
Abstract
Objective
Peripheral artery disease affects approximately 250 million people globally. Multiple randomised controlled trials have compared bypass and endovascular interventions but the optimum revascularisation approach remains unclear. The recently published BEST-CLI and BASIL-2 trials provide current and robust data addressing this question, however their findings are not concordant. This systematic review and meta-analysis provides an overview of the worldwide randomised evidence comparing bypass surgery and endovascular revascularisation in lower limb peripheral artery disease.
Methods
A comprehensive literature search of MEDLINE, Embase and CENTRAL databases was performed of all time periods up to 7 May 2023 to identify randomised controlled trials comparing bypass and endovascular revascularisation for treating lower limb peripheral artery disease. The primary outcome was major amputation. Secondary outcomes were mortality, re-intervention, 30-day adverse events and 30-day mortality. Odds ratios were calculated and pooled using the random-effects model. Risk of bias was assessed using the Cochrane risk of bias 2 tool.
Results
Fourteen cohorts were identified across thirteen studies, enrolling 3840 patients. There was no significant difference in major amputation (OR 1.12; 95% CI 0.80-1.57) or mortality (OR 0.96; 95% CI 0.79-1.17) between the bypass and endovascular groups. Bypass was associated with a significant reduction in re-intervention compared with endovascular treatment (OR 0.57, 95% CI 0.40-0.82).
Conclusions
These findings suggest that rates of major amputation and mortality are similar following bypass and endovascular interventions. Patients who undergo bypass surgery have a significantly lower re-intervention rate post-operatively.
Keywords
Introduction
Peripheral artery disease (PAD) affects approximately 250 million people globally. 1 Patients with PAD may have symptoms of intermittent claudication (IC) or chronic limb-threatening ischaemia (CLTI), presenting as ischaemic rest pain, lower limb ischaemic ulceration or gangrene. One-year mortality in patients with untreated CLTI is greater than 20%. 2 The management of PAD includes aggressive control of modifiable cardiovascular risk factors, treatment of infection and revascularisation to improve blood flow to the affected limb. Revascularisation carries risks of procedural morbidity and re-occlusion and is generally reserved for those with CLTI or lifestyle limiting IC that has failed non-operative management.1,3 Whether an open bypass surgery or endovascular therapy first approach is most appropriate for patients undergoing revascularisation has been unclear and identified as a research priority in the recent Global Vascular Guidelines on the Management of CLTI. 1
Several randomised trials have explored the optimal revascularisation approach without consensus and prior systematic reviews have noted the limited availability of high-quality data.4-6 Until recently, the Bypass vs Angioplasty in Severe Ischaemia of the Leg (BASIL) trial was the largest randomised controlled trial (RCT), 7 however the recent Best Endovascular vs Best Surgical Therapy in Patients with CLTI (BEST-CLI) 8 and Bypass vs Angioplasty in Severe Ischaemia of the Leg 2 (BASIL-2) 9 trials have provided large and up-to-date data. These trials are unique compared to previous literature due to their large size, recruitment specific to CLTI and a pragmatic design allowing inclusion of all modern endovascular techniques at clinicians’ discretion. Despite this, BEST-CLI and BASIL-2 used different primary outcomes with different observed results, which may relate to specific inclusion of patients with infrapopliteal disease in BASIL-2.8,9 Given the availability of these data, updated systematic review and meta-analysis of all randomised trials is warranted.
This systematic review aimed to combine studies comparing bypass surgery and endovascular revascularisation to determine which is superior in terms of major amputation, mortality and re-intervention for patients with lower limb PAD. It was hypothesised that bypass surgery was associated with a reduced rate of major amputation and re-intervention following revascularisation, at the expense of greater procedural mortality.
Methods
This review was performed in accordance with the Preferred Items for Systematic Reviews and Meta-Analyses (PRISMA) statement and Cochrane Handbook for Systematic Reviews of Interventions.10,11 The study was registered with the International Prospective Register of Systematic Reviews (PROSPERO; registration number CRD42023416609).
Eligibility Criteria
The population included any patients undergoing an infra-inguinal revascularisation procedure for PAD. This included patients with both IC and CLTI. Inclusion was limited to prospective RCTs comparing outcomes following revascularisation by endovascular techniques (including angioplasty, stenting or any other technique) and bypass surgery (using autologous or non-autologous conduit). Studies were excluded if they were non-comparative, retrospective, non-randomised or did not include results for at least major amputation, the primary outcome of interest.
Outcomes
The primary outcome was major amputation (proximal to the ankle) at any point during follow up. Secondary outcomes were mortality (at any point during follow up), re-intervention (at any point during follow up, where major and minor re-intervention were reported separately major re-intervention was used), pre- and post-operative ankle brachial index (ABI) (timing of ABI post-operatively varied between studies), 30-day mortality and 30-day adverse events (defined as a major adverse cardiovascular event or any other listed peri-operative complication, reported as number of patients suffering at least 1 major complication when available, or number of individual complications summed when complications reported separately).
Search Strategy
A comprehensive literature search was performed following librarian consultation in electronic databases MEDLINE, Embase and Cochrane Central Register of Controlled Trials. Reference lists of relevant literature and systematic reviews were also screened for eligible studies. All time periods and languages were included, up to 7 May 2023. Controlled vocabulary and keywords were used relating to PAD, bypass surgery, endovascular interventions and RCTs. Validated RCT filters were used for MEDLINE 11 and Embase 12 searches. The full search strategy is detailed in Supplemental Table 1. Duplicates were removed and 2 reviewers independently screened records for inclusion based on title and abstract. Relevant studies were screened in full for eligibility. Disagreements were resolved by consensus between the 2 extracting authors.
Data Extraction and Appraisal
Data extraction was performed independently by 2 authors (AP, SP) using a standardised form including study design, baseline characteristics, intervention details and outcome measures. Data was extracted from the results of published trials and pooled for statistical analysis. Included studies were appraised independently by both authors using the Cochrane risk of bias 2 (RoB 2) tool and classified into low, some concerns or high risk of bias. 11 Any discrepancies in data extraction or risk of bias assessments were resolved by consensus between the 2 extracting authors.
Statistical Analysis
Analyses were conducted on an intention-to-treat basis. Meta-analysis was conducted using a random-effects model considering expected heterogeneity between studies. The inverse variance method was employed to estimate the pooled effect size taking into account both within-study variance and between-study variance. This approach was followed due to variations in effect sizes across the included studies. Heterogeneity between studies was assessed to understand the extent of variability in effect sizes and interpreted as low (0%–49%), moderate (50%–74%) and high (75%–100%). Due to the relatively small number of eligible studies identified, we used the Sidik-Jonkman method to assess variance between studies (tau2). The results of the meta-analysis for both primary and secondary outcomes were presented as odds ratio (OR) and 95% confidence interval (CI). All analyses were performed using R software 4.2.3 using ‘meta’ and ‘dmetaR’ packages. Statistical significance was set at ≤0.05.
