
Abstract
Introduction
Studies have reported higher infection and mortality rates from coronavirus disease 2019 (COVID-19) for disadvantaged groups in the U.S. population. However, racial and ethnic differences in fatality rates, which measure deaths among those infected, are not as clear.
Objectives
The objectives were to (1) estimate the fatality rate after COVID-19 infection by racial and ethnic groups and (2) determine the extent preexisting health conditions account for differences in fatality rate between the racial and ethnic groups.
Methods
Data for all adults aged 18 and older (n = 24,834) who had a confirmed COVID-19 infection captured in the electronic health records (EHRs) of a major health care organization (HCO) from the beginning of the pandemic to March 28, 2021 were used to estimate the fatality rates for three racial and ethnic groups: Hispanic, non-Hispanic African American, and non-Hispanic White. Elixhauser's comorbidity index was calculated using the enhanced ICD-9-CM and the ICD-10 diagnosis codes. Logistic regression models were used to compare differences in fatality between racial and ethnic groups. Odds ratios and 95% confidence intervals were reported for all models.
Results
The age-specific fatality rates non-Hispanic White, non-Hispanic African American, and Hispanic groups were 0.23%, 1.05%, 0.55% for age group 18–59 years old; 2.44%, 4.50%, 5.28% for 60–69; 5.42%, 10.11%, 8.49% for 70–79, and 17.33%, 20.79%, 20.39% for 80–90. After adjusting for age, sex, and preexisting conditions, the fatality risk remains significantly higher for non-Hispanic African American (adjusted odds ratio [adj. OR] = 1.85, 95% CI 1.41–2.44) and Hispanic individuals (adj. OR = 1.91, 95% CI = 1.53–2.39) compared to non-Hispanic White individuals.
Conclusion
Hispanic and non-Hispanic African American individuals have a higher risk of fatality from COVID-19 compared to non-Hispanic White individuals. The higher risk remains after adjusting for sex, age, and preexisting conditions. Health care providers could help to increase vaccination rates in these vulnerable populations by addressing the social and cultural barriers with their patients.
The World Health Organization declared the coronavirus disease 2019 (COVID-19) a global pandemic on March 11, 2020 (World Health Organization, 2020). The first reported case of COVID-19 in Washington State was on January 19, 2020. Cases have since spread throughout the United States, reaching over 39 million cases as of August 2021 (Centers for Disease Control and Prevention, 2021).
A study using electronic health records (EHRs) of a large health care system that covering California, Oregon, and Washington examined almost 600,000 patients who tested for COVID-19 between March 1 and December 31, 2020, found Hispanics had a statistically significant higher risk of in-hospital mortality than non-Hispanic White, with adjusted odds ratio (adj. OR) of 1.41 (Dai et al., 2021). They also reported higher, but not statistically significant, mortality risk for Black (adj. OR = 1.05), Native Hawaiian/Pacific Islander (adj. OR = 1.17), American Indian/Alaskan Native (adj. OR = 1.92), Other race/ethnicity (adj. OR = 1.09), and Unknown Race (adj. OR = 1.01). The estimated mortality risk was lower for Asian compared to non-Hispanic White, but again the difference was not statistically significant (adj. OR = 0.93).
In a separate study, Acosta et al. (2021) used data from the U.S. Centers for Disease Control and Prevention (CDC) COVID-19-Associated Hospitalization Surveillance Network (COVID-NET) to examine racial/ethnic disparities in rates of hospitalization, ICU admission, and in-hospital death from March 2020 to February 2021. COVID-Net is a catchment area of 99 counties in 14 states that included California, Colorado, Connecticut, Georgia, Iowa, Maryland, Michigan, Minnesota, New Mexico, New York, Ohio, Oregon, Tennessee, and Utah. The study conducted detailed medical record abstraction for 25,281 hospitalized patients and found the age-adjusted “death rates were highest among American Indian or Alaska Native (AIAN) persons, followed by Latino and Black persons” (Acosta et al., 2021). The cumulative age-adjusted death rate ratios (adj. RR) were significantly higher for AIAN (adj. RR = 7.19), Asian or Pacific Islander (adj. RR = 1.64), Black (adj. RR = 2.58), and Latino (adj. RR = 3.85) compared to White.
