
Abstract
Background:
Type 1 diabetes management for young children requires caregiver involvement to prevent serious health complications. Objectives: Explore the lived experience of rural caregivers’ health management routines and perceptions of an occupation-based coaching (OBC) intervention.
Methodology:
Following a 12-week, OBC telehealth intervention designed to promote diabetes management and caregiver psychosocial well-being, researchers interviewed eight rural caregivers to explore their perceived quality of life utilizing a phenomenological approach.
Findings:
Three themes emerged related to caregivers’ OBC intervention needs: occupational deprivation and decreased well-being; longing for connection with social supports; and desire for knowledgeable, relatable, and accessible providers. Two themes emerged related to their experiences postintervention: satisfaction with diabetes management and psychosocial support and renewed hope for childhood normalcy.
Conclusion:
Despite drastic shift in family routines after a child’s T1D diagnosis, caregivers reported acceptability of OBC for improving health management routines in a rural community following OBC intervention.
Plain Language Summary
Families living in rural communities report many barriers to managing their child’s type 1 diabetes cares. Occupation-based coaching is an emerging occupational therapy intervention that can be delivered over telehealth. Families who participated in a 12-week clinical trial then completed an interview to discuss their experiences of raising a child with type 1 diabetes in a rural community and what areas they would like included in an occupational therapy intervention. The caregivers also discussed how the intervention improved their overall health and well-being.
Type 1 diabetes (T1D) is a chronic condition that affects one in every 400 youth, with rates expecting to increase by 65% from 2017 to 2060 (Centers for Disease Control and Prevention [CDC], 2020; Tönnies et al., 2023). T1D management includes the management of insulin levels, self-care skills, adjustments to daily living routines, glycemic vulnerabilities, diabetic ketoacidosis, nutrition monitoring, and developmental and psychological changes which all require consistent caregiver involvement (ElSayed et al., 2023). Consequently, the health management plan of a child with T1D requires periodic reassessment to ensure that the plan aligns with the roles and routines of the family and primary caregiver. Due to the intricate nature of T1D, it is important to consider the child’s caregivers and the challenges regarding its management that may require support and services.
Due to the complexity of the child’s health management routine, it is common for caregivers to experience stress and occupational deprivation (Gallegos et al., 2023; Wozniak et al., 2023). A caregiver’s psychosocial well-being has a strong impact on their ability to perform health management tasks. Evidence suggests that caregivers experience increased symptoms of stress, anxiety, and depression (Gallegos et al., 2023; Wozniak et al., 2023). Specifically, Wozniak and colleagues (2023) found that 31.4% of caregivers of children with T1D reported moderate caregiver burden and 8.6% of caregivers reported severe to very severe burden. However, when looking at caregiver burden for mothers of younger children was higher, they reported moderate or severe to very severe burden (71.4% for ages 0–4 years; 85.7% for ages 5 to 9 years; Gallegos et al., 2023). This is an alarming trend, because T1D management requires long-term proactivity and vigilance from the caregiver until the child reaches an age to independently manage their diabetes cares.
Caregivers’ access to quality disease education and medical intervention are necessary components of the health management routine. People with chronic conditions living in rural and medically underserved communities experience additional health disparities related to access and quality of care (CDC, 2020; Jewell et al., 2023). Children with T1D living in rural areas are no exception; they have significantly lower rates of appointment adherence, higher glucose levels, and decreased patient-provider communication compared with those living in urban areas (Gill et al., 2022; LePage et al., 2021; Stumetz et al., 2016). These disparities call for a more accessible model of care. To address health disparities in children with T1D living in rural communities, occupational therapy practitioners can utilize innovative methods of service delivery such as telehealth. Telehealth is a delivery model that has potential to overcome access barriers and provide patients living in rural communities with quality health care services (Feldhacker et al., 2022).