Results
The search strategy identified 865 reports, with 3 additional studies identified from manual searching of previous systematic reviews. Article screening is detailed in a PRISMA diagram in Figure 1. A total of 14 cohorts (including 2 from the same study
8
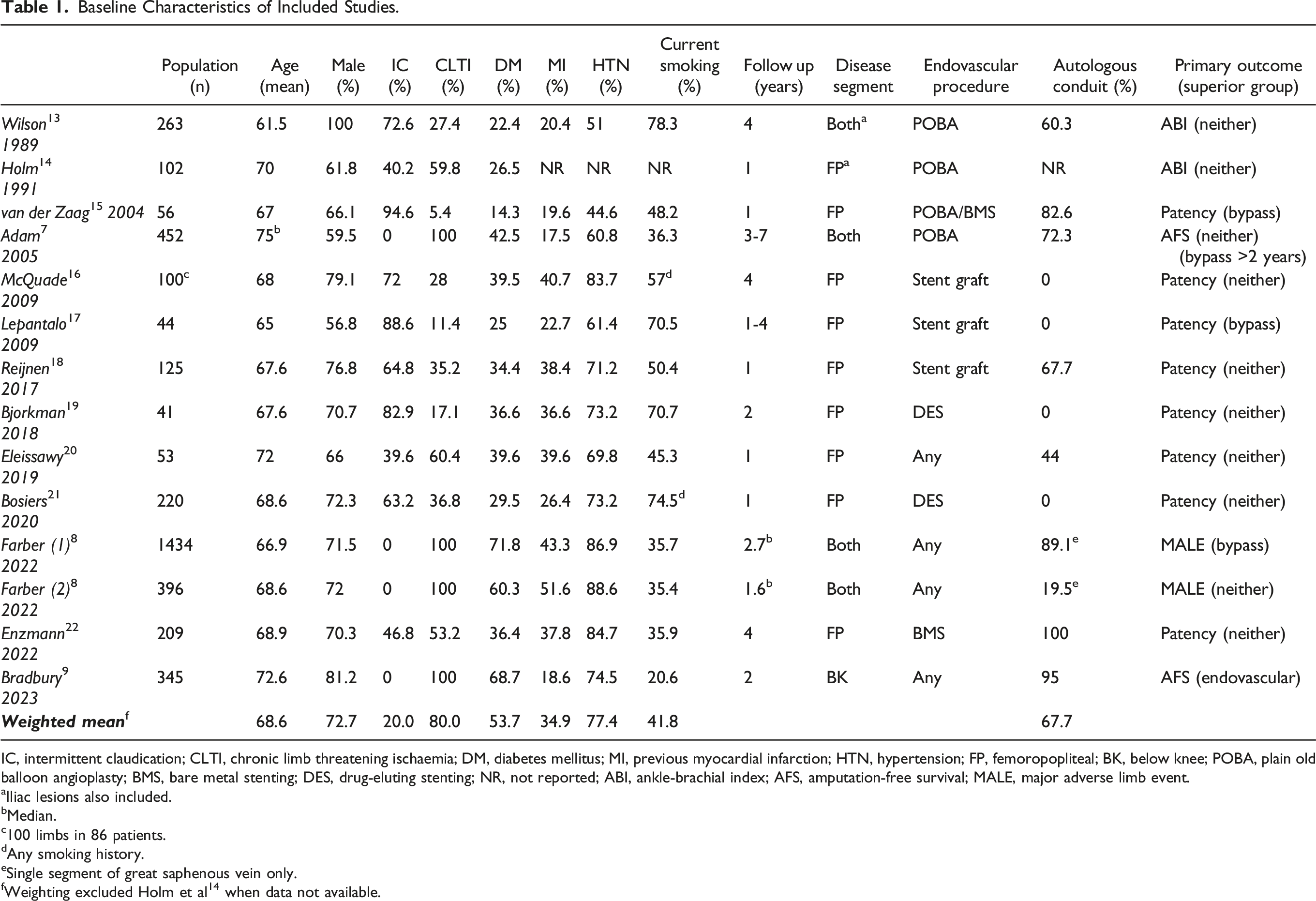
) were included with a final population of 3840. The baseline characteristics of included studies are listed in Table 1. Follow up ranged from 1 to 4 years, apart from the BASIL trial
7
which included follow up to 7 years for a small number of patients. The median follow up duration was 1.8 years. The majority of studies were published in the last 10 years, with 2 publications prior to 2000.13,14 The sample size of included studies was small, with BASIL,
7
BEST-CLI,
8
and BASIL-2
9
representing the largest trials encompassing 68.4% of the total study population. Whilst these 3 largest trials enrolled only participants with CLTI, most smaller trials also included patients with IC. The weighted mean proportion of patients with CLTI was 80.0%. The majority of studies included femoropopliteal disease only, with only 1 study specific to below the knee disease.
