
Abstract
Purpose
The disproportionate impact of COVID-19 on racial/ethnic minority groups in the United States was recognized early in the pandemic (Graff et al., 2021). African American, Latino, and American Indian/Alaska Native children and youth had a higher risk of infection and more severe disease compared with White children and youth (Magesh et al., 2021). Racial/ethnic minority families were also more likely to experience adverse socioeconomic effects of the pandemic (Ambrose, 2020). Among racial/ethnic minority groups, immigrants were at particular risk of experiencing COVID-19 disparities (Clark et al., 2020; Islamoska et al., 2022). Latinos are the largest group of immigrants in the US, comprising around half of US immigrants (Batalova et al., 2021; Budiman et al., 2020). COVID-19 disparities among immigrants have been attributed to a concentration of immigrant workers in front-line essential workforce employment and in jobs with limited benefits that prevented or decreased the ability of immigrant workers to take time off from work due to illness or exposure (Faghri et al., 2021; Graff et al., 2021; Horner et al., 2022). Language barriers to accessing information about COVID-19 and health services related to diagnosis and treatment of COVID-19 infections may have also played a role (Cohen-Cline et al.; Otto et al., 2021).
COVID-19 disparities stemmed from long-standing structural inequities for racial/ethnic minority, immigrant, and low-income populations in the US (Khanijahani et al., 2021). The need for awareness and proactive policy changes to address social determinants of health and their impact during pandemics has been widely discussed when evaluating lessons learned from the COVID-19 pandemic (Perkins et al., 2021; Singu et al., 2020). Little is known, however, about the experiences of immigrant families with children who had COVID-19 during the pandemic. This information is needed to improve the public health response in future pandemics and to develop programs and policies that address longstanding inequities in health and opportunity for immigrant families exacerbated by the pandemic. Thus, the purpose of this mixed methods study
Methods
Study Design and Data Sources
We conducted a mixed-methods study utilizing the following data sources: 1) Surveys of parents/legal guardians (hereafter referred to as parents) of a child with a positive SARS-CoV-2 test resulted at Children's Hospital Colorado (CHCO) that included parent perspectives on factors contributing to and outcomes resulting from pediatric COVID-19 infection; and 2) Focus groups with Latino immigrant adults to explore their perceptions of the causes of COVID-19 disparities for Latino immigrant families compared with US-born families. The development of survey content and focus group discussion topics was guided by the social-ecological model (Centers for Disease Control, 2022b). We describe our study population as immigrant families in this study based on the established definition that an immigrant family includes at least one internationally-born parent (Martin et al., 2023). Study activities were approved by the Colorado Multiple Institutional Review Board.
Parent Surveys
Data Collection
The survey sample was drawn from the data repository for the Children and COVID-19 in Colorado (CCC) Study at CHCO Health System which includes a network of hospitals, emergency departments, and outpatient care centers serving approximately 280,000 unique patients each year. The CCC study has been previously described elsewhere (Graff et al., 2021). The survey sampling frame included patients <18 years of age identified with SARS-CoV-2 via molecular test March-December 2020. A list stratified by ethnicity (Latino vs. Non-Latino) was generated in random order by month. The list combined March and April as SARS-CoV-2 testing became available during the last week of March 2020 at CHCO. We then sequentially contacted the primary caregiver listed in the medical record from the randomly generated list for each of the 9 months with the aim of achieving a 2:1 ratio of Latino vs. non-Latino participants in each month sampled with a goal of 75–100 surveys based on survey funding and timeline feasibility The oversampling of Latino participants was determined a priori based on emerging evidence of COVID-19 disparities among Latino populations. Insufficient data were available for power and sample size calculations given the rapidly evolving nature of the COVID-19 pandemic. A study research assistant completed up to three phone, text, or email contacts to each caregiver until 10–12 participants were recruited per month. Participants were offered to complete the survey in English or Spanish. Participants who could not complete the survey in English or Spanish were excluded. Surveys were orally-administered by phone by a trained research assistant fluent in both English and Spanish and responses entered directly into REDCap (Harris et al., 2009). Surveys were conducted between January and August 2021 and participants received $20 remuneration.
