
Abstract
Privilege, distrust, individual choice, and parental care all factor into vaccine resistance, but the consequences are anything but personal.

There are about a hundred women and a few men, virtually all White and seemingly all between their late-20s and mid-40s, in this suburban hotel ballroom. In the back, a small group of women stands wearing babies on their chests. Others sit on the floor as their babies roll on blankets. Throughout the day I have listened to talks about macrobiotic diets and alternatives to medical treatment for children, I have browsed the expo hall of vendors selling organic foods and homemade lotions. At lunch, I sat next to women eating vegan, gluten-free, or raw-only meals as they traded health tips, recipes, and stories of organic cooking classes for their children. All of these parents expressed a desire to optimize their children’s health and a willingness to work hard to do so.
Barbara Loe Fisher takes the podium as the highly anticipated final keynote speaker. Several women rise to their feet at her introduction. Although this organization explicitly supports “holistic parenting” and “green living” and does not officially oppose vaccines, they have identified points of intersection with the National Vaccine Information Center (NVIC), the largest American organization opposed to vaccine mandates and Fisher, its founder.
Fisher stands in silence as a slide show of smiling babies and occasional White teenage girls fades in and out behind the podium, accompanied by a recording of simple piano music. Interspersed are pictures of women with picket signs emblazoned with pictures of babies. “Dead from DPT” reads one. One Black baby’s photo appears among the sea of White babies. A slide reads simply, “All these children died after vaccination.” Then, “Protecting health and informed consent since 1982. – NVIC.”
I’ve heard a version of Fisher’s talk multiple times over my decade of research on parents who refuse some or all recommended childhood vaccines. She speaks about motherhood—how we love these children in ways we never thought we could and how many of their children had their lives disrupted by legally required vaccines. Fisher tells her signature story—how her now-adult son was harmed at the age of 2½ by the vaccine against diphtheria, pertussis, and tetanus (DPT), how she didn’t know to question vaccines or the doctors who told her they were safe.
Fisher is passionate and clear: “It’s your health, your family, your choice.” She weaves motherhood and love for babies together with critiques of science, pharmaceuticals, and genetically modified foods. She returns to mothers’ intuition and references the Brave New World in which we find ourselves. “There is no individual liberty more important than biological integrity,” she emphatically states. “And there is no limit to what states can take away.”
More than an hour later, she wraps up with a call to action. “As women, mothers, grandmothers. We need to take a stand for vaccine liberty so our children and grandchildren can make choices tomorrow. No forced vaccination. Not in America!”
“As women, mothers, grandmothers. We need to take a stand for vaccine liberty so our children and grandchildren can make choices tomorrow. No forced vaccination. Not in America!” BARBARA LOE FISHER
Barbara Loe Fisher spearheaded the largest national campaign against vaccine mandates, first in 1982 as a group calling itself DPT—Dissatisfied Parents Together—in a critique of the vaccine she believes harmed her son and later as NVIC. NVIC defines itself not as anti-vaccine, but as a group fighting for informed consent and parents’ rights and against government overreach. This organization and several like it oppose efforts to increase vaccination, including expansion of mandates that children provide proof of immunization to register for school, limitations on parents’ abilities to opt out of those requirements, increased funding for vaccines, and requirements that parents receive educational information in support of vaccines.
Over the last decade, I have studied how parents come to refuse some or all recommended vaccines for their children. I attended meetings of groups like the one described above, talked to parents, pediatricians, researchers, attorneys, and policy makers, and observed conversations about vaccines in communities, online, at children’s hospitals and professional meetings, and among parents. Although I spoke with mothers and fathers, women are most likely to make healthcare decisions for their children, and thus, are most likely to make vaccine decisions. These mothers draw from a wide range of sources of information including popular news sources, peers, and media. The mothers in my study overwhelmingly define their efforts to gather information to feel informed as essential to making good decisions for their children. As one mother of two unvaccinated children advises, “Do as much reading and research [as you can] and then make an individual decision. I don’t think that our experience is ever gonna be the same as somebody else’s experience.”
