
Abstract
Intermittent pneumatic compression (IPC) is designed to aid wound healing and limb salvage for patients with critical limb ischaemia who are not candidates for revascularisation. We conducted a systematic review of the literature to identify and critically appraise the evidence supporting its use in this population. A search was conducted in Embase, MEDLINE and clinical trial registries up to the end of March 2013. No date or language restrictions were applied. Quality assessment was performed by two people independently. Quality was assessed using the Cochrane risk of bias tool and the NICE case-series assessment tool. Two controlled before-and-after (CBA) studies and six case series were identified. One retrospective CBA study involving compression of the calf reported improved limb salvage and wound healing (OR 7.00, 95% CI 1.82 to 26.89, p<0.01). One prospective CBA study involving sequential compression of the foot and calf reported statistically significant improvements in claudication distances and SF-36 quality of life scores. No difference in all-cause mortality was found. Complications included pain associated with compression, as well as skin abrasion and contact rash as a result of the cuff rubbing against the skin. All studies had a high risk of bias. In conclusion, the limited available results suggest that IPC may be associated with improved limb salvage, wound healing and pain management. However, in the absence of additional well-designed analytical studies examining the effect of IPC in critical limb ischaemia, this treatment remains unproven.
Introduction
Optimal treatment for patients with critical limb ischaemia involves revascularisation along with a multidisciplinary approach to controlling pain and cardiovascular risk factors. 1 Alternative treatments for patients who are unsuitable for open or endovascular intervention are limited, with approximately 50% undergoing primary amputation and 50% receiving medical treatment only. The efficacy of pharmacotherapy in this latter group is limited, however, with trial data showing a 20% mortality rate and 60% amputation rate at 6 months. 