Measures
The survey assessed illness of household members at the time of the child's positive SARS-CoV-2 test, activities of the child and household members, COVID-19 mitigation practices in the household, sources of COVID-19 information and COVID-19 vaccination intention. We also collected family sociodemographic information, including parent nativity (US-born vs. immigrant) parent gender, educational attainment, parent health literacy using a validated single question (Chew et al., 2008; Sarkar et al., 2011), employment status and type, household income, household economic and food insecurity, access to household car, home internet access, self-efficacy related to web-based health information, primary home language, parent English proficiency via US Census Bureau question (Deitrich & Hernandez, 2022), child age, child nativity, and child usual source of healthcare. Economic insecurity was assessed using a question based on the National Academy of Medicine recommended question for healthcare assessment of financial strain (Adler & Stead, 2015). Food insecurity was assessed based on reports of increasing pandemic-related food insecurity using one of the Hunger Vital Signs questions (Hager et al., 2010). Self-efficacy related to web-based health information was assessed because of the rapid proliferation of online COVID-19 information/misinformation using a question used in prior research on information and communication technology use in low-income populations (Chilukuri et al., 2015).
Community Focus Groups
We partnered with two immigrant Latino-serving community organizations, Aurora Community Connection and Amigos de México, to conduct Spanish-language focus group discussions. The partnering community organizations recruited participants from among members of advisory groups and/or other organization programming via text message, social media groups or in-person contact. Focus group participants were recruited separately from survey participants, and we did not include survey participants in focus groups. Community organizations received a stipend for their recruitment efforts and space provision. Focus group discussion guide topics included: 1) perspectives on the reasons for COVID-19 disparities among Latino populations); 2) perspectives on the COVID-19 vaccines for adults and children and reasons for then-emerging disparities in vaccine uptake for Latino populations; 3) perspectives on potential return to in-person school, and 4) perspectives on possible long-term effects of the COVID-19 pandemic on the Latino community and strategies to reduce negative impact. The focus group guide can be found in Appendix 1. One focus group was conducted virtually using the Zoom virtual meeting platform and two focus groups were conducted in person. Each focus group was moderated by one of the study investigators (LRD) (bilingual in English and Spanish) and a bilingual English/Spanish research assistant (VV or SL). At the beginning of each focus group session the study purpose, risks, benefits, processes for maintaining data confidentiality and the expectation of participants to not share information discussed during the group were explained and any questions answered. Participants could elect not to continue, though none did. Consent was not documented as the study was granted a waiver of documentation of informed consent. Focus groups lasted between 60 and 90 min and participants were remunerated $30. Digital focus group recordings were transcribed and translated by a commercial transcription company and de-identified prior to analysis.
Analysis
Quantitative Analysis
We compared household COVID-19 experiences, use of mitigation measures, vaccine intention and sociodemographic information between participants stratified by nativity (US-born vs. immigrant) using Chi-square and Fisher's exact test for categorical variables and t-test for continuous variables. A preliminary review of quantitative data demonstrating that characteristics of immigrant parents were similar to those of Latino immigrant parents resulted in the decision to stratify analysis by parent nativity rather than by Latino vs. non-Latino ethnicity.
Qualitative Analysis
Qualitative data analysis was completed using the online qualitative analytics program Dedoose (Dedoose). Both coders (LRD, ST) reviewed all transcripts to develop preliminary codes and then used an iterative consensus process to determine a clear definition of codes and consistent application by both coders. During initial development and use of the codebook, one transcript was coded by both coders. The remaining transcripts had one primary coder and a secondary verification coder. We used established methods for addressing differences in coding due to multiple coders by addressing all coding discrepancies and reconciling them with discussion and consensus (Patton, 2015). Member checking was completed with leaders of partnering community organizations via a summary of focus group findings which they provided written feedback on or discussed with a study investigator (LRD); no changes to analytic findings were requested. Trustworthiness of the data is supported by the member checking, use of an audit trail whereby data were checked and rechecked through data collection and analysis, our use of a clear coding schema with a verification coder for each transcript, and review of analysis and interpretation by study team members who were not involved in the qualitative coding and analysis.
Results
Quantitative Data
Of the 260 potential parent participants contacted, 78 completed the survey. Among survey respondents, 55% were US-born and 45% were immigrants. Characteristics of the surveyed parent, their family, and the index child are included in Table 1. Notable differences between the two groups included that immigrant respondents reported higher food insecurity, lower income, and lower levels of education. Immigrant respondents were also more likely to be at risk of limited health literacy (28.6% vs 0%, p = 0.0001).