Occupation-based coaching (OBC) is a collaborative, family-centered occupational therapy intervention where the practitioner collaborates with the caregiver to achieve self-identified goals through reflective questioning, which can be delivered via telehealth (Little et al., 2018; Smith et al., 2023). Jewell and colleagues (2025) conducted a pilot randomized controlled trial to examine if OBC telehealth intervention improved child health outcomes, parental self-efficacy, and family quality of life and participation. While preliminary findings suggested improvements in family-centered participation goals for the intervention group over the control group (n = 16, p < .05) and for self-efficacy (p < .05), it is not known what the lived experience was of the families who participated in the study. Therefore, the purpose of this study was to explore the rural caregivers’ perceptions of the content and receipt of the telehealth OBC intervention. Furthermore, gaining an intimate exploration of caregivers’ of children with T1D lived experiences can help shape intervention approaches in this emerging area of practice. The research questions were: How do the lived experiences of rural caregivers of children living with T1D shape the need for OBC telehealth intervention? How do rural-dwelling caregivers of children living with T1D perceive the acceptability of telehealth OBC to address their family and child’s health management needs?
Methods
Research Design
This qualitative study utilized a phenomenological approach to provide an intimate insight into the lived experiences of caregivers of children with T1D living in rural communities following participation in a 12-week OBC telehealth intervention. In-depth interviews allowed researchers to gain an extensive understanding of caregivers’ DM needs and OBC intervention acceptability. The Creighton University Institutional Review Board approved this study, the original clinical trial was registered at ClinicalTrials.gov (NCT04753099), and all caregivers provided informed consent for the interviews.
Informants
Researchers utilized criterion sampling to recruit from a list of 10 families who previously participated in 12 weeks of telehealth OBC intervention. Eight caregivers consented and participated in the study and met the following inclusion criteria: resided in Colorado, Nebraska, Iowa, or Minnesota, lived in a rural community defined as a minimum of a 1-hour commute from a pediatric endocrinologist office (LePage et al., 2021), had internet access, were 19 years of age or older, and were the primary caregiver of a child aged 2 to 12 years diagnosed with T1D.
Instruments
The interdisciplinary, community-engaged research team developed a semi-structured questionnaire. The initial questionnaire was informed by a literature review and diabetes health care provider and patient and caregiver input, resulting in 12 open-ended questions and additional probing questions to facilitate continued discussion and to clarify the caregiver’s responses. An expert panel of qualitative researchers then reviewed the questionnaire for content validity (n = 3). The questionnaire included additional questions to gather demographic information. As community partners were involved in the development and review of the questionnaire, no formal pilot testing was completed.
Procedures
Utilizing the participant database from the randomized controlled trial, the researchers emailed an information letter to all potential informants. After interested caregivers gave verbal consent, individual interviews were scheduled. Researchers, both trained female doctoral students, not affiliated with the clinical trial (names blinded for review) completed 30- to 60-minute interviews using the semi-structured questionnaire. The interviewers did not have a personal connection to T1D. Interviews were recorded digitally on Zoom Platform (Zoom Video Communications Inc., 2016). Caregivers completed the interviews from their homes. Interview recordings were transcribed verbatim and manually coded.
Data Analysis
Moustakas’ (1994) seven steps of phenomenological data analysis guided the data analysis process. The second and third authors completed analysis Steps 1 to 6, and they were not affiliated with the previous clinical trial. From the transcribed data, the second and third authors coded the relevant expressions and extracted and listed them in a table using horizontalization, (Step 1). Specifically, we highlighted and then combined significant caregiver statements. All researchers completed bracketing throughout all stages of analysis to reduce bias due to the use of community-engaged research methods. Second, researchers determined invariant constituents by reviewing extracted horizons for overlapping, repetitive, and vague expressions (Step 2). In the third step, invariant constituents, or the repetitive statements, were clustered to produce five preliminary themes which were then organized in a table (Step 3). Next, invariant constituents and preliminary themes were validated through collaboration of five independent researchers (two trained doctoral students, one health care provider, and two experienced researchers, one with a dual role as caregiver). Validation required researchers to check for compatibility between horizons, core themes, and original caregiver data (Step 4). Two researchers constructed individual textual descriptions of the caregivers. Individual textual descriptions combine verbatim interview quotes and researcher observations to construct a narrative of the caregivers’ experiences (Step 5). The next step involved constructing individual structural descriptions with the use of individual textual description and imaginative variation (Step 6). Imaginative variation allowed researchers to view the phenomenon through additional perspectives by analyzing perception structures. The first through fifth authors completed the final step, which involved the review and consolidation of individual textural and structural descriptions to produce a composite textural-structural description (Step 7). The composite description organized invariant constituents and core themes to represent the collective experiences of the caregivers (Moustakas, 1994). This allowed researchers to gain an understanding of the collective perceptions involved in the investigated phenomenon, resulting in five final themes.
