
Abstract
Occupation-centered lifestyle interventions improve health and delay age-related declines in older adults; however, little is known about the impact of a brief telehealth lifestyle program delivered individually. This pilot investigated the Holistic Occupational Performance Empowerment (HOPE) program on occupational performance and health-related quality of life. Twelve community-dwelling older adults completed six weekly lifestyle sessions to enhance behavior change toward individualized health goals. Goal Attainment Scaling (GAS) and the Short Form 20-Item Survey (SF-20) were administered preintervention and postintervention to measure program outcomes. Among 36 health-related goals, 69.4% achieved or exceeded the expected level of attainment. A paired samples t-test revealed statistically higher posttest GAS scores compared with pretest scores, indicating significant improvements in occupational performance. SF-20 mental health scores increased postintervention, although not significantly. Preliminary findings suggest that HOPE could positively impact occupational performance in community-dwelling older adults warranting a future large-scale randomized controlled trial.
Plain Language Summary
Previous occupational therapy (OT) programs focusing on lifestyle (e.g., physical activity, stress management) have been successful in improving the health of seniors living independently in the community; however, little is known about lifestyle programs delivered virtually (i.e., videoconferencing over the computer). This article examines the meaningful daily activities of seniors before and after participation in a 6-week virtual OT lifestyle program. Twelve seniors participated in the program which included goal setting, problem-solving, health education, and reflection. Each participant focused on three personalized goals for a healthier lifestyle throughout the program. Nearly 70% of goals achieved or exceeded the expectations of the seniors. This initial finding shows that the virtual OT lifestyle program can positively impact seniors and support healthy aging. More research is needed to determine if the results can be replicated with other seniors, including those from diverse backgrounds and living situations.
Keywords
Nearly 95% of older adult Americans live with at least one chronic disease and 80% manage multiple conditions (National Council on Aging, 2023). The health and social needs of older adults become increasingly complex with age, adverse life events, diminishing social networks, financial hardship, and medical comorbidities (National Institute on Aging, 2020). Chronic diseases are the leading causes of death and disability in the United States, contributing to 90% of the nation’s US$4.3 trillion in health care costs (Centers for Medicare and Medicaid Services, 2022; Kockanek et al., 2024). Despite spending far more than other high-income countries, the United States ranks last on health care outcomes and access to care (Schneider et al., 2021). An aging population, a society burdened with diseases, and escalating costs present an urgent need for health care reform.
Health promotion and prevention services will be critical as consumers, health professionals, payors, policy makers, and others navigate a new health care paradigm toward value-based care and reimbursement (Sadek et al., 2023). Interprofessional collaboration focusing on chronic condition management improves overall health and life satisfaction, and it is supported by national legislation and health initiatives, like the Affordable Care Act and Healthy People 2030 (Office of Disease Prevention and Health Promotion, n.d.). Occupational therapy practitioners are uniquely suited to address the impact chronic conditions have on health and engagement in meaningful daily activities (Fields & Smallfield, 2022; Lambdin-Pattavina & Pyatak, 2023). Occupational therapy services are well-documented in promoting health and improving occupational performance, quality of life, and well-being in community-dwelling older adults (Berger et al., 2018; Pyatak et al., 2022).
Occupational therapy practitioners utilizing a health promotion approach may ground their practice in a variety of intervention frameworks including lifestyle medicine or Lifestyle Redesign®. Lifestyle medicine is an interprofessional discipline incorporating lifestyle change as the primary modality to address the root causes of chronic disease (Clayton & Bonnet, 2023). Most chronic diseases are preventable and can be linked to at least one lifestyle behavior: tobacco use, poor nutrition, physical inactivity, and excessive alcohol use (Centers for Disease Control and Prevention, 2022). Lifestyle medicine professionals use health behavior change interventions to treat, prevent, and—when used intensively—reverse chronic health conditions by targeting these modifiable behaviors (Clayton & Bonnet, 2023).
Lifestyle Redesign is an approach to health promotion specific to the field of occupational therapy which fosters sustainable lifestyle change by creating habits and routines and engaging in meaningful occupations (Clark et al., 2015). Based on the Well Elderly studies, 6 to 9 months of Lifestyle Redesign improved occupational functioning and quality of life, delayed age-related declines, and reduced health care costs for community-dwelling older adults (Clark et al., 1997, 2012). The approach has since expanded to different populations, health conditions, settings, and modes of delivery both in research and clinical practice (Pyatak et al., 2022). Lifestyle Redesign has demonstrated clinically relevant and cost-effective outcomes; however, it has not been widely accepted within occupational therapy practice because the original program was perceived as costly of time and resources (Cassidy et al., 2017; Takagi et al., 2022). Broader adoption of health promotion by the profession has been further challenged by a dearth of practitioners working in community settings, poor reimbursement, and limited support from larger health systems (Cassidy et al., 2017; Sadek et al., 2023).
A lifestyle program of shorter duration may overcome these potential barriers and be more acceptable to clients, practitioners, and payors alike. Two studies conducted outside of the United States reported promising findings of occupation-centered, health promotion interventions consisting of one to four sessions (Takagi et al., 2022; Zingmark et al., 2014). Furthermore, a lifestyle program delivered virtually may present a viable solution to curb the myriad challenges often faced by older adults with chronic conditions, such as mobility impairments (Pyatak et al., 2022). Telehealth delivery increases access to services, reduces costs, and produces positive health outcomes while providing comparable satisfaction to face-to-face models (Feldhacker et al., 2022; Mitchell et al., 2023).