Demographics and Characteristics of Survey Respondents.
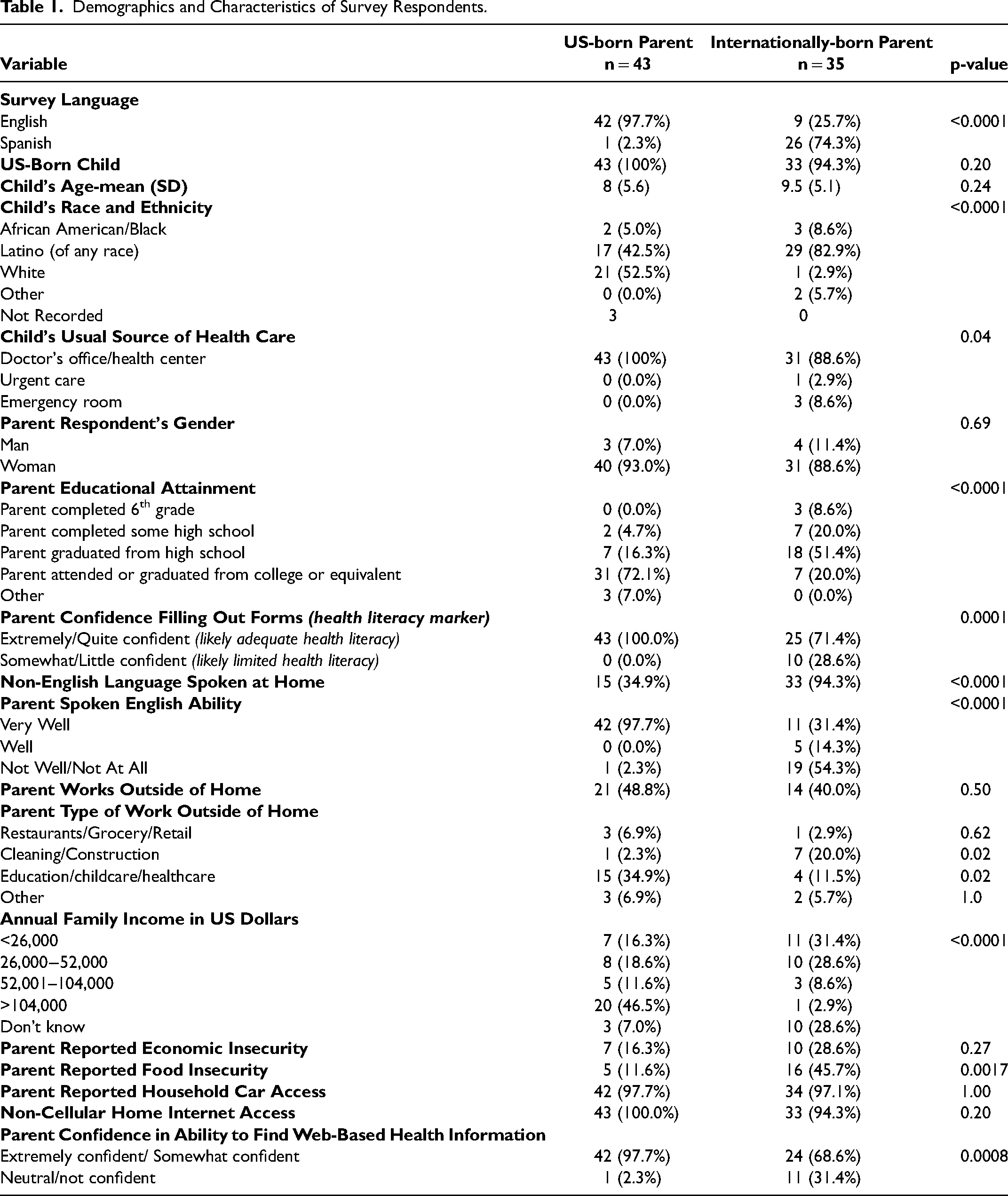
Table 2 displays information regarding families’ COVID-19 experiences and beliefs. There was no difference in the number of data sources used for COVID-19 information by nativity; however, immigrant respondents were less likely to indicate health care providers (37.1% vs 72.1%, p = 0.0028) or the Health Department (37.1% vs 72.1%, p = 0.0028) as information sources. Immigrant respondents were less likely to report that their children participated in activities outside the home (0% vs 16.3%, p = 0.01) and less likely to report travel outside the state in the two weeks prior to the child's positive SARS-CoV-2 test (0% vs 23.1%, p = 0.002), while simultaneously being more likely to report working outside the home (85.7% vs 60.5%, p = 0.01). We found no difference in COVID-19 vaccination intention by parent nativity.
