not meet their child’s individualized needs (Averett, 2021; Neece et al., 2020). Parents reported that meeting their child’s educational needs at home was one of the greatest challenges of the pandemic (Neece et al., 2020), and parents of students with complex communication needs often faced even greater challenges such as their child having difficulty accessing remote learning, losing out on communication growth that happens through peer interaction, and losing access to school-provided AAC devices (Therrien et al., 2022).
Family Empowerment
Our conceptual framework for this study came from the concept of empowerment, which can be defined as the process through which people have positive control over their lives, including in their knowledge, attitudes, and actions (Koren et al., 1992; Rappapon, 1984). Rappaport (1984) explained that empowerment was “easy to define in its absence: powerlessness, real or imagined; learned helplessness; alienation; loss of a sense of control over one’s own life.” Conversely, empowerment means that a person has both a sense of control and the actual power to effect one’s own life in a positive way.
Empowering families is an important goal in special education (Hsiao et al., 2018), and empowerment in this context is typically measured at three levels: family, service-system, and community (Koren et al., 1992). Family-level empowerment refers to how parents feel empowered to support their child’s learning and well-being at home; service system empowerment relates to how families get supports and services for their child; community empowerment relates to families’ roles in disability services at a systems-level. The Family Empowerment Scale (Koren et al., 1992) is one of the most widely utilized measures of empowerment in special education. It includes three subscales addressing each of these areas of empowerment (i.e., family, service system, community). Several researchers have used it to understand how empowerment relates to factors such as well-being and stress for parents of children with disabilities (Burke et al., 2020; Minnes et al., 2015). For instance, Minnes et al. (2015) found that increased parent empowerment predicted well-being, and lower empowerment predicted distress. Similarly, Burke et al. (2020) found that empowerment was negatively correlated with stress.
Family Empowerment and Social Support
Another important aspect to a conceptual understanding of empowerment is the idea that empowerment is not simply an internal characteristic of a person. Instead, conceptual models of empowerment focus on the connections between the individual strengths and competencies of individuals to their broader social ecology—the relationships and support the individual has through formal programs and from professionals, but also from their “natural” supports such as family and friends (Perkins & Zimmerman, 1995; Rappapon, 1984). Thus, family social support includes both formal sources—such as organizations, agencies, and educational professionals— and informal relationships, such as friends and family (McIntyre & Brown, 2018). Formal and informal social support is important in improving outcomes for families of children with disabilities, including decreasing stress and increasing resilience (Burke et al., 2020; Burke & Hodapp, 2014). For instance, Zhao et al. (2021) investigated the impact of formal and informal social support for 486 families of children with disabilities in China, finding increased support predicted higher resilience and lower stress for parents. Across a series of studies, Burke and colleagues found that parents of children with IDD who reported higher satisfaction with family-school partnerships also reported lower stress (Burke et al., 2020; Burke & Hodapp, 2014).
Yet, research exploring the relationship between family supports and empowerment is more limited (Burke et al., 2020; Pisula & Banasiak, 2020). In a study focused on Polish fathers of children with autism and Down syndrome, Pisula and Banasiak (2020) found that availability of and satisfaction with social supports were not correlated with empowerment for fathers of children with autism, but they were for fathers of children with Down syndrome, at least related to empowerment in the community. Burke et al. (2020) found family–school partnerships were positively correlated with empowerment. However, these studies have focused on empowerment related to navigating the service system, not necessarily empowerment related to how parents support their children’s learning and well-being at home. Furthermore, quantitative methods have dominated this body of literature; qualitative inquiry could complement existing knowledge by providing in-depth, contextualized understanding of families’ experiences.
Purpose of This Study
The purpose of this study was to provide in-depth understanding of the experiences of families of children with complex communication needs throughout the 2020–2021 school year, particularly as they relate to support and empowerment. Much of the currently available research regarding the impact of the COVID-19 pandemic has focused on the initial months, during lockdowns from Spring of 2020 and in the midst of emergency remote learning (e.g., Oster et al., 2021; Willner et al., 2020). Less is known about experiences later in the pandemic. Furthermore, other findings suggest that having a child with more complex needs, such as related to communication or behavior, was associated with increased challenges for families during the pandemic (Navas et al., 2022; Willner et al., 2020), and yet there has not been a lot of focus on this important population, particularly related to family empowerment. Therefore, we sought to address these gaps through three research questions:
Method
This descriptive qualitative study involved semi-structured interviews conducted across three time points during the 2020–2021 school year (Fall, Winter, Spring). Data came from a larger mixed method project which aimed to examine the experiences of families of elementary-aged children with complex communication needs during the COVID-19 pandemic. Institutional review board approval was received for this larger project. Qualitative description is focused on providing a straightforward interpretation, in which analysis remains fairly data-near (Sandelowski, 2010; Willis et al., 2016). Because qualitative description can take on different forms (Sandelowski, 2010), it is especially important to understand the paradigm which guides researchers. We operated out of a pragmatic paradigm, which means we made key decisions (e.g., sampling, data collection, data analysis) based on our desire to gain practical understanding about a real-world issue that could then be used to inform action (Kaushik & Walsh, 2019; Patton, 2015).
Positionality relates to potential research bias in data analysis and interpretation, as well as issues of power in how studies are designed and conducted. Our primary research team was comprised of two graduate students in special education and their faculty advisor, who were all female, White, had prior experience working with students with extensive supports needs, and approached the work with a strong desire to understand how schools and teachers can better support students and families. The second author was a mother, but no members of the research team were parents of children with disabilities, and thus were most like “outsiders” in relation to the experience of participating parents, even though the notion of insider/outsider status is not really a simple dichotomy because people have multiple, and often fluid and context-dependent identities (Bayeck, 2022). In the case of this study, we all as researchers were impacted alongside participating parents by the COVID-19 pandemic in many ways, creating a broader shared experience between researchers and participants. To address bias, we used reflexive practices such as critical discussion and memoing throughout all stages of the study to examine our positionality and identify and address potential biases (Patton, 2015). Related to power, we sought to build rapport and create equal-power relationships in our interactions with participants (e.g., by having participants choose interview times, by taking a conversational approach that allowed participants to share beyond what was in the interview guide).