Similarly, Laurencin et al. (2021) used data from the Connecticut State Department of Public Health to investigate differences in COVID-19-Associated death rates among Blacks, Hispanics, and Whites from March 1, 2020 to February 28, 2021. The study calculated monthly age-adjusted mortality rates and found significantly higher rates for Blacks compared to Whites that decreased over the course of the pandemic. The age-adjusted mortality rates ratios for Blacks compared to Whites were 2.93, 2.80, 1.77, 1.62, and 1.60 in March, May, August, November 2020, and February 2021, respectively. The pattern over time was not as clear for Hispanics. The age-adjusted mortality rates ratios for Hispanics compared to Whites were 1.25, 1.66, 5.03, 1.56, and 2.54 in March, May, August, November 2020, and February 2021, respectively.
In Texas, the first presumptive case of COVID-19 occurred on March 4, 2020, in Fort Bend County (Texas Health and Human Services, 2021). A week later, 22 cases were reported in the state (Texas Health and Human Services, 2021). On March 16, 2020, the first death related to COVID-19 occurred in Matagorda County (Texas Health and Human Services, 2021). By the end of March 2020, stay-at-home orders began, social distancing was mandated, and travel quarantines were imposed (Svitek, 2020). Within a year, the virus has spread to all 254 Texas counties; even rural counties were not spared from COVID-19 fatality (Texas Health and Human Services, 2021). As of December 18, 2021, at least 3.6 million cases of COVID-19 have been confirmed and almost 80,000 deaths have occurred in Texas. (Texas Health and Human Services, 2021).
The pandemic has hit minority communities the hardest. In the Texas Rio Grande Valley region, which has 90% Latinx individuals, mortality rates were two times higher than statewide rates (Solomon, 2020). The mortality rate findings are consistent with earlier findings from New York City that reported a two times higher age-adjusted mortality rate for Hispanic/Latinx individuals compared to non-Hispanic White individuals (Macias Gil et al., 2020). Likewise, African American individuals have had higher infection rates and deaths (Alcendor, 2020). The infection rate was three times higher, and deaths were almost six times higher in non-Hispanic African Americans than non-Hispanic Whites (Alcendor, 2020).
The reasons for the racial disparities are difficult to discern. Some studies have suggested that culture may play a role (Nafilyan et al., 2021). The practice of living in multiple generation households, common in Hispanic and African American groups, could increase the chance of infection among people in the household, especially the elderly (Nafilyan et al., 2021). Other studies suggest that higher infection rates may be due to increased comorbidities in minority populations (Gravlee, 2020; Tai et al., 2021). Hispanic and African American groups have higher rates of hypertension, obesity, and diabetes (Alcendor, 2020; Ebinger et al., 2020). The comorbidities have been associated with increased fatality, particularly when clustered as in metabolic syndrome (Ferdinand, 2020; Xie et al., 2020). Still, other studies point to systemic problems, such as minorities living in overcrowded neighborhoods or the lack of health care facilities in minority areas (Gravlee, 2020).
This study examines racial and ethnic differences in fatality for adults who had screened positive for COVID-19 in the Southeast Texas region using data obtained from EHRs. The study's objectives are (1) to estimate the fatality rate after positive COVID-19 screening for each racial and ethnic group and (2) to determine the extent to which differences in clinical characteristics can account for differences in fatality rate between the racial and ethnic groups.
Methods
Data Source
TriNetX, a global data platform, was used to identify a cohort of adults who had a positive COVID-19 test result. The data selected was restricted to the EHRs of one primary health care system serving the Southeast Texas community. The health care system consisted of four different campuses and a network of community clinics in nine cities. In the fiscal year 2020, the health care system had over one million outpatient encounters, more than 100,000 emergency department visits, over 250,000 telemedicine encounters, and more than 168,000 hospital patient days. This health care system also provided lab services for COVID-19 screening for other organizations in the region.