Trustworthiness
To establish trustworthiness, the researchers employed reflexivity, member-checking, collaboration between the researcher and the caregivers, a thick description of the research process, and validation (Curtin & Fossey, 2007). Researcher reflexivity occurred by electronically documenting and in-depth team discussions throughout the data analysis process. Caregivers reviewed transcribed interviews and final themes as a form of member-checking, with no modifications. The researchers provided a thick description of the research process by providing a detailed description of the contexts that surround the investigated phenomenon through keeping detailed meeting minutes and an audit trail. To increase dependability, the researchers worked independently to code and theme transcribed interviews. Researchers collaborated to discuss findings, code caregiver responses, and arrive at the conclusion of final themes. Similar to Marshall and Long (2010), we did not seek to reach saturation, as we intended to highlight the individual meaning ascribed by each caregiver (Saunders et al., 2018). Validation occurred using a certified diabetes educator and care specialist and two qualitative expert researchers.
Results
Eight of the 10 caregivers who were asked to participate in the interviews completed semi-structured interviews following participation in an OBC telehealth intervention. Two caregivers declined participation due to time commitment. Eight caregivers were from seven rural-dwelling families, including seven females and one male. These interviews explored caregivers’ lived experiences of telehealth intervention and the meaning they give to occupational engagement and quality of life while managing their child’s diabetes. Caregivers’ ages ranged from 34 to 50 years with an average age of 40.8 years; seven were married. Two caregivers held an associate degree, two caregivers held a bachelor’s degree, and four caregivers held a master’s degree. Seven caregivers identified as White and one identified as Mixed (i.e., White, African American, and Hispanic). The children’s ages at the time of T1D diagnosis ranged from 12 months to 9 years and time since diagnosis ranged from 11 months to 8.5 years. The families lived an average of 202 miles from the nearest pediatric endocrinologist clinic. One caregiver reported living with three people, three caregivers reported living with four people, and one caregiver reported living with five people in the same household. See Table 1 for details.
Informant Demographic Data.
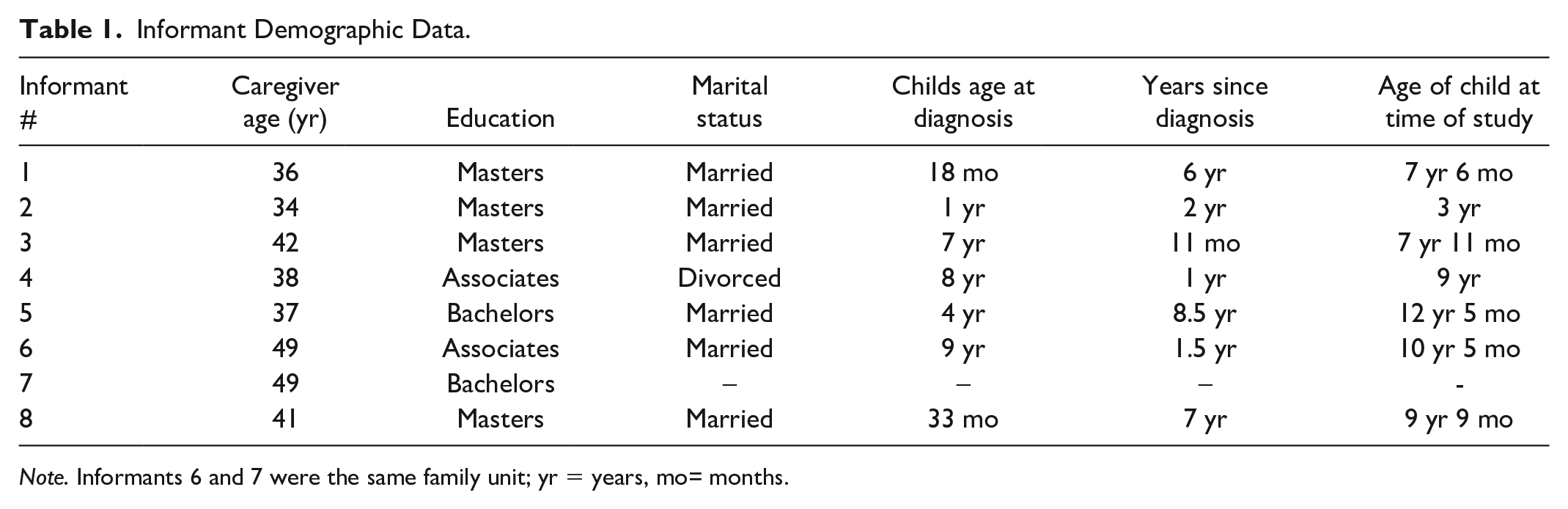
Note. Informants 6 and 7 were the same family unit; yr = years, mo= months.
