
Abstract
Angiolymphoid Hyperplasia with Eosinophilia (ALHE) is a benign vascular proliferative disorder with uncertain etiology and pathogenesis. The aim of this paper is to report a case of ALHE in the temporal artery and discuss the general aspects of this pathology. A 29-year-old female black patient sought the Vascular Surgery Outpatient Service, complaining of bulging in the right temporal region, associated with pain and local discomfort. Physical examination revealed pulsatile bulging in the right temporal region measuring approximately 2.5 × 1.5 cm. Nuclear Magnetic Resonance showed an expansive fusiform lesion in the superficial soft parts of the right temporal region, measuring 2.9 cm in the longest longitudinal axis. Surgical excision proved to be the best therapeutic option for the patient in this case. Histopathological sections showed the proliferation of vessels of different sizes, covered by swollen endothelium, prominent inflammatory infiltrate composed of lymphocytes, plasma cells, eosinophils, and scarce histiocytes. Immunohistochemical analysis of the lesion showed positivity for CD31, corroborating the diagnosis of ALHE.
Introduction
Angiolymphoid Hyperplasia with Eosinophilia (ALHE) is a benign vascular proliferative disorder with uncertain etiology and pathogenesis. 1 First described in 1969 by Wells and Whimster, being called Subcutaneous Angiolymphoid Hyperplasia with Eosinophilia. 2 The actual incidence and prevalence are unknown. It has no sex predilection and affects individuals of all ages, with an incidence peak in the second to fourth decades of life (mean age of 37.6 years), being more reported in Asian and white patients. 3
ALHE usually presents as reddish and/or violet nodules, 4 single or multiple, and may affect different regions of the body, most commonly the ear and periauricular region, face, and scalp. 3 Itching, pain, and bleeding are the most reported symptoms. 3 Among the main etiological hypotheses are neoplastic vascular proliferative process, previous trauma, 5 insect bites, 2 states of hyper-estrogenism, pregnancy and use of combined oral contraceptives (COC),6-8 herpes virus infection 8 and T-cell clonality in some cases, which may correspond to a low-grade lymphoproliferative disorder. 9
Surgical excision of the lesion is the main treatment option and is associated with lower recurrence rates. In ALHE, recurrences typically occur locally, and other therapeutic intervention possibilities include pulsed laser and carbon dioxide, argon laser, intralesional and topical corticosteroids, and cryotherapy, but they show inferior clinical benefit. 10 The spontaneous resolution of the lesion has also been reported in some cases. 3
The aim of this paper is to report a case of ALHE in the temporal artery and discuss the general aspects of this pathology. Written informed consent from the respective patient was obtained, and the study was approved by the Professor Edgard Santos University Hospital Complex ethics committee.
Case Report
A 29-year-old female black patient, born and resident in Salvador of Bahia, Brazil, sought the Vascular Surgery Outpatient Service, complaining of bulging in the right temporal region, associated with pain and local discomfort. The condition had spontaneously emerged 2 years before and the mass growth was progressive.