The TriNetX Platform contains only de-identified data as per the de-identification standard defined in Section §164.514(a) of the HIPAA Privacy Rule. The process by which the data is de-identified is attested to through a formal determination by a qualified expert as defined in Section §164.514(b)(1) of the HIPAA Privacy Rule. This study does not meet the definition of a “human subject” outlined under Federal regulations 45CFR46 and is not considered human subject research (NHRS). IRB review is not required.
Data quality checks were performed by TriNetX. The checking of basic formatting of data fields, enforcing a list of required fields, rejecting those records where the required information is missing, and ensuring referential integrity of the data that span multiple database tables to guarantee that the data joined successfully. The data maps to a set of standard terminologies, such as HL7 administrative standards, ICD-9-CM, ICD-10-CM, ICD-10-PCS, CPT, and LOINC.
Sample Selection
The data query was conducted on March 28, 2021. The query identified 28,275 adults with positive test results with LOINC codes of 945345-5 (SARS-CoV-2 RdRp gene presence in respiratory specimen), 94500-6 (SARS-CoV-2 RNA presence in respiratory specimen), or 9088 (SARS coronavirus 2 and related RNA presence). After excluding cases of unknown race (n = 2,768), and those who identified as Asian (n = 549), or Native Americans/Pacific Islanders (n = 124), the final cohort consisted of 24,834 adults with the COVID-19 infection. Although we would have liked to include Asian and Native Americans/Pacific Islander individuals in the study, the number of deaths in the Asian and Native Americans/Pacific Islanders groups were too few to provide stable estimates for data analysis purposes. Similarly, people who self-identified as multiple races were excluded for the same reason. The excluded group comprised of more men than women (66.5% vs. 33.2%), tended to be in the younger age group (83%, 10%, 4% and 2% in 18–59, 60–69, 70–79, and 80 years old or older, respectively), and had the lowest percentage of death, 0.67%.
The final study sample included both members and non-members of the study health care network. The COVID-19 screening tests were provided to anyone in the service area. The screening results were captured and recorded by the EHRs system. For nonmembers, the screening results might be the only record in the EHR unless treatments for COVID-19 were obtained in the study health care network. Preexisting conditions were not captured for those who never received any treatment from the study health care network.
Measurements
COVID-19
Only results from reverse transcriptase – polymerase chain reaction (RT-PCR) tests were used to identify positive cases. The date of the first positive incident was captured and used as the index event.
Demographics
Demographics included self-reported sex, race, ethnicity, and marital status and map to HL7 administrative standards. TriNetX reported only the year of birth, which has been date shifted. The year of birth was subtracted from the year of COVID-19 screening to calculate age. Sex was coded as male or female. Race and ethnicity were recoded into Hispanic, non-Hispanic White, and non-Hispanic African American. For the remainder of the paper, we will refer to non-Hispanic White as White, and non-Hispanic African American as African American.
Preexisting Medical Conditions
Diagnosis codes were used to identify preexisting conditions. The diagnosis must have occurred at least 60 days before the COVID-19 lab date to ensure the conditions were not associated with COVID-19.
Elixhauser's Comorbidity Index
We applied the coding algorithm (Quan et al., 2005) that used the enhanced ICD-9-CM and the ICD-10 diagnosis codes to capture the 31 comorbidities identified by Elixhauser (Elixhauser et al., 1998) as increasing the risk of fatality. We also added smoking as an additional comorbidity.
Analytical Methods
All analyses were conducted using SAS Software 9.4, SAS/STAT 15.1. Fatality distribution by demographic categories was explored using descriptive statistics and reported as percentages of death. Percentages were also calculated for each preexisting condition by race and ethnic groups. Logistic regression models were used to adjust for multiple risk factors for fatality. Three models were constructed. In Model 1, all demographic variables were entered and retained. In Model 2, comorbidity, as measured by the Elixhauser's score, was added to the demographic model. For Model 3, all 32 comorbidity conditions were included with the demographic variables, and a backward elimination method kept only the significant factors defined as those with a p-value less than .05. Odds ratios and 95% confidence intervals were computed for all models.