Caregivers reported the challenges they experienced to remain engaged in valued occupations while caring for a child with T1D. These challenges may be due to the occupational imbalance where childrearing and health management of children take priority over caregiver’s other occupations. Caregivers described how they were required to balance engagement in valued occupations while managing T1D. This balancing act created occupational disruptions, especially in sleep, social participation, and leisure. Three distinct themes emerged related to caregivers’ experiences after their child’s diagnosis that they would have liked support from health care providers: occupational deprivation and decreased well-being; longing for connection with social support; and a desire for knowledgeable, relatable, and accessible providers. Two themes emerged related to their experiences after receipt of the telehealth OBC intervention: satisfaction with diabetes management and psychosocial support from the intervention and a renewed hope for childhood normalcy. There were no diverse cases or minor themes. Overall, the caregivers reported satisfaction with OBC as it provided validation of their lived experience of raising a child with diabetes in a rural community and the family-centered nature of the intervention. The caregivers also reported a sense of hope that their children can successfully participate in important everyday activities.
Themes Related to Caregivers’ Reported Needs to Address Through OBC
Theme 1: Occupation Deprivation and Decreased Well-Being After Diagnosis
Caregivers described occupational disturbances from caregiving for a child with T1D. Caregivers and their children with T1D may experience drastic changes in their roles and routines after diagnosis. Overwhelmingly, the areas of social participation and sleep were discussed as most impacted. All caregivers described similar experiences detailing how the complexity and knowledge of managing T1D prevented them from leaving their child under another person’s care. A caregiver described how the complexity of care impacted their social engagement for an extended period following when their child received their T1D diagnosis: “After she got diagnosis, I just, it was more than a year that I didn’t take her to . . . anything where she was watched by someone else” (I2).
Caregivers described how their social participation was impacted by their increased family health management routines. A caregiver provided insight into the severity of this disturbance stating, “I think I just stopped, like I stopped doing virtually anything” (I2). Other reported feeling forced to discontinue valued occupations to provide care for their child with T1D. A caregiver described the experience of attempting to balance the occupations of social participation and sleep: I would not go to activities or sometimes I would not go places if we were having a tough day keeping in range and I was like, we are not going to go there . . . they are going to have this type of food there, and we have already struggled for whatever reason today . . . we probably won’t be able to [manage well and] I will be up even more than I already been up . . . the change in sleep was such a huge problem for me. (I8)
Sleep was the occupation that caregivers consistently experienced disturbance within their routines. Many caregivers described the lack of sleep nightly, due to the constant worry for their child with T1D coupled with the constant demands of monitoring their child’s health, stating “I do not get sleep, I do not get, um, eight hours of sleep at night. Usually, average four to five hours but not consistent” (I1). Another caregiver described, “Before [receiving technology] I didn’t sleep more than like two or three hours at a time” (I8). Another caregiver provided insight that suggests the impact that lack of sleep has on the caregiver’s ability to perform their daily activities and said, “My ability to get sleep affects my ability to control my stress level and my ability to handle life” (I3). The occupational deprivations these caregivers experienced in their daily lives may lead caregivers to long for more connection to have support as a caregiver of a child with T1D.
Theme 2: Longing for Connection With Social Supports
Caregivers of a child with T1D expressed a desire for social support and connection from people who share similar experiences with T1D. One caregiver explained, “. . . folks like us that live in rural communities . . . do not have the same support system” (I1). Many caregivers explained how living in a rural community places additional limitations on the availability of social support. The caregivers expressed how difficult it is to express personal difficulties as caregivers of a child with T1D, stating: And so, I cannot explain this to anyone else and I do not want them to have to go through it, just to understand it. But if you can find someone who has lived that and can share that that is helpful, that is wonderful. (I3)
Many caregivers expressed concerns regarding the coordination of care for their child with T1D. One caregiver stated, “It is not like I can just call anybody up . . . hey, can you help me, can you watch my kiddo at last minute, you know I have to plan ahead” (I1). She further described how living in a rural community limits access to others who could assist with her child’s diabetes management. Another caregiver expressed similar concerns by stating, “I’ve been called a helicopter parent because I won’t let him out of my sight, or I am very limited on who I let watch her and seen as controlling” (I8). These desires to establish connections through shared experiences to support social relationships were essential to their quality of life. The desire for an increased personal connection extended to care providers as well.