COVID-19 Knowledge and Impact on Survey Respondents.
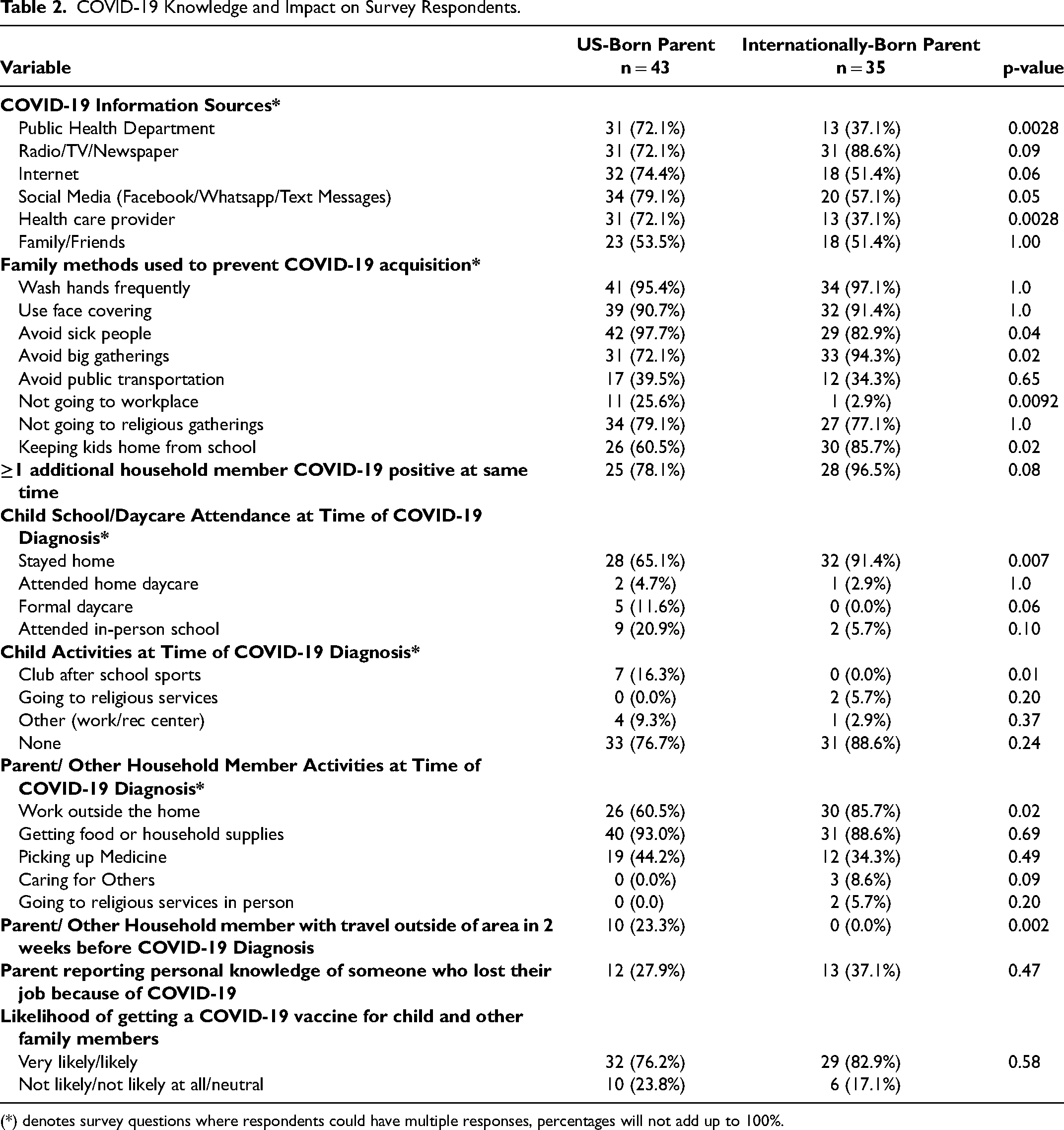
(*) denotes survey questions where respondents could have multiple responses, percentages will not add up to 100%.