1 Intermittent pneumatic compression (IPC) has been proposed as an adjunct to best medical care, aimed at preventing amputation, relieving pain and promoting wound healing by increasing arterial blood flow in distal limbs. While the exact mechanism of action is unproven, a number of possible effects have been postulated to explain why IPC would increase arterial blood flow, including increased arteriovenous pressure gradient, stimulation of endothelial vasodilators, suspension of the venoarteriolar reflex and stimulation of collateral artery growth.2–4 Despite this technology having been available in its present form for well over a decade, uncertainty remains about its clinical effectiveness in a population who are in urgent need of effective treatment options. The aim of this review is to identify and critically appraise the clinical evidence on whether IPC treatment is superior to medical care alone in patients with critical limb ischaemia who are not candidates for percutaneous transluminal angioplasty (PTA) or surgical revascularisation.
Methods
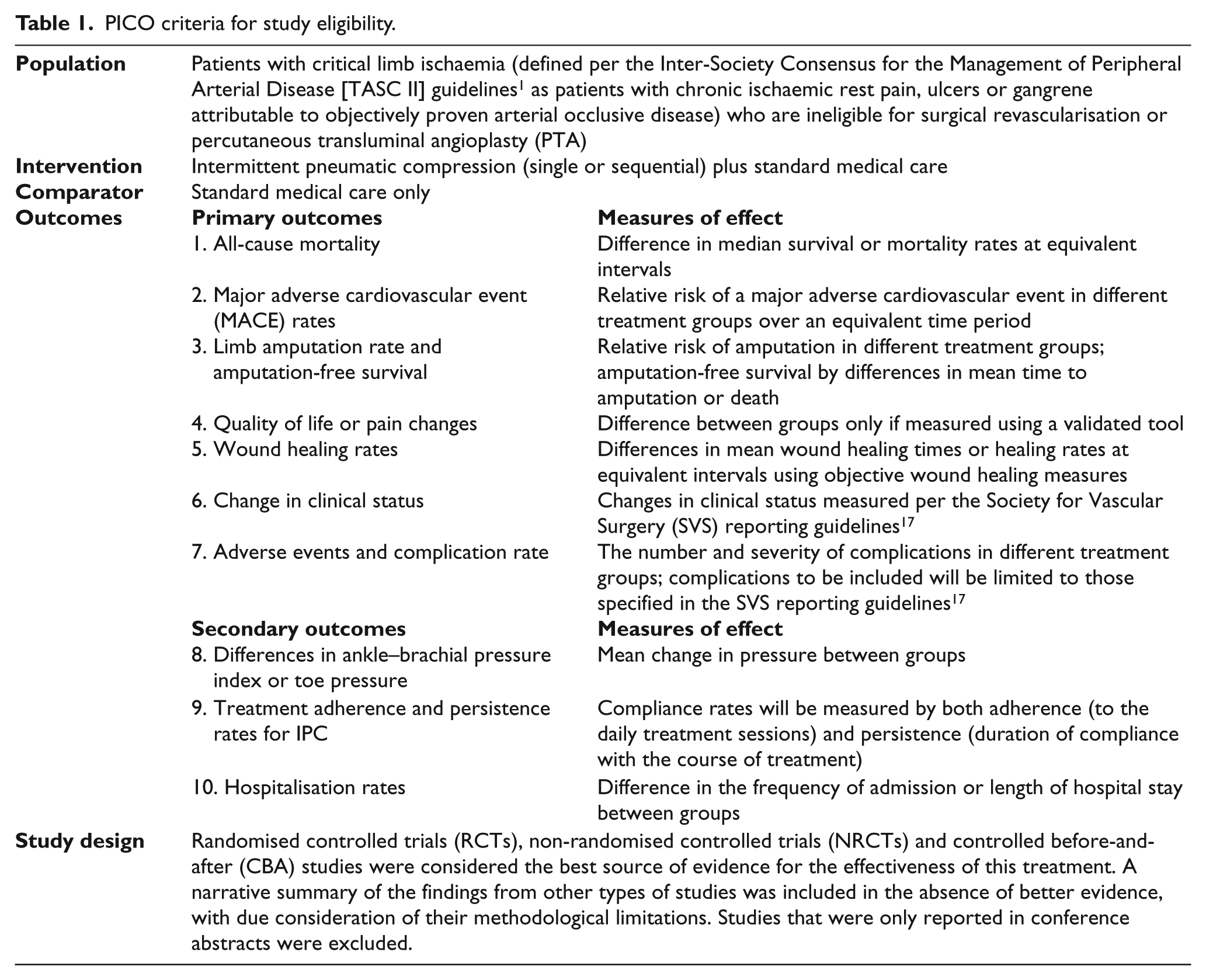
A search for studies comparing IPC plus standard medical care to standard medical care only in patients with critical limb ischaemia who were ineligible for revascularisation was conducted in Embase, MEDLINE and Scopus. The ISRCTN Register, the Cochrane Central Register of Controlled Trials and ClinicalTrials.gov were also searched. No date or language restrictions were applied. All searches were carried out up to the end of March 2013. Hand-searching of reference lists of relevant studies and previous review articles was also performed. Device manufacturers and leading authors in this area were contacted to identify other relevant published or unpublished studies, as well as ongoing or planned studies. The criteria for including studies are shown in Table 1.