9
Most bypass surgeries were performed using an autologous conduit (weighted mean 67.7%), however 4 studies16,17,19,21 exclusively used non autologous conduits. A variety of endovascular procedures were performed, with the availability of more advanced techniques reflected in more recent trials. PRISMA diagram of included studies. Baseline Characteristics of Included Studies. IC, intermittent claudication; CLTI, chronic limb threatening ischaemia; DM, diabetes mellitus; MI, previous myocardial infarction; HTN, hypertension; FP, femoropopliteal; BK, below knee; POBA, plain old balloon angioplasty; BMS, bare metal stenting; DES, drug-eluting stenting; NR, not reported; ABI, ankle-brachial index; AFS, amputation-free survival; MALE, major adverse limb event. aIliac lesions also included. bMedian. c100 limbs in 86 patients. dAny smoking history. eSingle segment of great saphenous vein only. fWeighting excluded Holm et al
14
when data not available.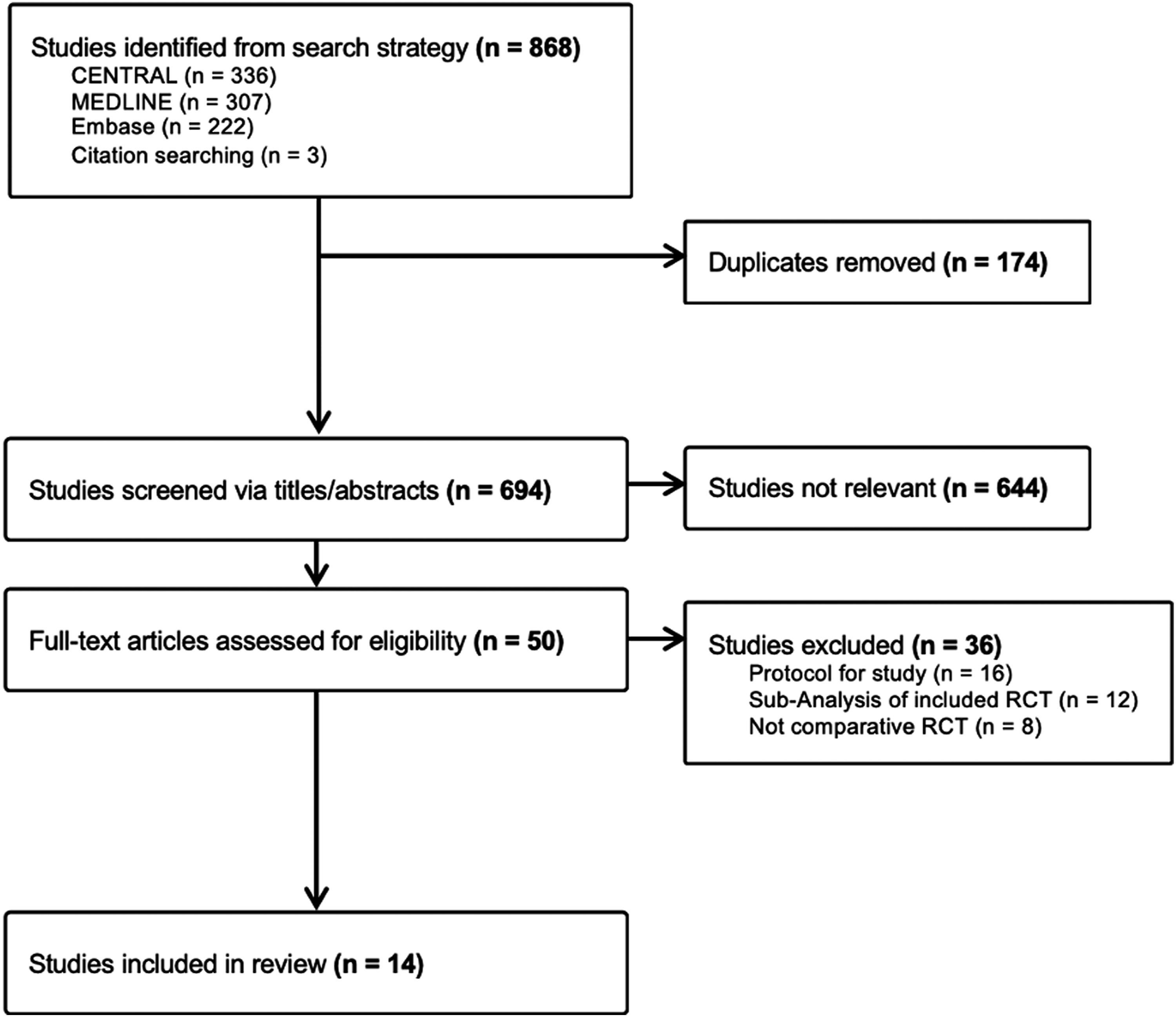
Baseline Characteristics and Outcomes of Patients Undergoing Bypass and Endovascular Revascularisation.
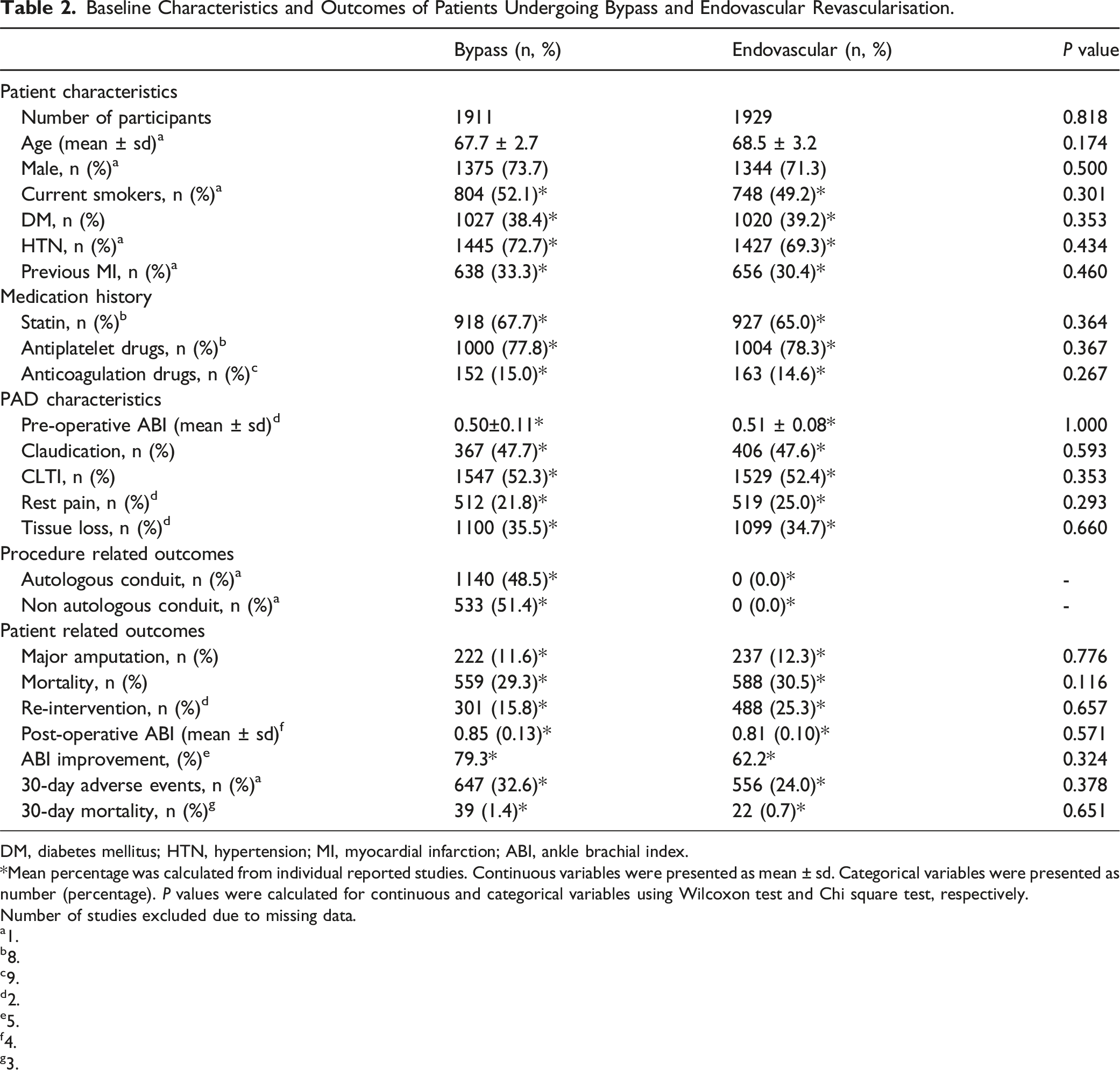
DM, diabetes mellitus; HTN, hypertension; MI, myocardial infarction; ABI, ankle brachial index.
