
Abstract
Participatory research in occupational science and therapy seeks to redress the occupational concerns of diverse communities. To explore occupational therapy practitioners’ (OTP) perspectives on health enablers and barriers for Black people with intellectual and developmental disabilities (IDD). 23 OTPs, educators, and students participated in a World Café conference session. Participants were prompted to discuss facilitators, barriers, and the influence of OT on the health of Black adults with IDD. Three themes emerged: (a) Negotiating culturally specific and systemic understandings of health, (b) leveraging professional privilege and community partnerships to expand occupational possibilities and access, and (c) confronting implicit bias, racialized ableism, and structural barriers to health care and occupational engagement. OTPs are positioned as institutional agents of possibility and advocacy who can amplify client expertise, critically examine systemic barriers, and co-create health-promotion rooted in clients’ realities. This study contributes to calls for anti-racist, justice-oriented OT praxis.
Plain Language Summary
Black people with intellectual and developmental disabilities (IDD) often face barriers to quality health care due to racism, ableism, and other unfair systems. This study asked occupational therapy practitioners (OTPs) to share their thoughts about what helps or gets in the way of health for Black people with IDD and what role OTPs may play in supporting them. We used a participatory conversation method called the World Café at a state occupational therapy (OT) conference. OTPs, educators, and students came together in small groups to talk about important questions like: How can OTPs support the health of Black people with IDD? What makes it easier or harder for them to be healthy? Three main ideas came out of these conversations: (a) health means different things to different people; (b) OTPs can help open doors by using their position and privilege to create new opportunities for clients and to stand up against unfair practices; and (c) bias and stereotypes cause real harm. The group discussed racism and ableism in health care and how OTPs must reflect on their identities and experiences to better support Black people with IDD. This study shows that OTPs can make positive changes in the care of people with IDD by building relationships with communities, challenging unfair systems, and working alongside clients as partners. It also calls for the OT profession to commit to equity and justice in both health care and everyday life.
Keywords
Black people with intellectual and developmental disabilities (IDD) often face barriers to quality health care due to racism, ableism, and other unfair systems. This study asked OTPs to share their thoughts about what helps or gets in the way of health for Black people with IDD and what role OTPs may play in supporting them. We used a participatory conversation method called the World Café at a state occupational therapy (OT) conference. OTPs, educators, and students came together in small groups to talk about important questions like: How can OTPs support the health of Black people with IDD? What makes it easier or harder for them to be healthy?
Three main ideas came out of these conversations: (a) health means different things to different people; (b) OTPs can help open doors by using their position and privilege to create new opportunities for clients and to stand up against unfair practices; and (c) bias and stereotypes cause real harm. The group discussed racism and ableism in health care and how OTPs must reflect on their identities and experiences to better support Black people with IDD.
This study shows that OTPs can make positive changes in the care of people with IDD by building relationships with communities, challenging unfair systems, and working alongside clients as partners. It also calls for the OT profession to commit to equity and justice in both health care and everyday life.
OT Perspectives on Health Care Enablers and Challenges in Serving Black People With IDD
There remain ongoing calls for occupational science and therapy (OS/OT) scholars to engage in critical, collaborative, and emancipatory research approaches aimed at redressing the occupational concerns of diverse communities (Magalhães, 2023). More specifically, OS/OT scholars have been challenged to understand, elucidate, and disrupt processes of marginalization (Bailliard et al., 2020); discuss how the discipline produces and reproduces colonial thought (Ahmed-Landeryou, 2023) and institutional violence (Turcotte & Holmes, 2024); critically interrogate the discipline’s values (Venkatapuram, 2023) to support knowledge production in service to social transformation (Smith et al., 2025); and apply anti-racism as epistemic praxis (Wijekoon & Peter, 2023). We build upon these appeals to include a responsibility to incorporate participatory approaches. These approaches aim to transform the conceptualizations and theorizations of occupation by challenging the barriers that prevent the community from engaging with practitioners and researchers (Kitzie et al., 2020).
Participatory Research in Occupational Science and Therapy
OS scholars have employed participatory methods to investigate and expose normalized structural inequities, with an emphasis on everyday living (Benjamin-Thomas et al., 2021; Trentham & Neysmith, 2017). Participatory methods are contextually situated, political, and collaborative, driving social change and generating an immediate, relevant impact on the communities they engage with (Aldrich & Marterella, 2012; Godoy Almeida, 2025). Each project, regardless of method, onto-epistemologically situates a person as a knowledgeable informant of the social world. Consequently, participatory research posits that a person’s lived experience and intersectional positionality are critical for ameliorating the complex problems impacting them (Johnson et al., 2025).