Dr. Partha Sarathi Sahana, Flickr CC
Making personal decisions as parents—free from coercion— is their stated priority. As individuals who express skepticism of expert recommendations, they comprise a collective effort to resist governmental efforts to increase vaccination usage. They work together against public health claims for vaccines by insisting vaccines should always be a personal choice, administered as parents feel is best for their own children. Yet, their insistence that vaccines should follow personal preference rather than community obligation may ignore the fact that infectious disease can only be kept at bay by collective participation in public health.
Resisters’ insistence that vaccines should reflect personal preference rather than community obligation may ignore the fact that infectious disease can only be kept at bay by collective participation in public health.
One veteran’s vaccination records.
Bill Smith, Flickr CC
Privilege and Choice
There are no mandates to vaccinate children in the U.S. and no federal laws requiring vaccination. Rather, families who wish to enroll their children in schools or childcare settings must show evidence that their children have received specific vaccinations. These state laws, passed between the 1960s and 1980s, were intended to reduce risk of infection that results when children—required by law to receive an education—are in close quarters. By requiring vaccines, states also received federal funding to make vaccines accessible to everyone, at every income level. At the time, none of this was particularly controversial. Polls from this time period suggest that many Americans—as many as 25%—did not know their state had a compulsory vaccine law; most said they planned to have their children vaccinated anyway. Even so, laws seem to matter. States with stricter vaccine laws have higher rates of vaccination and fewer outbreaks of vaccine-preventable diseases than do states with more lenient laws or greater access to exemptions.
States with stricter vaccine laws have higher rates of vaccination and fewer outbreaks of vaccine-preventable diseases than do states with more lenient laws or greater access to exemptions.
All 50 states now require evidence of vaccination for school attendance, with opt-out exceptions for children with medical conditions that make them poor candidates for vaccination. All but three states (Mississippi, West Virginia, and, as of 2016, California) allow parents who hold religious beliefs that would be violated by compulsory vaccination to exercise an exemption. The result of lobbying efforts by Christian Scientists, these exemptions are often broadly written. They are inclusive of other faiths and appear to be used by those without strong faith beliefs or religious membership, too. Today, 18 states also allow parents to opt out of vaccines for personal or philosophical beliefs. The use of these non-medical exemptions has become increasingly controversial; vaccine refusals are associated with increased disease outbreaks.
Non-medical exemptions are not used equally by all families. According to national data, parents who refuse vaccines by choice are most likely to be White, college-educated, and have a higher average income than most American families. This contrasts with families whose children are under-vaccinated because of limited or inconsistent access to healthcare providers or lack of economic resources. Those children are most likely to be Black, to have a younger mother who is single and does not have a college degree, and to live in a household near the poverty level. Increasingly, children in rural communities are also limited in their abilities to get vaccines because of supply and distribution challenges. Certainly, there are families of color and low income families who distrust vaccines or don’t seek them out for ideological reasons, but public opinion polls show that low income families express greater support for legal mandates than do those families with more resources.