PICO criteria for study eligibility.
Preliminary screening of all returned results was carried out by a single person (PM) to eliminate studies that were clearly not relevant. Assessment of eligibility of studies and identification of multiple reports from single studies was carried out independently by two people (PM and either PH or CT). Any disagreements were resolved by discussion. Data extraction was performed independently by two people (PM and CT), disagreements were resolved by discussion. Assessment of the risk of bias of included studies was performed by two people independently (PM and CT). Risk of bias and quality assessment tools depended on the study design. The Cochrane risk of bias tool 5 was chosen for assessing randomised controlled trials (RCTs), non-randomised controlled trials (NRCTs) and controlled before-and-after (CBA) studies, using the nine-item checklist developed by the Cochrane Effective Practice and Organisation of Care Group (EPOC). 6 For cohort studies the SIGN-50 quality assessment tool 7 was chosen and the NICE appraisal tool 8 was used to assess case series.
Results
Our search identified eight completed studies and two planned studies that met the inclusion criteria (Figure 1).
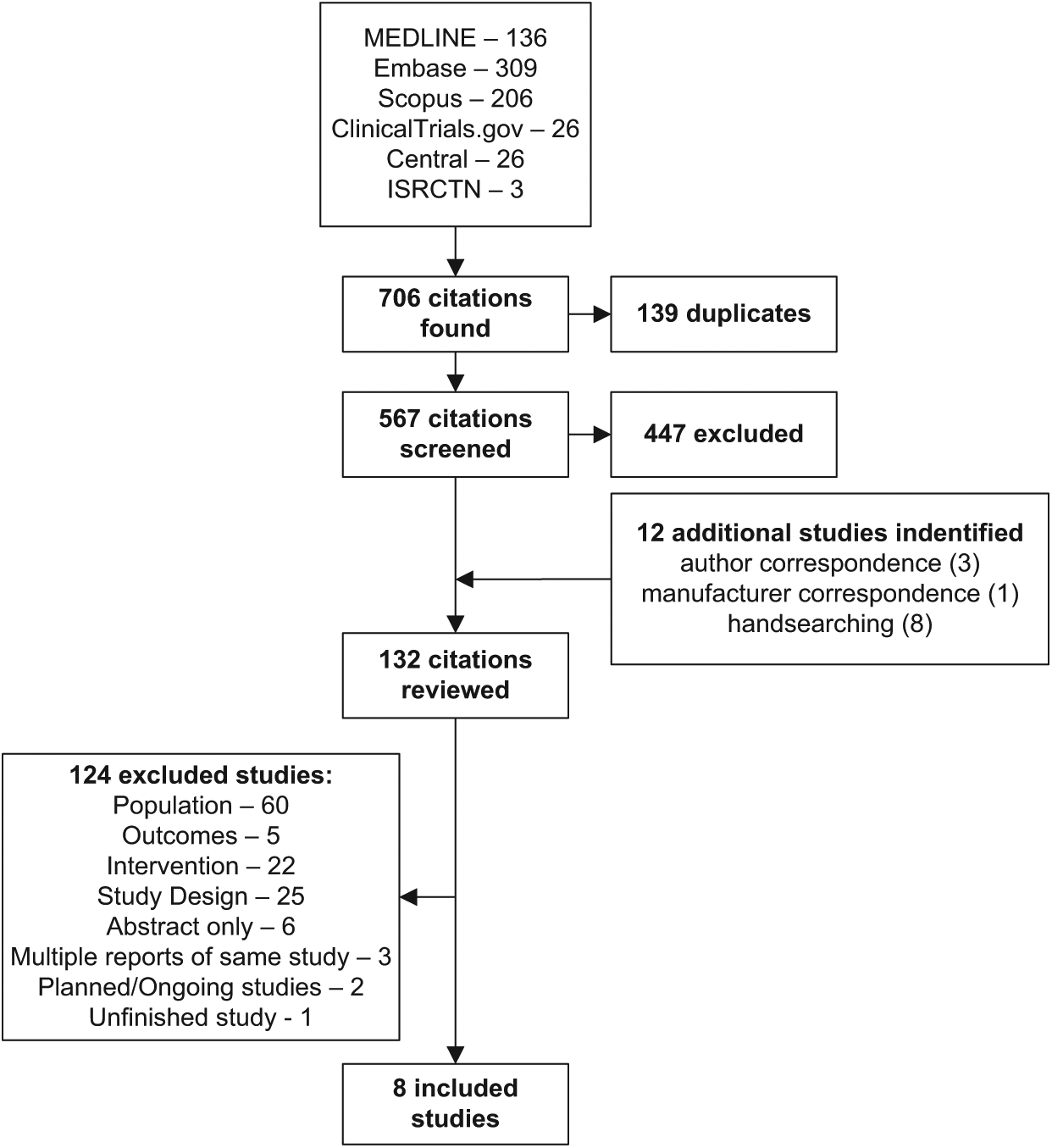
Flow chart of study inclusion and exclusion.
No RCT or NRCT studies were identified. Two CBA studies were included,9,10 along with six11–16 descriptive studies (case series). The assessment of study quality found both CBA studies to have a high risk of bias (Figure 2). All case series inherently carry a high risk of bias and the performance of each one was scored on eight criteria (1 if met, 0 if not). Results of the quality appraisal and a summary of each included study are shown in Table 2.
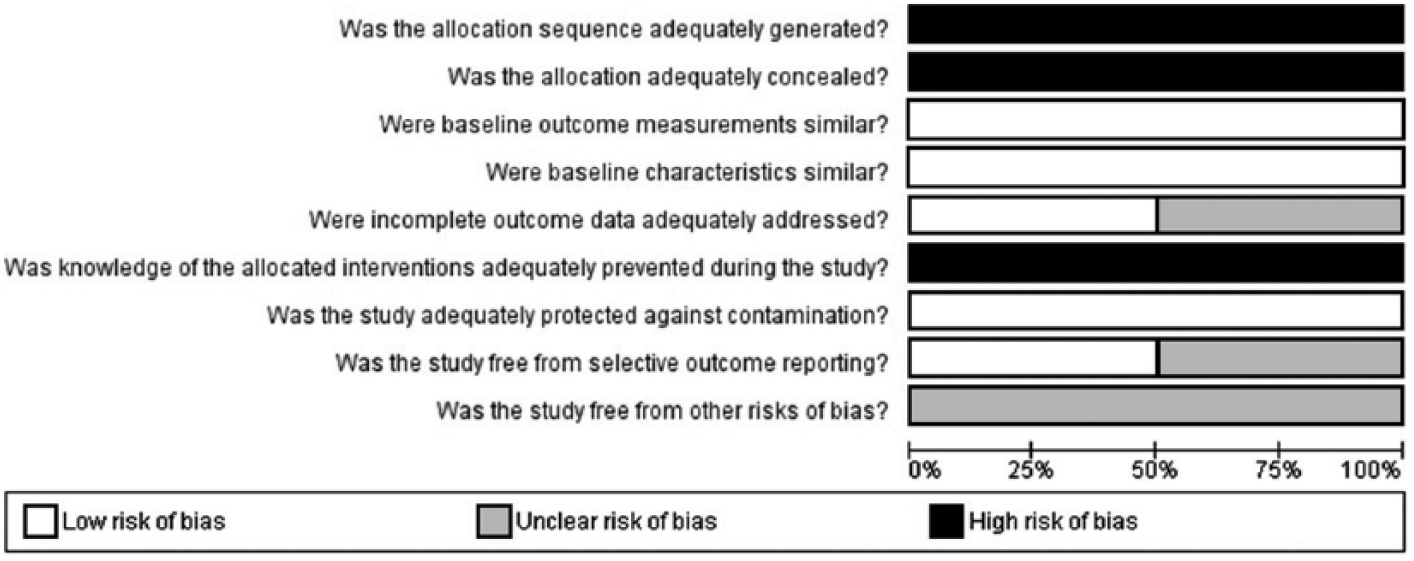
Review of authors’ judgements about each risk of bias item, presented as percentages across both included controlled before-and-after (CBA) studies.
Details of included studies.