Results
Sample Characteristics
The study consisted of 24,834 adults who tested positive for COVID-19 since the pandemic's start through March 2021. The sample had more women than men (53.2% and 46.8%), especially for the Hispanic and African American groups (54.9%, 53.5%, and 51.5% for Hispanic, African American, and White, respectively). The age distribution differed by racial and ethnic groups with the Hispanic and African American groups having a higher percentage of individuals in the younger age group compared to the White group [median age: 39, 44, and 47; mean ± SE: 41 ± .16, 45 ± .29, and 48 ± .17].
Racial and Ethnic Differences in Fatality by Age and Sex
The racial and ethnic differences in fatality by sex and age are shown in Table 1. Overall, African Americans had the highest percentage of death among the three racial and ethnic groups, and Hispanics had the lowest percentage of death. However, the patterns differ when examined by age group. In each age group, Hispanics had a higher proportion of fatality than Whites. The higher proportion of fatality is known as the Simpson's paradox, where the age-specific fatality proportions between the groups are in the opposite direction to the overall proportion between the groups. The denominator played a crucial role in Simpson's paradox. Hispanics had fewer people in the older age groups than Whites. The fewer people there are, the less they contribute to the overall rate. The highest fatality rate was in the 80 years and older age range, where minority groups exceeded Whites by three percentage points (20% vs. 17%).
Racial and Ethnic Differences in Mortality by sex and age Among Adults With Coronavirus Disease 2019 (COVID-19).

Racial and ethnic differences within gender were observed. Overall, men were two to three times more likely to die from COVID-19 than women. Among men, African American individuals had the highest fatality (3.80%); White individuals had the lowest (2.29%); and Hispanic individuals were somewhere in between (2.68%). Among women, African American individuals had the highest fatality rate (1.57%); Hispanic individuals had the lowest (0.77%); and White individuals were somewhere in between (1.21%).
Racial Differences in Preexisting Conditions
Table 2 presents by race and ethnic groups, the 31 preexisting conditions identified by Elixhauser et al. (Elixhauser et al., 1998) plus one additional risk factor, smoking. Of the 32 preexisting conditions, African American individuals had the highest prevalence in all pre-existing conditions, except for hypothyroidism. Hispanic individuals had a higher prevalence compared to White individuals in uncomplicated diabetes (9.78% vs. 7.58%), complicated diabetes (6.62% vs. 5.21%), and obesity (25% vs. 17.81%). Other conditions with a slightly higher prevalence in Hispanic individuals than White individuals were liver disease (4.77% vs. 4.66%), blood loss anemia (1.04% vs. 0.99%), and deficiency anemia (3.88% vs. 3.28%). Hispanic individuals had the lowest prevalence among the three racial and ethnic groups for all other conditions examined.
Prevalence of Comorbidity.

Adjusted Fatality Risk
Table 3 shows the results from the three logistic regression models. The sex-age adj. OR from Model 1 showed that African American and Hispanic individuals had 2.2 and 1.9 times higher fatality risk, respectively, compared to White individuals. After adding the Elixhauser's comorbidity score to the demographic model, the adj. ORs were slightly reduced for African American individuals (adj. OR = 1.85) but remained the same for Hispanic individuals (adj. OR = 1.91), as shown in Model 2. Model 3 displayed an alternative model that specified all 32 individual preexisting conditions instead of one total score from the Elixhauser's index. After the backward elimination process, Model 3 identified seven preexisting conditions as significant risk factors and one protective factor for fatality for this COVID-19 cohort. The adj. ORs for the African American and Hispanic groups were 1.82 and 1.83, respectively, indicating a higher fatality risk than the White group. The seven risk factors were pulmonary circulation disorders (adj. OR = 1.55), hypertension-complicated (adj. OR = 1.74), paralysis (adj. OR = 2.02), diabetes-complicated (adj. OR = 1.50), liver disease (adj. OR = 1.54), lymphoma (adj. OR = 2.54), and psychoses (adj. OR = 1.67). Hypertension-uncomplicated had a protective effect (adj. OR = 0.76).
Logistic Regression Results Showing Adjusted Odds Ratios (adj. ORs) for all-Cause Fatality Among Adults With Coronavirus Disease 2019 (COVID-19).
