
Abstract
Members of socially marginalized communities have always suffered the most acute effects of natural disasters, and they have also been the slowest to recover. Thus, it is not surprising that the COVID-19 pandemic appears to be following a similar trajectory. This article details race disparities, social status and place, and their independent and combined effects on Americans' social and emotional health as COVID-19 infection rates began to accelerate across the country.

We are witnessing a watershed moment in the social health history of the United States as we find ourselves in the middle of a worldwide COVID-19 pandemic. For many, anxiety and fear have become a “new normal”—pervasive, persistent, and pernicious. In turn, the country’s collective emotional well-being is threatened. By the time we get the “all clear,” the impact of this public health crisis will have substantially affected the economic, political, cultural, and social foundations of American society. How Americans collectively think— and talk—about the pandemic and its effects will likely reflect the inequities of the pandemic’s social, health, and economic repercussions in much the same way as it has for natural disasters (e.g., hurricanes Katrina, Ike, Harvey, and Maria) and the more recent 2009-2010 H1N1 pandemic.
These themes are already taking shape in our national conversation. News stories, preliminary research, op-eds, and countless other accounts describe a nation divided over policies meant to mitigate the virus’s spread, the accessibility of testing, the economic impact of the pandemic, and the necessity of building resilience for future outbreaks. How we respond and who has greater access is not only the result of a complex intersection of social vulnerabilities, but spatial ones, as well.
Inequalities of People, Places, and Spaces
Residents of socially marginalized communities have always suffered the most acute effects during times of widespread crisis. They have also been the slowest to recover. Therefore, it is not surprising that the COVID-19 pandemic appears to be following a similar trajectory to the natural disaster scenario. News accounts are providing us with grim reminders of just how significant health disparities are in the U.S. Eighty percent of hospitalizations and seventy percent of all COVID-19 related deaths in Louisiana have occurred among African Americans living in low-income and marginalized communities, while communities of color throughout New York City reported higher rates of coronavirus infection and mortality during the height of the virus’s spread, particularly in those neighborhoods with lower incomes. Across rural America, COVID-19 has ravaged Hispanic and Latino communities, particularly those associated with the ranching and meatpacking industries. More broadly, the Centers for Disease Control and Prevention reported in the early summer of 2020 that while African Americans and Latinos comprise smaller proportions of the overall population than non-Hispanic Whites, they accounted for a disproportionate share of confirmed COVID-19 cases, hospitalizations, and deaths nationwide. Thus, the current COVID-19 pandemic brings to the forefront long-standing health disparities and vulnerabilities in the United States.
Our research is a response to this widespread inequality, but with a particular interest in examining the social-psychological and behavioral aspects of the COVID-19 pandemic as it played out in the United States in March 2020. In particular, we turn the spotlight on the intersection of social status and place, and their independent and combined effects on Americans’ social and emotional health as COVID-19 infection rates accelerated across the country. Much of this continues to remind us of the ugly underside of American communities where health care access is unequal, chronic illness is disproportionate, and health disparities look more like 1st world versus 3rd world than suburban versus urban.
Questions to Answer
How worried are we, and is fear distributed uniformly across social groups and communities throughout the United States? How does our level of exposure to immediate or nearby COVID-19 cases or deaths impact our current level of fear? In turn, how is fear or perceived threat related to maladaptive social and physical behaviors? These are the types of questions guiding our work. We draw on data from a nationally representative, post-strata weighted sample of 10,368 adults living in U.S. counties as part of an online survey that was distributed during the week of March 23, 2020. In it, we asked a series of questions aimed at better understanding the intersectionality of individuals, place, fear, and a variety of social, behavioral, and mental health outcomes in the context of the COVID-19 pandemic.
One of the most impactful aspects of this study is that we have been able to take stock of popular and political anecdotes early in the coronavirus pandemic related to fear, worry, and concern and examine the empirical validity—and breadth—of not only those sentiments, but the subsequent social behaviors that follow as they also impact specific locations across the nation. In particular, we find levels of fear, depression, suicide ideation, and food insecurity to be elevated across the nation, but especially so in some places among some individuals. As we elaborate below, individual, community, and spatial vulnerabilities have shaped—and will continue to do so—behaviors during every stage of the pandemic.
Of course, addressing these intersections matters for public health practitioners, as well as the communities they serve, because perceptions of threat, feelings of fear, mental health symptoms, and food access all condition how individuals and their communities respond to the virus’s spread. For example, we know the adoption of personal mitigation strategies (e.g. hand washing, physical distancing, mask wearing) and novel coronavirus policies (e.g. lockdown orders, select closures of schools and religious institutions) are predicated on some level of personal and communal assessment of risk. Thus, understanding fear, threat, and other “downstream” social problems through both an individual and community or spatial lens sheds light on the kinds of unequal impact that we have already observed as the pandemic unfolds.
