
Abstract
The aim of the present study was to explore health-related quality of life (HRQoL) and associated variables among all community-dwelling older women (≥65 years) (n = 2724) on Åland, a Finnish self-governing island community. A total of 1023 women participated (mean age 72.9 ± 6.8 years). Absence of depression, absence of diagnosed disease(s), having the opportunity to engage in meaningful leisure activities, and never or seldom feeling lonely explained, together with socio-economic control variables (i.e. age, education and economic situation), 34.4% of the variation in physical health. Absence of depression, strong inner strength, and never or seldom feeling lonely explained, together with socio-economic control variables, 27.7% of the variation in mental health. HRQoL was rated as relatively good, although special attention should be paid to women aged 80+years. To promote HRQoL, interventions aimed at preventing, detecting and treating depression should be prioritised. In addition, interventions aimed at reducing feelings of loneliness are also recommended in order to enhance overall HRQoL.
Introduction
All nurses have a fundamental responsibility to promote health. 1 The mission of health promotion is to be fulfilled at individual, group and societal level, and it is based on the premise that health is more than just absence of disease. Health-promoting activities focus on the person’s life-world in relation to health, illness and suffering, and are assumed to be permeated by dialogue, participation and equality. 2 The need for health-promoting activities is growing in importance as life expectancy increases in all countries in northern Europe. 3 In the Nordic countries there have been cut-backs in institutional care and older people are now expected to live at home.4–6 For nurses, and also from a societal perspective, the promotion of health-related quality of life (HRQoL) among community-dwelling older persons is potentially an area deserving attention, in respect of poor self-rated health and of health service utilisation and hospitalisation.7,8
Ideally, every person should remain independent and active for as long as possible, yet older people are a very heterogeneous group with an individual diversity that increases with age. 9 In general, women live longer, 10 are more disabled and report more health problems than men.10,11 Older women are also more likely to live alone,11–13 which has been associated with frailty, 13 lower life satisfaction, and lower income level. 14
From a public health perspective, it is of interest to know more about health-related quality of life (HRQoL) in order to be able to support older people and for society to better deal with the challenges that come with an ageing population. To enhance health in older women Åland is of specific interest to study as it is known that the morbidity index for this province is the lowest in Finland. 15 Also, compared with other Nordic countries, women in Åland are expected to live longest, with a longevity in excess of 84 years. 16 Identifying factors related to better self-rated health indicates for nurses areas of possible health-promoting activities in the target group. The aim of this study was therefore to explore health-related quality of life and associated factors among community-dwelling older women.
Material and methods
This was a descriptive, population-based, cross-sectional study.
Setting
The study was conducted on Åland, a Finnish island community in the Baltic Sea with approximately 28,900 inhabitants. The island community is a self-governing, Swedish-speaking area. As in other Nordic countries, health-care is publicly provided and largely financed by taxes, and there are well-established systems for primary care. 3
Sampling and participants
Every woman registered at the Local Register Office on Åland and of age 65 years or older (n = 2724) was sent a questionnaire in May 2010. Of these, 57% returned their questionnaires after one reminder (n = 1555). Those who lived in service flats or nursing homes or who had not registered their housing condition were excluded (n = 84). The main interest was HRQoL, so non-respondents to the SF-12 Health Survey were also excluded (n = 448). This gave a total of 1023 participants with a mean age of 72.9 ± 6.8 years. The non-respondents to the SF-12 Health Survey were significantly older (76.4 ± 7.2 years) than the respondents (p < 0.001), less likely to be married or divorced and more likely to be widowed (p < 0.05). The mean age of those who did not return the questionnaire (n = 1,169) was 77.7 ± 8.8 years.
Questionnaire
The questionnaire was sent by post together with a prepaid response envelope and a letter containing general information about the study plus information about consent. The questionnaire included the following:
HRQoL. The SF-12 Health Survey
17
was used to describe HRQoL. Some items are scored as absent/present while others are scored on a Likert scale, with ranges varying from item to item. Two sum-scores are generated: the physical component summary (PCS, physical health) and the mental component summary (MCS, mental health), with both having a potential score in the range 0–100. Higher scores indicate higher HRQoL. The survey has been shown to be psychometrically valid and reliable among independent-living older adults.17,18 No missing values were accepted when analysing the results. Social variables were explored by asking about whether respondents were co-habiting, had children or had someone close to share both troubles and joy with. The response options were Yes or No. Physical variables were explored by asking whether respondents had a diagnosed disease and whether they had the opportunity to engage in meaningful leisure activities. The response options were Yes or No. Emotional variables. The Geriatric Depression Scale (GDS) was used to estimate depression. In this study, the 15-item version was used with a potential range of scores from 0 to 15. Scores ≥ 5 indicate depression.