Accordingly, OS scholars have worked to leverage participatory research to redress various social problems including using cultural translation activity to intervene on Brazilian social services program delivery (Godoy Almeida, 2025); applying participatory digital methodologies to combat ableism and individualism alongside dis/abled children and youth in South India (Benjamin-Thomas et al., 2018, 2021); and partnering with Canadian senior citizen activists to develop and implement advocacy materials to steer policy decisions and sway public perceptions about old age and citizenry (Trentham & Neysmith, 2017).
Participatory methods within OT scholarship have also gained momentum (Asaba & Suarez-Balcazar, 2018; Hammel et al., 2015). Scholars have sought to further community engagement with both service recipients and OTPs themselves. Through the utilization of participatory methodologies that access the knowledge of communities in context, research has identified barriers and supports for community participation (Heffron et al., 2018) and health-promoting occupations (St John et al., 2018) for people with IDD. It has also facilitated partnerships between the IDD community and health care stakeholders (Bendixen et al., 2022; Johnson et al., 2025), built communities of practice (Marcolino et al., 2021), and improved knowledge translation (Bennett et al., 2016).
Overall, participatory OS/OT literature highlights how the discipline can (a) gain more nuanced understandings of occupations within multiply marginalized communities through participatory methods; and (b) have a positive impact toward transformative actions aimed at ameliorating occupational injustices. Hence, participatory methods provide occupational scientists and therapy scholars a vehicle to study occupation while upholding values of social justice.
Health Care Disparities Impacting Black People With IDD
Black people with IDD face stark and persistent health disparities that reflect deeply rooted systemic inequities (Jones et al., 2020; National Disability Institute, 2020). Research has highlighted significant gaps in service utilization and health care spending, with over half of Black people with IDD reporting poor or fair health status and fewer than 10% having access to private insurance (Johnson et al., 2025; Scott & Havercamp, 2014; Williamson et al., 2017; Yearby, 2018). Moreover, studies show that Black people with IDD are between 9% and 29% less likely to receive services compared with their White counterparts (Harrington & Kang, 2016). These disparities extend beyond access and include racialized differences in provider engagement, particularly in conversations around health care transition planning and long-term supports (Li et al., 2021). The cumulative effect of these inequities directly impacts the quality of life for Black and other racially minoritized people with IDD.
The intersection of racial and disability identities presents unique systemic challenges for Black individuals with IDD and their care partners. These challenges are often described as a continuous struggle shaped by both racism and ableism (Johnson et al., 2025). The lived experience at these intersections not only informs personal identity but also significantly influences how individuals access and navigate health care systems. In a study involving Black and Latinx adults with IDD, Li et al. found that participants faced distinct barriers to care rooted in historical and ongoing discrimination. These institutional barriers included negative and/or absent provider communication, a lack of timeliness and helpfulness in care, and long-standing violations of patient trust (Li et al., 2018). Such discrimination led some to forgo treatment altogether, an experience not commonly reported among White service recipients. These findings underscore the urgent need for culturally affirming supports and interventions that reflect the complex realities of multiply marginalized populations.
Addressing health inequities for Black people with IDD requires a research approach that situates these disparities within broader historical, social, and political contexts. This includes examining how power structures, institutional practices, and dominant narratives shape disability and health care access. Without a critical interrogation of the structural forces that sustain inequity, health services and OT research risk perpetuating the invisibility and erasure of Black disabled lives. This understanding can be facilitated by research processes (i.e., participatory methods) that aim to contextualize and grapple with the entwining constructs of difference and social inequality, health care contexts, power relations, and the ways multiply marginalized people resist contradictory identity categorizations (Johnson et al., 2021; Rice et al., 2019; Richardson & Stoneman, 2019).
Within OT scholarship, research that includes race as an analytic construct to better understand what, how, and why health care access for Black people with IDD remains an issue is sparse (Little et al., 2024). Furthermore, scholarship that explores how OTPs engage this community, if at all, is limited (Benevides et al., 2022). The lack of disciplinary engagement with the structural factors that perpetuate health services disparities for those who are Black and disabled not only sustains these disparities but renders their experiences invisible (Bailey et al., 2017, 2021; Richardson & Stoneman, 2019).
The World Cafe
Our research employed the World Café (TWC), a participatory method that posits that communities possess the necessary knowledge and creativity to address issues affecting them. TWC mobilizes this belief by facilitating in-depth, exploratory, critical reflection to generate possibilities for action with community members who may or may not know each other (Brown & Isaacs, 2005). Community praxis is leveraged through seven principles developed by Brown and Isaacs (2005) as outlined in Table 1.