The Holistic Occupational Performance Empowerment (HOPE) program is a brief occupation-centered, lifestyle-focused intervention designed for individual telehealth delivery. HOPE includes aspects of both lifestyle medicine and Lifestyle Redesign and was developed for the prevention and management of chronic conditions in community-dwelling older adults. This study investigated the program feasibility of HOPE and examined preliminary outcomes of occupational performance and health-related quality of life.
Method
Research Design
This nonrandomized pilot study utilized a single-group, pretest–posttest design. The Creighton University Institutional Review Board approved all procedures, and the study was registered at ClincialTrials.gov. All participants provided informed consent prior to their involvement.
Participants
Participants were recruited through advertisements posted at health, fitness, and community centers in nonurban towns located in two northwest states. Additional recruitment occurred through chain-referral and purposive sampling. Interested participants contacted the researchers to complete a telephone screening. Eligible participants were English-speaking, community-dwelling adults aged 65 years or older, were independent with activities of daily living, had adequate vision and technology skills to participate in a telehealth intervention, and lived within 40 miles of an interventionist (first or second author). Because the program was developed for the prevention and management of chronic conditions, participants with and at risk for chronic conditions qualified for HOPE. Participants were excluded if they scored less than 12 on the telephone version of the Montreal Cognitive Assessment (Version 2.1; Nesreddine, 2021), indicating mild cognitive impairment.
Measures
Feasibility
To assess feasibility, the researchers collected data on recruitment and program attendance. Session length was recorded weekly and total treatment time was calculated postintervention for each participant. Potential adverse events and study complications were also documented.
Participant Demographics
Participants completed a sociodemographic questionnaire to collect information on gender, age, race, education, annual household income, living situation, assisted household activities, other health services provided, number of medications self-administered, and number of self-reported chronic conditions (Table 1). They also completed the Short Assessment of Health Literacy–English (SAHL-E) which measures health literacy of English-speaking adults by assessing pronunciation and comprehension of 18 common medical terms (Lee et al., 2010). Scores on the SAHL-E range from 0 to 18, with scores of 14 or below indicating low health literacy. The internal consistency (α = .89, p < .05) and content validity (r = .94, p < .05) of the SAHL-E are good (Lee et al., 2010). The SAHL-E was conducted at baseline only to inform the delivery of HOPE and support behavior change and health-related outcomes (Stormacq et al., 2020).
Sociodemographic Characteristics of Participants at Baseline.
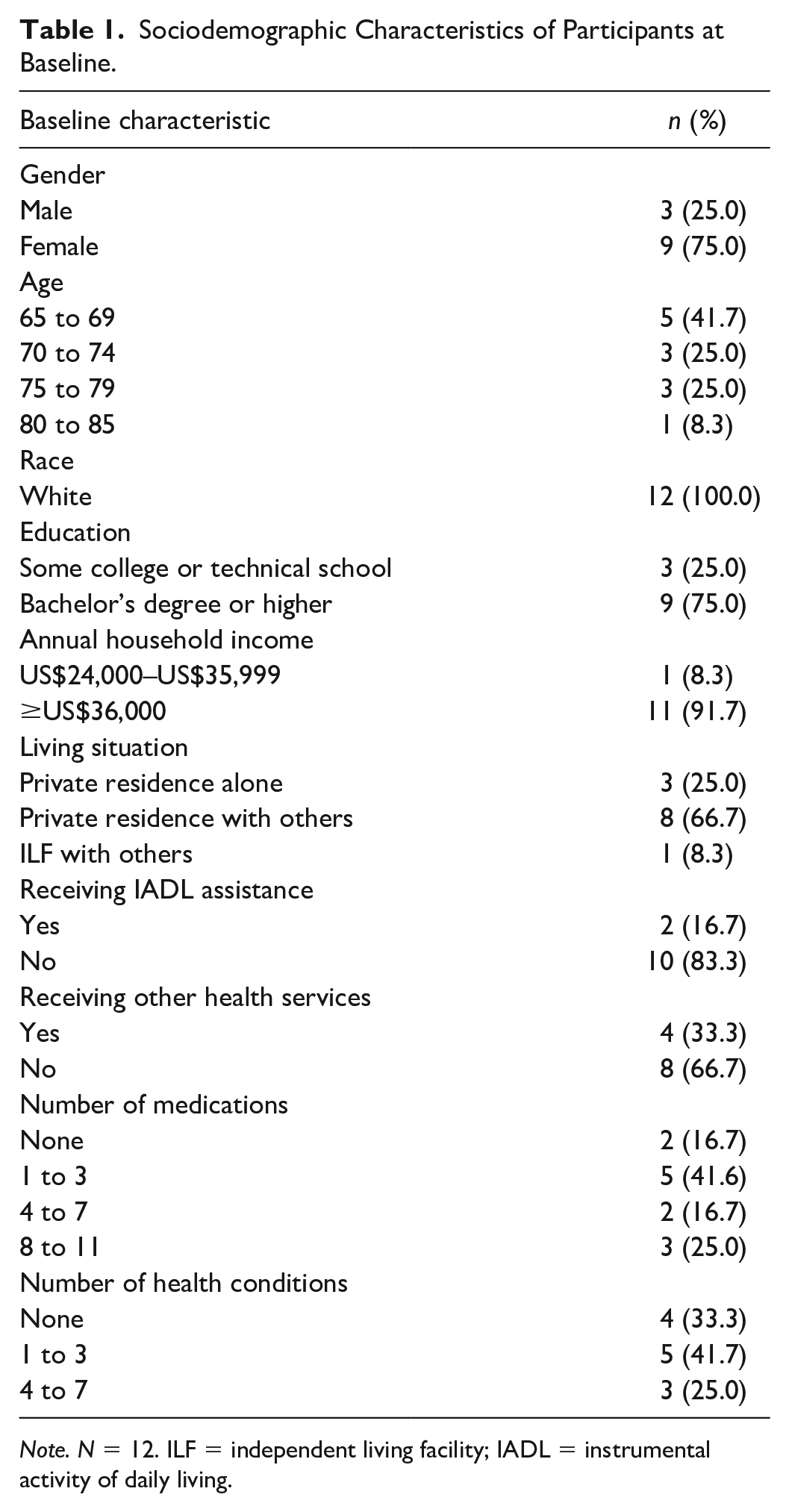
Note. N = 12. ILF = independent living facility; IADL = instrumental activity of daily living.