19
The 15-item version of the GDS is a well-validated tool for screening depression in older adults.
19
When analysing the results, no missing values were accepted. There was also a question ‘Do you feel needed?’ with the response options Yes or No, and a question ‘Do you feel lonely?’ with four response options that were dichotomised as Yes (often or sometimes feel lonely) or No (seldom or never feel lonely). Variables related to dealing with adversity. The ability to deal with adversity was measured by the Inner Strength Scale (ISS).
20
The ISS is a Likert scale with 20 questions, and items range from 1 to 6. All items are phrased positively and the scores range from 20 to 120, with higher scores denoting stronger inner strength. The ISS has been found to be a valid and reliable instrument for obtaining a multifaceted understanding of inner strength.
20
When analysing the results, three missing values were accepted and were replaced with the mode value of the respondents. Socioeconomic control variables are standard explanatory variables: i.e. age, marital status (married/not married), education (higher education, i.e. studies beyond elementary school, or not) and economic situation (the respondents finished the sentence ‘Regarding my finances …’ and the three response options were dichotomised as ‘Yes, I have enough money to cover costs and to save some’, ‘I have enough money but there is nothing left’, interpreted as having enough money for personal needs, or ‘No, I do not have enough money’).
Statistics
SPSS version 21.0 was used for statistical calculations. One-way between-groups analysis of variance (ANOVA) was performed to explore the impact of age on physical and mental health. Effect size was calculated by means of eta squared, and the result was interpreted according to Cohen, 21 with 0.01 being a small effect, 0.06 being a medium effect, and 0.14 being a large effect. Bonferroni correction was used for post-hoc comparisons. The independent t-test was used to compare participants with or without specific characteristics. A p-value of < 0.05 was regarded as statistically significant. Significant variables were included in multiple regression modelling, together with socioeconomic controls, in order to find factors that independently explained the variance in the PCS and MCS scores. The independent variables were tested for multicollinearity, outliers, normality and linearity. Marital status strongly correlated with co-habiting (r = 0.87), and was therefore excluded. In the final models, the variables that independently explained the variance in the dependent variable are presented.
Ethical considerations
The project was approved by the ethical committee of Åland’s Public Healthcare Service. A letter enclosed with the questionnaire described the voluntary nature of participation, the confidentiality of the data and presentation of the results. A completed questionnaire was regarded as consent to participate.
Results
Mean values of the PCS and MCS scores for socioeconomic control.
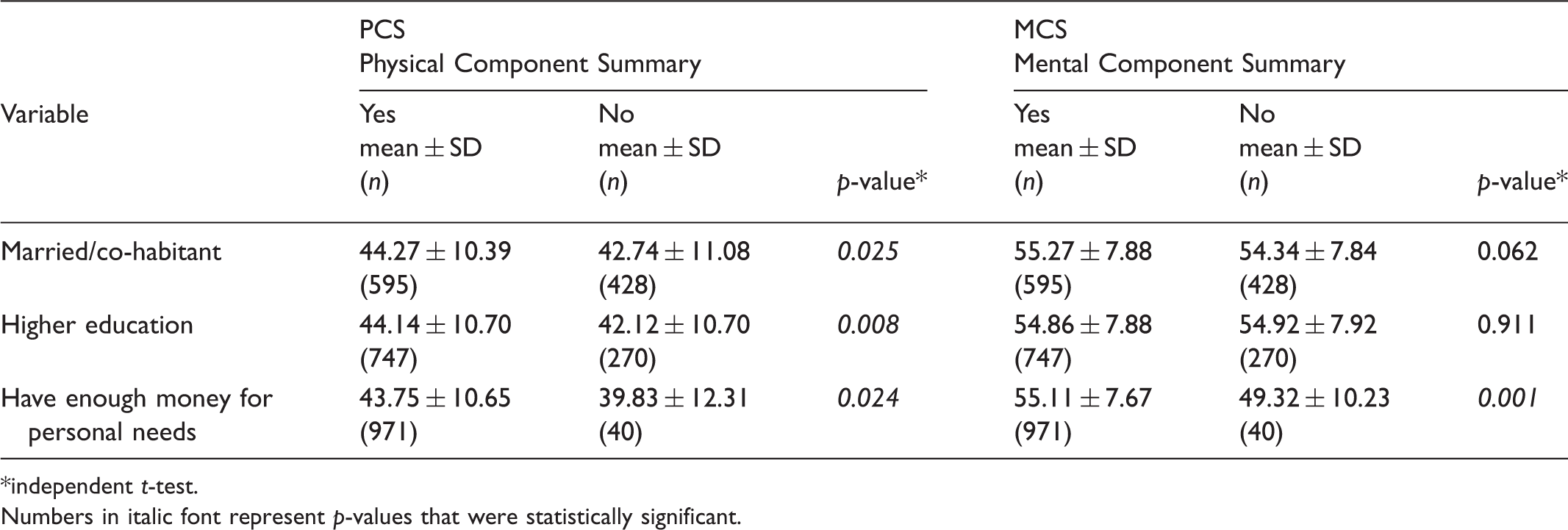
independent t-test.