Participants
Participants were 37 parents of kindergarten to fourth-grade students who had complex communication needs. Participants were recruited for the larger project via flyers and emails that were distributed through school districts, service providers, and community disability associations. Recruitment materials directed interested families to a study website which had additional information about the study and an interest form. Families who completed the interest form were contacted by a member of the research team to be screened for eligibility by phone, and then to provide consent to participate. To be included, families needed to live in Tennessee and have a child with IDD who (a) received special education services in a public school in kindergarten to fourth grade and (b) had complex communication needs, which we operationalized for the study as using prelinguistic (e.g., gestures) or early linguistic communication (e.g., single words and/or some short 2–3 word phrases), measured through parent report on the Communication Matrix (Rowland & Fried-Oken, 2010). Approximately two-thirds of children (64.9%) had access to aided AAC at home but not all used it regularly. All students whose individualized education program (IEP) teams had made decisions about eligibility for alternate assessment were eligible. Some IEP teams of younger students (i.e., kindergarten and first grade) had not yet made decisions regarding alternate assessment eligibility.
Children in this study had extensive support needs, which we evaluated by having parents complete the Supports Intensity Scale–Children’s Version (SIS-C; Thompson et al., 2016). The SIS-C scores are standardized and address the level of support that children need relative to other same-age children with IDD. The mean standardized percentile score was 37.7 (SD = 24.8), which meant that, on average, children had more intensive support needs than approximately 37% of other same-age children with IDD, with wide distribution across the sample. Also, based on results from the SIS-C, nearly half of children had intensive behavioral support needs (48.6%) and roughly one-third had intensive medical support needs (32.9%), as show in Table 1.
Parent Characteristics, Household/Family Characteristics, and Child Characteristics.
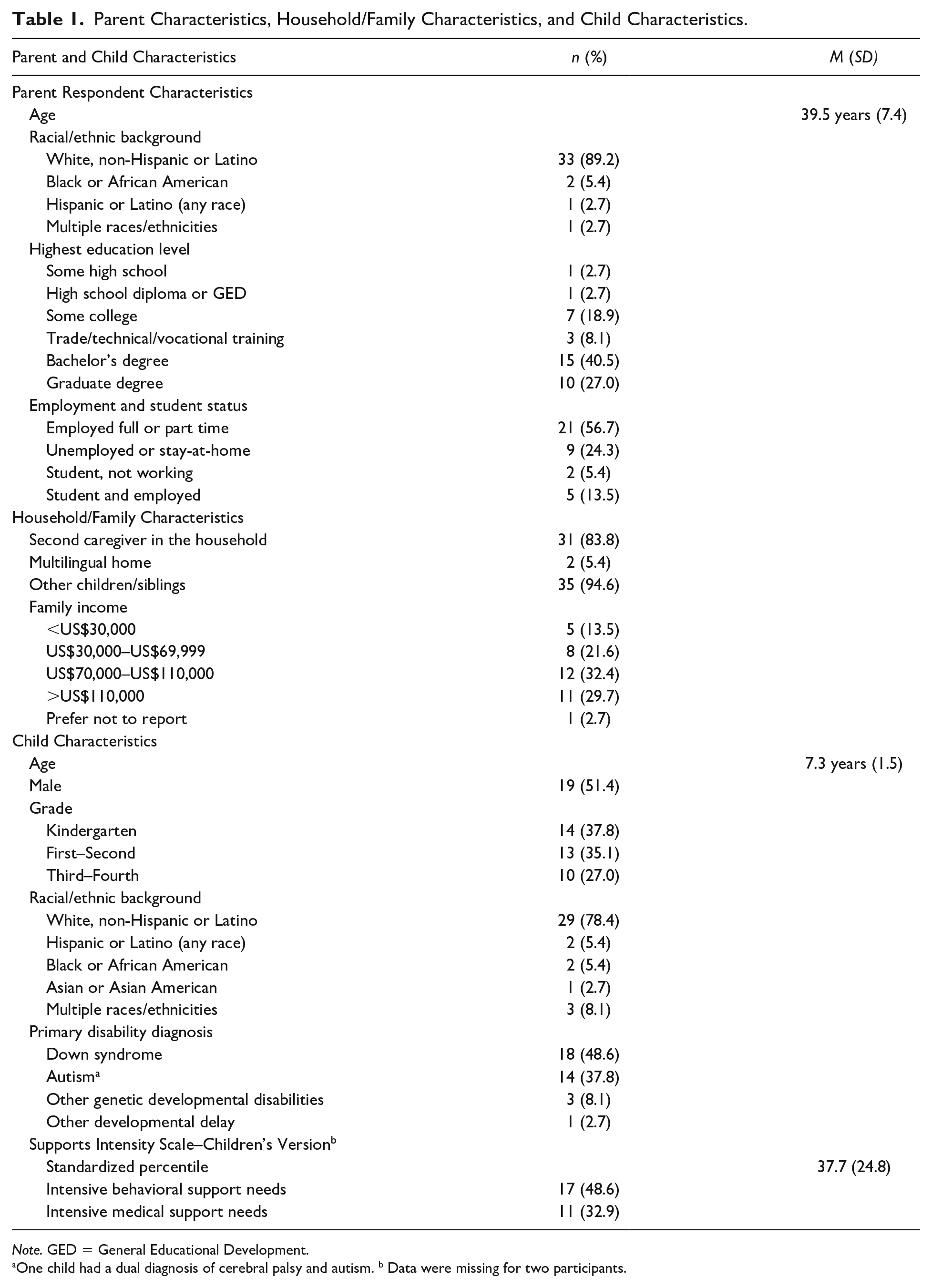
Note. GED = General Educational Development.
One child had a dual diagnosis of cerebral palsy and autism. b Data were missing for two participants.