Theme 3: Desire for Knowledgeable, Relatable, and Accessible Providers
Caregivers reported frustrations regarding the limited knowledge exhibited by health care providers regarding pediatric T1D treatment. The lack of awareness of health care providers was echoed across access and emergency services available within rural settings. One caregiver expressed, “It’s definitely not the PCP’s [primary care provider’s] fault here in the area, we in a rural, but they’re not familiar with diabetes either” (I1). Another caregiver shared a similar experience stating, “The nurses there do not what to care for a child with type I” (I10).
Frustration was expressed due to the understanding caregivers felt was lacking from the patient-provider relationship. “You can know textbook diabetes, but that doesn’t equip you to be able to take care of one participant or person” (I4) was a common statement expressed by caregivers in the study. The same caregiver discussed the value of feeling heard, making connections, and having the ability to communicate with their child’s health care team. “If this study has taught me anything it’s how important all those other side pieces are to being able to do this because of those little side pieces, those side supports aren’t in place, the whole building’s going to fall over” (I4). She further elaborated on the importance of having a relationship with members of their child’s health care team, “and I’m intrigued by how much more empowered I could become by having, you know, a relationship with a pediatric endocrinologist” (I4).
Caregivers expressed frustration due to insurance dictating when emergency care is necessary as well as caregiver need of fighting for coverage of the materials and supplies needed to care for their child. “The frustration and the stress of trying to get everything covered and not drain the bank so that she can have the supplies that make handling the disease easier . . . it’s very frustrating for me” (I4).
Themes Related to Caregivers’ Receipt and Perceptions of OBC After Intervention
Theme 4: Satisfaction With Diabetes Management and Psychosocial Support
Participation in OBC sessions empowered caregivers to take a proactive health management T1D approach. Caregivers discussed appreciation for having regular check-in meetings to hold them accountable to progress toward goals established to improve their child’s health management. A caregiver shared, “They [occupational therapy interventionists] held you accountable, you know actions instead of procrastination. So, that was really good” (I6/7). Accountability was perceived as a benefit alongside proactive management of their child’s T1D: I guess more proactive too instead of reactive we were able to set goals going forward . . . I think the best thing about this experience was having check ins and keeping both myself accountable, ahead of time rather than just adjusting after the fact . . . being a tad more proactive is very helpful. (I5)
OBC interventionists are trained to provide guided discovery and joint planning within intervention, allowing caregivers to feel supported while also providing autonomy within the care of their child (Dunn et al., 2018). For example, one caregiver shared, “It was just good to have someone else . . . not call out different patterns because [they see them] . . . but just saying like Hey, and what could you do different?” (I5).
Following the OBC intervention, caregivers expressed a change in response to diabetes management to include proactive measures, “You cannot control it, but I am going to be more proactive instead of responsive diabetes management is the responsibility of helping your diabetic child, whether it’s a child or whoever live their best life” (I3). Results suggest addressing the caregiver from a psychosocial perspective may improve overall well-being for caregiver and child, leading to balance. Balance was discussed within the context of benefits of OBC intervention, there was a commonality among caregivers for seeking out and finding that balance within daily life in relation to their own health as well as their child’s health. “Life is finding that balance, finding that balance” (I1). Following the OBC intervention caregivers reported an improved understanding of holistic care for themselves, “[I have gained] a better understanding of overall health and how that will help. . .both mental health and physical health life and managing diabetes care” (I8).