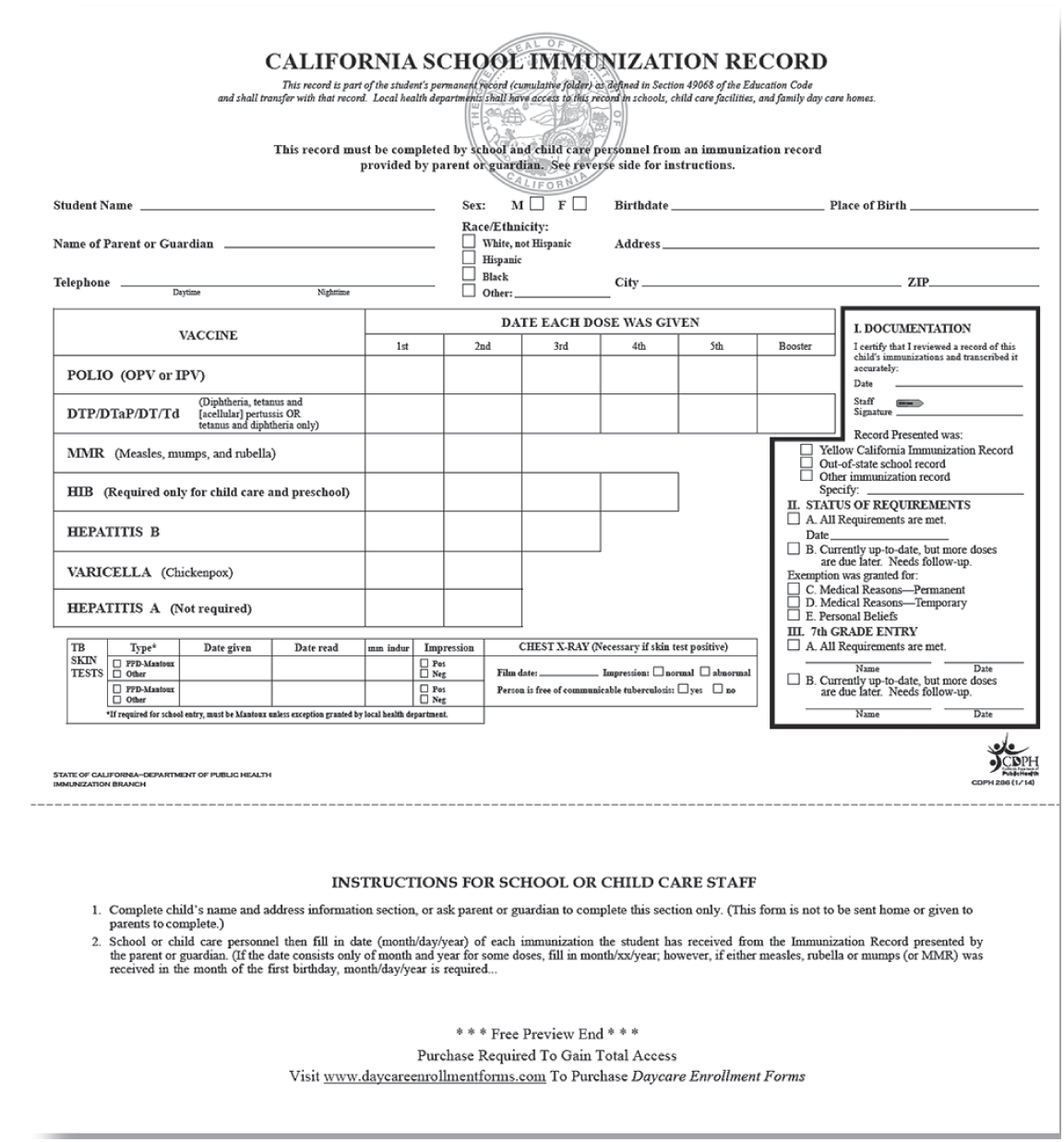
California’s daycare enrollment immunization schedule in 2017.
Public Domain
Although children in communities with low vaccine rates have as much as a 30-fold increased risk of contracting a vaccine-preventable disease, other risks may impact families differently. Unvaccinated children exposed to infection may face a state-enforced quarantine for up to three weeks, even if they never get sick, which families with less work flexibility may struggle to manage. Several proposals to increase insurance premiums for unvaccinated enrollees and state and federal rules that allow public assistance benefits to be reduced because of incomplete vaccination all highlight how low-income families have less freedom to make individual choices without serious repercussions. Some low-income families who want vaccines struggle to get them, which also forecloses choice.
A Movement of Individualists
Parents who question the safety and necessity of vaccines and opt out of some or all vaccines for their children encourage others to do the same, insisting that parents, not doctors or researchers, are best able to decide what children need. Many also advocate against state laws that aim to strengthen vaccine access or requirements. Yet, these parents generally do not see themselves as part of a movement. Celebrity Jenny McCarthy, the longtime, best-known face of what is popularly called the anti-vaccine (or anti-vax) movement, insists, “I am not anti-vaccine. I’m in this gray zone of, I think everyone should be aware and educate yourself and ask questions.” Like other parents, she imagines that the goal is simply increased individual consumer choice.