*Mean percentage was calculated from individual reported studies. Continuous variables were presented as mean ± sd. Categorical variables were presented as number (percentage). P values were calculated for continuous and categorical variables using Wilcoxon test and Chi square test, respectively.
Number of studies excluded due to missing data.
a1.
b8.
c9.
d2.
e5.
f4.
g3.
Major Amputation
Major amputation data was reported in all 14 cohorts. The mean rate of major amputation was 11.6% and 12.3% in the bypass and endovascular groups, respectively (P = 0.776). ORs for major amputation are displayed in Figure 2, demonstrating no statistically significant difference between the 2 groups (OR 1.12, 95% CI 0.80-1.57, P = 0.486) with low heterogeneity (I2 = 17%, P = 0.27). Forest plot showing the odds ratio of major amputations between bypass vs endovascular treatment in people with peripheral artery disease.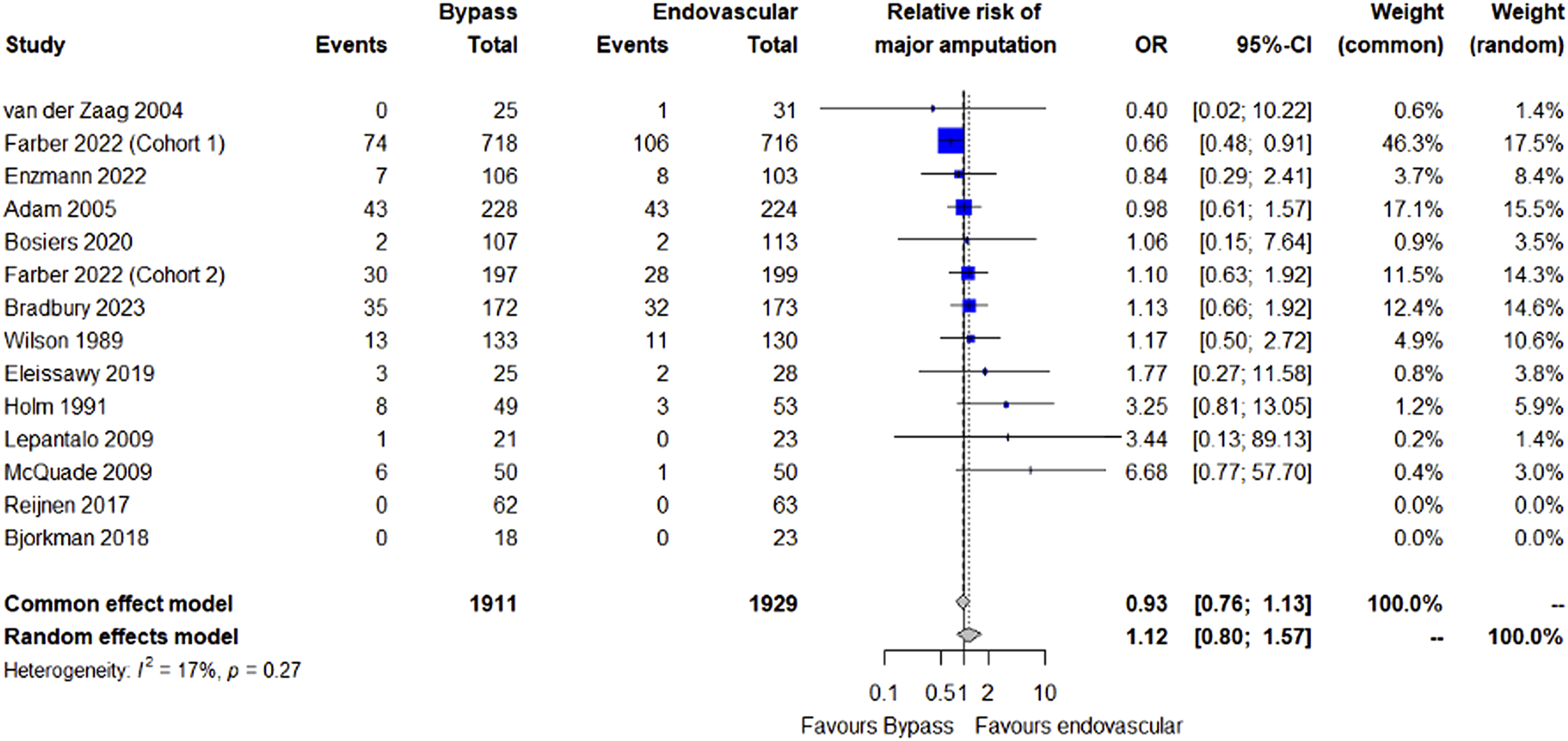
Mortality
Mortality data was reported in all 14 cohorts. The mean mortality rates were 29.3% and 30.5% in the bypass and endovascular groups, respectively (P = 0.116). Odds ratios for mortality are displayed in Figure 3 demonstrating no statistically significant difference between the 2 groups (OR 0.96, 95% CI 0.79-1.17, P = 0.681) with low heterogeneity (I2 = 0%, P = 0.57). Forest plot showing the odds ratio of mortality between bypass vs endovascular treatment in people with peripheral artery disease.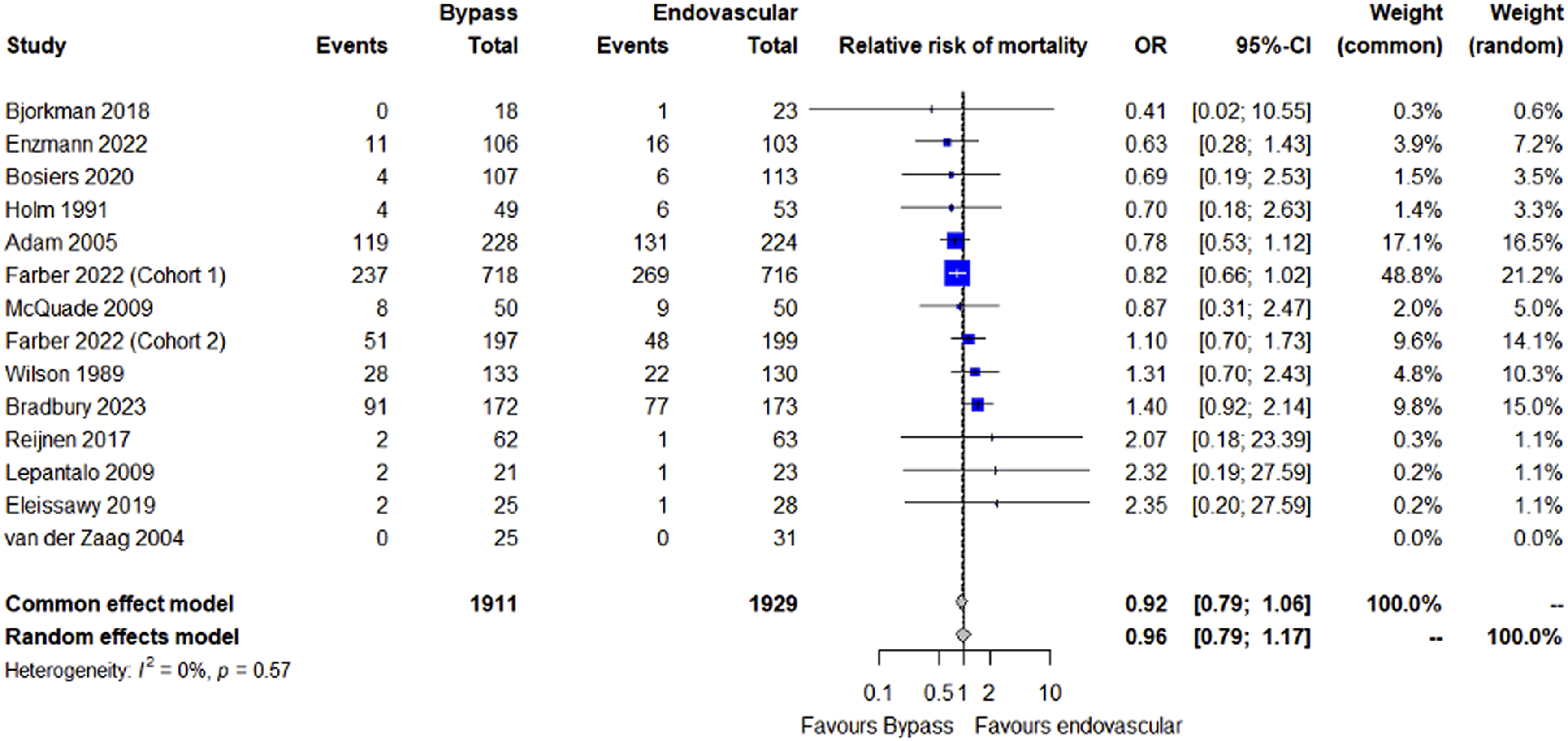