Individual Fear and Threat Amidst COVID-19
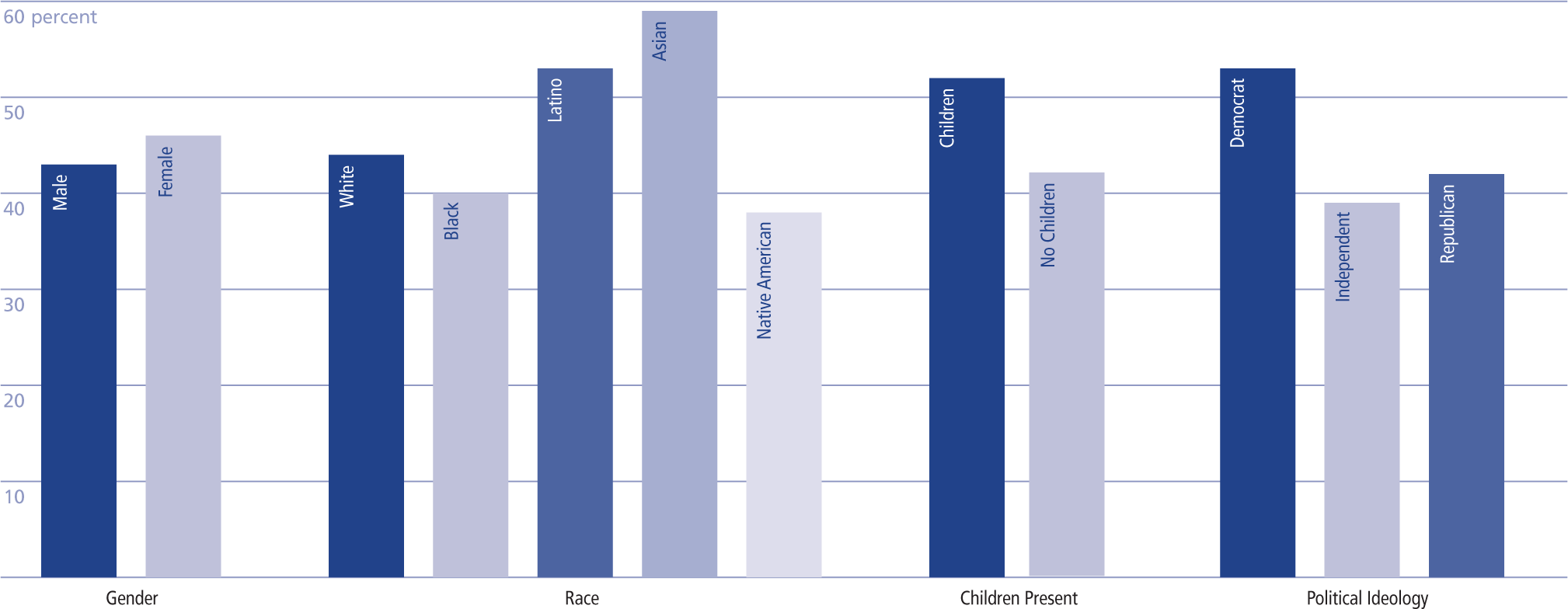
In the chart on the next page, we illustrate some of the most important disparities, specifically the mean percentage of respondents across social groupings that are “very” or “extremely” worried about themselves or their family getting infected with COVID-19. As is clear from the figure, females, Latinos and Asians, respondents with children, and self-described Democrats express more concern or perceive more threat from coronavirus compared to their counterparts. Notably, Blacks and Native Americans express less fear and threat, despite the early and profound impact of the virus on their communities. This disparity might reflect structurally produced inequalities with regards to how certain people access information, particularly early on in the pandemic. This could yield both disproportionately high infections and relatively low fear. Despite widespread warnings and words of caution during the early stages of the coronavirus pandemic, not all communities and socio-demographic groups express fear and/or concern in the same manner.
Additionally, more comprehensive models utilizing our survey data reveal important differences in the ways that fear and worry impact mental health outcomes, even in light of disparities in social and psychological resources that are available to people during the COVID-19 health crisis. Indeed, some groups tend to have less robust social resources, less optimism, a lower sense of connectedness to their community, fewer social ties, imited social support, and a lack of access to food. Yet, fear is itself positively associated with increased levels of depression, anxiety, and suicide ideation, net of these resources and other social vulnerabilities. In short, the disparities in fear, illustrated in Percentage that are “very” or “extremely” worried they/family will get infected with COVID-19, manifest themselves as greater risks for some individuals to experience social or psychological problems amidst the pandemic. Moreover, our data show that some of the psychological fallout of fear undermines other aspects of well-being, including food insecurity. Those who are more fearful may be avoiding food stores or other face-to-face means of food acquisition (e.g. food banks, other emergency food provision services, and even restaurants) that they might utilize if they had less fear of the virus itself. Given the already limited means of food acquisition open to a large proportion of individuals across the U.S., fear may be undermining an already tenuous food situation, particularly for the most socially vulnerable.