Table 1 reports additional information about participants. Roughly half of children were male (51.4%), and most had diagnoses of Down syndrome (48.6%) or autism (37.8%). However, many children had multiple diagnoses, including intellectual disability, cerebral palsy, attention-deficit/hyperactivity disorder, apraxia of speech, and seizure disorders. Most parents were biological mothers (83.8%); five were biological fathers (13.5%), and one was an adoptive mother (2.7%). Most were White (89.2%), lived in two-parent homes (83.8%), and had a Bachelor’s or graduate degree (67.5%). More than half of families lived in suburban settings (56.8%), almost a third in rural settings (29.7%), and the remaining families lived in urban settings (13.5%). Just over two-thirds of participants were employed full or part-time (70.2%) at the start of the study, though many later reported employment changes resulting from the pandemic (e.g., loss of jobs or hours, resigning to stay at home and care for children).
School services varied fairly widely because of the pandemic, and most families reported frequent changes in the format of their child’s schooling within and between data collection time points. At Time 1 (September/early October 2020), 16 children (43.2%) attended school in-person, 13 (35.1%) were fully virtual, and eight (21.6%) in a hybrid arrangement. Fewer children (24.3%) were able to attend school in-person in at Time 2 (January 2021), with most in a hybrid arrangement (i.e., combination of in-person and virtual learning; 45.9%), and 29.7% were fully virtual. By Time 3 (late April/May 2021), 21 children (56.8%) were attending school in-person; only three were fully virtual (8.1%), and all remaining (35.1%) were in a hybrid arrangement.
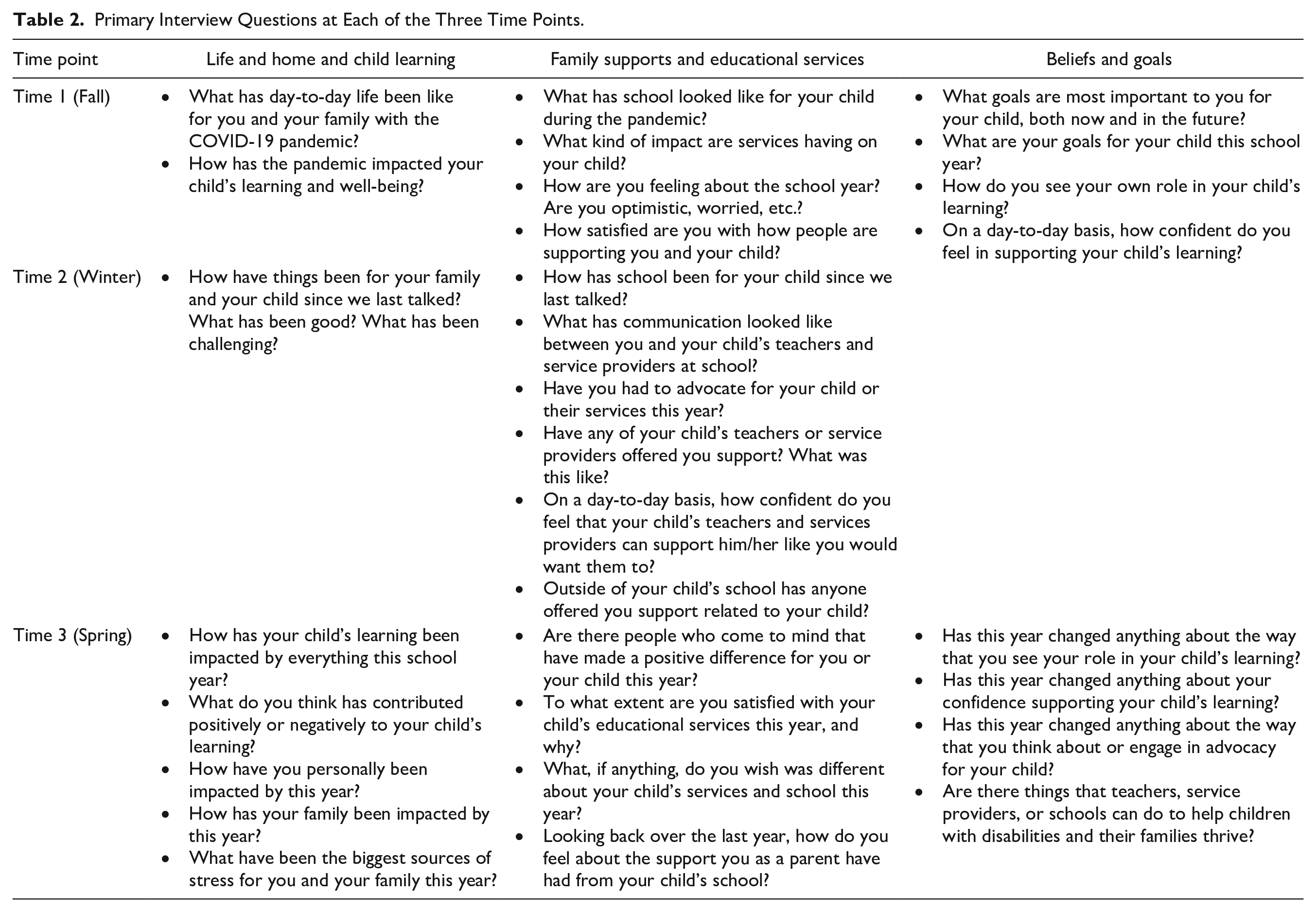
Data Collection
Data were collected through semi-structured interviews, conducted and recorded through Zoom. We conducted a total of 115 interviews across the three time points (described earlier), with little missing data—two participants did not complete the first interview, and one did not complete the final interview. The research team developed semi-structured interview guides to use at each time point (see Table 2), and each interview was conducted by one of four research team members, including the first and second authors (a graduate student and a faculty advisor) and two other graduate students. Each participating family was assigned to one interviewer so they could build rapport and trust across the school year (Grinyer & Thomas, 2012). This also allowed interviewers to conduct informal member checks by revisiting ideas raised in previous interviews with the same participant. We opted for this approach, rather than a more formal approach for member-checking, to reduce burden for families (Motulsky, 2021). Interviewers used the interview guide to provide consistency, but they adopted a conversational style that involved asking natural follow-up questions to encourage participants to expand or clarify their responses. Interview length ranged from 51 to 119 min (M = 84 min) at the first time point, 10 to 56 min (M = 33 min) at the second time point, and 19 to 81 min (M = 51 min) at the third time point. Interview lengths for the first and third time points were longer because additional data were collected as part of the larger project; approximately half of this reported time (at Time 1) to two-thirds of the time (at Time 3) was used to engage with participants using the semi-structured interview guide. After interviews, interviewers completed a written reflection to promote reflexivity and share early findings with other team members (Patton, 2015).
