
Abstract
Kimura’s disease (KD) is a rare chronic inflammatory or allergic disease. Angiolymphoid hyperplasia with eosinophilia (ALHE) is a benign vascular neoplasm. Their relationship has always been debated. This article reports two rare cases, one of each disease. One patient was a 48-year-old female that presented with a mass on her right mandible. She also had oedema erythema and wheals on her lower limbs. She was diagnosed with Kimura’s disease complicated with chronic urticaria. The second patient was a 23-year-old female that presented with multiple nodules of unequal size on the scalp. She was diagnosed with angiolymphoid hyperplasia with eosinophilia. The first patient recovered after being treated with surgical resection, glucocorticosteroids, cyclophosphamide and radiotherapy. The second patient underwent the first stage of surgical excision and is currently being followed-up. Comparison of the clinical and histopathological features of these two cases supports the theory that KD and ALHE are two separate disease entities.
Introduction
Kimura’s disease (KD), also called eosinophilic hyperplastic lymphoid granuloma, is a rare chronic inflammatory disorder. 1 Angiolymphoid hyperplasia with eosinophilia (ALHE), also called epithelioid haemangioma, is a rare angioproliferative disease. 2 Their relationship has always been debated. These two conditions were first thought to be different stages of a spectrum in one disease due to some of their similarities. 3 With further understanding, scholars have found many differences between these two diseases and they are now accepted to be two distinct histopathological entities. 4 , 5
This current case report describes two patients, one with KD complicated with chronic urticaria and the other with ALHE. This work clarifies the similarities and differences between these two diseases by comparing their clinical and histopathological features.
Case reports
Case 1
In July 2018, a 48-year-old Chinese female presented to the Department of Dermatology, Huangshi Central Hospital, Affiliated Hospital of Hubei Polytechnic University, Edong Health Care Group, Huangshi, Hubei Province, China with a progressive mass on her right mandible over 3 months, which was accompanied by oedema erythema and wheals mainly on the lower limbs. She had seen dermatologists constantly for her rash but did not notice the mass. She reported no fever, night sweats or weight loss. She had no other medical conditions or respiratory symptoms and was otherwise systemically healthy. Her family had no genetic history. Upon physical examination, a nontender and non-erythematous palpable mass with no clear boundary was found in the right submandibular region (Figure 1a). Several enlarged lymph nodes were also observed in the right neck and supraclavicular areas. Wheals were scattered across the trunk and lower limbs, especially on the lower limbs (Figure 1b).

Clinical features of case 1, a 48-year-old Chinese female that presented with a progressive mass on her right mandible that was accompanied by oedema erythema and wheals mainly on the lower limbs: (a) a palpable mass that was nontender and non-erythematous, was observed in the right submandibular region; (b) wheals were scattered on her lower limbs; (c) enhanced computed tomography imaging of her nasopharynx showed a soft tissue mass (1.9 cm × 1.1 cm) in the lateral part of the right submandibular gland.
An enhanced computed tomography (CT) scan of the nasopharynx showed a soft tissue mass (1.9 cm × 1.1 cm) in the lateral part of the right submandibular gland (Figure 1c). Chest CT imaging revealed small lymph nodes in the supraclavicular area. Abdominal CT imaging showed no abnormalities. Laboratory tests displayed white blood cells (8.23 × 109/l) and eosinophils (2.15 × 109/l, 11.2%, normal range: 0.02–0.52 × 109/l, 0.40–8.00%). Immunoglobulin (Ig)E levels were elevated at 245 IU/ml (normal range <100 IU/ml). Liver and kidney functions were normal. An incisional biopsy of the mass showed preserved lymph node architecture with hyperplastic lymphoid follicles and patchy expansion of germinal centres (Figure 2a). The interfollicular region contained numerous eosinophils and interstitial fibrosis (Figure 2b). Eosinophilic abscess was noted in some areas (Figure 2c). The patient was finally diagnosed with Kimura’s disease with chronic urticaria.

Histopathological features of case 1, a 48-year-old Chinese female that presented with a progressive mass on her right mandible that was accompanied by oedema erythema and wheals mainly on the lower limbs: (a) preserved lymph-node architectures with hyperplastic lymphoid follicles and patchy expansion of germinal centres (haematoxylin and eosin, original magnification × 5); (b) the interfollicular region contained numerous eosinophils and interstitial fibrosis (haematoxylin and eosin, original magnification × 10); (c) eosinophilic abscesses were observed in some areas (haematoxylin and eosin, original magnification × 40). The colour version of this figure is available at: http://imr.sagepub.com.
After surgical resection, the patient underwent four courses of treatment that included the following: 500 mg/day cyclophosphamide intravenously on 1 day, then 100 mg/day prednisone orally for 4 days. The patient then received local radiotherapy (PGTVnd 42.4GY/20F’) for 14 days after 2 days of drug discontinuation. Each course of treatment lasted 21 days. The patient was followed up for 6 months without relapse.
Case 2
In March 2021, a 23-year-old Chinese female presented to the Department of Dermatology, Huangshi Central Hospital with multiple nodules on the scalp for 2 years, without pain and itching. She denied any history of head trauma and had no other medical conditions or relevant genetic history in her family. Upon physical examination, numerous skin coloured nodules measuring approximately 0.5–3 cm (Figure 3a) were found on the occipital area (Figure 3b). No enlarged superficial lymph nodes were observed. Blood count and hepatic and renal function were normal. A biopsy of the lesion showed many irregular hyperplastic vessels with hypertrophic endothelium in the dermis; and endothelial cells protruded into the lumen and assumed a spiked appearance (Figure 4a). The vessels were surrounded by a density of lymphocytes and a small number of eosinophils (Figure 4b). The patient was diagnosed with ALHE. Owing to the presence of numerous lesions, staged surgical excision of the lesions was recommended. The patient has already undergone the first stage of excision and will receive the second stage of excision after 3 months. She is now being followed-up.