Qualitative Data
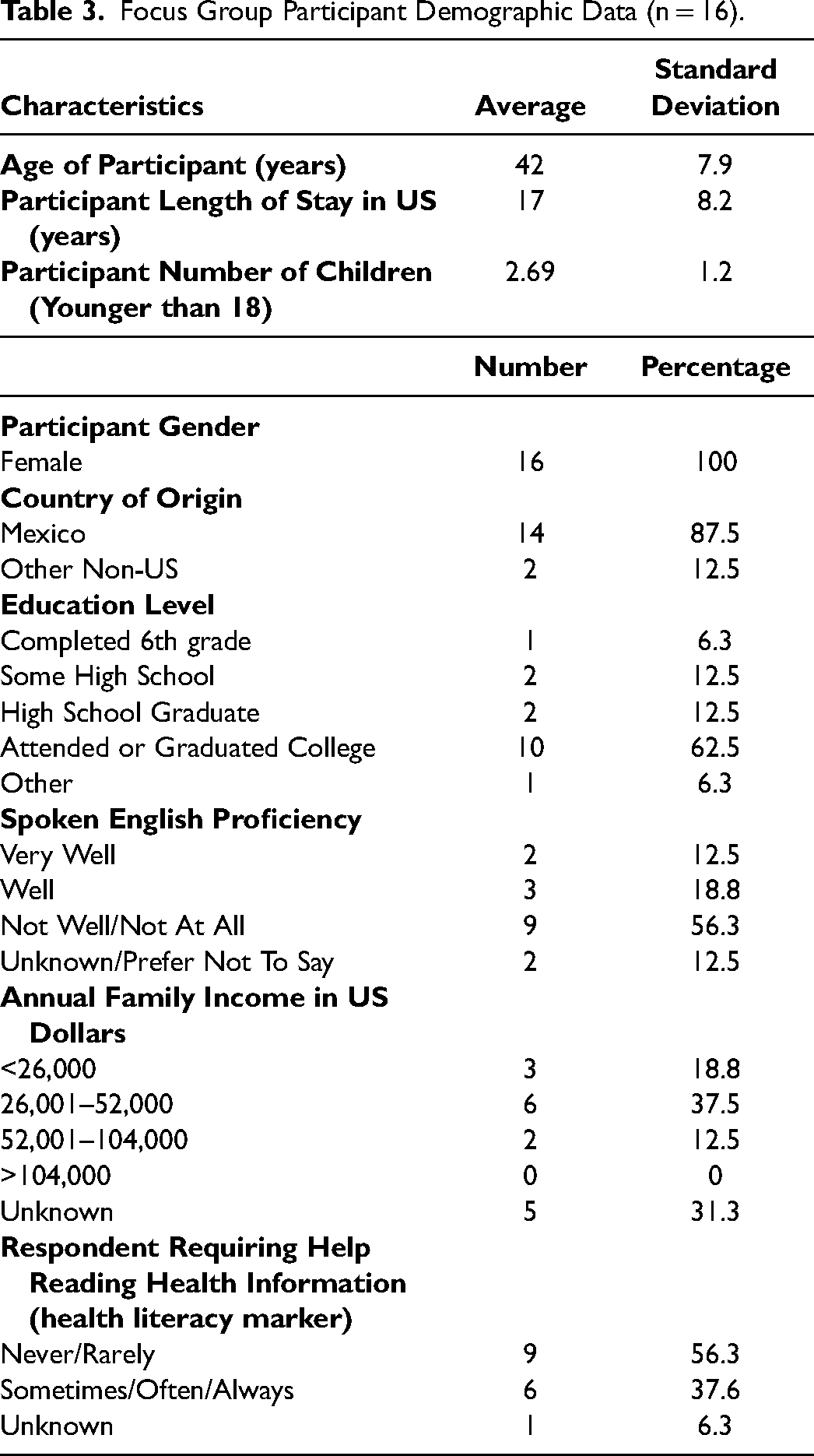
Table 3 displays characteristics of the 16 focus group participants. We identified three themes related to the disproportionate impact of COVID-19 on Latino communities: 1) interplay of COVID-19, work and financial stress; 2) the challenge of information access and discerning misinformation; and 3) the acute and chronic social impacts of COVID-19. Table 4 displays sample quotes for each theme.