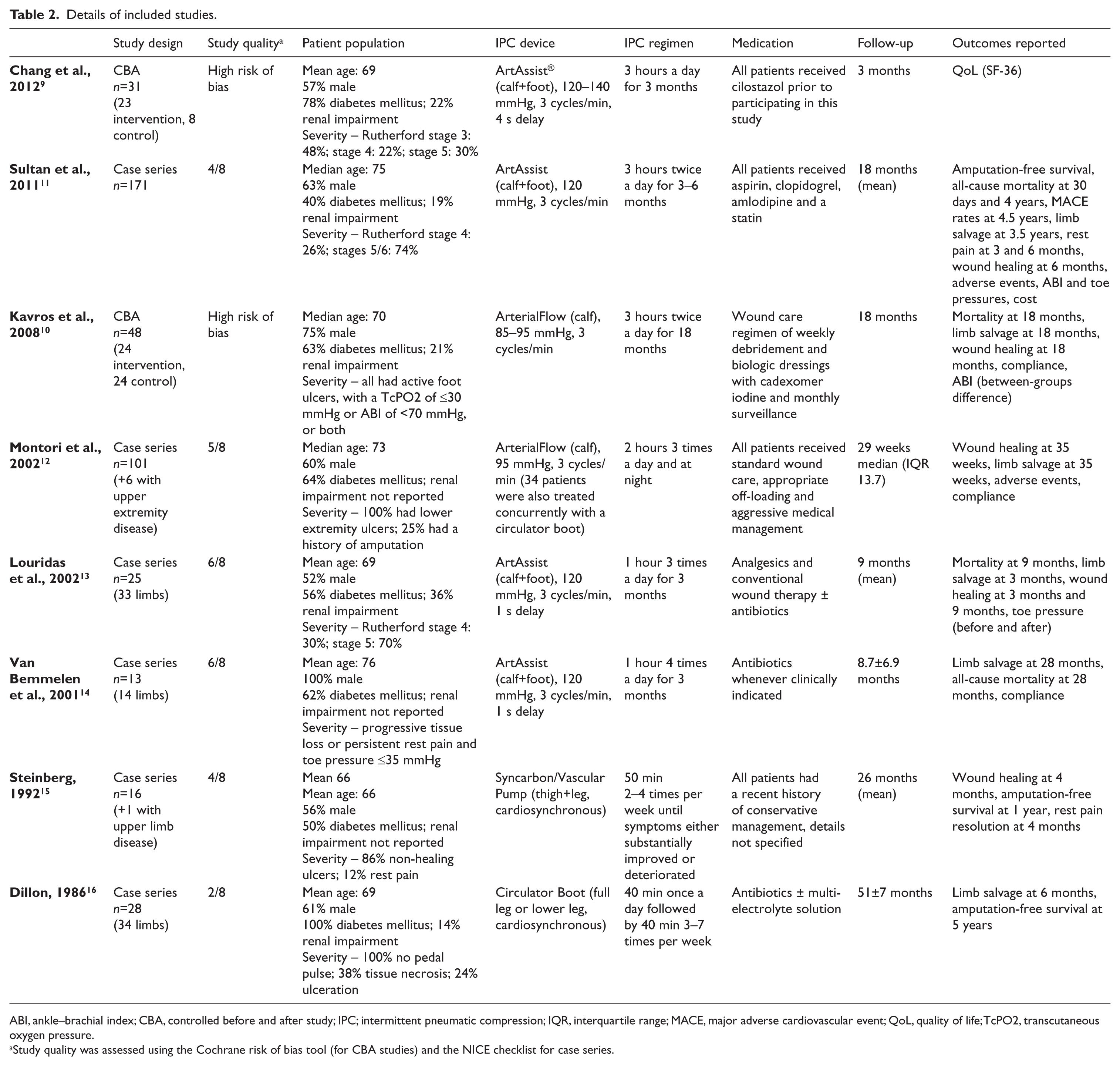
ABI, ankle–brachial index; CBA, controlled before and after study; IPC; intermittent pneumatic compression; IQR, interquartile range; MACE, major adverse cardiovascular event; QoL, quality of life; TcPO2, transcutaneous oxygen pressure.
Study quality was assessed using the Cochrane risk of bias tool (for CBA studies) and the NICE checklist for case series.
No studies reported results on hospitalisation rates or change in clinical status as measured per the Society for Vascular Surgery (SVS) reporting guidelines. 17 All included studies carried out since 2000 involve either the ArtAssist® (ACI Medical, San Marcos, California) or ArterialFlow (DJO, Vista, California) IPC devices. Studies from beyond this point involve devices that are programmed to provide compression that is synchronised with the patient’s heartbeat (cardiosynchronous compression, CSC). These devices include an electrocardiogram module that activates the pump following every one or two QRS complexes detected. This is in contrast with more recent studies that involved devices that do not monitor heart rhythm and are programmed to provide less frequent compression (three times per minute).
Mortalit.y
The only comparative study that reported all-cause mortality failed to find a significant difference between the control and intervention (ArterialFlow). Case series estimates of the mortality rate following IPC treatment with the ArtAssist device were not fully consistent with this data (Table 3).