Primary Outcomes
Goal Attainment Scaling
Goal attainment scaling (GAS) is a method for measuring goal progression achieved during an intervention (Turner-Stokes, 2009). GAS utilizes a 5-point Likert-type scale ranging from −2 to +2 where higher scores indicate greater goal attainment. Baseline scores are set at either −2 or −1 depending on the level of functioning preintervention. Participants rate their goals postintervention capturing the degree of attainment achieved: −2 (much worse than expected), −1 (somewhat worse than expected), 0 (as expected), +1 (somewhat better than expected), or +2 (much better than expected). Goals are weighted based on importance and achievement difficulty, then standardized into an aggregated goal attainment T-score. GAS has acceptable interrater reliability (ICC = .83) and is commonly used within mental health, rehabilitation, and geriatric settings (Marson et al., 2009). GAS was conducted preintervention and postintervention to assess change in occupational performance.
Short Form 20-Item Survey
The Short Form 20-Item Survey (SF-20) measures health-related quality of life (HRQoL) along six subscales: physical functioning, role functioning, social functioning, mental health, current health perceptions, and pain (RAND Corporation, n.d.). Subscales vary with responses rated on 3- to 6-point Likert-type scales. Five subscales are scored with the highest score representing the best possible outcome (i.e., highest functioning); however, the lowest score on the pain subscale represents the best possible outcome (i.e., no pain). It has good internal consistency (α = .81–.88, p < .01; Stewart et al., 1988) and excellent test–retest reliability (ICC = .96; Carver et al., 1999). The SF-20 was conducted preintervention and postintervention to assess change in HRQoL.
Intervention
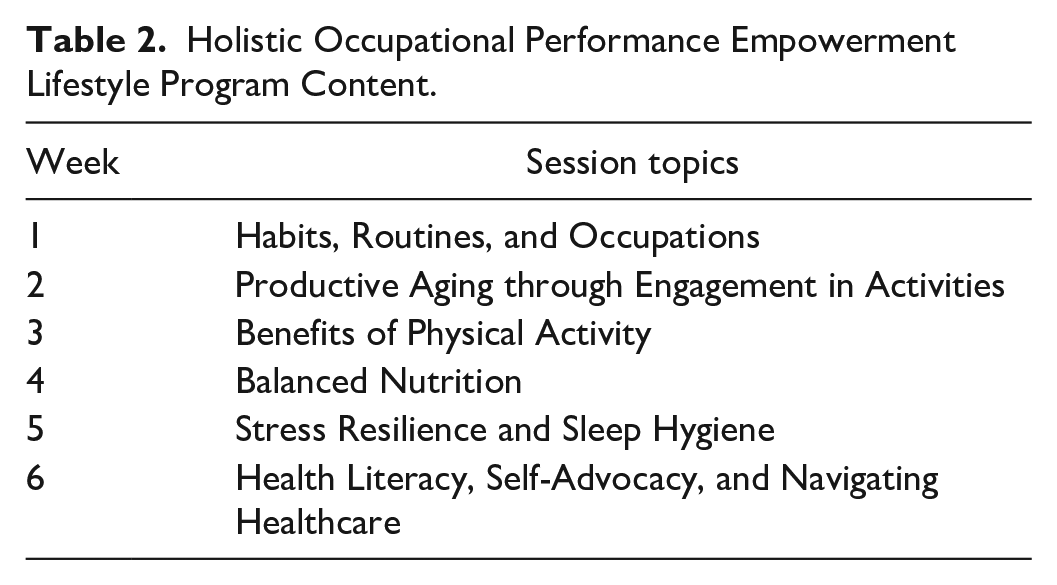
HOPE is an occupation-centered, lifestyle-focused health promotion intervention designed for individual telehealth delivery using HIPAA-compliant Zoom software (Version 5.12.2, https://zoom.us). HOPE consisted of six sessions provided weekly across 6 weeks with all participants following the same program sequence. Contrary to early Lifestyle Redesign trials (Clark et al., 1997, 2012), HOPE’s shorter duration was based on newer literature (Takagi et al., 2022; Zingmark et al., 2014) and the need for time- and cost-effective lifestyle programs (Cassidy et al., 2017). Sessions were planned for 45 to 60 minutes and each focused on a different lifestyle topic (Table 2).