Focus Group Participant Demographic Data (n = 16).
Example Focus Group Quotations From Latina Focus Group Participants by Theme.

Theme One: Interplay of COVID-19, Work and Financial Stress
Participants noted that both the need to work outside the home and disparate working conditions contributed to COVID-19 transmission in their families and communities. A common story was household COVID-19 illness that resulted from one adult member of the household contracting COVID-19 at work and then spreading it to others in the home (Quote 1). Participants noted that early in the pandemic many Latinos had jobs that were “essential” and required work outside the home while many other jobs were either suspended or moved to remote settings. Participants described a recognition that the risk of viral transmission in the workplace was high but working outside the home was critical to affording housing, food and utilities (Quotes 2–4). They reported if one took time off work due to illness, this resulted in family economic precarity due to missed wages (Quote 4). Workers could be fired for not presenting to work even during outbreaks (Quote 5) and participants reported working even when feeling ill out of this fear (Quote 6). The financial cost of illness in a family was extensive; the loss of work and loss of pay compounded by the fear of healthcare costs associated with COVID-19 illness led many to delay seeking healthcare (Quotes 7–9). Furthermore, a lack of time off for vaccination and fear of vaccine side effects preventing adults from working were identified as key contributors to vaccine hesitancy (Quotes 10, 11).
Focus group participants highlighted the increased challenges facing immigrant Latinos, specifically. Participants reported a lack of eligibility for financial assistance programs to recoup lost wages for illness/quarantine and difficulty accessing financial or other support resources (Quotes 12, 13), which increased household financial stress. Participants also noted that immigrant community members feared exposing their lack of legal authorization to work in US through COVID-19 vaccination and thus elected not to get vaccinated (Quote 14, 15).
Finally, though participants noted many challenges related to work and household finances, they also discussed how the community adapted to confront these challenges. Participants focused on community-led vaccination efforts as an example. Participants noted that there was an emphasis on conducting vaccine events in the evenings and on weekends when workers may be able to attend and engaging workplace leaders to help workers access vaccine events (Quote 17).
Theme Two: The Challenge of Information Access and Discerning Misinformation
Participants endorsed that a lack of access to accurate information contributed to COVID-19 disparities as it was difficult to obtain information in a language that they could understand from a trusted source (Quote 17). Participants described relying on information from their social network which included both local and international friends and relatives, even if it was bad information (Quotes 18, 19). They reported that social media information was likely to be misinformation, but the assumption that all online information was misinformation may have resulted in missed opportunities when important information (e.g., when vaccine fair advertisements were shared) (Quote 20). As the pandemic progressed, participants cited that local leaders, from politicians to family physicians to religious leaders, were important information sources (Quotes 21- 23). Many participants commented on the value of state politicians providing information in their native language, endorsing the perceived trustworthiness of this messaging (Quotes 24, 25). Local leaders, as with social networks, sometimes provided conflicting information which made it challenging for families to make decisions related to COVID-19 mitigation practices and vaccination. Participants provided examples of physicians both encouraging and discouraging COVID-19 vaccination (Quotes 26, 27) and some religious leaders acting as advocates of COVID-19 precautions and vaccines, while others spoke out against these (Quotes 28, 29).
The reliance on social networks increased opportunities for misinformation which participants felt may have contributed to adverse COVID-19 outcomes among community members (Quotes 23, 30). Though social media was the source of much misinformation, it was further propagated through personal interactions, such as phone calls with family (Quotes 31, 32). Participants discussed general misinformation, but there was also a significant focus on vaccine misinformation. Vaccination misinformation was perceived to be made worse by social network anecdotes about differences in government vaccination efforts between the US and other nations (Quote 33). Despite misinformation and barriers to vaccine access, there were also clear examples of successful vaccination efforts and transmission of reliable COVID-19 information (Quote 34).