Brown and Isaacs’ (2005) The World Cafe Principles.
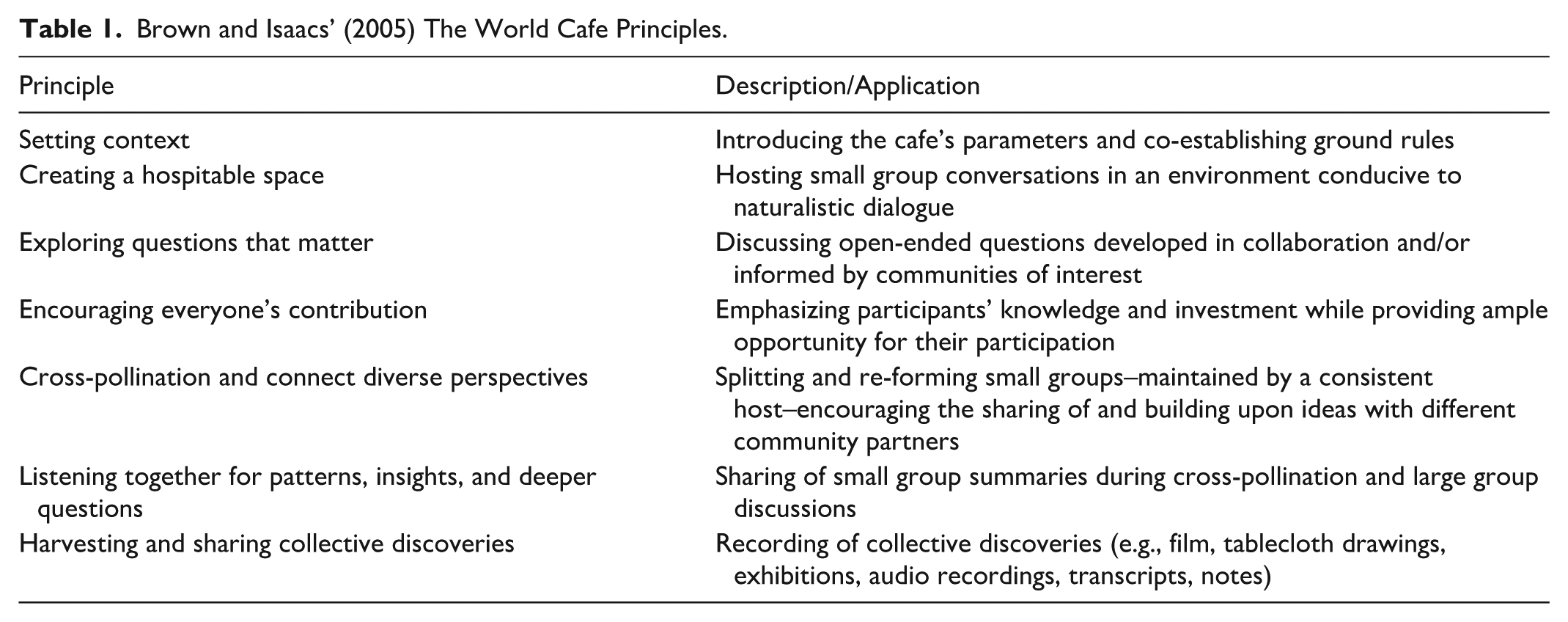
Although prompts initially structure conversations, TWC is distinctly marked by its conversational nature. Conversations are not controlled by facilitators, but are focused on the rationale, purpose, and parameters for participation in the café (Brown & Isaacs, 2005). This intentional structuring of the conversation’s context facilitates a natural flowing discussion. TWC’s participatory approach is complemented by living systems theory, which contends that within whole systems, symbiotic relationality exists between individuals (Baird-Wilkerson, 2003). It further asserts that nonlinearity, uncertainty, and adaptive self-organization are building blocks to change (Wells & McLean, 2021); thus, TWC brings together groups of people with different life experiences to discuss common interests and produce otherwise unforeseen outcomes and new knowledge.
Despite TWC’s methodological advantages for the study of occupation (Pettican et al., 2021), it has been utilized sparingly in OS/OT, with one notable exception: Mao et al. (2024), who explored OTPs’ challenges and strategies for intervention implementation. This project, however, affirms the benefits of TWC’s approach to data collection. Practically, TWC provides the opportunity to quickly collect data from many people at once. Furthermore, TWC’s adoption of more egalitarian and conversational processes generates data that reveals the ways participants are deeply connected in their doings. These connections enable participants who may not often engage in dialogue to juxtapose their similarities and differences across their experiences, positionalities, and actions. Findings represent both individual and collective experiences, allowing researchers to elucidate the structural and moderating influences on the occupational possibilities (Rudman, 2010), including clinical practice (Townsend et al., 2003) of TWC participants.