Holistic Occupational Performance Empowerment Lifestyle Program Content.
Two evidenced-based lifestyle frameworks informed the development of HOPE: lifestyle medicine and Lifestyle Redesign. To facilitate health behavior change consistent with a person-centered approach, HOPE incorporated coaching principles from motivational interviewing, appreciative inquiry, and positive psychology (Miller & Rollnick, 2023; Moore et al., 2015). Readiness for change was assessed throughout the program according to the Transtheoretical Model (Prochaska & DiClemente, 1983). Session topics aligned with the six pillars of lifestyle medicine (Clayton & Bonnet, 2023), while therapeutic activities were adapted from the Lifestyle Redesign manual (Clark et al., 2015). While working toward advanced lifestyle training (American College of Lifestyle Medicine, n.d.; Chan Division of Occupational Science and Occupational Therapy, University of Southern California, n.d.), the first and second authors developed the program and delivered the intervention. To ensure systematic delivery, a fidelity checklist adapted from Borrelli et al. (2005) was utilized after every session (Table 3).
Treatment Fidelity Checklist.
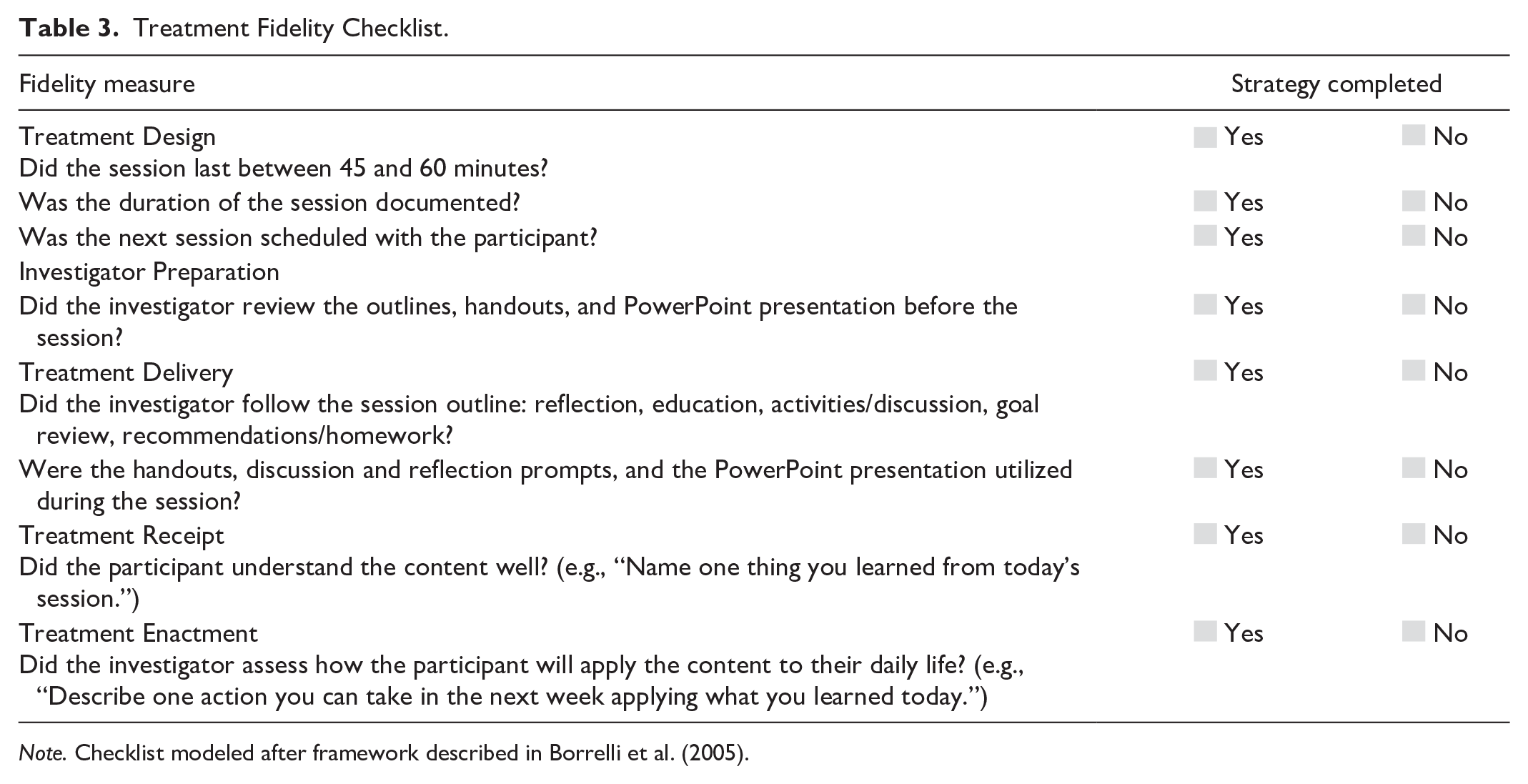
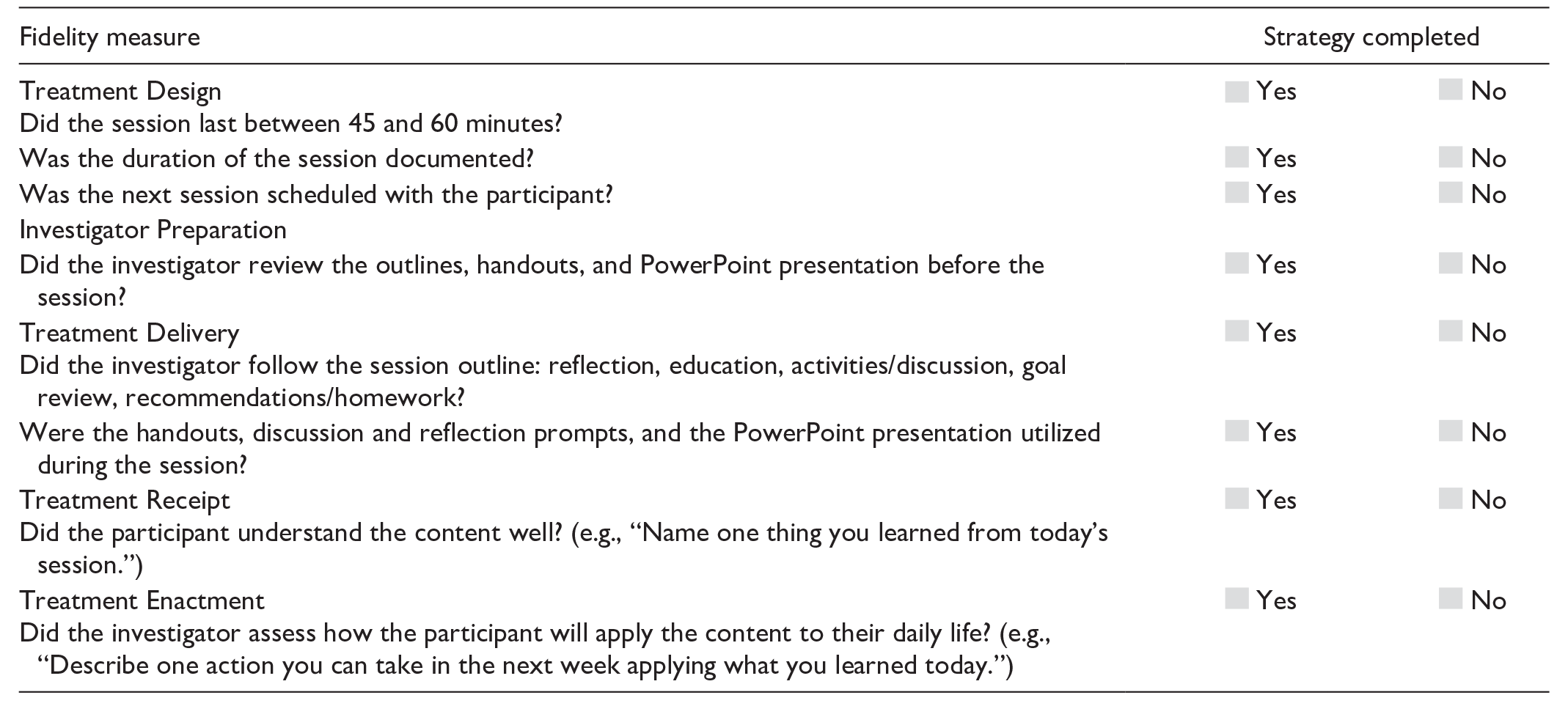
Note. Checklist modeled after framework described in Borrelli et al. (2005).
Data Analysis
Data were analyzed using IBM SPSS Statistics (Version 28; IBM Corporation). Descriptive statistics for categorical variables (e.g., gender, living situation) were represented as ns and frequencies, whereas continuous variables (e.g., GAS, SF-20) were expressed as mean values and standard deviations (SD). Change scores for the primary outcome measures were analyzed using a paired samples t-test or a Wilcoxon signed-rank test, depending on whether data followed a normal distribution.
To determine whether a dosage effect existed, associations between GAS and SF-20 change scores with average session length and total treatment time were analyzed using Spearman correlations. An independent samples t-test was conducted to examine significant differences in GAS and SF-20 change scores among sociodemographic characteristics, while Pearson correlations assessed associations between health literacy scores. A p < .05 was considered statistically significant.
For a pilot investigation where no known prior information exists to justify sample size calculations, a minimum of 12 participants per group is recommended based on feasibility, precision about the mean and variance, and regulatory considerations which will inform an appropriately powered future clinical trial (Julious, 2005).
Results
Of the initial 23 individuals interested in HOPE, 12 participants completed pretest and posttest measures. Seven individuals chose not to participate because of personal reasons (e.g., time commitment, scheduling conflicts) while another four did not meet the study’s inclusion criteria. Participant flow is detailed in Figure 1. Ten participants completed six sessions and two participants completed five sessions. No adverse events occurred because of the intervention; however, one participant had scheduled surgery and two others reported falls, one with a minor injury. Among the 70 treatment sessions completed, only one experienced a technology delay due to a software update.