Theme Three: The Acute and Chronic Social Impacts of COVID-19
Participants noted that impacts of the pandemic extended far beyond the virus’ illness course, causing massive disruptions to the lives of individuals and society. Many participants described that the support of family was a core part of their day-to-day life and recommendations to restrict gathering outside of the household unit were hard to follow (Quotes 35, 36). Participants believed that ongoing gatherings within the Latino community despite social distancing recommendations contributed to the spread of COVID-19, especially early in the pandemic (Quotes 37, 38). Many participants emphasized particular pandemic impacts on children including canceled activities, struggles with online schooling, and worsening child mental health (Quotes 39, 40). Participants expressed concerns about canceled or virtual-only developmental support services having long-term impacts on children's development (Quote 41). Despite improvements in virtual service availability during the pandemic, participants spoke of challenges accessing these services (Quote 42).
Though focus group discussions highlighted many challenges, participants provided several examples of resilience to the social impacts of the pandemic. Participants described Latino-serving community organizations that pivoted to develop specific community care programs to support families who were ill and unable to obtain groceries or other essential supplies and that provided mental health and financial support (Quotes 43, 44). Participants also spoke of the efforts they took as a family to find safe activities to do with their children to support their mental health and healthy development (Quotes 45–46). In addition, participants underscored the resilience and adaptability of children as evidenced by their success in returning to school in masks and enduring vaccination (Quotes 47–49).
Discussion
This study fills gaps in our understanding of how immigrant families with children experienced the pandemic and what factors may have contributed to disparities, particularly early in the pandemic. Findings from quantitative data analysis comparing experiences between immigrant and US-born parents to identify distinct experiences among immigrant parents were reinforced by the qualitative analysis including: lower socio-economic status and higher employment in essential services requiring continued work outside the home during the pandemic, thereby increasing the risk of infection and spread in immigrant families; and higher risk of limited information access related to language barriers and prevalent misinformation. We found no difference in vaccine acceptance between immigrant and non-immigrant families; however, access to culturally-tailored vaccine information in the preferred language and the need to accommodate work schedules hampered vaccine uptake. Overall, findings from our study and participants’ reflections show that the pandemic will have long-term impacts on Latino and other immigrant communities by exacerbating pre-existing disparities. While aspects of resiliency among immigrant families are encouraging, future public health emergencies are likely to continue to have a disproportionate negative impact on immigrant families if there are not investments in public health directed specifically toward these communities.
Our study identified a clear link between work and COVID-19 disparities for immigrant populations. Others have reported an overrepresentation of immigrants in public facing, essential services and high-risk work environments during public shutdowns early in the pandemic (Macias Gil et al., 2020; Đoàn et al., 2021). Compounding the risk of infection in these work environments was the fear of lost wages or a lost job if a worker did not present when ill with little recourse if the worker was undocumented. Financial support resources and broadened eligibility for social services were instituted to address unprecedented domestic need in the wake of the COVID-19 pandemic. These resources, including increases in unemployment and Supplemental Nutrition Assistance Program benefits, as well as rent assistance and eviction moratoriums, were vital in the efforts to combat the spread and impact of the pandemic (Banerjee & Zipperer, 2022; Ingold, 2022; Rees-Jones et al., 2022). However, focus group participants discussed that these resources, meant to help the most in need, were often unavailable to at-risk immigrant populations due to eligibility restrictions. These findings are consistent with other studies showing that lack of access to pandemic-associated social safety net program may have further compounded the disparate impact of the pandemic on immigrant families (Clark et al., 2020; Đoàn et al., 2021).
A lack of official non-English language information, compounded by an abundance of misinformation, likely contributed to COVID-19-related disparities among immigrant communities. While organizations such as the Centers for Disease Control (CDC) began releasing information on COVID-19 in non-English languages in the early months of the pandemic, findings from our study indicate that these resources may have been under-utilized by local public health agencies and/or not frequently accessed by immigrant families (Centers for Disease Control, 2022a). Though these materials may have been helpful to some degree if disseminated, CDC materials lack locally-tailored information on testing, vaccination and other community-specific resource support, thus improved dissemination would not have addressed all disparities in information access. Our findings demonstrated no significant differences in the number of information sources utilized by parent nativity indicating that both populations were eager to seek out COVID-19-related information. Focus group findings revealed significant difficulty identifying locally-relevant COVID-19 information in their language from reputable sources, such as the health department. Focus group participants, however, highlighted that Spanish-language information from the state's governor was particularly valued and trusted. The discussion on the value of this information is somewhat in contrast to the expectation that information dissemination should prioritize information via local community members. Thus, our findings may indicate that a variety of information sources from local community members to respected public officials with a consistent message would be most impactful in promoting desired public health behaviors.