Research Objectives
The TWC session described in this article was conducted within a larger Critical Participatory Action Research (CPAR), which aimed to (a) elucidate structural factors, specifically structural racism and ableism, that impact how racially minoritized people with IDD access and utilize health care, and (b) facilitate the development of consumer-provider informed mechanisms that improve health pathways. To our knowledge, this larger study is the first of its kind in OT that not only directly engages Black adults with IDD and their care partners, but also facilitates their engagement with health care providers. A more in-depth description of the larger CPAR study can be read elsewhere (redacted for review); however, the initial four meetings of the larger CPAR focused on Black young adults with IDD and their care partners naming and framing the contextual factors that influence their access to and quality of care. Despite the simultaneous recruitment of both Black adults with IDD, their care partners, and health care providers, providers remained underrepresented in the study. As such, during the fifth meeting, questions generated from the previous four CPAR discussions were shared with the study’s community research partners for feedback in preparation for this TWC study designed with OTPs, educators, and students in mind.
The TWC session was conducted to capture OTP’s underrepresented perspectives and to improve provider recruitment to the broader study. Although the study’s community partners specifically included Black adults with IDD and their care partners, questions were expanded to include all Black people with IDD, regardless of age, to account for the spectrum of practice areas reflected at a statewide OT association conference. Given this diverse representation of experience and a lack of OT literature engaging with Black people with IDD, questions were designed to capture the average OTPs’ perspectives to begin establishing a baseline for the larger study and future research. The research questions guiding this TWC became the following:
Subsequently, the purpose of this article is to both present (a) OTPs’ perspectives on their perceived health care enablers and challenges in serving Black people with IDD; and (b) how TWC, as a participatory research method, generated these perspectives by engaging practitioners in critical and collaborative research applicable to multiply marginalized communities.
Researcher Positionalities
The authors comprise an early-career investigator and two doctoral students. The first author identifies as a Black, nondisabled female; both the second and third authors identify as White and nondisabled, while the second identifies as female and the third as male. Their diverse and intersecting identities shaped their engagement in action research with multiply marginalized communities, influencing both the theoretical frameworks they adopt and the research methodologies they employ. The first author’s repeated encounters with anti-Black racism and other intersecting forms of oppression against ethnic and gender minoritized groups strongly inform her perspective. The second author brings a critical lens to the study through her reflective scholarship on White racialization and the ideology of whiteness. The third author’s contributions are grounded in his scholarly work on community-driven, political social transformation as shaped by his queer identity.
Methods
The World Café as a Conference Session
This research used TWC during an oral presentation at the annual fall conference of the North Carolina OT Association. The session description was advertised as a “works in progress” presenting preliminary findings from a CPAR study, and an opportunity to participate in ongoing research with sociocultural and anti-racist implications important to OT practice and minoritized people with IDD. Born out of a desire to cultivate a representative sample of practitioners across the state, anyone present at the conference was able to attend the session regardless of career stage, practice area, or expertise. Consent to participate in semi-structured roundtable discussions was included.
The session began with a 30-minute overview of the larger CPAR study (e.g., the current research team, inclusion and exclusion criteria, the consent process, theoretical guideposts, hypothesis and aims, and methodological design and activities) and its transformative potential to positively impact multiply marginalized communities. This overview was briefly followed by a bulleted list of preliminary findings from the study’s previous four meetings. Participants then had the opportunity to ask clarifying questions before signing consent forms to participate in the TWC. It was also explained that participants could withdraw consent and excuse themselves at any point during the session. The remaining time was utilized through (a) a 15-minute large group discussion to frame un/healthfulness as a lead for TWC prompts; (b) a 30-minute period of rotating roundtable discussions in 10-minute intervals to discuss each prompt; and (c) a 15-minute final summarization and analytic discussion. During the large and small group discussions, three graduate research assistants, including the second and third authors, took notes. The notes aided data collection and supported the research assistants in their role as “café hosts,” who provided prompts and summaries of previous discussion rounds. Audio recordings for all group discussions were transcribed verbatim following the recommendation of Schiele and colleagues (2022).
Participants
The participants included OTPs (n = 12), OT educators (n = 5), and OT students (n = 6), including one pre-OT undergraduate intern. Of the 23 in attendance, only five identified as Black. All participants were employed or matriculated through an OT academic program in North Carolina. Participants who completed the TWC portion of the session were given a US$25 gift card.