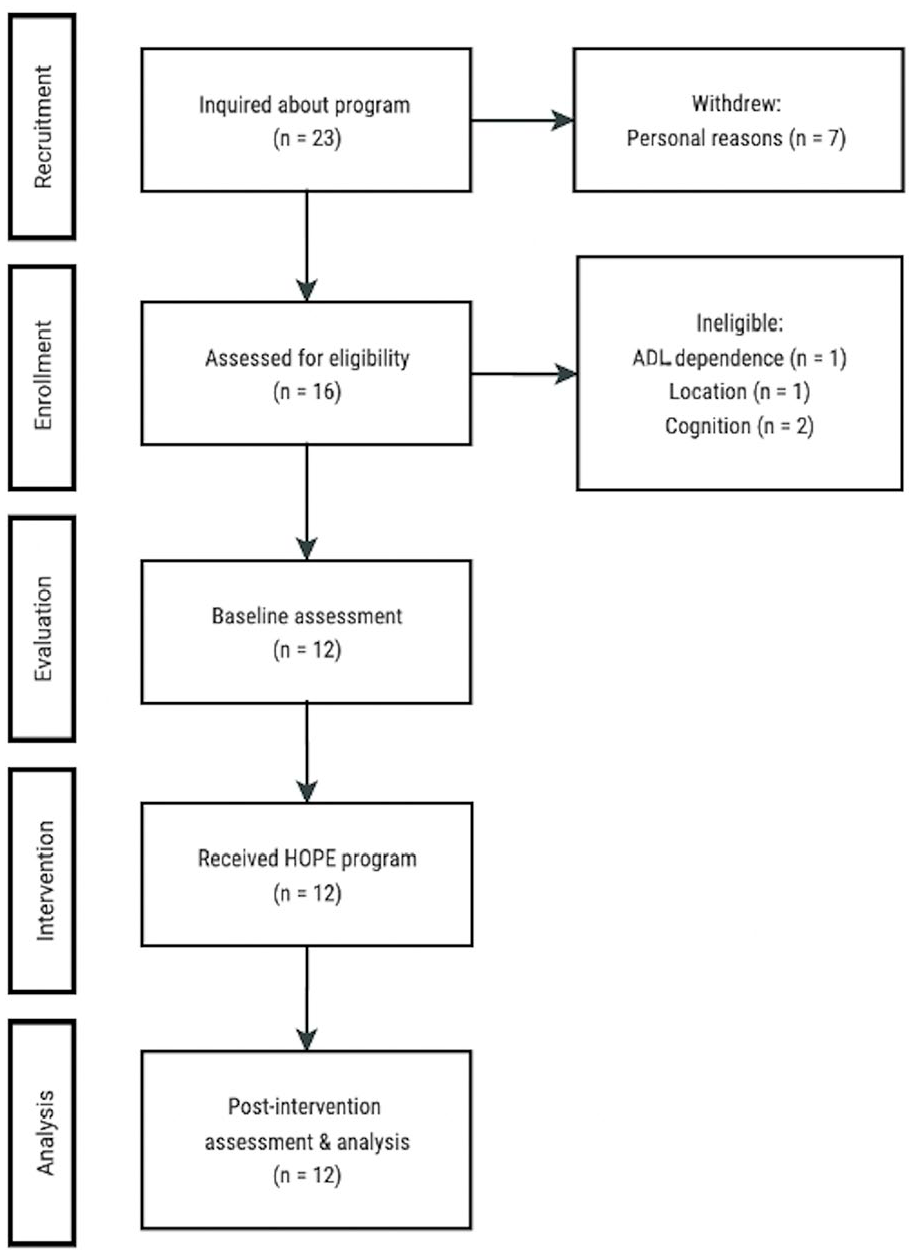
Participant Flow.
Sociodemographic characteristics of the participants at baseline are presented in Table 1. The participants included nine women and three men aged 65 to 85 years who were all White with greater than a high school education. Four participants received other health care services during the intervention (e.g., dietician). Two-thirds of participants reported at least one health condition, while one-third reported none. All participants scored 16 or higher on the SAHL-E, indicating adequate health literacy.
Occupational Performance
Each participant identified three occupation-centered, lifestyle-focused goals, resulting in 36 health-related goals. Goals related to nutrition (n = 14), physical activity (n = 9), self-management routines (n = 5), sleep (n = 4), social connectedness (n = 3), and stress management (n = 1). Progress was made in 94.4% of established goals, with eight of 36 (22.2%) goals achieving an expected level of attainment and 17 of 36 (47.2%) goals exceeding an expected level of attainment. Aggregate posttest GAS scores were 28.43 points higher than pretest GAS scores (Table 4). Participants had statistically significant increases in occupational performance following completion of HOPE as demonstrated by a paired samples t-test (p < .001).
Mean Values and Standard Deviations of Scores on Primary Outcome Measures.