Information barriers were particularly salient to COVID-19 vaccination. In our survey, we found no difference in COVID-19 vaccination intention between immigrant and US-born respondents. Colorado, however, had one of the widest disparities in COVID-19 vaccine uptake for Latinos (Ndugga et al., 2022). The disparities in Colorado were attributed, at least in part, to difficulty reaching immigrant Latino populations, as this was a common across the country (Demeke et al., 2023; Ingold, 2022). Focus group respondents enumerated many vaccination barriers. They cited misinformation and mistrust of the vaccine, but also barriers related to work schedules and immigration status. Vaccine misinformation was not limited to social media or social networks, but also stemmed from religious leaders and even physicians. The mixed influence of political and social leaders and physicians on COVID-19 vaccine uptake is well-documented and affected non-immigrant populations as well (Rivas-de-Roca & Pérez-Curiel, 2023). Given this, it is not entirely clear why disparities for Latino populations were so pronounced in Colorado, but perhaps there was a synergistic effect between particular logistical barriers for immigrant Latinos and misinformation.
Finally, our study provides important information on how the impact of the COVID-19 pandemic on immigrant families extended beyond COVID-19 morbidity and mortality. Focus group participants pointed to significant concern about the mental health effects for children, particularly the impact of isolation. Immigrant parents were more likely to report work outside of the home, but their children were less likely to attend in-person school or other activities. Taken with the findings related to the necessity of work outside the home this suggests that immigrant families may have been more likely to isolate their children to limit COVID-19 exposures and protect household working adults. These family decisions may have increased the negative mental health impacts of the pandemic. Immigrant families may also have had limited access to in-person services for their children. As the pandemic progressed, return to in person education occurred more rapidly in the non-Hispanic white population, than among minority children (Oster et al., 2021). Multiple studies point towards the benefits of in-person education compared with remote learning and the substantial negative impact of the closure of school and other public activities on children already experiencing poverty and systemic disadvantage (White et al., 2021).
Our study has several possible limitations. First, participants in the quantitative portion of this study were recruited from among patients with a positive SARS-CoV-2 test at one health system which may have biased our results, as some immigrant populations may not have accessed testing at the study health system. Early in the pandemic, however, the health system was among a limited number of sites in the region performing pediatric SARS-CoV-2 tests. Second, focus groups included only Latino immigrant parents whose child was not required to have had with a past SARS-CoV-2 infection, though all participants talked about COVID-19 illness experiences. Latinos are the largest immigrant group in the US, locally and nationally, but their experiences may be distinct from those of other immigrant groups. Survey findings included immigrant groups other than Latinos, Latino survey participants were not included in focus groups, and we did not conduct focus groups with US-born parents. Thus, this may have affected the inferences made between the quantitative and qualitative data. Lastly, it should be noted that given the timing of these conversations, focus group participants were interested in having further discussion around the then newly available vaccines for COVID-19. The impact of vaccinations on work, the explosion of misinformation surrounding COVID-19 vaccines, and the role that these vaccines had socially, both as a mechanism of lifting restrictions and as an increasingly political statement, could not be disentangled from any discussion regarding the distinct impact of COVID-19 on Latino communities.
Conclusion
Overall, we identified several factors contributing to the disproportionate impact of the COVID-19 pandemic on immigrant families, including the need to work outside the home, precarious socioeconomic status, language barriers, and lower health literacy combined with abundant misinformation. These factors likely exacerbated existing vulnerabilities and worked synergistically to compound the COVID-19 exposure risk and COVID-19 impact in immigrant communities. Our study also identifies important points of resiliency in immigrant families during the pandemic and high vaccine intention. In conclusion, avoiding exacerbation of disparities in the next public health emergency requires focused investments in policies and approaches specifically directed at immigrant communities. These efforts must include a significant focus on the largest immigrant community in the US, Latino immigrants, but should also be inclusive of the many additional immigrant communities who face similar risks of pandemic impacts.
Footnotes
Acknowledgements
We acknowledge the time and efforts of the leaders and staff of Aurora Community Connection and Amigos de México in coordinating the focus groups. We thank all of the participants for their time and contribution to this study.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by institutional funds from the Children's Hospital Colorado Research Institute's COVID-19 Child Health Research Award.