Analysis
The World Café data set was constructed from recordings and transcriptions of each roundtable conversation and the large-group synthesis. To enhance analytic rigor, TWC participants’ insights were validated in real time as the café hosts reviewed responses, synthesized themes across groups, and invited immediate feedback and clarification prior to the session’s end (Schiele et al., 2022). This iterative process not only enhanced credibility but also ensured that participants’ perspectives were accurately represented in subsequent analyses.
All three authors employed an iterative thematic analysis of the TWC data set, with each author independently coding using a scheme inductively developed from the codebook of the larger CPAR study, to identify key ideas and comments shared by the participants, occupation-centered perspectives, and contextual nuances (Braun & Clarke, 2021; Kitzie et al., 2020). Following this initial coding, the authors iteratively compared their application of codes and findings, generated additional codes reflecting collective insights arising from the dialogic structure of TWC, redefined definitions, and developed emergent themes/subthemes until consensus was achieved (Braun & Clarke, 2021). While the TWC coding structure aligned with already established categories from the larger CPAR study pertaining to health, disability, social and structural determinants, and occupation, these data were organized into distinct themes as a part of the analytic process for this manuscript, separately from the broader CPAR study.
Findings were analyzed across the entirety of TWC; however, they are presented below alongside each instigating prompt before being synthesized into global themes within the discussion. This is done to reflect the method’s iterative small-to-large group discussion format and the lived, conversational structure of TWC, both of which are centered around prompts (Brown & Isaacs, 2005; Monforte et al., 2023).
Research Ethics
Approval by the Office of Human Subjects Research at the University of North Carolina at Chapel Hill was obtained for onsite recruitment, consent, and data collection procedures.
Findings
Prompt 1: In What Ways Might OTPs Influence the Health of Black People With IDD?
Two main themes dominated the conversations: (a) the challenges of negotiating culturally specific views of health with broader social and structural perspectives; and (b) the importance of diverse racial and disability representation and community-centered partnerships among OTPs.
Negotiating Health
Responses highlighted the tensions participants experienced when attempting to define and identify influences on health. Participants noted how health is defined by cultural lexicon but implemented or practiced in individualized ways. Culture in this sense is not limited to Black and other racially minoritized people but includes disability as a cultural group. While practitioners discussed this critical distinction, they also noted that how health is understood is often determined by society at large (and subsequently by the dominant group) and the institution in which one is employed. One participant affirmed: It varies from person to person, rather than being a system, like, okay, how do I provide care for this person, so they feel that they’re healthy versus society’s determination of health, and what it means to be healthy.
Representation and Connecting to Community
There was consensus that OTPs can influence health, and recognition that their influence is situated in a broader sociopolitical context that mediates how understandings of health are perpetuated, accessed, and practiced by Black people with IDD. Participants noted that to have an influence on the health of Black people with IDD, OTPs are assumed to have access to the population, and that whatever access they do have is unproblematic, as confirmed by one practitioner participant: . . .where are the Black people? Why is this institution only serving white people? Because we know it’s not just white people that have IDD. . . in what ways do our do policies and procedures disadvantage the African American population from even knowing about or seeking services here? What do we need to change to take down this sort of implicit focus on whiteness, so that other people actually get served?
Although participants were not explicitly asked to reflect on whiteness ideologies, their candid conversation yielded an acknowledgment of its role in sustaining inaccessibility. Participants went on to remark that disparate representation of Black people also occurs within the OT workforce and suggested that this problem, in addition to accessing the Black IDD community, might be confronted by cultivating cultural bridges and enhancing therapeutic relationships through diverse representation. One student participant remarked, “It’s important to think about, and just representation or being able to see yourself. . .being able to find commonality in some way with the individual that you’re working with. I guess that’s just like a therapeutic relationship.” Participants agreed that this process of “bridge-making” also validated community members’ expertise about their own health. For example, an educator affirmed: . . .ask questions and [get] to know the person. . .to really make sure that they’re feeling like you’re not the expert, like they truly are that expert. . . in this situation, they’re Black and IDD. That’s a completely different thing than white with IDD. . . .you’re acknowledging that, they’re the expert in their life, and you’re not.
Participants were encouraged to challenge the café host’s summary after each rotation. Although participants could steer their conversations in whichever direction they felt drawn to, the two themes described above demonstrated “staying power” across group rotations. Discussions stemming from this prompt also emphasized the importance of acknowledging implicit bias and the role of OTPs as critical advocates for services, referrals, and situated care.
Prompt 2: What Do You Consider to be Facilitators to Health for Black People With IDD?