Physical examination revealed pulsatile bulging in the right temporal region measuring approximately 2.5 × 1.5 cm, with fibroelastic consistency, not adhered to deep tissues, and without local skin changes (Figure 1). There were no palpable regional lymph nodes. The patient denied a history of local trauma or insect bites and reported monthly injectable contraceptive use. No similar family history information. The peripheral blood eosinophil count was normal. A and B: Clinical Examination: Bulging in the right temporal region without local skin change.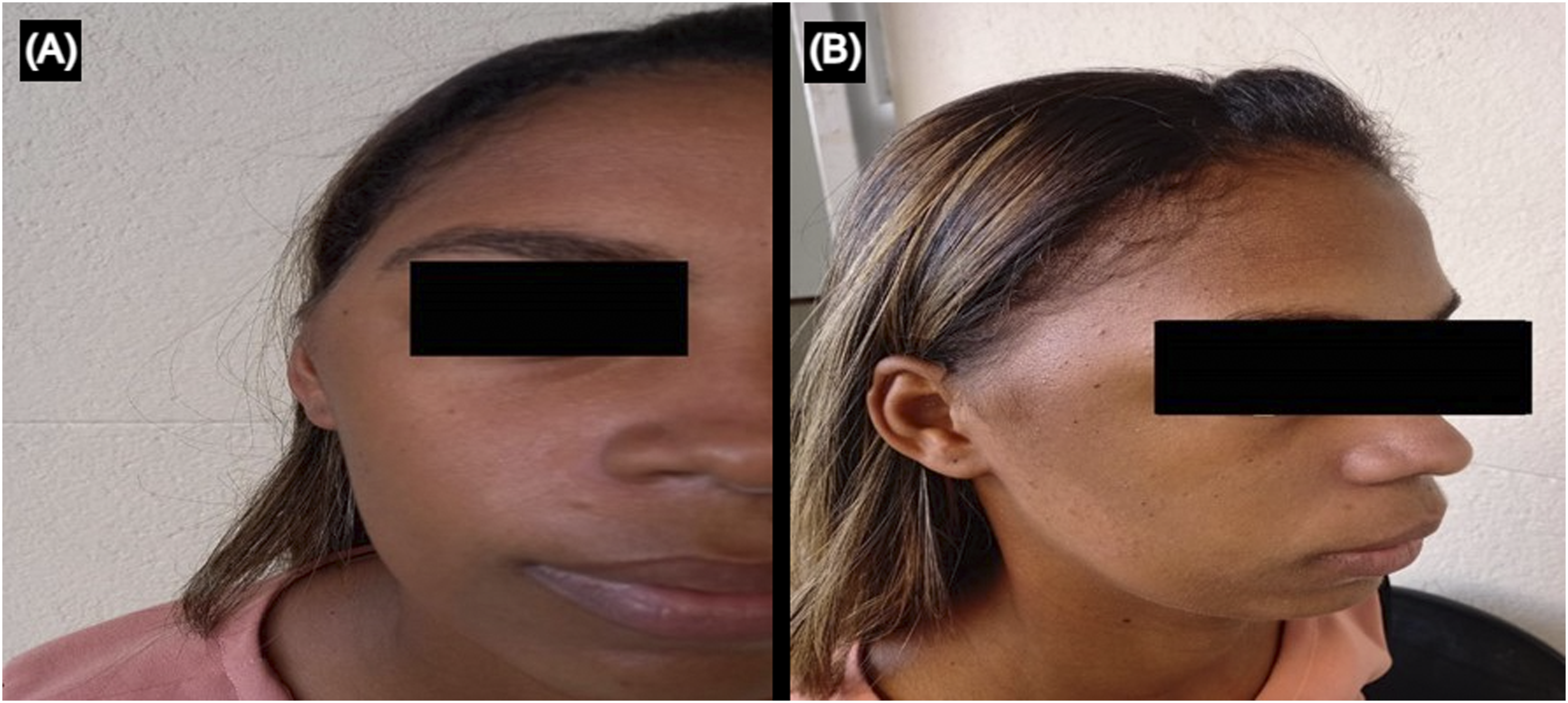
A preoperative ultrasound scan (USS) was performed, suggesting a right temporal artery aneurysm. Nuclear Magnetic Resonance showed an expansive fusiform lesion in the superficial soft parts of the right temporal region, measuring 2.9 cm in the longest longitudinal axis and about 1.7 × 1.3 cm in the longest transversal axes, whose contours