Comfortability and positive interactions with OBC providers were viewed to have a potential positive impact on caregiver’s psychosocial well-being. Caregivers shared the benefit of relationships and rapport within the OBC interactions by stating, “This study helped because it treated me as a person. . .I feel like I’m in therapy right now” (I3). Caregivers found benefit in the reflective nature of the OBC intervention. For example, one caregiver stated, I just like having someone to talk to that understood and yeah . . . I could vent some frustrations of the disease . . . I felt like there was a safe place to like vent that frustrations of the disease and you cannot do that with your other diabetic team. (I2)
Caregivers reported that the ability to confidently manage their child’s T1D through a proactive approach allowed them to attend to their own psychosocial needs as a caregiver. One caregiver shared, “It was nice to also have that connection and know that you are being heard and somebody cares” (I1). Caregivers reported that attending to their own psychosocial needs facilitated improved family quality of life, allowing improved participation in valued occupations. For example, caregivers expressed an improvement with their quality of life when they were able to observe their efforts making a positive change with their child’s diabetes management. One caregiver stated, “That gives me more energy to try to make her numbers good too. Cause I know she will be feeling . . . good and be happy” (I2). When caregivers felt like they provided best care, it allowed them to address their own needs as the caregiver, “We were doing the intervention and everything . . . when your life doesn’t revolve around diabetes, you’re able to step back and include that [time for] . . . things you [as a caregiver] needs” (I8). “We have lived and breathed this for so long that we’re just . . . in routine . . . we know what works best and what doesn’t” (I1). Caregivers expressed that managing T1D over time becomes integrated into a normal way of life thus becoming a “new normal.”
Theme 5: Renewed Hope for Childhood Normalcy
Caregivers expressed a renewed hope for childhood normalcy. Establishing a sense of normalcy resulted in less interruption of engagement in desired activities and potentially improved enjoyment of life. Caregivers worked to achieve this sense of normal so that their children too can live life fully and “normally”: Our daughter has always been able to enjoy the activities she does . . . she just does something that she wanted to do; we are going to do it . . . night-time blood sugars were not exactly, but she was able to enjoy that just as any other girl her age totally would. (I5)
A caregiver shared about her child participating in the telehealth intervention, “It was good to see her engaged and part of it . . . and it was nice because we came up with goals and plans and crushed them all” (I4). When caregivers and children can be confident with diabetes management they reported more acceptance of the disease and achieving a new normal. One caregiver said that “Becoming an astronaut at NASA is the only job that is off the table, but I think otherwise the sky is the limit” (I3).
Discussion
The caregivers shared intimate accounts of their lived experiences regarding the navigation of their complex T1D health management routine, providing details on gaps in health care and how OBC filled these family health management needs. The findings included three themes related to what occupational therapy practitioners should address in an OBC intervention: the caregivers’ occupational deprivation and psychosocial well-being, the longing for social support, and the desire for proficient health care providers; and two themes related to the caregivers’ views after receipt of OBC: satisfaction with diabetes management, and renewed hope for normalcy in their child’s life.
Caregivers’ Experience After Child Receiving T1D Diagnosis and Areas for Occupational Therapy
The caregivers’ role in their child’s T1D health management routine created challenges in their ability to engage in salient occupations and experience overall health and well-being. These drastic disturbances in day-to-day roles and routines were due to the occupational imbalance where childrearing and health management of child take priority over the caregiver’s ability to engage in other valued occupations. It was not surprising that caregivers reported challenges with caring for a child with a chronic condition and the subsequent declined participation in their personal leisure activities (Piran et al., 2017). It also was not a surprise that rural caregivers in this study reported increased stress and occupational deprivation as prior studies found similar findings (Jewell et al., 2023; Wozniak et al., 2023). However, caregivers were able to adapt as their child’s health management routine became the new normal. This suggests that the caregiver self-efficacy improved over time, which was in alignment with the quantitative findings of this clinical trial (Jewell et al., 2025) and other caregiver-focused, health promotion coaching studies (e.g., Bourke-Taylor et al., 2023; Little et al., 2018; Smith et al., 2023).
The caregivers expressed a longing for connection and social support in their personal lives and challenges of accessing social support in rural communities. Caregivers reported using extra caution when selecting a care provider for their child due to others’ decreased knowledge about T1D management. Caregivers shared that this desire for connection extended to the trust they had with health care providers to provide adequate care for their child. An expected finding from this study showed the lack of emotional support that caregivers felt from traditional health care providers upon initially receiving the diagnosis for their child. These results are consistent with the findings of a scoping review that detailed the lack of support caregivers received from family physicians while caring for a family member during their course of treatment (Parmar et al., 2020). Caregivers expressed trust they had in their child’s health care providers was dependent on positive versus negative provider interactions. The difference between those experiences includes how much knowledge the provider had about T1D.