Two central perspectives arose from Prompt 2: (a) accessing occupational possibilities, and (b) leveraging power and privilege. Both perspectives were situated under participants’ shared belief that OTPs could serve as “agents of possibilities” as it pertained to positively impacting the health of Black people with IDD.
Accessing Occupational Possibilities
Practitioners felt that their position as OTPs, given the profession’s clinical emphasis on choice, allowed them to facilitate client agency. To evidence this, several practitioners shared how they sought to expand access to previously unexplored or inaccessible occupations in their work. One participant relayed: I think OTs can positively influence the health of Black people as well, just by exposing them to diverse leisure, diverse occupations are things that they may not have been exposed to. And just not thinking of them as you know, your culture typically does this. But having open conversations about the things that they choose.
Participants echoed the importance of dialogue with clients surrounding their occupational choices across rotations. They felt that increasing occupational possibilities required tact to ensure client-centered practice. Further, they recommended that the first step to doing so is familiarizing oneself, and community partners if they are unaware, with existing community resources and their associated occupational demands. Although outside of the scope of OT practice, participants recognized that OT was only able to become an “agent of possibility” when Black people with IDD received an official diagnosis, and they remarked that this was one of the most significant facilitators for health.
Leveraging Power and Privilege
Expanding upon responses in Prompt 1, participants shared that OTPs should be intentionally reflexive about assuming authority around which occupations their clients should pursue. They emphasized that OTPs should not only be more cognizant of the cultural privilege and power ascribed to being a health care provider, but to strategically leverage it to facilitate better health for Black People with IDD. One practitioner reflected that: OTPs, regardless of their racial identity, are often in positions of greater privilege than the clients that they serve. It might be a a Black therapist without IDD who’s working with a Black client with IDD or it might be a white therapist without IDD who’s working with a Black client with IDD, and using those advantages and privileges to leverage change, not in a way that’s like speaking over someone’s experience but amplifying people’s experiences because the practitioner always has more power.
Participants recognized that regardless of one’s socio-political positioning, the fact that they were practitioners afforded them structural power to influence the health and well-being of Black people with IDD. This recognition was accompanied by an understanding that OTPs have a responsibility to amplify, not assume, community perspectives not only within health care encounters but across institutional and political contexts.
Prompt 3: What Do You Consider to be Barriers to Health for Black People With IDD? What Role Does OT Play in Eradicating Those Barriers?
Given Prompt 2’s orientation toward facilitators, the responses discussed above exhibited a noticeably positive tone regarding service provision. This understanding of OT became more nuanced as participants explored the discipline’s relationship to barriers. Themes central to Prompt 3 included (a) intersectional preparedness to engage Black service recipients, and (b) problematizing “knowledge”/critically interrogating what is known about Black people and people with IDD.
Intersectional Preparedness
Feedback concerning barriers to health for Black people with IDD confirmed that practitioners recognized unspoken or unacknowledged requirements they must fulfill to meet the community’s needs. Participants characterized these requirements as a radical confrontation of one’s social position; that is, sitting with how being racialized as White and able-bodied influenced their perceptions of and preparedness to engage Black people with IDD. A participant reflected, As a white practitioner, I’m thinking, am I going to have some implicit bias and maybe not address a Black client’s pain, symptom or something like that, the same way I would a white client. But then I’m also thinking culturally, like, I’m sure there are cultural differences. I’m not aware of them. I’m sure there are cultural differences in how a Black family responds to having a child with an IDD diagnosis or condition versus how a white family might respond to that. If I’m only aware of my life experiences, I’ve only seen white families respond to it, or live with that. That’s all I can kind of bring to my services, I guess.
Coming “into awareness” must accompany a process of unlearning and relearning that brings into focus the intersections of culture, race, and disability by recognizing and addressing bias, cultural differences, and privileges/power acquired through one’s racializations. Participants did not suggest this as an intellectual exercise, but as a call to actualize being in community with Black people with IDD.
A Critical Interrogation of Knowledge
Participants unpacked how coming to “know” the community (i.e., Black people with IDD and their care partners) you are working in also requires a nuanced understanding of the sociopolitical history of disability and its intersection with anti-Black racism. A participant remarked, “if you’re someone with IDD, I think that you might be feeling so consistently undermined”; to which another practitioner added: I think often there are assumptions about competency for individuals with IDD. Like people with IDD are not assumed to be competent, even though that’s like the mantra of working with folks in the IDD community. And I think for Black folks with IDD, especially, like men who, adults who are maybe larger than a lot of providers who might assume that they’re aggressive, or they’re scary, even more so than an individual with IDD who is white or another racial identity. I think these kinds of assumptions about behavior, how we’re going to show up in space, really kind of creates these barriers to seeking healthcare.