Numbers in italic font represent p-values that were statistically significant.
Total scores on the PCS 1 for participants with or without specific characteristics.
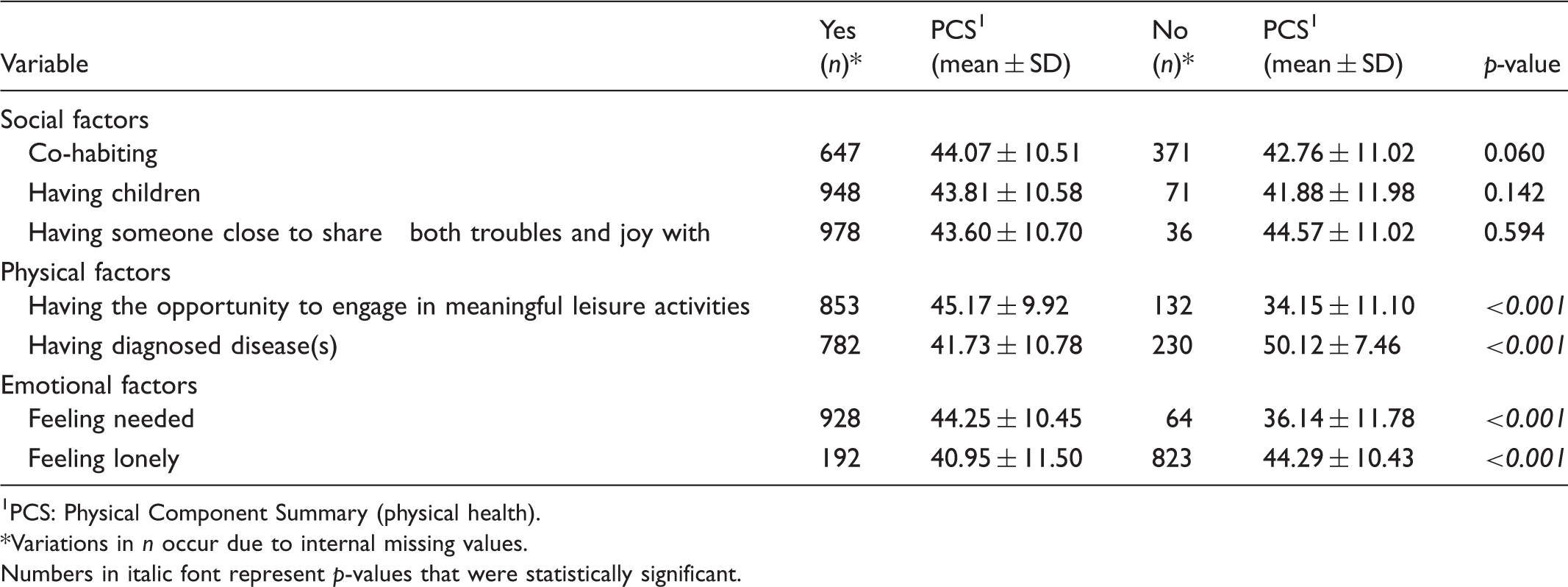
1 PCS: Physical Component Summary (physical health).
Variations in n occur due to internal missing values.
Numbers in italic font represent p-values that were statistically significant.
Total scores on the MCS 1 for participants with or without specific characteristics.