The Social Geography of COVID-19 Fear
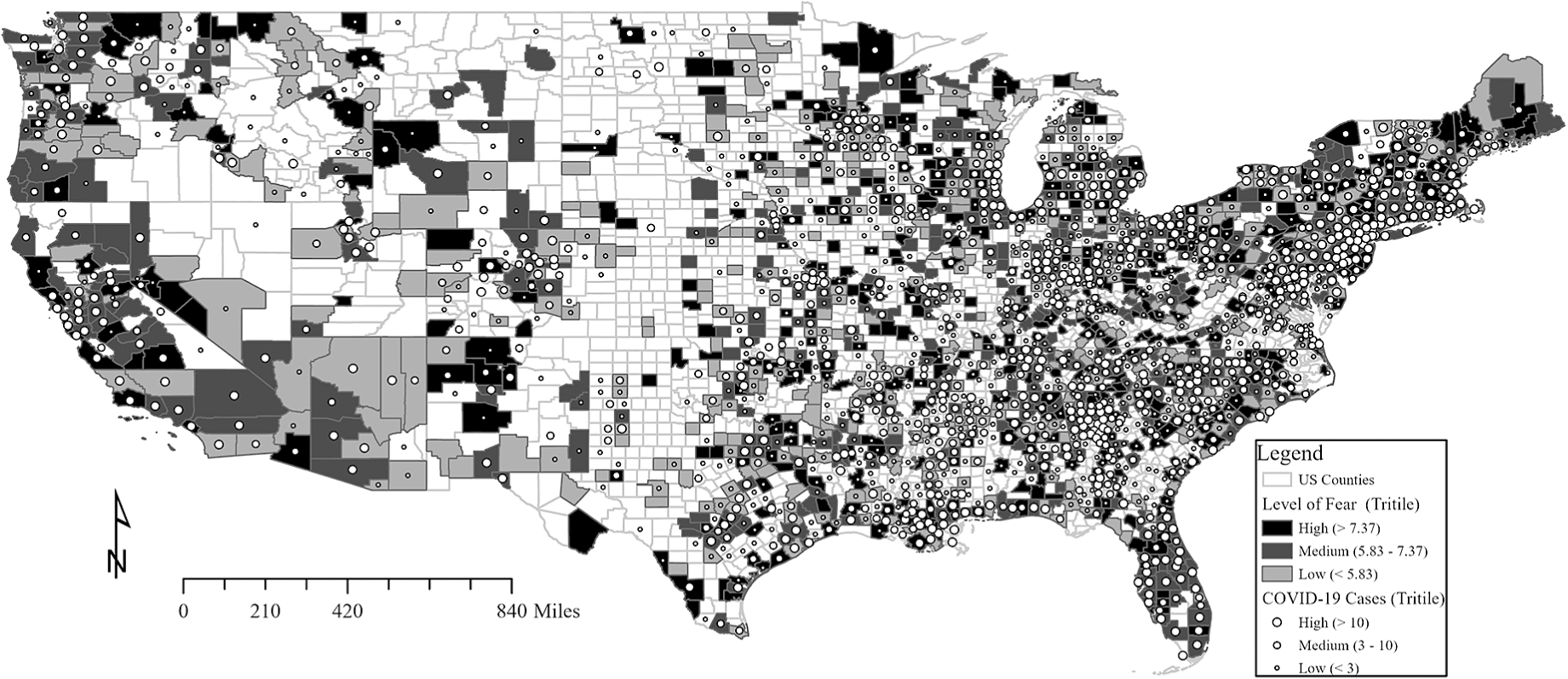
Another part of the pandemic story is the disparity across geographic space for each of these social outcomes, as well. As an example, the map on the next page highlights how fear is unequally distributed across communities. Fear tends to cluster around specific locations, notably those places that have high virus incidence and greater social and economic vulnerability. How this translates into individual and community well-being is an important part of our ongoing work. For instance, we find that the spatial distribution of coronavirus cases and deaths, as well as healthcare infrastructure and community rates of poverty in their own communities, coincide with individual vulnerabilities and fear as they impact respondents’ mental health symptomology.