Results.
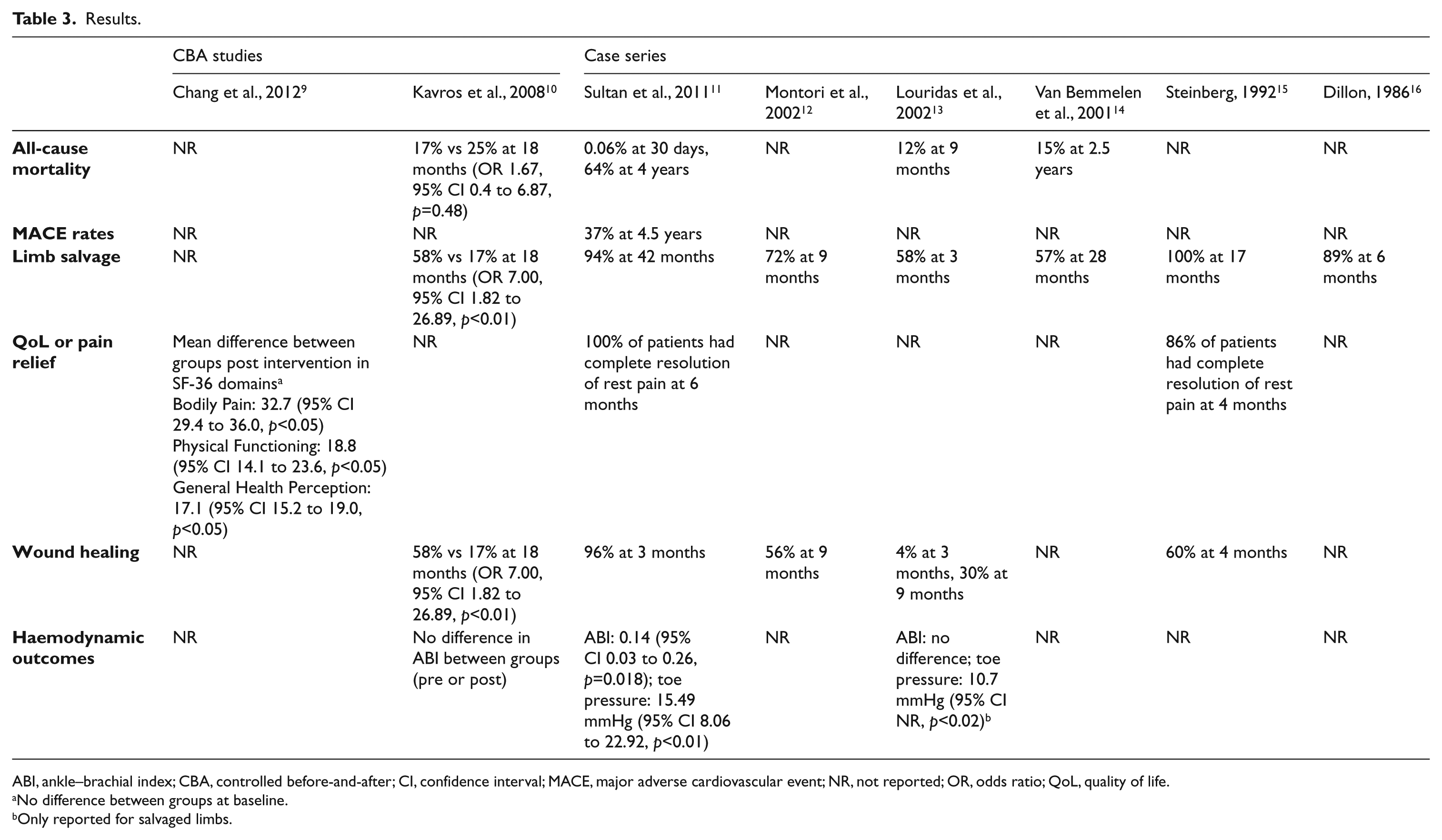
ABI, ankle–brachial index; CBA, controlled before-and-after; CI, confidence interval; MACE, major adverse cardiovascular event; NR, not reported; OR, odds ratio; QoL, quality of life.
No difference between groups at baseline.
Only reported for salvaged limbs.
MACE rates
One case series 11 reported the rate of major adverse cardiovascular events (MACE) in patients treated with IPC (37% at 4.5 years). While no directly comparable data from controls are available, a subsequent analysis comparing this patient group to historical matched controls that underwent primary amputation 18 reported a MACE rate of 68% at 4.5 years in the amputation group.
Limb salvage and amputation-free survival
Estimates of limb salvage rates were provided in seven studies (see Table 3). The only study to include a comparison group found a large, statistically significant effect in favour of IPC treatment. However, estimates for this outcome showed a lack of consistency, with some showing almost full long-term limb salvage and others showing significant limb loss at 3 months. Amputation-free survival is defined as the time from receiving the intervention to amputation or death, or the percentage of patients alive and without amputation at a given time period after the intervention. Only one case series 11 reported this outcome, with the median amputation-free survival time being 18 months. A comparison of results at different intervals is shown in Figure 3.