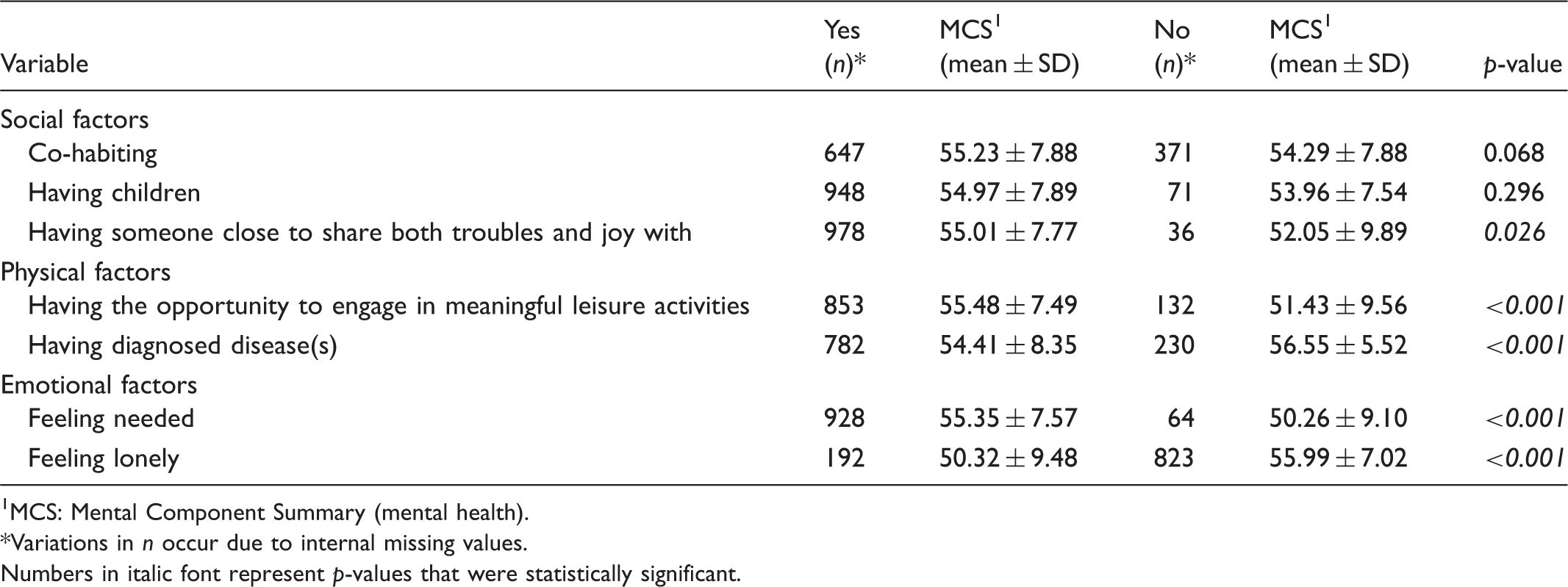
1 MCS: Mental Component Summary (mental health).
Variations in n occur due to internal missing values.
Numbers in italic font represent p-values that were statistically significant.
Multiple regression models of variables with a unique contribution to the PCS and the MCS scores.
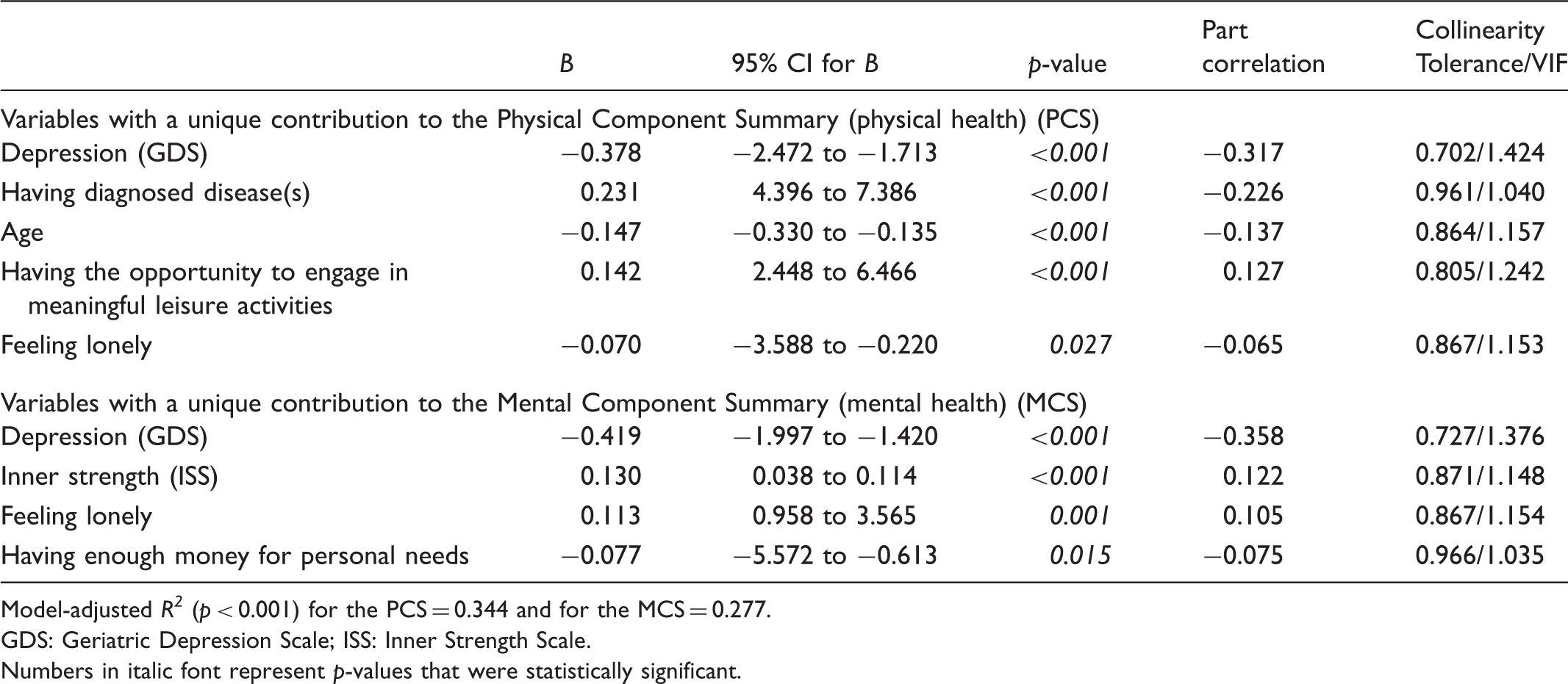
Model-adjusted R2 (p < 0.001) for the PCS = 0.344 and for the MCS = 0.277.
GDS: Geriatric Depression Scale; ISS: Inner Strength Scale.
Numbers in italic font represent p-values that were statistically significant.
The absence of depression, the absence of diagnosed disease(s), having the opportunity to engage in meaningful leisure activities and never or seldom feeling lonely, including socioeconomic controls, accounted for 34.4% of the variance in the PCS score (p < 0.001). Absence of depression, strong inner strength, never or seldom feeling lonely, including socioeconomic controls, accounted for 27.6% the variance in the MCS score (p < 0.001).
Discussion
The results show that depression was the strongest explanatory variable associated with HRQoL and, together with loneliness, explained both poorer physical and mental health. It is well known that loneliness and depression are strongly associated,12,22,23 and that both depression and loneliness, in addition to poorer quality of life, lead to an increased need for social and health-care services.23,24 Furthermore, better physical health was – not unexpectedly – partly explained by lower age and absence of disease(s), but also by being able to engage in meaningful leisure activities. Participation in various social/leisure activities has previously been associated with health, longevity, and psychosocial wellbeing. 25 Motivation to participate in leisure activities may however be predicted by opportunities (perceptions concerning choices of leisure opportunities available), as well as constraints 26 such as economic factors, impaired physical health, pain and depressive symptoms.25,27,28 Furthermore, better mental health was explained by strong inner strength and having enough money for personal needs (in addition to absence of depression and not feeling lonely). It has been shown that inner strength can mediate the relationship between self-rated health and disease, 29 including depression.29,30
Lastly, our results show that the older women on Åland rated their HRQoL as relatively high for both physical and mental health compared to other studies on older women in Scandinavia,31,32 as well as on the older population in general.33–35 The youngest age group (65–69 years) reported both better physical and mental health than all the other age groups, while the oldest (80+ years) reported the poorest physical and mental health. With this in mind, and even though older persons are a very heterogeneous group, it is important for health-care personnel to pay special attention to the oldest old (80+ years) with regard to HRQoL.