Percentage that are “very” or “extremely” worried they/family will get infected with COVID-19
Sadly, this public health crisis has already stretched through the summer and now into the fall. More than 8 million confirmed cases have been tallied and more than 225,000 deaths recorded as of late October 2020 according to the Johns Hopkins University COVID case tracking website. What we know will change drastically over the coming months as sociologists, psychologists, and public health practitioners continue to untangle the near-term impact and long-term fallout of this pandemic. Right now, we know that fear remains heightened, and its impact on the generalized anxiety, depressive symptoms, food insecurity, protective health behaviors, and economic actions (e.g. panic buying) among adults living in the United States remains significant. However, a public health crisis of this magnitude will likely have long-lasting effects that our country and its residents will be feeling for years to come.
Recovery from disasters is a slow, arduous process—it is a marathon, not a sprint. Our social, economic, and political infrastructure will need time to fully re-engage and reformat. The consequences of COVID-19 spreading will be felt unevenly, just as recovery will leap forward for some communities while improving only incrementally for others. Our individual recovery will depend greatly on who we are, where we live, how vulnerable we are to the aftershocks of a disaster like this, and the resiliency of the communities where we live and are surrounded by. Not unlike a natural disaster, where we find ourselves during this pandemic requires a whole new set of plans and strategies. What we need is a complete and thorough analysis of social, medical/health, legal and political institutions and the role they have played during public health crises like the one that we are currently experiencing. If we know anything, it is that this pandemic has revealed critical structural weaknesses and inequities system-wide, and going back to the way things were will likely accomplish very little.
Many individuals have been cut off from their normal routines and workplaces. The same has been true of many—if not most— social scientists. However, unlike many in our nation, sociologists know that the COVID-19 pandemic will further entrench key inequalities that have long plagued our society. Our own data illustrate this: threat and fear, mental health problems, and food insecurity are more pronounced for some individuals and communities than others. Social resources are unequally distributed. In turn, social behaviors directly related to the virus vary across demographic groups and geographic space. Not surprisingly, the pandemic has touched some individuals and communities more than others.
Our task will be to systematically examine the mechanisms by which socio-emotional manifestations of fear, concern, worry, and their attending social behaviors come to define the boundaries of those inequalities. Like our own project, others will need to ask, seek out, and describe the spatial, temporal, and social patterns relating to how individuals of different backgrounds respond to this crisis, both during and after. We will need to ask how the complicated intersections of race, age, gender, social class, and community context impact the mental and physical health of individuals, as well as the health and stability of the communities where they live. While a daunting task, exploring these questions will make all of us—and especially the most vulnerable—better prepared to respond to the next crisis.
Post-COVID-19 Society
Fear and perceived threat related to COVID-19—as well as the consequences that follow it—is, of course, only the tip of the sociological iceberg. Our roles as scientists will be critical in the coming months and years. A host of questions will need to be answered through a variety of methodological approaches and study designs. As demographers and community-oriented scholars, we might ask: how quickly will communities “bounce back” from the health and economic fallout from the pandemic, which ones will recover more quickly, and why? Leveraging intersectional perspectives, we might consider what the gender, racial, ethnic, and class disparities look like in terms of recovery. For educational sociologists, we need to be thinking about how school district policies related to COVID-19 affect the learning of all students, but particularly those representing under-resourced or disadvantaged groups. Likewise, as criminologists, we might ask: how has crime changed amidst the unfolding COVID-19 pandemic and, in turn, how have criminal justice actors changed their behaviors to post-COVID-19?
County-level average level of fear and confirmed COVID-19 cases within each county through March 26
Critically, like our own study, addressing such questions will entail taking a hard look at individuals and the social and geographic contexts in which they live. Our study marks an early look at the social and spatial cleavages across which the current public health crisis has played out, including how individuals perceive the threat of the virus and the psychological and social consequences of that fear amidst differences in individual, contextual, and spatial vulnerabilities. Such an early look demonstrates the potential importance of access to information, fear, and infection rates early in the pandemic for the trajectories that those individuals and communities have taken (and which are beyond the scope of the current remarks to address).
Much has changed since late March when our survey was administered; many of those groups and communities in our data that expressed little fear in mid-to-late March have now experienced surges of new cases, hospitalizations, and deaths. Clearly, we have a long battle ahead of us to not only manage the spread of the virus in order to fully understand the social, psychological, and economic fallout of the pandemic and its recovery across communities throughout the nation. Unfortunately, that fallout will likely be another story of individual and contextual inequality where yet another chapter of injustice, discrimination, and unfairness will be written in the U.S. narrative.
Data Availability
Data pertaining to this publication will be available with all identifiers removed after the three-year period of sequestered data based on the author’s agreement with the National Science Foundation. Data will be made available in SPSS and STATA format. In addition to the individual level survey data, all publications, research briefs, and Infographics will reside on the Community and Family Institute website for reference and citation use: cfi.uark.edu.