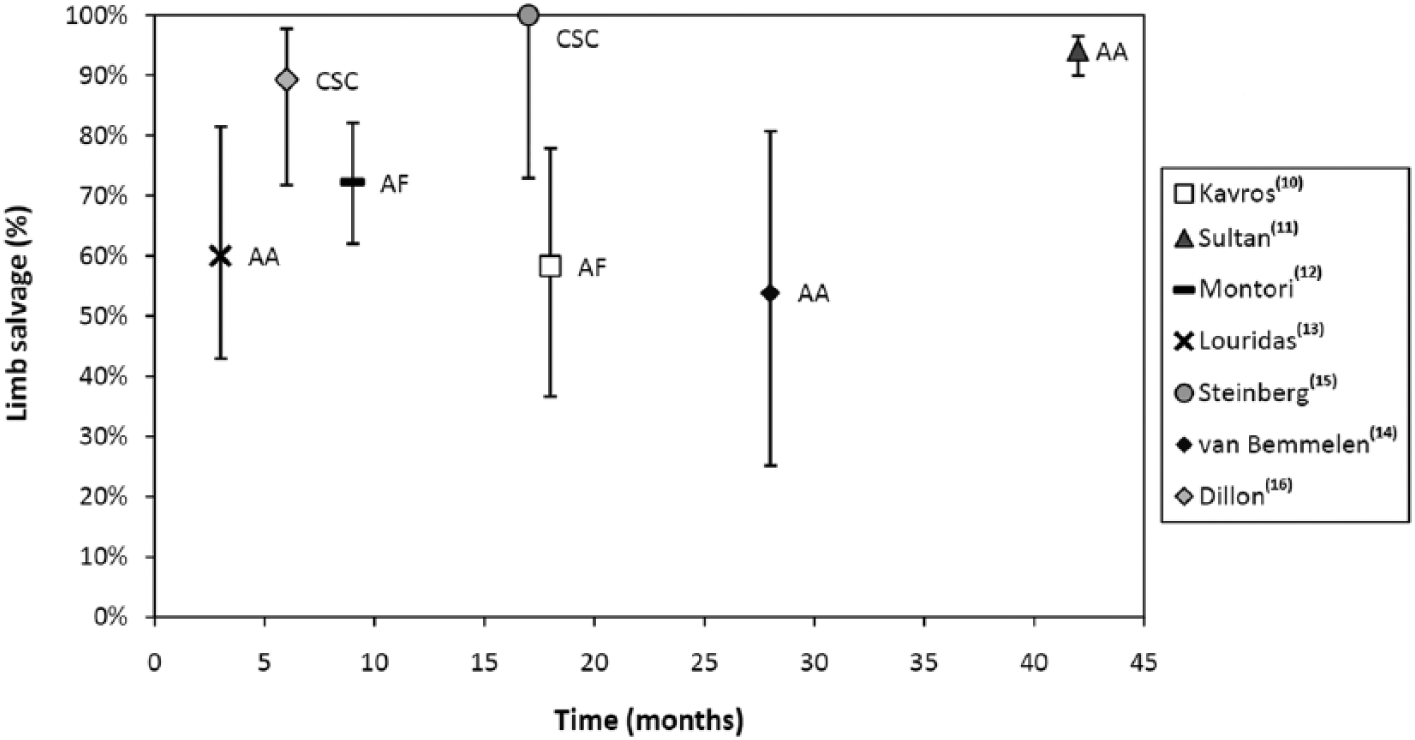
Limb salvage results. (AA, ArtAssist IPC device; AF, ArterialFlow IPC device; CSC, cardiosynchronous compression device. Bars indicate 95% confidence intervals.)
Quality of life and pain relief
Quality of life (QoL) and pain relief results were included if they were measured by a validated tool (e.g. SF-36) or if presented as the number of patients with complete resolution of rest pain associated with critical limb ischaemia. One CBA study 9 showed significant differences in SF-36 scores for bodily pain, physical functioning and general health perception in the post-intervention treatment group (see Table 3). Using the reliable change index 19 to evaluate clinical significance in SF-36 outcomes for this age group, only the changes in bodily pain and physical functioning domains exceeded the threshold for clinical significance. Two case series reported complete rest pain resolution in a high percentage of patients receiving IPC treatment (86% at 4 months 15 and 100% at 6 months 11 ).
Wound healing
Wound healing was reported in five studies (Table 3). Similar to limb salvage, high levels of heterogeneity were seen in the reported results for this outcome. Improvements in wound healing were only eligible for inclusion if measured by an objective scale. Since no studies used such a scale these results only reflect complete wound healing rates. As with limb salvage, the only comparative study that reported results for this outcome found a large, statistically significant effect in favour of IPC treatment. 10 A comparison of reported results at different intervals is shown in Figure 4.