Primary Interview Questions at Each of the Three Time Points.
Data Analysis
Interview data were analyzed using a team-based, inductive approach to general qualitative analysis (Saldaña, 2021; Thomas, 2006). Strategies to ensure rigor and promote credibility and trustworthiness included researcher reflexivity, utilizing multiple interviews to build trust and allow for ongoing member-checking, creating an audit trail of decisions and data, conducting iterative rounds of analysis, and triangulating across researchers (i.e., by engaging in collaborative coding and analysis) and across sources (i.e., comparing and synthesizing findings across multiple interviews; Brantlinger et al., 2005; Patton, 2015).
After interviews were transcribed verbatim and de-identified, they were imported into Dedoose (Version 9.0.46), a web-based program for qualitative analysis. We then completed four iterative cycles of coding. A codebook was created and updated throughout analysis, archiving older versions to create an audit trail. In the first coding cycle, three team members (i.e., the first and third authors and an undergraduate assistant) completed structural coding (Saldaña, 2021), which involved labeling and indexing relevant excerpts to be further analyzed in later cycles. Structural codes were broad codes related to the research questions (i.e., three structural codes related to “family supports” and two to “empowerment”) that were developed collaboratively and then coded independently by a member of the team after training from the first author. Coders met regularly throughout the coding process to clarify and ask questions as they arose, and the faculty advisor also checked transcripts to confirm consistency across coders.
The second cycle consisted of open coding, which aimed to break down the longer excerpts into more discrete parts and codes (Saldaña, 2021). The first and third author collaboratively coded each excerpt flagged during the structural coding, inductively generating open codes. Codes were organized in a simple hierarchy, using two primary “parent” codes aligned with the first two research questions: (a) family supports and (b) empowerment. Within family supports, “child” codes were (a) desired supports, (b) received supports, and (c) loss of supports, with seven additional subcodes for desired supports and eight subcodes for received supports. In addition, 11 child codes were generated as open codes within empowerment. Then, the third coding cycle involved identifying themes and subthemes. All excerpts were exported to a document that clustered excerpts by code. The first and third authors carefully reviewed excerpts and memoed, independently generating possible themes and subthemes by identifying connections across codes. The two researchers then met to reach consensus with the second author who provided critical feedback and peer debriefing. Finally, following this meeting, the first author conducted a final coding round that involved revisiting transcripts to search for confirming and disconfirming evidence. No disconfirming evidence was found, but additional excerpts were coded which expanded understanding of themes in nuanced ways.
Following this inductive process, we addressed the final research question about how family supports were associated with empowerment through example cases which illustrated family experiences. We chose to identify individual cases in addition to our across-case analysis (described earlier) so that we could interpret and describe families’ experiences as both a whole and its parts (Ayres et al., 2003). Our use of coding and sorting—and then identifying themes—captured the commonalities of experiences, but we felt that looking at and through individual cases (i.e., one family’s experience across the school year) would best provide the contextual richness needed to examine how families’ supports connected to their empowerment.
Given our large sample size, it was not practical to think that we could report on all participants. Thus, we sought to identify a smaller number of cases (i.e., a number feasible for reporting) which could exemplify how support influenced family’s feelings of empowerment. To identify these cases, we collaboratively re-reviewed the excerpts within the previously coded themes and found two main patterns for how supports were associated with empowerment: (a) communication and relationships with providers either supported or hindered advocacy and trust, and (b) how professionals provided resources and training either supported or hindered experiences with at-home learning. Therefore, we chose to identify and report four example cases related to these patterns, with two cases for each—one example of how supports empowered families, and the other where families were impacted negatively. After identifying the four cases collaboratively, the first author reviewed all coded excerpts for each case and wrote memos about the family’s experiences, periodically collaborating with the second author for feedback, and eventually developing brief, one-paragraph descriptions of the case.
Results
Family Supports
Three themes were related to family supports: (a) supports from providers, (b) supports from others, and (c) loss of supports.
Supports From Providers
Teachers, paraprofessionals, service providers, and school administrators were important sources of support for families, and three subthemes were included in this theme: (a) relationships with providers, (b) communication, and (c) training and resources.
Relationships with Providers
Parents felt especially supported by providers when they had a strong personal relationship—marked by professionals respecting parents, offering support and encouragement, and truly knowing and connecting with their children. Parents who felt that their child’s teachers and therapists respected them described their child’s school team as “great listeners” and “willing to make adjustments.” Other parents felt disrespected and unheard. Hannah, a mother of an autistic third grader, described the tension she felt with her child’s speech therapist, saying: “We don’t mesh well, and so I feel like anytime I say something, it’s just brushed under the rug.” Parents often focused on the impact of a single professional, describing them as “a sounding board,” “always encouraging,” and “my go-to person.” For Olivia, a mother of a kindergartner with autism, this person was her daughter’s special education teacher: “I feel I can call her anytime of the day or night, and just have a conversation or cry or just show her a great picture of [child] doing a puzzle. So that’s been great.”
Equally important for strengthening relationships was that parents felt professionals truly understood, cared about, and made a difference for their child. Parents highlighted connection with and support of their child beyond what they felt was expected or required, describing them as going “above and beyond.” Susan, a mother of a first grader with Down syndrome described school’s response when she suggested celebrating Down syndrome awareness month as a school:
And the principal, his teachers, they were just all really supportive and gave great feedback. And that’s really important to me as a parent to have a place where he feels like he belongs . . . where it feels like the school is supportive of him and our ideas.