Movements that have made the personal political and the political personal—from movements for women’s rights to those of students—have been effective in creating social change. Many health movements have placed personal experience, intuition, and situated ways of knowing at the center of healthcare decision-making. For example, women have fought against sterilization without consent, football players have argued for better research on concussions, and veterans have advocated for better treatments for post-traumatic stress. These and other health movements have made healthcare better. Patient concerns, experiences, and perspectives have guided research and treatment, and even changed clinical definitions.
Opponents of vaccine mandates see themselves in this tradition. Yet, the prevention of infectious disease raises new stakes for entire communities—not just the individuals making the decision. In these ways, the personal is not just political, it’s infectious. This matters for several reasons. Not all families, for example, are similarly able to weather a serious illness: inflexible work and fulltime care-giving roles, as well as health insurance access, can affect options for dealing with illness. And not all children have immune systems that can defend against a vaccine-preventable disease, or are even old enough to be vaccinated. For a small number, vaccines will be ineffective at inspiring an immune response. When most people in the community are vaccinated, these people are protected. However, in prioritizing each family’s goals for their own children, rather than a sense of community responsibility for those who are most vulnerable, vaccine opponents risk rendering these significant differences invisible.
An anti-vaccine sign at a 2010 Tea Party rally in Minnesota.
Public Domain

Vaccine Objections
So what are they worried about? Parents’ concerns about vaccines are multi-faceted, but include worries about when and how vaccines are offered, the adequacy of safety testing and monitoring, or even whether recommended vaccines are necessary. Underscoring all these concerns is a larger distrust of the state, which fuels calls for resistance to public health laws.
Increasing vaccines, decreasing trust. Most American parents today hail from a 1980s and 1990s generation that received up to 16 injections of vaccines against 8 illnesses: measles, mumps, rubella, diphtheria, tetanus, pertussis, Hib, and polio. In contrast, today’s kids receive up to 26 shots to immunize against 14 childhood illnesses. Most are given by primary care providers—most often pediatricians—in the first five years of life, with some offered in the first month after birth. This increase reflects both the licensing of new vaccines against common serious childhood illnesses and efforts to offer boosters to increase the probability a child will develop and maintain immunity against a particular disease. For many parents, the sheer number of injections raises concerns. Likening the view that vaccines can overwhelm the immune system to other challenges that could overwhelm the body, Leanne, a mother of four partially vaccinated children, explains, “You get somebody in the hospital with pneumonia and a leg infection and earache. You’re trying to deal with all different kinds of things in the body system, and I felt the same way with the shot. They’re trying to deal with all these different chemicals and just an overload on their system.”
Physicians and scientists are quick to point out that, since the technology for manufacturing vaccines has improved, children actually receive fewer bacterial and viral proteins—about 150 today compared to about 3,000 from the schedule in the 1980s and 1990s. They also highlight how infants encounter trillions of bacteria in the birth canal alone, demonstrating the capacity of their immune systems. Yet, these scientific explanations are largely unconvincing to parents who feel there are just too many vaccines and that babies’ bodies are too small to handle it. When a pediatrician insisted vaccines could be live-saving for an infant, Carolyn, a mother of three unvaccinated children, recalls insisting, “‘I’m making a choice, and who are you? And why is it that I have to do this in this time with a little infant?’ And I said no way.” Many parents, like Carolyn, point to babies’ size and vulnerability as a reason to reject vaccines.
Safety and distrust of regulation. Vaccines, like other products regulated and licensed by the Food and Drug Administration (FDA), undergo testing to ensure safety, purity, and efficacy. Once a vaccine is licensed, an advisory group within the federal Centers for Disease Control and Prevention (CDC) study its efficacy and safety and then make recommendations regarding when it should be offered to children. Professional organizations often endorse the CDC-recommended schedule, and states often codify these recommendations into school requirements. Margaret, the mother of two unvaccinated children, distrusts such coordination: “Well, basically the insurance companies and the drug companies are all working together. They’re all—the state health department as well. You look at their advisory board members, and you will see former drug reps and lobbyists. It’s all very convenient for them.” Another mother explains: “I guess I’m somewhat of a skeptic by nature. I’m very wary of government involvement… if it’s FDA-approved. That means nothing to me.” As parents describe their choice to resist vaccines, they often cite the collaboration and coordination between manufacturers, healthcare providers, and government agencies as suspicious.