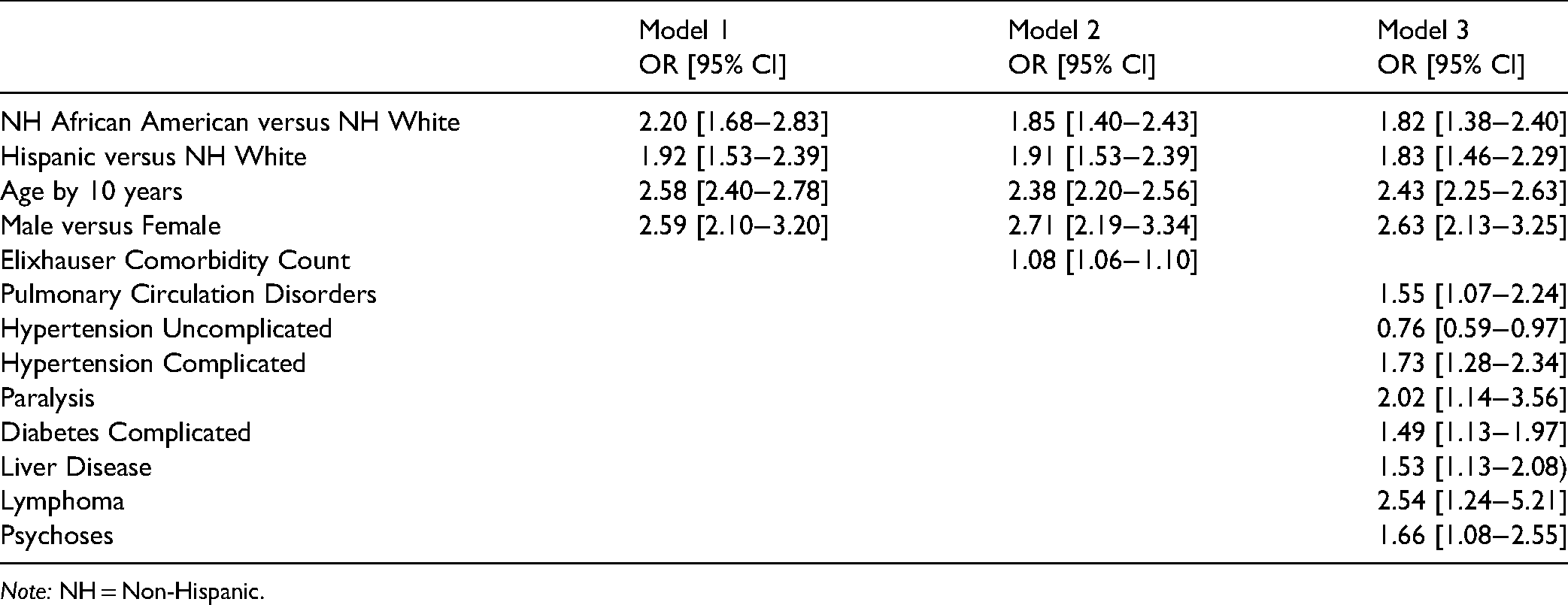
Note: NH = Non-Hispanic.
Discussion
This study examines the racial and ethnic differences in fatality risk using EHRs of 24,834 adults who tested positive for COVID-19. The fatality risk was found to be higher for Hispanic and African American individuals than White individuals. The almost twofold increased risk persists even after accounting for age, sex, and comorbid conditions. These findings are in alignment with other studies (Acosta et al., 2021; Dai et al., 2021; Laurencin et al., 2021) that also reported higher COVID-19-associated mortality for African Americans and Hispanics compared to Whites.
COVID-19-related deaths are most likely to occur in older persons and men. The proportion of deaths among adults ≥ 60 years of age or older was not distributed evenly among racial and ethnic groups in our sample. For Hispanics and African American individuals, older age had a greater impact on mortality than White individuals. Similarly, among men, African American individuals have the highest fatality rate.
Some studies have suggested that a higher prevalence of preexisting medical problems in minorities could contribute to the racial and ethnic differences in fatality (Ebinger et al., 2020). In our cohort, African American individuals have the highest prevalence of all 32 preexisting conditions examined, except for hypothyroidism. Hispanic individuals have the lowest prevalence for all conditions examined, except for obesity, diabetes (uncomplicated and complicated), liver disease, and anemia (blood loss and deficiency) which are higher than White individuals. In our multivariable models, we adjust for the effect of these preexisting conditions on fatality. The preexisting conditions account for only a minimal reduction in fatality risk. Race and ethnicity remain a significant independent predictor of fatality.