Re-intervention
Re-intervention data was reported in all except 2 cohorts19,21 which were excluded from the re-intervention analysis. Re-intervention was common with rates of 15.8% following bypass and 25.3% following endovascular revascularisation. Definitions used for re-intervention varied between studies. Most commonly, re-intervention was reported as any repeat revascularisation on the ipsilateral limb. One trial
8
reported minor and major re-intervention separately. In this case only major re-intervention (requiring thrombectomy or thrombolysis) was collected to avoid double counting patients who underwent both minor and major re-intervention. Figure 4 shows a significantly lower rate of re-intervention following bypass surgery (OR 0.57, 95% CI 0.40-0.82, P = 0.006), however there was a moderate amount of heterogeneity between trials (I2 = 59%, P < 0.01). Forest plot showing the odds ratio of re-intervention between bypass versus endovascular treatment in people with peripheral artery disease.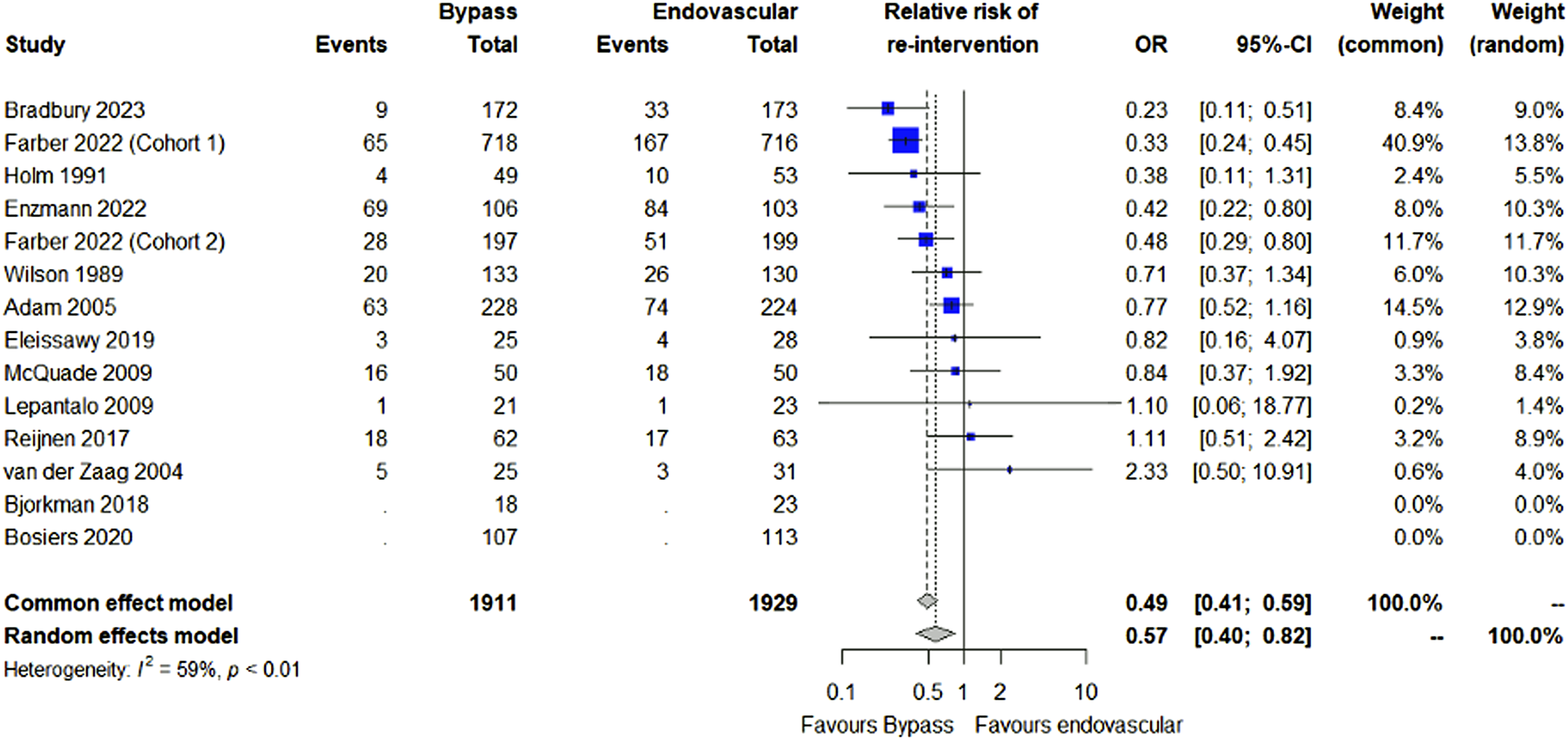
Other Outcomes
Both procedures provided an increase in ABI, with no significant difference between bypass surgery and endovascular revascularisation (79.3% vs 62.2% increase, P = 0.324). There was no significant difference in the risk of 30-day adverse events (32.6% vs 24.0%, P = 0.378) and mortality (1.4% vs 0.7%, P = 0.651) between the bypass and endovascular groups.