Resistance and Parental Autonomy
Woven through the stories of individual choice is a core distrust of the state. Many parents, across the political spectrum, referenced the importance of freedom from government intervention or the ability to make choices without coercion. Molly, a mother of three unvaccinated children, feels strongly that parents should be educated about vaccines to make individual choices. She speaks to other parents about her concerns about vaccines, explaining that her goal is to “help inform them as to what their rights are and what their choices are, as opposed to just believing, ‘The government says, so I have to do it.’”
For parents like Molly, the decision to refuse vaccines for their children is much like any other parenting decision: individual families should choose what works best for them. As she sees it, there may be risks to not vaccinating and risks to vaccinating, it is up to each family to decide. Molly elaborates, “It’s like they need to make their own choices for their own family. People that have nudity in their house where they walk around nude around their kids all the time. Other people are like, ‘That’s gross, that’s child abuse.’ They’ve gotta figure out what’s right for their family.”
As parents criticize the state for imposing on families, they identify how each family should be empowered to consider their own risks and benefits. Although the risks of infectious disease to the community are different than the risks of nudity or many other choices, both center on an insistence that parents should be autonomous to make choices, even ones that are value-laden.
Altruistic Opposition
Vaccine resisters rarely seek to eliminate all vaccine use. Rather, parents insist that by advocating for other parents they can create healthier communities. Some argue that state efforts to prioritize vaccination allows other public health issues to be ignored. Many told me about the importance of organic food, nutritional supplements, breastfeeding, and avoidance of toxins as important factors in promoting good health, and argued that these aren’t supported by public policy. They see vaccines, a for-profit product, receiving state endorsement for seemingly capitalistic gains and other health challenges left without advocates.
Elizabeth, a mother of two unvaccinated children, referred to the “propaganda around healthcare in our country,” as being driven by “potentially capitalistic hype,” which she sees as prioritizes vaccines over other public health concerns: “I think the chickenpox vaccine is just a great example. How many kids have truly ever died of chickenpox? If you do the research it’s something like 1.2 a year or something. It’s like this miniscule number. Now, if that was your one child, I would understand that that’s 100% devastating, but there are way more children that die of drug infections and poverty and, you know, so many other social issues that we’re not fighting because the industries don’t have the resources to pump into [it].… Okay, we can convince everybody that their kid might be about to die from chickenpox, but really the likelihood of them dying from a car crash, you know—hunger, poverty, whatever it may be, are just—all of those things are so much more significant.”
CDC Global, Flickr CC

In light of the seemingly disproportionate attention vaccines receive over other public health threats, parents point to profit motives and government corruption as the most logical explanations. In this view, the state requires their resistance.
Vaccine Resistance for All?
A small and vocal opposition to vaccination has existed for as long as vaccines have been around. Since the first laws requiring smallpox vaccination in the 1800s, in fact, parents have argued that they—not the state—should have authority to decide what they and their children need and what they should consume.
These concerns are not going away. Surveys suggest that even among parents who support vaccination, more than 20% do not agree that following the recommended vaccine schedule is the safest course for their children. This limited faith in the official schedule and the experts who craft it suggests parents beyond this vocal movement in opposition to vaccines also feel distrustful. Decisions to refuse or delay vaccines will affect individual children who lack vaccines at the ages they most need them, but these choices carry risks to others. In these ways, individual choices don’t stay with the individual. Movements to resist vaccines may harm those outside those networks as outbreaks become more common. Ironically, as infectious disease outbreaks rise, families will likely look to the CDC, state agencies, and for-profit pharmaceutical companies to help.