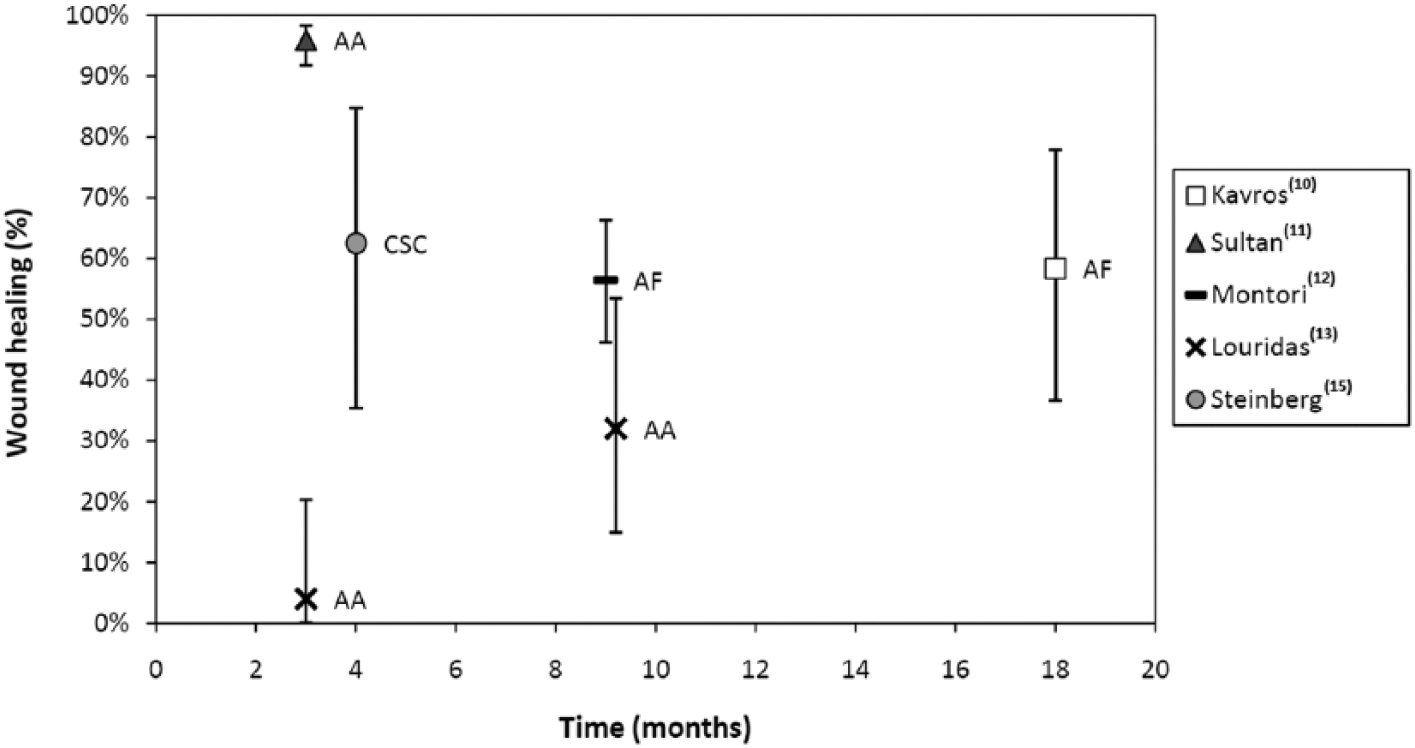
Wound healing results. (AA, ArtAssist IPC device; AF, ArterialFlow IPC device; CSC, cardiosynchronous compression device. Bars indicate 95% confidence intervals.)
ABI and toe pressure
Three studies reported a difference in ankle–brachial index (ABI) and toe pressures following IPC treatment. In two case series a statistically significant improvement (10–15 mmHg) in toe pressures was observed following treatment (Table 3).
Adverse events and compliance
No serious adverse events related to the use of IPC were reported. Among the less serious complications reported were abrasion of the dorsal foot as a result of the cuff rubbing against the skin 13 and localised pain associated with compression. 15 In one case series 12 involving 101 patients, 10 reported pain using the device (ArterialFlow), with seven patients (7%) discontinuing the treatment as a result. A single case of contact skin rash was also reported in this study.
Compliance with the treatment was discussed in two studies. Kavros et al. 10 reported that 20 out of 24 (83%) IPC patients complied fully with the allotted schedule of two 3-hour sessions per day, with no-one spending less than 4.5 hours a day using the device. In another case series 14 involving 13 patients who were instructed to use the device for 4 hours a day, the overall average daily use was approximately 2 hours. In this study the average daily use time for people with intact limbs was 2.4 hours compared to 1.1 hours in patients who underwent amputation, although patients who were less compliant could have been more infirm.
Discussion
The idea of using compression therapy to increase arterial blood perfusion was first described in the mid-19th century, 20 with initial results of the application of this treatment in the lower extremities of patients with obstructive arterial disease published in the 1930s.21,22 Despite the long history of this treatment there remains a lack of high-quality evidence demonstrating its effectiveness in patients with critical limb ischaemia who are not suitable for percutaneous transluminal angioplasty or surgical revascularisation. This review failed to identify any RCTs or NRCTs evaluating efficacy in this population. Two controlled CBA studies and six descriptive studies (case series) were included. Three different types of IPC device were examined in these studies: the ArtAssist device, which provides sequential compression to the foot and calf; the ArterialFlow device, which compresses the calf; and two different devices that supply leg compression that is synchronised with ventricular contraction of the heart.