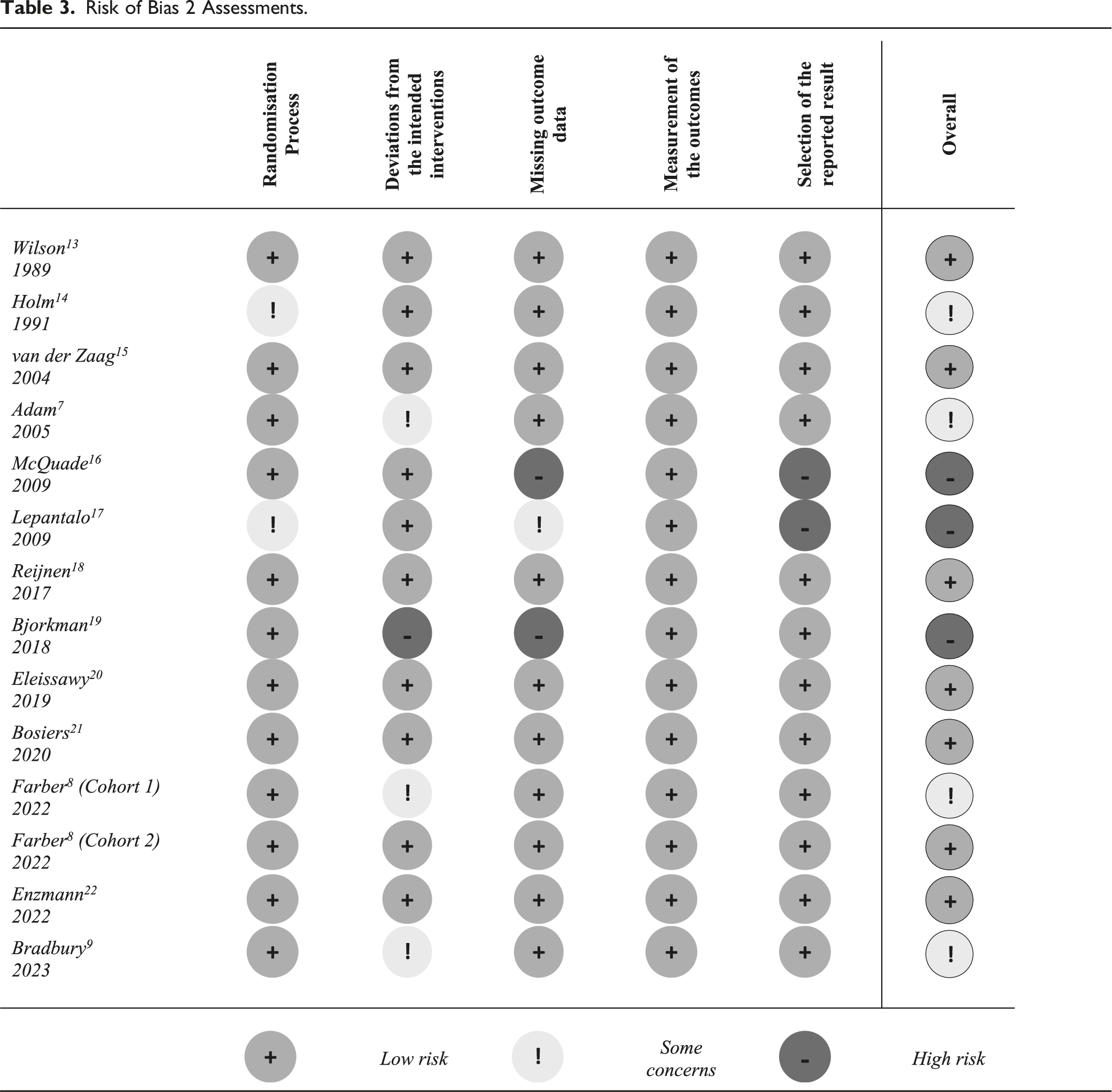
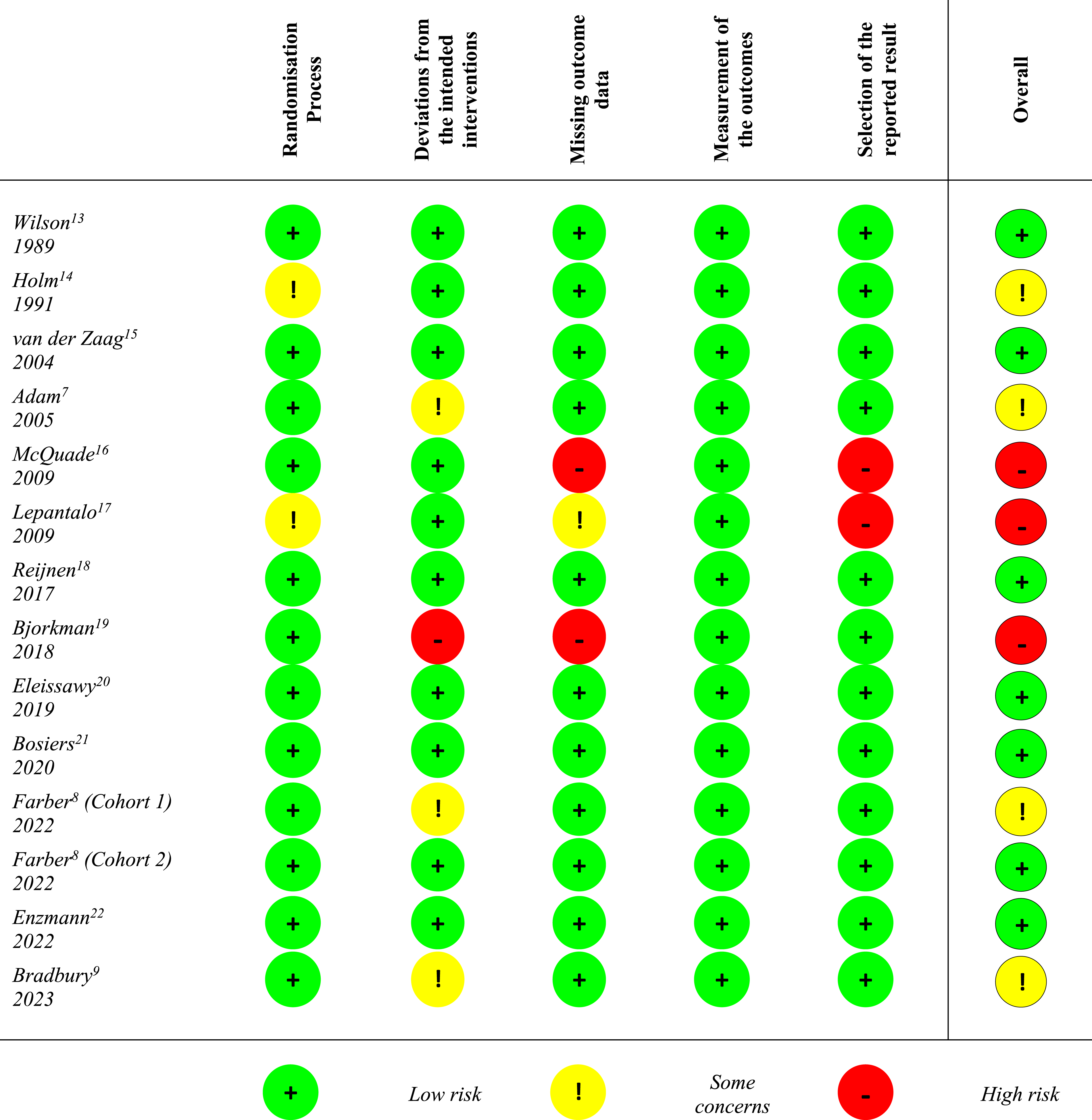
Risk of Bias
Risk of Bias 2 Assessments.
Discussion
Among patients with PAD, endovascular intervention is thought to have lower procedural risks and higher rates of re-intervention compared with bypass surgery, however there remains uncertainty as to which approach is most protective against limb loss. This systematic review and meta-analysis of 14 cohorts in 13 RCTs demonstrated no significant difference in the risks of major amputation, mortality, or peri-operative adverse events following bypass surgery or endovascular revascularisation for PAD. Patients who were allocated to endovascular intervention had almost double the risk of re-intervention compared to those who were allocated bypass surgery.
Major Amputation, Mortality and Re-Intervention
Prevention of major amputation is the primary goal of revascularisation in people with CLTI. Although amputation-free survival is the primary endpoint in many trials, major limb amputation is used here due to expected differences in limb outcomes, rather than overall survival which is often determined by other comorbidities. A greater number of studies could then be analysed, including those based upon anatomical outcomes such as patency or target lesion revascularisation, which often report major amputation but not amputation-free survival. Major amputation rates of 11.6% and 12.3% following bypass and endovascular revascularisation seen in this study are comparable with previous large population registries.23,24
The weighted mean proportion of patients with CLTI in the included studies was 80.0%. Whilst the major amputation rate in patients with IC may be significantly lower than those with CLTI, 24 this group represented only a minority of the included population. Inclusion of all patients with PAD meant data from 14 cohorts could be included, rather than only BASIL, 7 BEST-CLI, 8 and BASIL-2. 9
All-cause mortality was high in both population groups (29.3% and 30.5%, respectively). This reflects the relatively poor prognosis of patients with PAD despite revascularisation due to systemic atherosclerotic disease, with a known 20%–26% 1-year mortality in those diagnosed with CLTI. 1 These results emphasise the importance of best medical therapy among this particularly high-risk group of patients.