Clinical features of case 2, a 23-year-old Chinese female that presented with multiple nodules on the scalp without pain and itching: (a) there were numerous skin coloured nodules on the occipital area; (b) some of the nodules were approximately the size of a cherry.

Histopathological features of case 2, a 23-year-old Chinese female that presented with multiple nodules on the scalp without pain and itching: (a) many irregular hyperplastic vessels with hypertrophic endothelium in the dermis. Endothelial cells were protruding into the lumen assuming a spiked appearance (haematoxylin and eosin, original magnification × 100); (b) the vessels were surrounded by a density of lymphocytes and a small number of eosinophils (haematoxylin and eosin, original magnification × 400). The colour version of this figure is available at: http://imr.sagepub.com.
This report was approved by the Ethics Committee of Huangshi Central Hospital, Edong Health Care Group (V1.0.2021.03.15). Specific information on the patients was completely de-identified in the manuscript. Written informed consent was obtained from the patients for the publication of this report. The reporting of these two case reports follows the CARE guidelines. 6
Discussion
Kimura’s disease was first described by Kimura and Sceto in China in 1937 and was later studied by Kimura and Ishikawa in 1948. 7 Since then, the disease has become widely known as Kimura’s disease. ALHE was first described in 1969, when it was thought that the two diseases represented different stages of the same disease spectrum; with KD being the late stage of ALHE. 3 In 1987, KD and ALHE were found to differ in terms of histopathological features. 4 Many scholars subsequently supported this view.5,8,9 Currently, KD is considered to be a rare chronic inflammatory or allergic disease and ALHE is thought to be a benign vascular neoplasm. 8
Kimura’s disease is an inflammatory disorder of unknown aetiology that most commonly presents as painless lymphadenopathy or subcutaneous masses in the head and neck region. 10 Patients are typically males of Asian descent in their 30s and the sex ratio is 4–7:1. 11 In the clinical setting, one or multiple painless deep hypodermic subcutaneous nodules are usually observed, mostly in the head and neck and mainly in the subcutaneous tissues, salivary glands or cervical lymph nodes. 12 Associated lymphadenopathy has been reported in 42–100% of cases. 13 Blood analysis shows hypereosinophilia and total immunoglobulin E elevation. 11 The most important pathological feature of KD is hyperplastic follicles with germinal centres surrounded by abundant eosinophilic infiltrations.1,13 Standard treatment for KD is currently not available. The main therapeutic methods are surgical resection, glucocorticoid therapy, cytotoxic therapy and radiotherapy.1,7 Owing to its frequent recurrence, comprehensive treatment is often required.1,14
Angiolymphoid hyperplasia with eosinophilia is a rare benign vasoproliferative disease of uncertain pathogenesis that frequently presents with single or multiple dermal papules or nodules on the head and neck. 15 A high incidence has been reported in female patients aged 30–50 years. 16 The histopathology of ALHE shows prominent vascular proliferation, enlarged endothelial cells that are cuboidal to dome-shaped, and sparse to heavy lymphocytic infiltrates with eosinophils. 17 The treatment of choice for ALHE is surgical excision, although relapse is common. 17 Other types of procedures, such as cryotherapy, 18 pulsed dye laser, 19 and carbon dioxide laser, 20 have been reported. Medical treatments include corticosteroids, topical imiquimod, tacrolimus and isotretinoin. 17
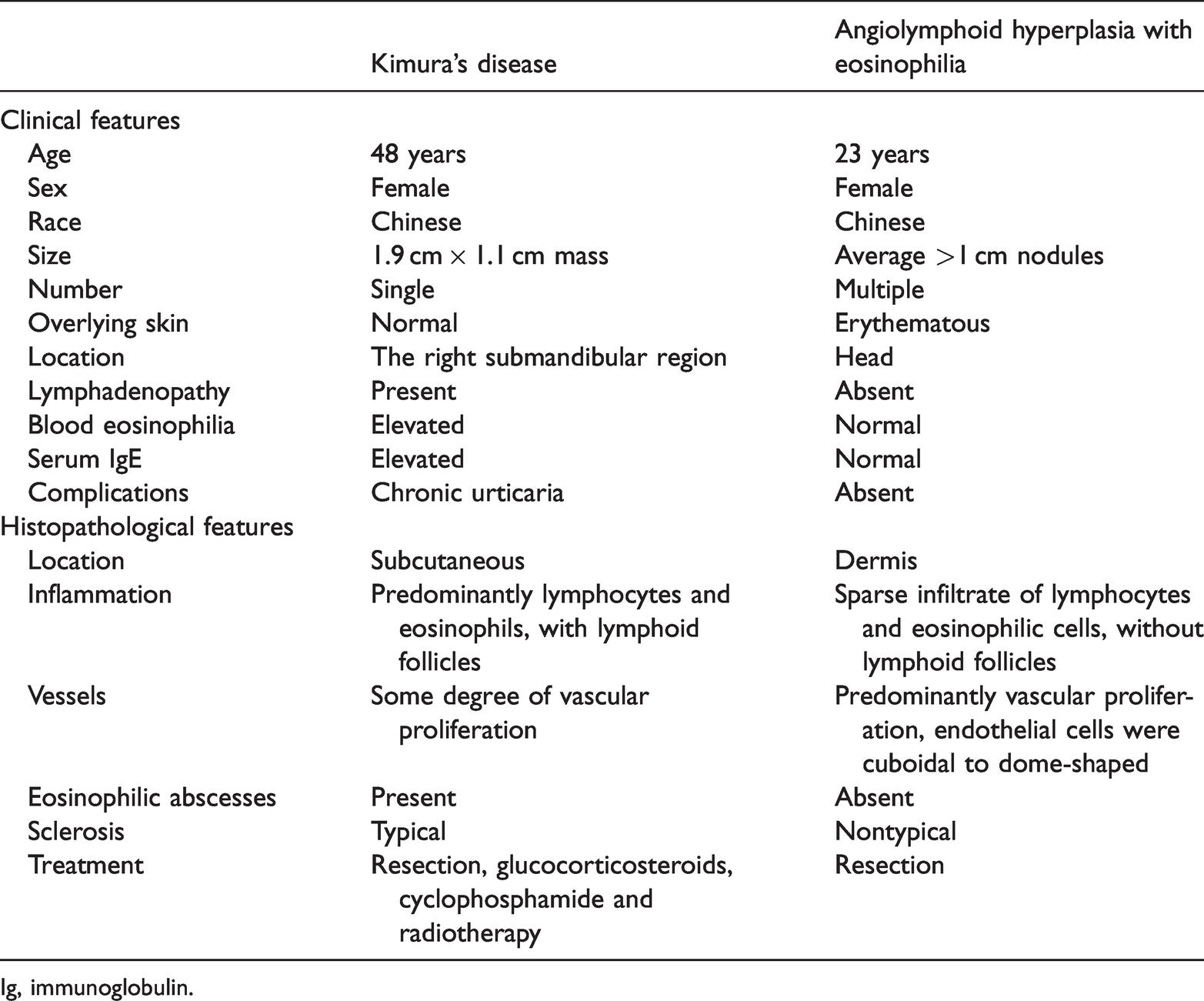
The clinical and histopathological features of KD and ALHE have been widely compared and the results are presented in Table 1.5,8,9 A comparison between KD and ALHE for the two patients in this work are summarized in Table 2. Many differences in the clinical and histopathological features are noted between KD and ALHE.
A comparison of the clinical and histopathological features of Kimura’s disease and angiolymphoid hyperplasia with eosinophilia.