Communication
Communication was also critical for parents to feel supported, such as through texting, email, phone calls, videoconferences, apps, daily communication logs, and face-to-face conversations. Parents emphasized that communication was always important, but the pandemic changed aspects of it—sometimes making communication better, and sometimes making it worse. Strong communication helped parents gain valuable insight; without this, parents felt “in the dark.” Carly, a mother who had an autistic third grader emphasized:
You got to remember, this is my child who cannot tell me anything about what you do to him—nothing. I’m giving you my whole heart in your hands. So, when I ask for communication, when I’m trying to find out something, it’s not that I’m belittling you. I’m not second guessing you. My kid can’t tell me, so I need you to tell me.
Although they varied in how often they wanted to be communicating with providers (e.g., daily, weekly, bi-weekly), it was not enough to be updated only at annual IEP meetings or quarterly progress reports. Michelle, who had a kindergartner with Down syndrome shared her frustration, saying: “I’m not hearing nothing for like 3 and 4 and 5 months, and I’m thinking, ‘What the hey?’ I want to be involved in my child’s education a tad more. At least hear about what’s going on.” Other parents felt frustrated that reports focused on challenges or problems rather than strengths. Mark, a father of an autistic third grader explained, “We appreciate how much you’re telling us what she’s doing wrong. Could you possibly slide in some stuff that she’s doing right every once in a while?”
Whether or not families felt supported by providers’ communication also depended on the responsiveness of these professionals. Some felt well-supported, describing “absolute open communication” and feeling “invited into the conversation.” Other parents described a “disconnect,” feeling “ignored” and that providers “didn’t listen” to them. Michelle explained,
I feel like I’m trying to reach out. I’m trying to be a part. I’m trying to be involved, and I don’t get as much feedback back. I’m like (shrugs), “Wow. I’m going above and beyond in my opinion, and yet I’m not seeing much, I’m not hearing much.”
Training and Resources
Another type of support related to “guidance,” “coaching,” and “instruction” from providers, which especially helped parents feel more equipped to support their child at home during remote learning. Carly explained,
When I can see [ABA therapist] give me an idea, I’m like “Oh, I can run with that!” And I can do those things with [my child]. But as far as trying to do it on my own— Oh, I would not. I feel like I would flounder.
Some parents also described physical supports from teachers and therapists who delivered materials to their home during COVID-19 lockdowns or quarantines—resources like worksheets, books, visual aids, and picture symbols for communication support.
Many parents, though, received little support for remote learning. They felt overwhelmed and frustrated, like Stephanie, a mother of a kindergartner with Down syndrome: “I don’t know what to do with [my daughter]. I don’t know how to help [her]. I’m not the teacher—what do you want me to do?” Moreover, even parents who said they knew teachers were “doing all they can,” were emphatic about the challenges they faced during periods of learning at home. Stephanie explained, “Virtual learning is not working. Services aren’t working. School is not— it’s just not working.” At times during the year, several parents felt the only support that would be truly meaningful was not possible: in-person learning. Rachel, a mother of a first grader with Down syndrome, described the tension in returning to virtual learning after a brief period in-person: “There’s just no comparison in terms of her level of engagement. But we have elected to keep her learning remotely because there’s still significant exposure risk. But that was a hard decision.”
When students were in school in-person, parents still explained they felt supported when teachers and service providers helped them know how to provide a “continuation” of what students were learning at school. Julie, a mother of a fourth grader with Down syndrome explained, “I like when they send home what she’s been reading in the classroom so that we can do that again in the evening. And just help reinforce what they’re already doing.”
Supports From Others
Beyond providers, families described receiving or needing other supports, including from disability organizations, governmental programs, family, friends, and social media. Some parents had ample support, but others did not. Rachel described her family’s impact: “It’s impossible to measure honestly. There’s no way. I can’t imagine navigating this year [without them].”
Parents frequently emphasized the impact of friends and family, using terms like “a huge help,” and a “village” to describe the support of relatives and close friends. These relationships offered valuable community and encouragement. Olivia explained, “I don’t think I could go through what we’ve been through, just finding out her diagnosis, but even this year in particular with the pandemic, without having someone every day that I can just talk to about something.” Families struggled without this support, as Hannah explained, “It’s been very isolating . . . We don’t have any immediate family or friends who could really help us at the drop of a hat.”
Financial support also had a significant impact on many families, who described grants and governmental assistance as “a game-changer,” and “our lifeline.” Families used this support for varied purposes, such as child care, medical care, therapies, and basic living expenses. Others talked about how stressful it was to try to access such supports. For example, Brittany, a mother of a kindergartner with a rare genetic condition described the arduous process to apply for a state health care waiver: “People feel like it’s not worth it for them to even go through it, because they also don’t even know if they’re going to be approved. It’s just a headache to deal with.”
Supports such as disability organizations or advocates connected some families to helpful information, resources, and opportunities. Yet, many parents felt stranded and disconnected, unsure of how to support their child or access needed services. Parents emphasized that people such as pediatricians should be more aware of the impact of disability for children and families, and then to be better at connecting parents with information and resources. Rachel explained,
When I think about things that create barriers, or just really make it feel like getting what your child needs is insurmountable, that’s the example that I keep going back to— that no one knows what I’m talking about. I can go to Google and find more information than I can from any of the people that are professionally engaged in her education and her care.
Loss of Supports
Many families talked about grieving the supports they had lost. Conversations about supports were replete with the caveats “before COVID . . .,” “pre-COVID . . .,” and “we used to . . .” For many, therapies, playgroups, babysitters, and other critical supports “disappeared” or “completely stopped.” Tracy, a mother of a third grader with a genetic condition and autism, felt they were “always trying to catch back up” after short breaks in school or services, and that this was far worse during the pandemic. She explained, “[The pandemic] has really highlighted how detrimental it can be when all of their services just come to a halt for an extended period of time.” Carolyn a mother of an autistic third grader, explained the impact of lost support:
Depleted. Every support system that we had was ripped out from under us . . . You feel isolated. To take away that some support [you had before the pandemic], it’s exhausting. And so, there’s many roles expected that we can’t meet. We were not superhuman. We shouldn’t have to be. And for a long time, there was no other choice but to be everything.