Our findings suggest bypass surgery may be more durable than endovascular procedures. Increased re-intervention has significant implications on health care utilisation and subjects a multi-morbid population to repeated procedures. Further, secondary bypass after initial endovascular intervention has been shown to have inferior long-term outcomes to primary bypass.25-27 Avoiding re-intervention by providing a durable first revascularisation procedure is therefore important. Our study did not explore the optimal modality of re-intervention. Factors including health care accessibility, patient comorbidities and individual preferences all contribute to whether repeated minimally invasive endovascular re-interventions, or more invasive surgical intervention with less frequency, may be more appropriate. Clinicians should anticipate re-intervention during initial revascularisation and avoid techniques which may compromise future procedures. Separate investigations focussing on the optimal sequence and modality of re-intervention following bypass surgery and endovascular revascularisation are required.
Prior literature, including a Cochrane review 28 and multiple meta-analyses,4,5 similarly demonstrate no significant difference in major amputation or mortality after bypass surgery or endovascular revascularisation. Other reviews including observational studies 6 show comparatively higher rates of long-term major amputation and mortality after endovascular revascularisation, however this may relate to greater co-morbidity in those selected for minimally invasive procedures in non-randomised observational studies. Further analyses of the initial BASIL trial have also demonstrated improved overall survival following bypass surgery in those patients surviving beyond 2 years. 29 The BEST-CLI 8 trial, the largest and highest weighted study in our analysis, demonstrated a reduction in major adverse limb events or death following bypass compared with endovascular revascularisation when an autologous conduit was available. The majority of studies included in this meta-analysis did not report outcomes stratified by the availability of autologous conduit, preventing sub-group analysis. This sub-group may have improved outcomes following bypass surgery, which may translate to reduced amputation risk compared with endovascular intervention. A major contributor to the difference in major adverse limb events observed in BEST-CLI, 8 was a significantly higher rate of major re-intervention after endovascular procedures (23.5% vs 9.2%), as was seen in our review. Reduced re-intervention was also seen following bypass in the BASIL 7 and BASIL-2 9 trials, supporting the results seen in our analysis. BEST-CLI 8 has been criticised because of the implications of the high endovascular re-intervention rate (23.5%) on its outcomes, however this was comparable to our findings (25.3%).