were well defined, with emphasis on the temporal artery permeated to the fusiform lesion described. A new USS was performed in the operating room, using a 12 MHz linear transducer (GE Logic, 2016), which showed circumferential thickening of the right superficial temporal artery without changes in the flow pattern seen within the lumen (Figure 2). A and B: Ultrasound examination showing a hypoechoic nodule surrounding the right temporal artery. Note the absence of intranodular flow on color Doppler while normal arterial flow.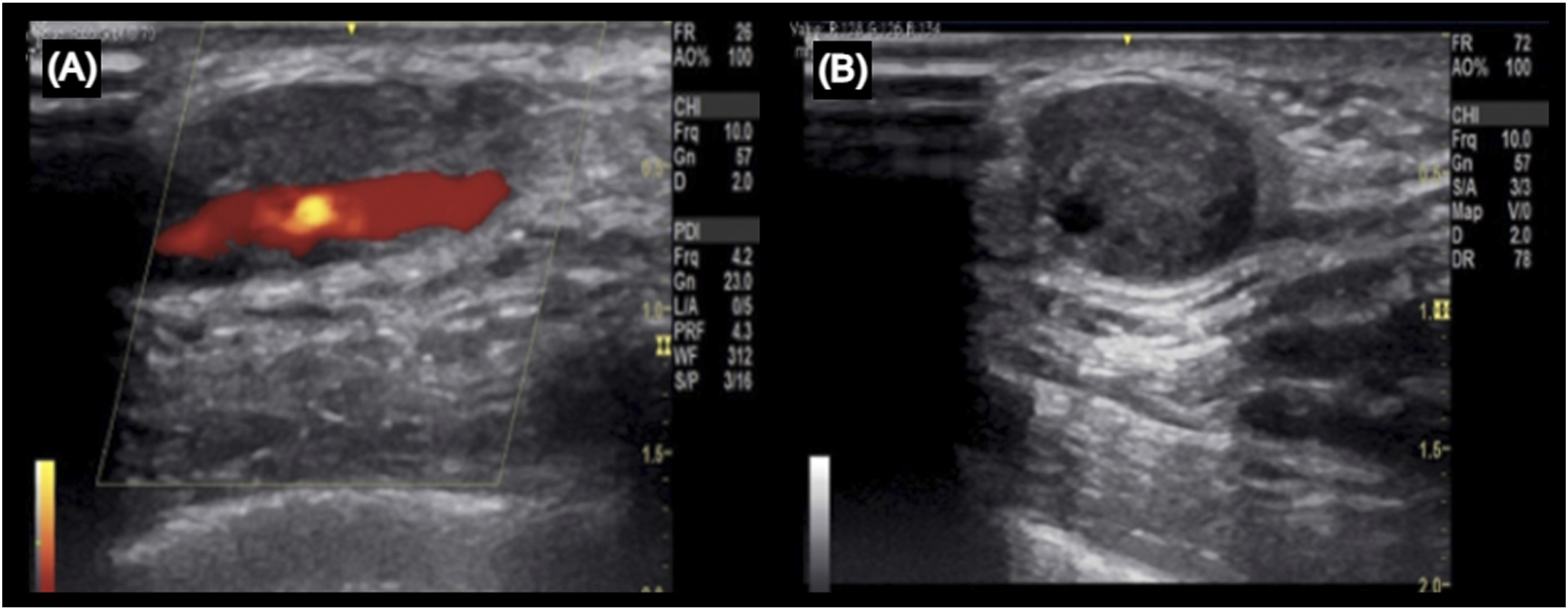
Surgical resection of the affected segment of the right temporal artery was performed under general anesthesia. The biological material was fixed in 10% formalin and sent for pathological anatomy examination (Figure 3). Histopathological sections exhibited an artery fragment showing intimal proliferation. Between the media and adventitial layers, there was a proliferation