Although parents often talked about losing supports because of the pandemic, many also emphasized that they lost support when their child transitioned out of early childhood and into the K–12 school system. Lisa, a mother of a third grader with autism explained her experience:
[Early intervention providers] were instrumental in asking us if we wanted things that we didn’t even know really were available. So after you cross over to that mark from going from three years old and preschool to getting into school, the teachers support you, but it’s still lost. I don’t necessarily know what we should be doing for him or what I should be asking for.
Empowerment
Our second research question was concerned with family experiences of empowerment. Two themes were (a) advocacy and trust, and (b) empowerment at home.
Advocacy and Trust
Parents often talked about empowerment in light of being an advocate for their child—advocating for related service minutes, paraprofessional support, AAC devices, increased time in general education settings, and more. Nicole, a mother of a kindergartner with autism explained, “We, as parents are the main advocates for our children. And if we don’t talk or we don’t stand up for them, there’s nobody else who’s going to do it.” During the pandemic, advocacy changed for some parents. They found themselves needing to advocate for services they would have taken more for granted in other years, like in-person services and basic IEP compliance. Many parents explained the pandemic had “heightened” the way they saw themselves as an advocate for their child, such as Melissa, a mother of a kindergartner with Down syndrome who explained, “I just think it’s [advocacy] probably grown a little bit of stronger; I didn’t want my child to get lost in the chaos of everything that was taking place.” Other parents felt they had been an advocate for their child “from the day he was born,” and that the pandemic had not changed that.
Some parents navigated the advocacy process with ease. For others, advocating felt like going to battle. Parents whose advocacy yielded positive outcomes felt heard and respected, recounting that, “Our school system’s been super accessible,” “they were all open ears,” and “there was no pushback at all.” Grace, a mother of a first grader with Down syndrome recognized her daughter needed in-person therapies when they were doing virtual learning and reached out to her child’s team to discuss this: “[The SLP] goes, ‘I totally agree. Let’s add it.’ So she was on board with me.” Other parents described interactions with the school as a “fight,” anticipating they would “have to argue with someone about it every time,” and explaining that they had to be “very aggressive.” Several parents described their schools as unwilling to provide requested services, even after years of requests. Katherine, mother of a first grader with Down syndrome explained, “I’ve been asking for an evaluation since 2017 for [child] to have an [AAC] device to see if he would benefit from it. And the school was against it. They never would.”
Because of these experiences, it was clear that advocacy was closely linked with trust. Trust for some families grew as they were heard and understood by school staff—when their advocacy was met with a positive response. Others felt they did not need to be involved in every decision because they were able to trust their child’s educational team. Susan explained,
I trust that they are definitely building on the skills that he knows, and I trust them to be doing that. And I can see results of that. But I definitely don’t feel like I’m the parent who’s like. “Tell me exactly what you’re doing with him.”
Conversely, many parents experienced conflict with the school—whether during the pandemic or before—and they were distrustful. As a result, they became even more adamant that they had to be involved in every aspect of their child’s education, fearing their child would not get what they needed. Abbey, a mother of a first grader with autism and cerebral palsy, explained, “Oh, I’m very involved— whether I want to be or not sometimes.” This continual fighting left parents feeling frustrated, leading them to “run out of steam.” Rachel explained,
It becomes theater to convince school systems to just give us what we feel like we need for our child. And everyone does not have the energy for that. I don’t even have the energy for it, but I just know it’s what has to happen . . . If that’s what every parent has to do—deliver an Academy Award winning performance to get their principal to agree to have their child get an aide—there’s just a long way [to go].
At-Home Learning Experiences
Parents also talked about their confidence supporting their child’s learning at home. Day-to-day life was often challenging, especially when children were learning remotely. Parents talked about the weight of the extra responsibilities, particularly as they struggled to juggle work schedules and/or care of multiple children who were all learning virtually. Mark explained,
[The pandemic] puts more of the onus on me to make sure that she’s getting where she needs to be. And that’s stressful because both my wife and I work, so there’s limited time in our daily schedules to get to that . . . It has indicated to me that we need to do more and that’s difficult because it’s hard to find that 25th hour in the day to do more.
Despite the challenges, many parents felt the “silver lining” was that it provided them with much deeper insight into their child’s education—describing their experiences as being “eye-opening” and “building their understanding” of their child’s strengths, preferences, and abilities. Yet, others expressed that virtual learning had only increased their “guilt,” created “pressure,” and in an unwanted way, placed the “burden of education” more squarely on their shoulders.
Parents’ roles were impacted by how school played out (e.g., in-person, virtual, hybrid). Some families felt they were supporting what teachers and service providers were teaching, but others felt they had become their child’s primary or only teacher—a job they did not want or feel equipped for. They explained, “That’s not my job,” and “I’m his mom. . . . I don’t want to be his teacher.” Tracy explained: “[I] don’t feel like it’s my job to be a therapist. Because there’s a reason that people go to school for those things— I don’t know everything.”
Furthermore, even parents in similar roles still described a range of confidence levels, influenced by their own personality, experiences, and support from the school. Amanda, a mother of a second grader with Down syndrome, described the impact of coaching and feedback from her child’s therapist: “I would not be as confident if I had no outside help from someone who has studied this and worked with folks with this and had success.” Katherine explained:
We’ve had so much support that’s been helpful with the different therapies. I have just felt really empowered to do the schooling myself. I’ve learned how he learns, and I’m able to relate to him best- better than anybody else.
Association Between Supports and Empowerment
The final research question addressed how supports might be associated with families’ feelings of empowerment. We identified four case studies highlighting the ways families’ experiences with support impacted their empowerment, either as a facilitator or a barrier.