Both of the identified CBA studies were judged to be at high risk of bias. There was a general lack of consistency in the reported results for all outcomes across different device and study designs. One retrospective study reported a large statistically significant effect in favour of IPC for limb salvage and wound healing (OR 7.00, 95% CI 1.82 to 26.89, p<0.01) in a population that had non-healing wounds from previous toe or transmetatarsal amputation. 10 The other study, a prospective controlled before and after trial examining changes in quality of life associated with IPC treatment, found significant improvement in the bodily pain, physical functioning and general health perception domains of the SF-36 scale. 9 Case series data differed considerably between studies, with wound healing at 3 months ranging from 4% to 96% in studies that used the same IPC device. Mortality results from case series were more consistent. However, while these types of descriptive study designs are useful for hypothesis generation and proof of concept, they are not sufficiently robust to establish causality. A further source of heterogeneity is differences in the medical care provided to participants of included studies. Some studies did not provide adequate detail on the treatment being provided in conjunction with IPC and none mentioned the use of prostanoids. Although there is some uncertainty in relation to the optimal medical regimen in this cohort, it is unlikely that historical studies involved what would currently be considered best medical care. Greater consistently in the choice of pharmacotherapy used in both treatment and comparison groups in any future studies would allow for a better estimation of the incremental benefit, if any, of using IPC.
Given the paucity of evidence demonstrating the effectiveness of IPC in critical limb ischaemia, is it inadvisable to perform subgroup analysis of different types of patients. Analysis of this type increases the risk of bias and therefore further limits the extent to which meaningful conclusions can be drawn from what is already a weak evidence base. Equally, there is insufficient evidence to perform subgroup analysis by study design, by type of device, or by different sets of compression parameters. The literature does, however, draw attention to the potential importance of patients with diabetes and those with renal failure. Given diabetes status as a risk factor for vascular disease 1 and its rising prevalence, the efficacy of IPC in this subgroup is of particular importance. It has been suggested that IPC is less effective in patients with renal failure (Louridas G, A randomised, placebo-controlled limb salvage trial using the ArtAssist pneumatic compression device. Unpublished observations, 2002; van Bemmelen PS, Personal communication, 2013), with the prognosis for this group being worse for both limb salvage and mortality.
Patients with unreconstructable critical limb ischaemia or those who are otherwise unsuitable for revascularisation generally have a poor prognosis, with the main treatment options being pharmacological management or primary amputation. The introduction of a treatment with a low risk of complications that could convincingly demonstrate even a modest clinical benefit might therefore be worthwhile in this population, given the lack of effective alternatives for some patients. Furthermore, considering the relatively low cost of the intervention compared to the consequences of failing to adequately manage this condition, there is a possibility that IPC may also be a cost-effective treatment option even if the magnitude of the effect size was small. Both these considerations depend on having robust evidence from high-quality studies, which is as yet unavailable.
A systematic review 23 of IPC in lower extremity arterial disease carried out in 2002, which included studies in patients with less severe PAD and healthy volunteers, found that treatment was associated with physiological benefits such as increased arterial flow, peak systolic velocity, end diastolic velocity and pulse volume. As with this review, the authors concluded that the use of IPC appears promising in patients with severe peripheral artery disease who are not candidates for surgery or percutaneous transluminal angioplasty – but more research is needed. A more recent review on IPC for treating chronic arterial ulcers 24 noted the lack of any prospective controlled studies comparing healing outcomes and the high level of heterogeneity that exists between available studies. It also concluded that further trials are warranted given the promising results to date.
In the absence of good-quality evidence, there is a danger that results from studies with a high risk of overestimating the effect of this treatment due to systemic bias are eventually accepted as sufficient to support routine use. A recent narrative review 25 is an example of how easily the debate can move on to not if, but why IPC is effective. The benefit of the systematic review methodology used in this study is that it clearly outlines the evidence base for IPC in the most clinically important patient group, rather than attempting to draw conclusion from a diverse population that includes patients with very different disease severity profiles and available treatment options, thus allowing clinicians and service providers to more reliably judge the likely consequences of choosing from among competing alternatives in the management of this disease.
Conclusions
There is a lack of experimental studies examining the clinical effectiveness of IPC in patients at risk of amputation who are not candidates for PTA or surgical revascularisation. Results from two controlled before-and-after studies indicate that the treatment may be associated with improved limb salvage, wound healing and pain management, but both of these studies were judged to have a high risk of bias. Insufficient data exists to discriminate between the effectiveness of the different modalities of IPC treatment that are available or to identify the optimal compression parameters to use. Additional well-designed analytical studies examining the effect of IPC are required before this technology can reliably be shown to improve outcomes in this patient group.
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.