Outcomes of the recent BASIL-2 9 trial appear contrary to previous evidence, with a reduction in major amputation and death following endovascular revascularisation compared with bypass. This likely relates to the anatomic distribution of disease, with BASIL-2 exclusively recruiting patients requiring infrapopliteal intervention. Sub-analysis of patients with infrapopliteal disease from the initial BASIL study did not demonstrate a significant difference between angioplasty and bypass surgery, potentially reflective of advancement in endovascular techniques over this period. 30 Our meta-analysis included patients with both femoropopliteal and infrapopliteal disease. Whilst the anatomical location of disease likely plays an important role in the optimal revascularisation procedure for an individual patient, differentiating these groups to perform separate analyses is challenging. PAD is a systemic disease and most patients have some degree of both femoropopliteal and infrapopliteal disease. Further, outcomes are rarely reported in separate disease segments in the existing literature. Outcome reporting based upon anatomical classification of disease, such as via the Global Anatomic Staging System (GLASS), 1 is an important consideration for future research.
Inclusion of the BEST-CLI 8 and BASIL-2 9 trials nearly doubles the available patients to address this research question (n = 3740, compared with 1458 without). Whilst formal analysis with and without inclusion of these trials was not pursued, BASIL-2 was the only trial with a primary outcome suggesting superior results following endovascular revascularisation. Given this, it is likely that future trials implementing the full array of endovascular interventions will continue to support the viability of endovascular revascularisation.
Specific Populations
Comprehensive treatment of PAD also requires aggressive control of modifiable risk factors. Provision of antiplatelet and statin therapy preoperatively was <80% in both groups. Data regarding other risk factor modifying therapies such as angiotensin-converting enzyme inhibitors (ACEIs), angiotensin receptor blockers (ARBs), medications for diabetes control, and emerging alternate anti-thrombotic strategies such as low-dose rivaroxaban, 31 were too infrequently reported to include, and may not have been available during earlier trials. These therapies may significantly alter prognosis for patients with PAD and emphasise the need for greater attention to non-operative optimisation.
High rates of diabetes (53.7%), previous myocardial infarction (34.9%), hypertension (77.4%) and current smoking (41.8%) were seen in this review. Included trials appear to show a changing patient demographic, with increasing prevalence of diabetes and decreasing rates of smoking over time, however this was not specifically analysed. Diabetes may be associated with more distal distribution of arterial disease, 1 which, as shown in the BASIL-2 9 trial, may be more amenable to endovascular revascularisation. Further evaluation of this trend may support increasing endovascular intervention moving forward.
Given the heterogeneity between populations, and incomplete reporting of some outcome variables, subgroup or meta-regression analyses of specific patient groups were deemed non-representative and not pursued.
Although there was a non-significant trend towards higher peri-operative adverse events following bypass surgery (32.6% vs 24.0%, P = 0.378), further analysis of this secondary outcome was not pursued due to heterogeneity in the included adverse events between studies. Dedicated research focussing on peri-operative outcomes is required.
Strengths and Limitations
This study systematically reviews and meta-analyses all RCTs comparing bypass and endovascular revascularisation for PAD and includes the results of the recently published BEST-CLI 8 and BASIL-2 9 trials. One other meta-analysis has evaluated results from these trials, however included only 3 cohorts. 32 Our study population was significantly larger which adds weight to the findings of this meta-analysis. Whilst our findings of increased re-intervention following endovascular intervention have been suggested previously, clinicians can now be confident this is supported by all available literature. Further, our study suggests that the optimal revascularisation approach remains uncertain despite these high-quality trials and justifies further research to guide management.
Apart from BEST-CLI 8 and BASIL-2, 9 all other trials included some patients with IC. This is an important limitation as these patients may not always require revascularisation and follow a notably different natural history to CLTI. Functional measures such as walking distance may be more appropriate outcomes for this population but were reported in no existing trials.
Availability of high-quality literature in this field remains limited, due to the challenging nature of research in a multi-morbid population, with heterogeneity in disease characteristics and procedures performed. The sample size of most included studies was small. Risk of bias was moderate or high in a large number of trials, particularly due to cross-over and loss to follow up. Further, non-standardised follow up durations for outcomes may present risk of bias. Due to the difficulty in performing RCTs in this population, publication bias from unpublished research is thought unlikely, although selection bias may have resulted from some patients not being considered for inclusion in RCTs. This may be due to differing perceptions regarding fitness for surgery, innate clinician preferences, or insufficient time for randomisation in acutely unwell patients. These findings may therefore not be generalisable to all populations.
Finally, there has been significant advancement in endovascular techniques throughout the included period. Limited reporting of outcomes stratified by specific endovascular procedures has prevented subgroup analysis or meta-regression of newer endovascular techniques, which may have improved outcomes compared with balloon angioplasty. Patient-level meta-analysis of the BEST-CLI 8 and BASIL-2 9 trials is expected and will expand upon this work. Ultimately, the most appropriate revascularisation strategy for an individual patient is likely more nuanced than simply comparing bypass and endovascular revascularisation dichotomously.
In conclusion, this systematic review and meta-analysis demonstrated that bypass surgery and endovascular revascularisation for PAD result in comparable rates of major amputation, mortality, and peri-operative outcomes. Despite this, patients who undergo bypass surgery have a significantly lower rate of re-intervention. Further evaluation as to whether these results are reproducible in specific patient populations, including those with infrapopliteal disease, and following particular procedures, namely bypass with autologous conduit and specific endovascular interventions, is warranted.
Supplemental Material
Supplemental Material - Meta-Analysis of Randomised Controlled Trials Comparing Bypass and Endovascular Revascularisation for Peripheral Artery Disease
Supplemental Material for Meta-Analysis of Randomised Controlled Trials Comparing Bypass and Endovascular Revascularisation for Peripheral Artery Disease by Angus H. Pegler, Shivshankar Thanigaimani, Siddharth S. Pai, Dylan Morris, and Jonathan Golledge in Vascular and Endovascular Surgery
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
Data Availability Statement
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.