How Do Communication and Relationships with Providers Impact Experiences with Advocacy and Trust? (Lexi and Michael)
Lexi was a kindergarten student who received special education services under eligibility for autism. She lived at home with her parents and younger brother. Her mother, Olivia, described being “very satisfied” with the “respect” and “open communication” she received from all members of her child’s educational team. Olivia’s relationship with Lexi’s special education teacher was especially impactful, and she described her as a person she could go to at any time for support and encouragement. She also expressed that she had “a great family and friend support system as a whole,” who provided “reinforcement” and “positivity” for her throughout the school year. Lexi’s school district was entirely virtual for most of the 2020–2021 school year, so Olivia worked with Lexi’s team to establish a modified educational placement in which Lexi received virtual instruction in the morning and attended an in-person daycare in the afternoons. Olivia explained that she did not have to “push” to get her team to agree to this educational arrangement; they came to the decision together. For Olivia, there was a clear connection between open communication and the effectiveness of the advocacy process, explaining that “things go a lot further, faster.” Her relationship with Lexi’s team inspired her to continue to engage in advocacy on a larger scale: “I want to get into advocating, not just for myself but for other students, because I want everyone to have this kind of experience with their team.” She summarized the impact of these experiences: “I’m ecstatic with where we are and I really just want this to be like this for the next 12 years of her schooling.”
Michael was a first-grade student with autism and cerebral palsy. He had extensive medical support needs and used an AAC device to communicate. He received special education services under developmental delay and attended school in-person throughout the year. Abbey was a single mother and explained that she did not really have support from other family members, saying “it’s kind of just me and Michael most of the time.” They had recently moved to a small, rural school district after previously attending a larger school. Involvement on Michael’s educational team was a high priority for Abbey. Despite this, she felt “communication was a big issue.” She explained that it was challenging to communicate with Michael’s team because the information she received was not consistent across team members. Abbey was also “very worried” that Michael’s team did not have sufficient experience or training to provide needed supports. Furthermore, she described a lack of support outside of school since moving to this smaller community, explaining “there’s not a behavioral therapist that’ll come to this area,” and “there’s no pediatric physical therapist in this valley.” Abbey identified that Michael was making minimal progress on his IEP and was “getting a lot of injuries at school.” Although she talked with many people at his school (i.e., his teachers, therapists, the school psychologist, the special education director, and the superintendent), Abbey saw, “they just never follow through” and “the IEP is just literally not being followed.” This eventually led her to reach out to an outside advocate and to decide that Michael would repeat first grade the following year. She explained:
My hope is while we’re finishing up this semester, that by me bringing in an advocate, by us bringing in enough help, they’ll get on board. And then maybe next year– unfortunately, I hate to say it, but I’m really hoping for a better year next year, because we kind of lost a lot of this school year.
How Do Training and Resources From Providers Impact Experiences with At-Home Learning? (Macey and Connor)
Macey was a second-grade student with Down syndrome and exceptional medical needs. She lived with her mother and father, who elected to keep her home and learn remotely throughout the school year to minimize their family’s health risks. Macey’s mother, Amanda, explained that Macey’s virtual learning typically involved two 15- to 30-min instructional periods each day via videoconferencing. Most of Macey’s instruction was provided by her parents, with support from her therapists and teachers. Amanda explained: “If we were not working heavily with her, this whole ordeal [virtual learning] would have set her way back.” Amanda was clear that her and her husband’s confidence to teach Macey at home came from the guidance and encouragement they received from Macey’s educational team, saying “having the support of her therapists has been a huge help.” Amanda described the ways that Macey’s speech, occupational, and feeding therapists offered “pointers” and “tips” to implement different strategies at home, as well as how to adapt when something was not working. Amanda summarized their experience:
They [Macey’s therapists] were very good at guiding us in what we needed to work on, how to get it accomplished. If we had a concern, going, “We can’t get her to do this. We’re trying, it isn’t working,” They were a big cheerleading support system of, “No, let’s try this. Let’s back up and take baby steps.” So we’ve been given great support and advice by all the therapists, all her teachers.
Connor was a kindergarten student with Down syndrome who received special education services under the category of developmental delay. He lived at home with his parents, a younger sibling, an older sibling, and an older cousin, who his parents had custody of. His mother, Crista, opted for her children to learn remotely during the first 9 weeks of the year due to health concerns for Connor. Crista provided most of Connor’s instruction, based on resources from the school and plans she developed on her own. Crista felt confident supporting Connor’s learning at home when she received guidance or support, but she typically did not get this support. She explained: “His special education teacher just sent me home with a couple of worksheets . . . and I don’t really know what exactly I’m supposed to be doing with him.” She often felt that work sent from the school was not individualized to meet Connor’s needs, leaving her to “[try] to guess” what she should be doing. Crista explained, “it feels like I’m homeschooling.” Crista said that a saving grace was thinking back to Connor’s time with early intervention services, who had provided her with advice that she was using years later. She explained, “through [early intervention] I learned a lot of ways to make something like play educational.” Despite this, Crista was concerned that Connor would “fall behind,” and she was incredibly stressed. Ultimately, she chose to send Connor back to school in person after the first 9 weeks.
Discussion
We examined families’ experiences with empowerment and support in the midst of the COVID-19 pandemic during the 2020–2021 school year. The construct of empowerment provided a useful theoretical framework for our study because it links individual strengths and competencies (such as those of parents or family members) to each person’s surrounding social ecology (i.e., their supports), including support from professionals, friends, family, or others (Perkins & Zimmerman, 1995). Several findings extend prior knowledge related to family support, empowerment, and the ways in which these are connected for students with extensive supports needs and complex communication needs.
First, families’ experiences varied widely. To a great extent, the differences in school experiences reflect similar variations described in the broader literature. Schools and districts across the United States approached teaching and learning during the COVID-19 pandemic in varied ways, leading to widening challenges for children already most at risk, such as students with disabilities (Averett, 2021; Oster et al., 2021). For families in this study, virtual learning and the inconsistencies of schooling during the pandemic were filled with challenges. Other researchers have examined challenges during emergency remote learning in Spring of 2020 (Averett, 2021; Neece et al., 2020), but our findings indicate clearly that these persisted into the 2020–2021 school year, especially for families with students with complex communication needs. Supports made a difference for some families, but many struggled, feeling alone and overwhelmed. As illustrated in the case examples (i.e., Lexi, Michael, Macey, Connor), families in similar educational situations (e.g., in-person or virtual learning) had vastly different experiences with support, profoundly impacting their feelings of empowerment and well-being.