Participants, again, identified deficits in practitioners’ understandings around disability and anti-Black racism as a structural determinant of health care access for Black people with IDD, specifically, that unchecked biases and cognitive shortcuts may lead practitioners to enact care in harmful ways. A participant interjected with the following recommendation: [pay] attention to those things that might be missed. . .highlight this to the team. . .keep bringing it up, I’m gonna make sure that concerns are taken seriously. If we’re aware of this, we can lead a person to look beyond individual intervention to make sure this person is getting access, and I’m noticing areas in which they aren’t getting access, but my white client is getting that access, and I think that we can be that practitioner.
General consensus among participants was that OTPs, while enablers of occupational engagement, must contend with their role in upholding old and reinforcing new restrictions to care through intentional learning, relationship-building, and advocacy.
Discussion
This study explored the perspectives of OTPs regarding their influence on the health of Black people with IDD. Through a series of structured dialogues via TWC, participants articulated nuanced insights into the sociocultural, professional, and systemic factors that mediate therapeutic practice and health outcomes in this population. This discussion explores three overarching implications: (a) the need for cultural and structural fluency in OT practice; (b) the importance of OTP positionality and critical reflexivity; and (c) the role of OTPs as systemic advocates and facilitators of health equity.
Cultural and Structural Fluency
A key finding concerned the ongoing negotiation of health definitions between individual, cultural, and institutional contexts. Many participants highlighted that both race and disability must be understood as socially constructed frameworks that influence how health is conceptualized and enacted. That is, Blackness and disability are racialized cultural positions that deeply inform understandings of health, well-being, and quality of life (Adedeji et al., 2023). However, participants noted that dominant institutions and health care discourses often marginalize these conceptualizations in favor of White, able-bodied, middle-class norms, creating misalignment between clients’ (i.e., Black people with IDD) lived realities and the care they receive. These tensions align with previous critiques by OT scholars who question the concept of health as neutral and call for more pluralistic, community-rooted understandings of what it means for disabled people to thrive (Angell et al., 2020). Participants also reflected that they must not only validate the diverse ways in which Black people with IDD define health, but also actively interrogate the institutional structures that dictate whose definitions are legitimized. This requires OTPs to move beyond cultural humility to develop structural fluency (Haslanger, 2023)—a deeper understanding of how systems, institutions, and dominant ideologies shape access, recognition, and participation in health-promoting occupations.
Moreover, participants problematized what is commonly “known” about Black people with IDD in the OT and other professional literature, and discussed that culture should not be viewed as a monolith. Instead, OTPs must attend to the intersectional realities of Black people with IDD–where race, disability, class, and other social identities intersect to produce unique challenges and needs (Johnson et al., 2025). The conversations further indicated that OT practice must include a critical, inclusive redefinition of health, one that is co-constructed with clients rather than imposed upon them, recognizing that diagnostic overshadowing, racist stereotyping, and ableist assumptions can result in harmful care or the complete absence of care (Johnson et al., 2021; Johnson et al., 2025).
Practitioner Positionality, Critical Reflexivity, and Relationality
Across all prompts, participants emphasized the imperative of critical reflexivity in OT practice. They recognized that practitioners, by their training and institutional affiliations, possess structural power that must be wielded thoughtfully in their work with Black people with IDD. Several practitioners candidly reflected on their own racialized identities and how those identities shaped their clinical perceptions and readiness for interactions with clients. This awareness of bias, differential treatment, and knowledge gaps was essential but insufficient if not followed by action.
The notion of “intersectional preparedness”–characterized as a critical consciousness that compels practitioners to consider how their social position informs their perceptions and interactions–points to a broader call for OT education and practice to unlearn dominant narratives, actively engage in intersectional and critical reflexivity, and center social justice (Smith et al., 2025). As one participant noted, being “in community” with Black people with IDD demands more than cultural knowledge; it requires authentic relationships, sustained engagement, and recognition of community expertise. These calls echo frameworks such as critical disability studies and anti-racist OT, which urge the profession to reconceptualize its epistemologies and practices (Akrofi et al., 2025). Further, practicing at the intersection of race and disability requires more than technical competence; it necessitates an embodied commitment to social justice, community engagement, and accountability (Choudry, 2020).
TWC participants also expressed concern regarding the inaccessibility of OT services. Several participants pointed to the absence of Black clients in their practice settings and raised critical questions about how institutional racism and structural barriers inhibit access. They further identified OT’s current service models as being largely shaped by White-centric policies and procedures, which implicitly exclude Black communities. In response, participants highlighted the importance of racial and disability representation within the workforce. Representation was framed not simply as demographic diversity but as a critical foundation for building therapeutic relationships rooted in cultural resonance and trust. Participants emphasized that shared identities and a culturally responsive practice can foster more effective and affirming care.