of vessels of different sizes, covered by swollen endothelium. Mitotic figure was not observed. There was a moderate inflammatory infiltrate composed of lymphocytes, histiocytes, plasma cells, and eosinophils, sometimes differentiating lymphoid aggregates with well-differentiated germinal centers. There was also associated fibrosis (Figures 4A-B). Intraoperative Photos: A and B - Fusiform lesion of the right temporal artery, measuring 2.5 × 1.5 × 1.0 cm; C and D - A whitish-colored lesion in the temporal artery and preserved lumen seen with a Nelaton catheter inside. Histopathological Examination: A, Between the medial layer and the adventitia of the temporal artery, there are vessels of varying sizes, covered by prominent endothelium (asterisk). There is, in association, a mixed inflammatory infiltrate, composed of lymphocytes, plasma cells, histiocytes, and eosinophils (arrow), forming lymphoid aggregates with germinal centers (circle) (H&E); B, Detail, in greater magnification, showing vessels with swollen endothelium (asterisk) and abundant eosinophils (circle) composing the infiltrate (H&E); C, Note, in area, discontinuity of the temporal artery elastic lamina (asterisk), with associated vascular proliferation (Weigert staining); D, Immunohistochemistry showing positivity for CD31 in proliferated vessels.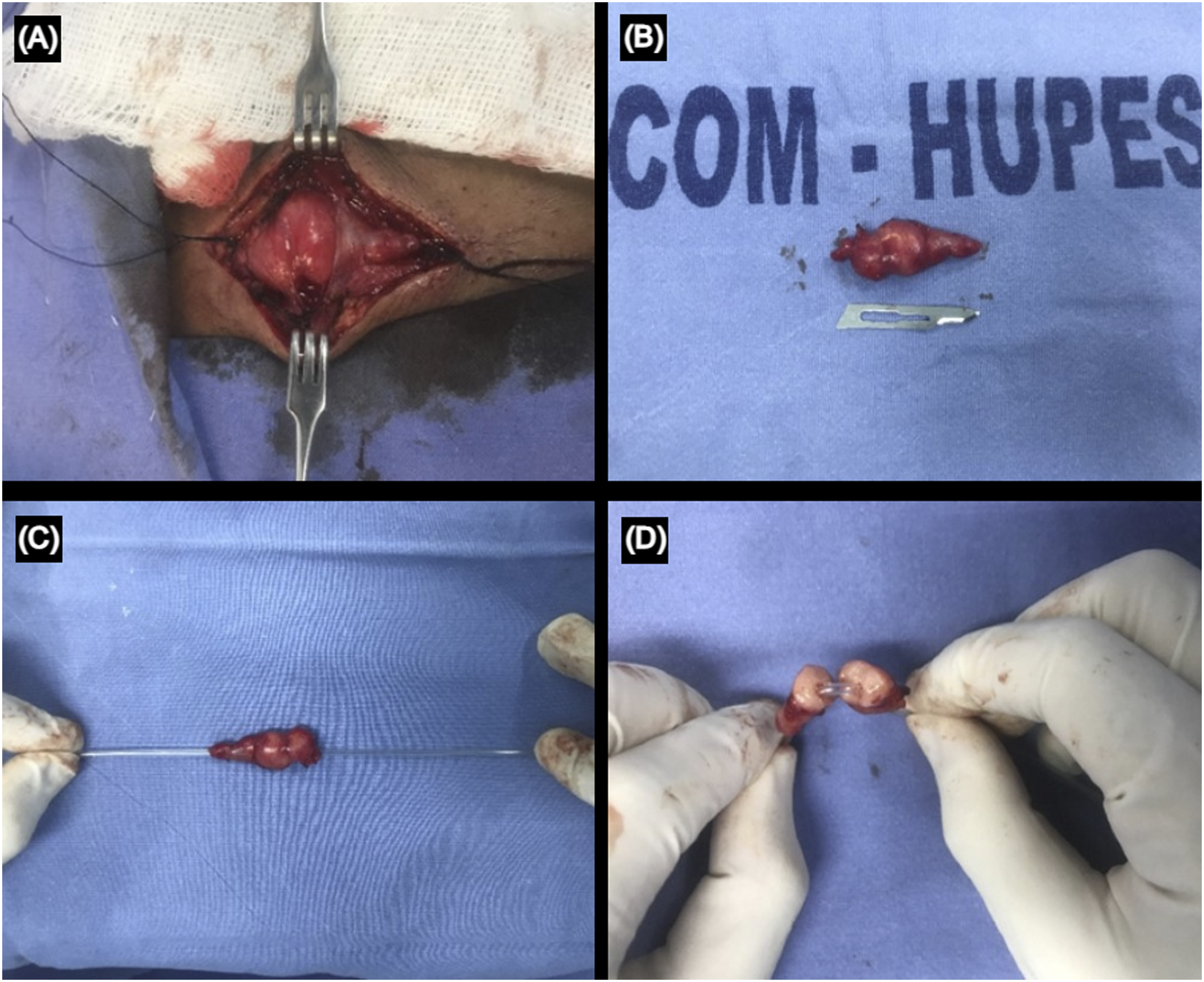
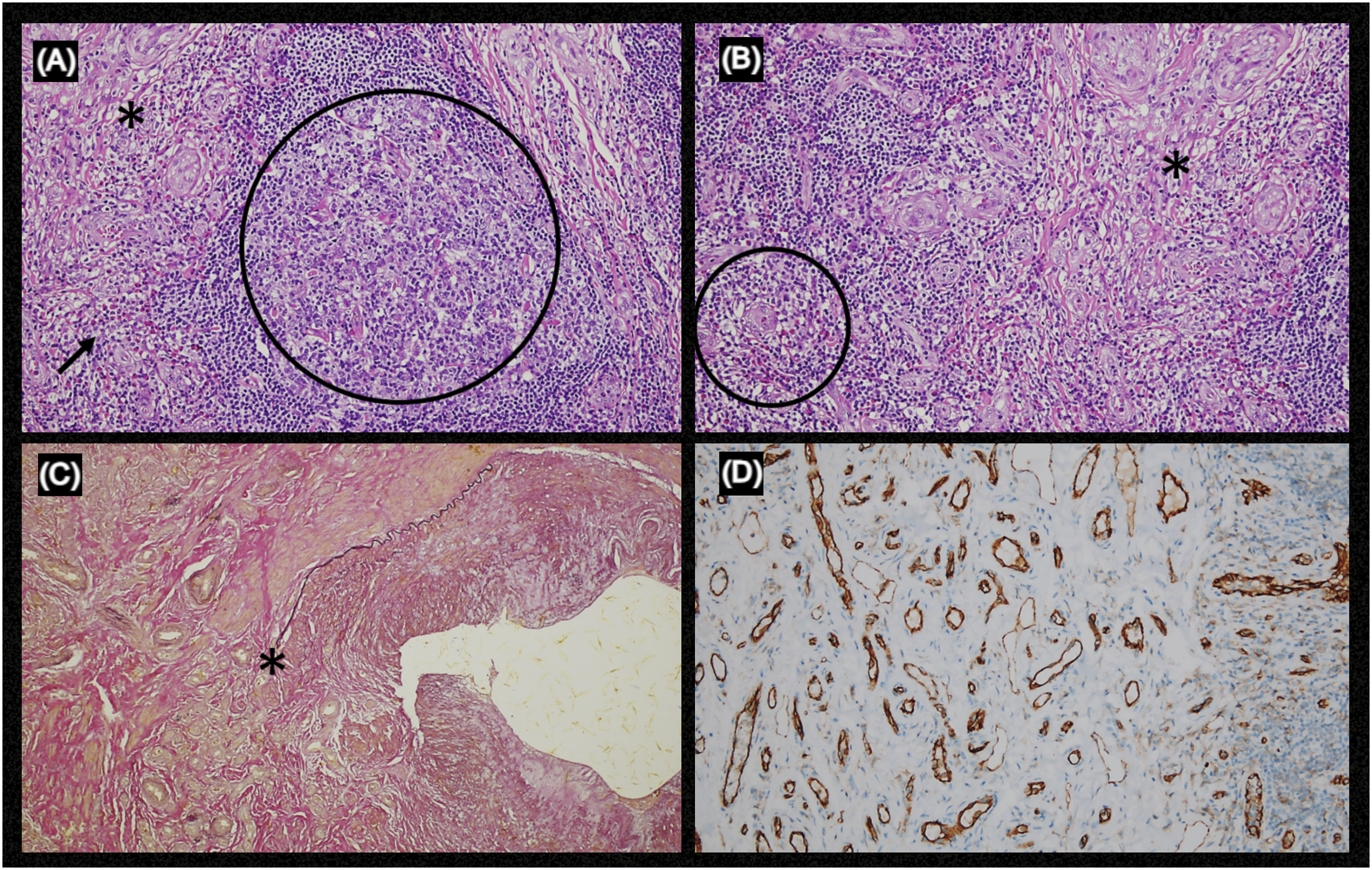
The Weigert special stain showed a rupture of the arterial elastic layer, with associated vascular proliferation. A complementary immunohistochemical study showed positivity for markers of endothelial proliferation: CD31 in proliferated vessels, CD45RO in the associated inflammatory infiltrate (Figures 4C-D), and CD34 and factor VIII were also positive. Such morphological aspects were compatible with the diagnosis of angiolymphoid hyperplasia with eosinophilia.