Second, families were impacted differentially by whether they felt a loss of supports. As might be expected, many parents felt depleted when supports disappeared during the pandemic. Yet, we were more surprised by how many families addressed losing supports as their children moved from early childhood special education to elementary school, particularly since this was not a focus of the study. Taking the findings of this study in conjunction with prior literature, the rippling effect that these losses create is clear: Families’ supports make a difference for their overall well-being, including related to stress and resilience (see Burke & Hodapp, 2014; Zhao et al., 2021) and empowerment (Burke et al., 2020). Efforts are clearly needed to address the loss of support resulting from the pandemic, as well as when families enter elementary school years.
Third, findings from this study underscored that supports from teachers and other providers matter deeply, including for parents to feel empowered to support their child through their advocacy and in their child’s learning at home. Support from professionals was especially helpful when it was based on quality communication, meaningful relationships, and trust. Although these qualities and practices are likely valued by most families with children with IDD, families in this study highlighted the had special importance because their children had complex communication needs, saying things like “My kid can’t tell me, so I need you to tell me” (Carly). Prior research has shown that advocacy is stressful for families, but that support from schools can help families feel more empowered as advocates for their children (Burke et al., 2020; Burke & Hodapp, 2014; Rios et al., 2021). Findings from the current study provide further insight into how and why such supports might make a difference: When providers establish strong relationships with families and pave the way for open, high-quality communication, this can build trust for families as they navigate the advocacy process. This may be especially impactful for parents of students with extensive support needs because they have to navigate relationships with a myriad of teachers and related service providers.
Limitations and Future Research
This study had limitations. First, participants overrepresented White, upper-middle class families and underrepresented families from diverse racial/ethnic, linguistic, and socioeconomic backgrounds. As significant disparities have emerged throughout the pandemic related to race and socioeconomic status, it is likely that a more representative sample may have yielded an even wider range of experiences (Colvin et al., 2022; Oster et al., 2021). Similarly, most children had a diagnosis of Down syndrome or autism, and all had complex communication needs. Families with children with other disabilities or types of support needs may have had different experiences. Second, we gained insight into families’ experiences by collecting data across three time points during the 2020–2021 school year—far more than we would have if we had only collected data at one time point. Yet, our study was not truly longitudinal because we did not focus on analyzing patterns of change over time. Although we anticipated we would be able to look longitudinally at how families’ experiences played out as the school year progressed, we were not able to do this because experiences varied from time point to time point within and across participants, seemingly tied to pandemic-related issues (e.g., pandemic “waves,” policy changes, remote/hybrid/in-person learning). Therefore, this study provides a rich snapshot of the 2020–2021 school year but is not truly longitudinal. Third, although we engaged in informal member-checking with participants across time points, we did not conduct formal member-checking. This study also only included data from interviews, rather than multiple sources, so we could not triangulate findings across sources. Finally, while our use of example cases provided the opportunity to illustrate the unique experiences of families in this study, this approach differs from both standard across-case qualitative description and from case study methodology.
This study provides insight into the experiences of families of children with extensive supports needs during the COVID-19 pandemic, revealing stark differences in services and outcomes for these families. Further research should seek to more clearly understand disparities for families and children with extensive supports needs coming out of the COVID-19 pandemic, with an emphasis on identifying means to provide equitable supports and services—both now and in the future. Results also point to the significant role that teachers and providers can play for helping families feel empowered as their child’s advocate and in supporting their child’s learning at home. Further research should explore how to effectively support and train teachers to implement family-centered practices and partner well with families, particularly after students have exited early intervention and early childhood special education.
Implications for Practice
The stories shared by families provide a powerful message about the impact professionals have—both positive and negative. Parents valued an open, reciprocal relationship with their child’s educators and service providers where their expertise was respected, and where trust was built over time. Trust seemed to be especially strengthened when families could see clear evidence that professionals would do what it takes to support their child well. One of the important findings was that many of the factors that contributed families feeling empowered (both at home and their advocacy) were actually things about the family–professional relationship that were established well before the COVID-19 pandemic, such as trust in providers, strong communication and support, and providers who actually listened and valued the perspectives of parents (Burke et al., 2020; Burke & Hodapp, 2014). When students have complex communication needs, communication, support, and trust from teachers is especially important to parents, because they are reliant on educators to provide crucial information about their child’s day to day experiences at school when their children cannot share this information themselves.
Thus, the findings of this study provide further impetus that educators and service providers need to have the attitudes, skills, and resources that help them build strong partnerships with family members (Hsiao et al., 2018)—in emergency situations like the COVID-19 pandemic, but also beyond. This has practical implications for the ways that school and district leaders build the capacity of their staff, but also for pre-service teacher preparation. Educators and service providers need more than surface-level understanding that family–school partnerships are important. They need to develop confidence—and have the time and resources—to use practices that build trusting partnerships with families, including holding strong views about the strengths of diverse families, implementing strong home-school communication, and using culturally responsive communication strategies that emphasize listening to and understanding families (Grant & Ray, 2018). As professionals and policy makers consider how to improve outcomes for families of students with extensive supports—including but not limited to emergency situations like the pandemic—they should examine opportunities to build up more robust and ongoing systems of support around teachers and providers themselves.
As a final practical takeaway, we think it is important that educators and other service providers remember that families have been impacted by the pandemic and the support that they either had or did not have during this difficult time. We anticipate that families will carry these experiences with them into future interactions with teachers and service providers. For some families, remote learning opened a window of insight into their child’s schooling, and they felt their confidence increase as they observed classes and therapy sessions through videoconferencing and directly supported their child’s learning at home. Yet for many, the pandemic aggravated challenges and increased stress related to their child’s learning. Teachers and service providers should seek to understand these histories for the families they serve so they can build or re-build trust effectively. Successful partnerships with families will have a far-reaching impact to help families feel and be empowered, ultimately supporting strong outcomes for children with extensive support needs and complex communication needs.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research was made possible by a special COVID-19 grant from the Spencer Foundation (#202100017).
Editor-in-Charge: Robert C. Pennington