Practitioners as Agents of Possibility and Advocacy
The idea that OTPs can serve as “agents of possibility” positions OT not merely as a rehabilitative service, but as a transformative practice capable of challenging stereotypes and expanding occupational choices and supporting access to previously unavailable or unconsidered opportunities. However, participants cautioned against the misuse of professional power in guiding clients toward activities that may reflect the practitioner’s cultural assumptions rather than the client’s authentic interests. The need for cultural humility and reflexive practice was emphasized, with practitioners urged to use their institutional leverage not to prescribe, but to amplify the voices and goals of the communities they serve.
The findings also underscore the critical need for systemic change. Participants noted how institutional whiteness and policies of exclusion prevent Black people with IDD from accessing services. The suggestion to diversify the OT workforce and build community-centered partnerships reflects a broader movement in health care toward structural competency and community-engaged practice (Wang, 2019). Practitioners must not only work within systems but also act as institutional witnesses and advocates. This means not only attending to individual occupational concerns and care needs but also raising awareness within care teams, identifying systemic disparities, and ensuring that concerns from Black clients with IDD and their care partners are heard and addressed.
Strengths and Limitations of TWC
The use of TWC enabled valuable dialogue between typically disconnected communities, namely Black people with IDD and OTPs. Although the former were not physically present, the perspectives of Black people with IDD and their care partners cultivated in the CPAR meetings preceding the TWC session set the ultimate agenda and questions presented to the OTPs in attendance. In this way, traditional power dynamics were subverted. Following TWC, five OTPs expressed interest in joining the study and were ultimately recruited. Before these new provider research partners began attending meetings, they were provided with findings from the previous five research meetings. Simultaneously, community research partners (i.e., Black people with IDD and their care providers) were provided with the emerging findings from TWC. This allowed both groups to share their thoughts on these findings before meeting face-to-face.
For those who experienced TWC in real-time, the method’s conversational structure naturally encouraged reflection on complex issues, such as anti-Black racism and White supremacy in health care, with participants contributing insights informed by their lived experiences and diverse professional roles. TWC made research participation more accessible to participants with varying levels of research experience, enhancing study enrollment and fostering inclusive knowledge exchange. Participants, especially students, expressed a sense of empowerment and professional validation through their engagement in the process, noting the session’s relaxed format and co-creative nature as instrumental in promoting an open exchange of ideas. This suggests that TWC has the potential to cultivate sustained practitioner engagement in participatory research, as it did with the larger CPAR study through recruitment of OTPs.
Despite its strengths, TWC is limited by structural and methodological weaknesses, particularly in addressing power imbalances, promoting dissent, and fostering reflexivity. During this TWC, participants were not encouraged to reflect on how identity and sociopolitical context shaped their contributions, nor was the influence of the facilitator examined. In addition, the fixed nature of discussion prompts—designed without attendee input—limited the potential for participants to lead the interrogation of hierarchical dynamics, especially among OTPs and students. The format also failed to ensure accountability in documenting participant demographics, including the level of experience or perceived expertise partnering in care with Black people with IDD, which hinders deeper analysis of how identity influenced the flow and content of conversations.
Conclusion
This study explored OTPs’ perspectives on health enablers and barriers for Black people with IDD, and the profession’s role in ameliorating the enduring health inequities experienced by this population. Findings from TWC affirmed that OTPs have the capacity, albeit complex, to impact the health of Black people with IDD in profound ways; however, this capacity is contingent upon their ability to interrogate systems of power, engage communities authentically and with cultural nuance, and practice in a way that is critically reflexive, relational, and rooted in equity. Further, the OT profession must commit to structural transformation, collective accountability, and sustained dialogue with the communities it serves. Only then can it fully realize its potential as a justice-oriented health profession.
Footnotes
Acknowledgements
We appreciate the time and contributions of Kierra Peak, doctoral candidate and graduate research assistant in the UNC Division of Occupational Science and Occupational Therapy, in the completion of this work. We also extend our deepest appreciation to Dr. Nancy Bagatell, Division Director of the UNC Division of Occupational Science and Occupational Therapy, for her thoughtful and constructive feedback during the analysis and writing of this manuscript.
Ethical Considerations
This study was approved by the University of North Carolina at Chapel Hill Office of Human Research Ethics (ID 21-3061)
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study presented in this manuscript was supported by the Robert Wood Johnson Foundation Health Equity Scholars for Action program under grant #79244
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data collected for the study discussed in this manuscript are not publicly available.