Implications for nursing
According to the ethical code for nurses, we have a fundamental responsibility to promote health, prevent illness and restore health. 1 Combining knowledge from the field of nursing with knowledge from the field of medicine and public health provides the basis for health-promoting practice. 2 Our results indicate the areas (all in the field of nursing practice expertise) in which health-promoting activities can be addressed in order to promote HRQoL among community-dwelling older women. In line with the results, a first step in the nursing process would be to assess whether there is a risk of loneliness and depression, or whether these are established. It is important to realise that loneliness is not the same as being alone. Loneliness manifests itself through subjective expressions 23 and therefore questions such as ‘Do you feel lonely?’, ‘How does loneliness affect your life?’ are appropriate ways in which to initiate a dialogue. When it comes to identifying depression, Ayalon, Goldfracht and Bech 36 suggest that one single question such as ‘Do you think you suffer from depression?’ can be used. Another option is to using screening tools to initiate a necessary discussion with the older person. GDS-15 is recommend for use in screening for depression as it is a validated tool, 19 easy to use (only yes and no answers), and is also suitable for use with the oldest old and with persons with mild cognitive impairment. 37 Nurses consequently need competences in person-oriented communicative skills, initiating dialogue and participation, as well as competence in clinical assessment of the patient by means of applying screening tools. Preliminary identification of diseases/symptoms still needs to be followed up by a more elaborate diagnostic procedure, 36 and the importance of collaborative care in facilitating a good interface when caring for older persons cannot be overestimated. Assessing needs and risks is in any case not enough; nurses also have to take account of the older person’s resources. 38 According to the results of this study, engaging in meaningful leisure activities and possessing inner strength could be such resources, since they are associated with better HRQoL.
The next step is to set up goals, and to plan for and implement interventions related to the older person’s needs, risks and resources in cooperation with a multi-professional team. It would appear that depressive disorders can be delayed or prevented 39 and successfully treated once identified, 39 and even small decreases in depression are related to a likelihood of improvement in self-rated health. 40 If nurses can bolster older people’s personal resources and environmental support by providing them with health-promoting activities, this can potentially result in better mental health functioning, a reduction in depression and enhanced perceptions of social support. 41 It has also been suggested that increasing inner strength in older people affected by disease could represent an intervention for enhancing experiences of health despite disease. 29 According to our results, another effective intervention for promoting HRQoL is encouraging involvement in meaningful leisure activities. Active ageing is advocated for enhancing quality of life as people age. 9 In order for nurses to be able to motivate involvement in leisure activities, as well as active participation in interventions related to depression and/or loneliness, a knowledge of cognitive or behavioural interventions or similar methods is emphasised.42,43 Nurse education must enhance education within this field in order to enable nurses to promote health in the future. Finally, continuous evaluation and documentation is essential in order to be able to ensure that the interventions have proved effective, and new goals must be set and reached.
Methodological considerations
There are a number of methodological considerations to be addressed in this study. The SF-12 Health Survey has been tested among older women, and its use in large community-based studies of older people is well supported. 44 However, our results might have been affected by the response rate. In total, 57% returned their questionnaire, which is in line with response rates for postal surveys in medical journals. 45 Nonetheless, there were many internal dropouts, and the results could have been affected by the lower response rate from older participants. The surveyed women mainly represented the third age (i.e. the young old); 11 the results therefore cannot necessarily be said to be representative of the fourth age, which is the one that suffers the most from comorbidity, declining cognitive status, depression and difficulties in activities of daily living. 46 Although this study was conducted within a limited island area, the results can be generalised to other older people (both men and women) living in sparsely-populated areas in Scandinavia. The cross-sectional design, which does not allow inferences in respect of cause and effect, can also be seen as a limitation. A longitudinal design would have provided opportunities for deeper analysis of these relationships.
Conclusion
Older women on Åland rated their HRQoL as relatively good. From a health-promoting perspective, our results show that special attention should be paid to community-dwelling older women aged 80+ years as they report the poorest HRQoL in terms of both mental and physical health. Our results also indicate that it is relevant to encourage older women to engage in meaningful leisure activities and to pay attention to individual health resources in order to support the elderly in overcoming adversities and ill health associated with ageing. In particular, our results suggest that nurses should identify older persons expressing loneliness and/or depressive symptoms. Changing the discourse of clinical practice and emphasising the promotion of health as an integrated part of practice rather than an occasional commitment can have an impact in terms of enhancing overall HRQoL among older women.
Footnotes
Funding
The authors are grateful to the King Gustaf V and Queen Victoria Foundation, the Åland Self-Autonomy’s Board 75th Anniversary Fund, the Åland Cultural Foundation for Medical Research and the Åland Society of Nursing for providing economic support for this study.
Conflict of interest
The authors declare that there is no conflict of interest.