Caregivers’ experiences after diagnosis within rural communities included a desire for social support. Lack of access may have been projected to the medical providers that families initially interacted with. This study suggests that caregivers received the psychosocial support they needed from occupational therapy practitioners during OBC sessions to improve their psychosocial well-being.
Caregivers’ Experiences Following Telehealth Coaching
OBC empowered caregivers to take a proactive approach regarding their child’s diabetes management. This holistic intervention supported caregivers’ comfortability with the provider. Findings from this study suggest that the psychosocial support the caregivers received during OBC sessions improved the caregivers’ overall quality of life. Implementation of the OBC model allowed for a diverse approach of emotional support and information exchange within a structured process to allow for successful intervention (Graham et al., 2010). This exchange of information led caregivers to share a hope for returning to normalcy post diagnosis. This was an expected finding as both Smith and colleagues found similar support for their telehealth coaching intervention (Smith et al., 2023).
Caregivers expressed their desire for their child with T1D to participate in occupations like their peers. Caregivers reported success with the management of their child’s T1D as OBC empowered them to take a proactive approach regarding their child’s medical management routine. Caregivers perceived an ability to achieve a new normal within the day-to-day management of T1D allowing for less occupational disruption and balance in occupational participation for themselves and their child. This was not surprising as Harris and colleagues (2022) found that mothers raising a child with a chronic condition improved their overall participation in health-promoting activities and leisure participation after participating in a 6-session occupational therapy coaching intervention. Furthermore, the mothers reported improved psychosocial well-being, specifically with improved energy levels and mood, less stress and anxiety, and increased self-awareness (Harris et al., 2022).
Study limitations include limited transferability due to the small sample with seven of 10 families (eight caregivers) participating in the interviews. The families in the clinical trial and those who participated in the interviews were a homogeneous sample, with all children using similar diabetes technologies (e.g., continuous glucose monitor, insulin pump), receiving usual care for endocrinology services (e.g., 3-month visits with their pediatric endocrinologist or pediatrician), and similar demographics (see Table 1). The study was at risk for the social and courtesy desirability bias. We attempted to mitigate this risk by using a trained interviewer who was not affiliated with the clinical trial. Furthermore, it is possible that the results were more favorable as the interviews occurred during the pandemic and the families may have felt more isolated than usual causing them to seek social support from the interventionists. Future research should include additional family members beyond the primary caregivers to offer a more diverse perspective of OBC intervention. Additional studies could explore the child’s perception of OBC intervention and their lived experience after diagnosis. Future research may also explore the use of OBC with a variety of chronic conditions and caregiver perspectives. Finally, future research should include follow-up interviews that focus on the feasibility of OBC (e.g., duration, frequency, intensity) and include additional probing questions to illicit more in-depth responses on the occupation-focused nature of the intervention.
Conclusion
Occupational therapy practitioners can assist caregivers with health management tasks including symptom and condition management, communication with health care providers, medication management, physical activity, nutrition management, personal care device management, social and emotional health promotion, and maintenance (American Occupational Therapy Association, 2020). OBC allows practitioners to collaborate with families addressing habits, routines, and roles that could provide a positive impact on the caregivers’ quality of life. Occupational therapy practitioners are skilled at collaborating with families to identify strengths and limitations that may limit or promote their participation in everyday activities. This research may be informative for occupational therapy practitioners and other medical providers to understand caregivers experience and perspectives when working with T1D clients in rural communities.
Footnotes
Author Disclosures
This manuscript was written in partial fulfillment of the second and third authors’ postprofessional Occupational Therapy Doctorate degree at Creighton University. The study findings were previously presented at the American Diabetes Association Scientific Sessions, American Occupational Therapy Association Annual Conference, and the Nebraska Occupational Therapy Association Annual Conference.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Creighton University Health Science Strategic Faculty Investment Fund.
Research Ethics and Patient Consent
Researchers obtained approval to conduct this study from Creighton University Institutional Review Board (IRB #2002161-01). This study was approved by Creighton University’s Institutional Review Board for the Protection of Human Subjects in Research, IRB #2000257, in accordance with the standards outlined in the 2000 Helsinki Declaration. All participants were provided written and verbal information of the study’s risks and benefits, that their participation was voluntary, and that their identity would not be disclosed. All participants provided informed consent.