Ig, immunoglobulin.
A comparison between Kimura’s disease and angiolymphoid hyperplasia with eosinophilia in the two patients described in this case report.
Ig, immunoglobulin.
In the present two cases, some distinctions from previously reported characteristics were noted. Case 1 with KD was a female aged 48 years, which is beyond the typical age range of 20–30 years. 11 More interestingly, she had a complication of chronic urticaria. To date, no reports have been published about KD complicated with chronic urticaria. This finding may also serve as evidence that Kimura’s disease is a chronic inflammatory or allergic disease. Case 2 with ALHE was a female aged 23 years, which is younger than the typical age range of 30–50 years. 16 More than 50 nodules measuring approximately 0.5–3 cm were observed. This result adds further evidence that ALHE is a benign neoplasm.
In conclusion, comparison of the clinical and histopathological features between KD and ALHE demonstrated their broad differences. Thus, this work supports the opinion that KD and ALHE are two separate disease entities.
Footnotes
Author contributions
Ailing Zou: approval of the final version of the manuscript; drafting and editing of the manuscript; collection of data; critical review of the literature; Mengyao Hu: approval of the final version of the manuscript; collection of data; critical review of the literature; critical review of the manuscript; Bin Niu: approval of the final version of the manuscript; drafting and editing of the manuscript; intellectual participation in propaedeutic and/or therapeutic conduct of the cases studied; critical review of the manuscript.
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.