The patient had a postoperatively uneventful evolution, with the surgical wound showing a good appearance. A final diagnosis of ALHE was established after analyzing clinical and histopathological data. The patient is under clinical follow-up, showing no signs of lesion recurrence after 6 months.
Discussion
Despite the case reports in the literature associating the occurrence of ALHE with previous local trauma and insect bites, the patient denied any of these factors. She reported only monthly injectable contraceptive use. In addition, she did not have a classic presentation of reddish and/or violet nodules and there were no skin changes at the lesion site. Only the complaint of local pain was mentioned, with no report of bleeding, ulcerations, pruritus, mandibular claudication, muscle cramps, or visual symptoms. ALHE has been associated as a possible cause of blood eosinophilia, 11 however, in the case described, the laboratory test did not show such variation.
Among the structures affected by ALHE, alterations in the subcutaneous tissue are more common, however, other small and medium-sized venous or arterial structures may be affected. Proliferation seems to start in the intima layer and may extend into the vascular lumen or through the media layer, generally remaining contained in the adventitia. 12
The choice for surgical resection was initially guided by the suspicion of a temporal artery aneurysm. Despite being a benign lesion, recurrence rates are high, being 40.8% in patients treated surgically and ranging from 50-100% in those treated non-surgically. 3 A comparison between different treatment modalities showed that surgical excision of the lesion is superior to others, including the use of topical corticosteroids, with fewer rates of local recurrences and higher improvement in symptoms. 13 Surgical excision proved to be the best therapeutic option for the patient in this case. As ALHE is a rare disease, there is no specific follow-up protocol for their patients in the literature.
Spontaneous resolution of the lesion is uncommon. Satpathy et al reported the case of an 11-year-old girl, presenting with histopathologically confirmed ALHE on the back of her left hand, which regressed within 10 weeks. 14 Radiological diagnosis of the lesion is not well established. The arterial wall thickening or mass, which can present with fusiform dilation, can lead to a wrong suspicion of an aneurysm. 15 In our report, the preoperative USS described a right temporal artery aneurysm as a possible result, although also being a rare entity. 16
Pathological anatomy is characterized by circumscribed proliferation of vessels with swollen endothelium, which projects into the vascular lumen, with abundant eosinophilic cytoplasm and cubic, cylindrical, or hobnail shape, without evidence of pleomorphism or mitotic activity. In association, there is a prominent inflammatory infiltrate composed of lymphocytes, plasma cells, eosinophils, and scarce histiocytes, sometimes differentiating lymphoid follicles. 17 Such morphological characteristics were observed in the present case. Immunohistochemical analysis of the lesion showed positivity for CD31, CD34, and factor VIII. Although their positivity is not pathognomic for ALHE, the diagnosis was corroborated since they auxiliate in the identification of endothelial proliferation.
Kimura’s Disease is the main differential diagnosis, however some aspects of the histopathological analysis of the lesion help in its differentiation. Kimura’s Disease is a disorder of the lymphoid follicles, with an absence of irregular and dilated blood vessels, non-bulging endothelial cells in the vascular lumen, without vacuoles in the cytoplasm, presence of numerous eosinophils and extension to the muscular fascia and sometimes to the skeletal muscle. ALHE is a disorder of blood vessels, which appear dilated and irregular, endothelial cells enlarged and bulging with one or more vacuoles in the cytoplasm; a number of eosinophils varies from none to numerous and there is no extension to the muscular fascia. 18
Angiolymphoid Hyperplasia with Eosinophilia (ALHE) disease is a rare clinical condition. We report a case of a vascular lesion with an unusual clinical presentation, in order to draw the attention of professionals working in this area to the differential diagnosis of this pathology with other more prevalent vascular lesions.
Footnotes
Acknowledgments
We thank CAPES and the Postgraduate Program in Medicine and Health of the Faculty of Medicine of Bahia, Federal University of Bahia, Salvador, Bahia, Brazil, for their educational support.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was carried out with the support of the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior – Brasil (CAPES) - Brazil - Financing Code 001.