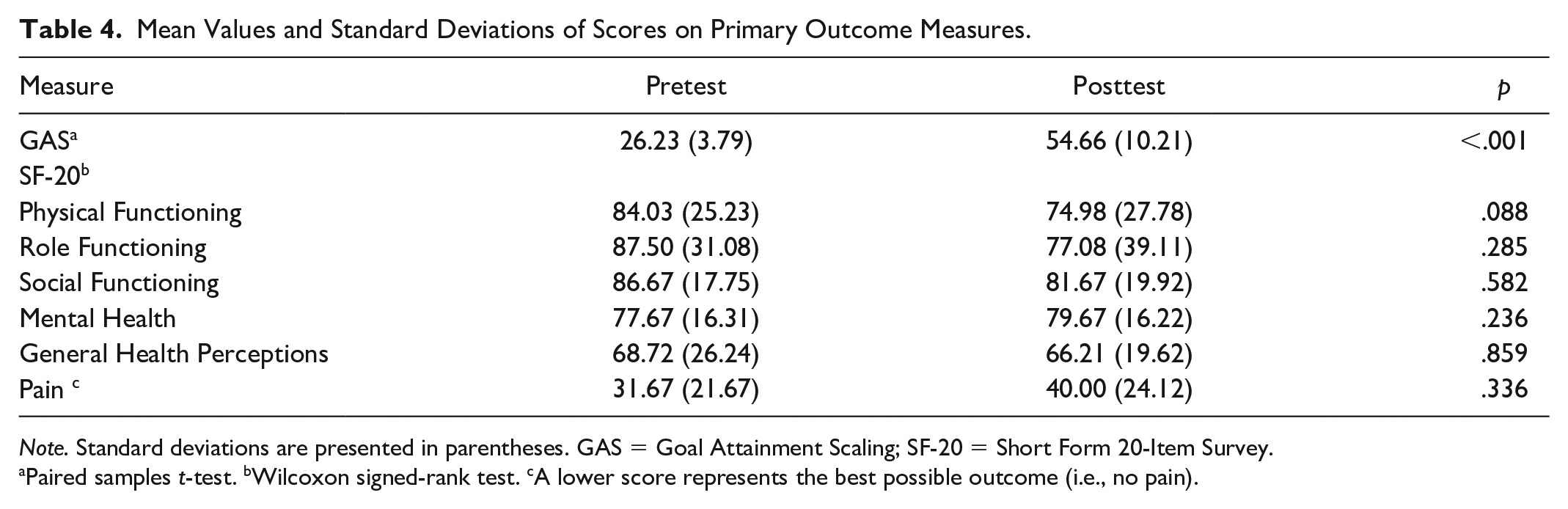
Note. Standard deviations are presented in parentheses. GAS = Goal Attainment Scaling; SF-20 = Short Form 20-Item Survey.
Paired samples t-test. bWilcoxon signed-rank test. cA lower score represents the best possible outcome (i.e., no pain).
Health-Related Quality of Life
One of the six SF-20 subscales showed an improvement postintervention (Table 4). Specifically, mental health scores increased by 2.00 points on average from pretest to posttest, but this change was not statistically significant (p = .236). Mean posttest scores of the other five SF-20 subscales declined compared with mean pretest scores, but none of these changes were statistically significant by a Wilcoxon signed-rank test (p = .088–.859).
Dosage
Participants attended an average of 5.8 sessions (SD = 0.39, range 5–6) with a mean length of 66.7 minutes (SD = 12.8; range 45.8–94.2). Participants averaged a total treatment time of 390.8 minutes (SD = 87.7; range 263–565) throughout the HOPE program. In examining whether a dosage effect occurred with GAS change scores, a Spearman correlation indicated that no such association existed for either average session length (r = −.189, p = .556) nor total treatment time (r = −.089, p = .783).
Relationships Between Participant Demographics and Primary Outcomes
Assuming normality for GAS scores, an independent samples t-test revealed no significant correlations between the sociodemographic characteristics. A moderate positive correlation was observed between GAS change scores and SAHL-E health literacy scores, but it did not reach the previously established significance level (r = .460, p = .132). No significant findings occurred between the SF-20 and the SAHL-E nor any other participant demographics.
Discussion
This study examined a brief occupation-centered, lifestyle-focused program delivered individually via telehealth. Preliminary results indicated HOPE contributed to an improvement in occupational performance among community-dwelling older adults with or at risk for chronic conditions. This finding aligns with previous lifestyle studies supporting the use of personalized goal setting for measuring occupational performance (Salar et al., 2022). The development of personally meaningful goals increases motivation, engagement, and ownership which subsequently improves self-efficacy and therapeutic outcomes (Kang et al., 2023). HOPE utilized a person-centered, collaborative-coaching approach while focusing on performance patterns and lifestyle-related challenges (Pyatak et al., 2022).
Lifestyle interventions have shown improvements in HRQoL in various populations (Clark et al., 2012; Uyeshiro Simon, & Collins, 2017). Contrary to these studies, HOPE revealed nonsignificant findings for the SF-20. Discrepancies may be explained by a small sample size, lack of a control group, or methodological differences. Nonetheless, current findings were consistent with a previous lifestyle intervention that also lacked significant HRQoL improvements (Levasseur et al., 2019). Postintervention scores from all SF-20 subscales showed downward trends except for mental health. Declines in scores may be attributed to participants’ greater awareness of their impairments (Levasseur et al., 2019). Although an appropriate outcome to measure in older adults with chronic conditions, there is limited research for occupational therapy telehealth interventions focusing solely on HRQoL (Feldhacker et al., 2022).
Only three studies exist within the occupational therapy lifestyle literature examining individual sessions without a group component, none of which investigated an intervention specifically for older adults (Mitchell et al., 2023; Pyatak et al., 2019; Uyeshiro Simon & Collins, 2017). In reviewing broader health promotion interventions for community-dwelling older adults, Berger et al. (2018) found significant improvements can be produced without a group format. Therefore, mechanisms supporting behavior change during HOPE may lie within the therapeutic approaches and activities implemented; for example, goal setting, health education, action planning, problem-solving, reflection, and skills training may contribute to self-efficacy and goal attainment (Berger et al., 2018; Bricca et al., 2023).