As with any EHR study, there are some limitations. First, about 12% of the cases (n = 3,441) had to be excluded from the study due to missing or unknown race/ethnicity or due to the small sample size for a specific race/ethnic group, such as Asian. The number of deaths in this excluded group was small, n = 23 (0.67%) compared to the groups included in the study which ranged from 1.6% to 2.6%.
Second, the study is limited by the data that are captured in the EHR. Only deaths that occurred in this health care organization (HCO) were captured. Deaths that occurred in the community or other HCOs were not captured in this data set. Deaths at home were related to several factors that contributed to not seeking medical care, such as financial constraints, lack of insurance, medical mistrust, and cultural factors such as fear of dying alone in a hospital without family members present (Opel et al., 2021). These factors were more prevalent in Hispanic and African American individuals than in White individuals. For example, in Texas, the percentages of uninsured are 27%, 16%, and 12% for Hispanic, African American, and White individuals, respectively (Grubbs & Wright, 2020). Likewise, medical mistrust has been prevalent in communities of color because of prior mistreatment and unethical public health experimentation. Patients have had their health care concerns dismissed or minimized when previously seeking care, creating a poor patient-provider relationship. The decreased confidence in their providers may create a barrier to seeking medical care, leading to worse outcomes. These factors have the potential of creating a bias of underestimating the death count by race. However, the bias would be in the direction of the results reported in this study.
Comorbidity is another factor that EHR may not fully capture. The EHR captures only subjects who received treatment or had an encounter within our health care system. Patients seen outside of our health care system would not have their data kept in our EHR. Thus, they would be coded as having no comorbidity, creating possibly a false negative for comorbidity. To address this concern, a sensitivity analysis was conducted with a sample of only those that had at least one encounter with the health care network before the COVID-19 screening. We assume that those who had an encounter were members of the network. By including only members of the health care network, the absence of a preexisting condition in the EHR would indicate no comorbidity rather than a false negative for comorbidity. A comparison of the odds ratios between the full sample and the members-only sample reveals a slight but nonsignificant decrease. The adj. ORs in the full sample and in the members-only sample are 1.85 and 1.80 for African American and 1.91 and 1.78 for Hispanic, adjusting for age, gender, and Elixhauser comorbidity index. In the model with the individual preexisting conditions, the adj. ORs in the full sample and members-only sample are 1.82 and 1.75 for African American and 1.83 and 1.70 for Hispanic. Again, the changes in odds ratios between the two samples are not statistically significant and still show an increased risk for fatality in Hispanic and African American individuals compared to White individuals.
Lastly, our study included a sample population from only one HCO serving a large but still limited geographical area. A statewide study is needed.
Our study has several strengths. First, the cohort is among the largest COVID-19 studies in Texas, with almost 25,000 adults who tested positive for COVID-19 in both community and hospital settings. Second, our study captures an entire 1-year period, from the beginning of the pandemic to March 28, 2021, reflecting the changes over time. Third, our study uses both race and ethnicity to capture more diversity than Black and White. Lastly, the availability of extensive historical data, although not available for all cases, allowed us to assess the effect of preexisting conditions on fatality outcome from the COVID-19.
Our study highlights significant differences in fatality risk among racial and ethnic groups for adults who tested positive for COVID-19 in the Southeast Texas region. The almost twofold higher fatality risk for Hispanic and non-Hispanic African American individuals compared to non-Hispanic White individuals cannot be fully explained by differences in age, sex, and preexisting health conditions, suggesting that other factors are at play. Additional studies that incorporate social, behavioral, and environmental factors are needed. Vaccination is effective in reducing mortality from COVID-19 infection. Health care providers might be more successful in encouraging their patients to get vaccinated by addressing social and cultural barriers in these vulnerable populations.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors thank the John Sealy Memorial Endowment Endowment Fund and the UTMB School of Nursing Research Innovation and Scientific Excellence Center for their support.