Limited studies within the occupational therapy lifestyle literature have utilized a telehealth component (Mitchell et al., 2023; Schepens Niemiec et al., 2018). Feasibility findings from HOPE coincided with recent telehealth studies containing similar intervention characteristics, such as lifestyle medicine education (Alothman et al., 2023), occupational performance coaching (Kessler et al., 2021), and a Lifestyle Redesign approach (Mitchell et al., 2023). Kessler and colleagues (2021) asserted the strength of the therapeutic relationship remained high with telehealth delivery. Moreover, Kang et al. (2023) reported high satisfaction, engagement, and person-centeredness with telehealth goal setting for adults with chronic conditions leading to positive feasibility findings.
Most lifestyle-focused health promotion programs for community-dwelling older adults have spanned 2 to 9 months (Cassidy et al., 2017; Clark et al., 1997, 2012; Lévesque et al., 2019; Maier et al., 2021). Berger et al. (2018) suggested individual health promotion programs should comprise multiple visits over at least 3 months. However, other researchers contended that briefer interventions are needed for translation to clinical practice (Cassidy et al., 2017; Takagi et al., 2022). The dosage of HOPE was consistent with previous studies demonstrating the feasibility of programs with few sessions implemented over a short duration (Takagi et al., 2022; Zingmark et al., 2014).
Despite variable amounts of total treatment time provided to participants, correlational analyses revealed no dosage effect for changes in occupational performance. Thus, significant improvements in GAS scores more likely occurred because of the lifestyle content and a strong therapeutic relationship (Kessler et al., 2021). This underscores the importance of HOPE delivered by an occupational therapy practitioner whose clinical judgment and specialized expertise determined the appropriate length of each session and treatment focus for each participant (Pyatak et al., 2022; Uyeshiro Simon & Collins, 2017). A duration of 6 weeks is often considered clinically appropriate and aligns with reimbursement dictated by third-party payers Leverentz & Salvati, 2024.
Many participants underreported their health conditions on the background questionnaire, disclosing additional conditions throughout the intervention. For example, hypertension was not perceived as a chronic condition since well-controlled by medication. Despite adequate health literacy scores, individuals may have limited knowledge of their conditions or available treatment options leading to poor self-management (Amdie & Woo, 2020). Contentment with medical recommendations (e.g., prescription medications) instead of seeking suitable alternatives (e.g., lifestyle modification) that are cost-effective with less adverse side effects may result. Traditional medical providers also cite a lack of confidence, knowledge, and skills regarding lifestyle recommendations, including exercise prescription (Rea et al., 2021). Furthermore, the strained health care system in the United States limits time and reimbursement when providing preventive care (Rea et al., 2021; Sadek et al., 2023).
HOPE possessed many strengths which led all participants to successfully complete the program without any attrition. Individual sessions promoted person-centered care, tailored treatment planning, and flexible scheduling (Uyeshiro Simon & Collins, 2017). Telehealth delivery increased program access despite existing or potential barriers like illness, transportation, or weather (Feldhacker et al., 2022). High attendance suggested the dosage of HOPE was acceptable to participants adding to its feasibility (Cassidy et al., 2017).
Limitations and Implications for Future Research
While appropriate for a pilot, this study had a small sample size and lacked a control group. Therefore, improvements in occupational performance could be attributed to other factors besides participation in HOPE. Future lifestyle research should consider a larger sample size and a randomized controlled design. In addition, incorporating a longitudinal component could assess long-term behavior change, whereas a mixed-method design could add depth and nuance to participants’ experiences, contributing further to HOPE’s feasibility.
There is evolving evidence that GAS can be utilized in research, yet some critics argue it produces potential bias secondary to subjective goal scoring (Krasny-Pacini et al., 2016). To prevent bias, the researchers ensured all goals were specific, measurable, achievable, realistic, and timely. Collaborative goal setting and goal management were inherent to the program’s person-centered approach. Future studies could also consider using an alternative or complementary outcome measure, like the Canadian Occupational Performance Measure (Law et al., 1998).
The first and second authors developed the program, delivered the intervention, and collected data. Regular fidelity measures attempted to counter any experimenter bias and ensure consistent delivery of the lifestyle content. Nonetheless, having the developer serve as the delivery agent the first time an intervention is tested can be useful regarding modifications for future scalability (Beets et al., 2021). Selection bias may have occurred if participants enrolled hoping to improve their health and lifestyle. Convenience sampling resulted in a homogeneous sample which limits generalizability of findings to other populations of community-dwelling older adults. Future programs should consider populations at greater risk for health declines and those with diverse sociocultural backgrounds.
Conclusion
This study examined the preliminary outcomes and program feasibility of HOPE, a telehealth lifestyle intervention combining aspects of lifestyle medicine and Lifestyle Redesign. Results indicated that HOPE contributed to an improvement in occupational performance among community-dwelling older adults with or at risk for chronic conditions. HOPE was deemed acceptable by participants and feasible to deliver as a brief and individualized telehealth program. This work contributes to the growing body of literature demonstrating a relationship between lifestyle, occupational performance, and health. Future research should explore readiness for change and social determinants of health to ascertain which populations would benefit most from lifestyle interventions. A large-scale randomized controlled trial is warranted to further evaluate the efficacy of HOPE.
Footnotes
Acknowledgements
The authors acknowledge and extend their appreciation to the study participants, as well as to Dr. Brenda Coppard and Dr. Donna Mann for their mentoring and expertise.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported in part by American College of Lifestyle Medicine Unrestricted Trainee Research Grant.
Ethical Approval
This study was registered at ClinicalTrials.gov (Identifier NCT05462626) on July 15, 2022, and it received ethical approval by the Institutional Review Board at Creighton University (#2002841) on September 23, 2022.