
Abstract
Public health crises around Thalidomide and Rubella changed American public opinion around abortion policy. But could the spread of Zika do the same amid an outbreak of new state-level abortion restrictions?

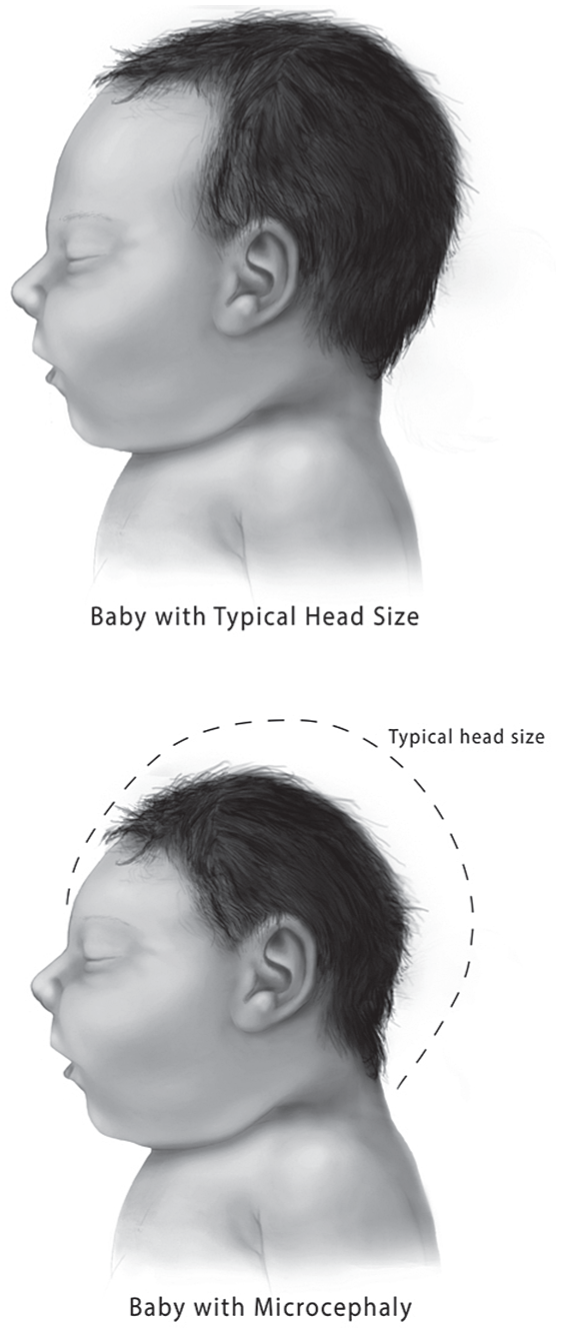
Babies with brain malformations, respiratory problems, and seizures. The Zika virus, which causes microcephaly and other grave health consequences for fetuses, has spread from country to country across the Americas, and even in the winter weather, is still being contracted locally by residents of Florida and Texas.
The birth of a severely neurologically impaired infant presents a crisis for an individual family. At the same time, as C. Wright Mills reminds us, even the most intimate and personal “troubles” intersect with the broader historical and cultural context. This larger level may be particularly difficult to see when the personal troubles seem rooted in biology. However, as Eric Klinenberg adeptly argued in his book on the Chicago heatwave, a public health emergency or even an individual death from heat exhaustion requires not just a medical autopsy but a social one. The silver lining of Zika may be that an illness becomes a catalyst for social change by leading governments to reevaluate policies, in this case reproductive rights laws. Thus, following Mills, we will get to the politics of Zika, but first, we must examine its history.
Zika was originally thought to cause no symptoms or only minor symptoms such as a rash, pinkeye, and fever that clear up quickly. First discovered in Africa in 1947, the Zika virus did not cause a mass outbreak until it started appearing in the 21st century on islands in the Pacific, notably Micronesia in 2007 and Polynesia in 2013. Health officials determined that a small percentage of infected people (one in 4,000) would develop a serious condition known as Guillain-Barré syndrome, which can cause paralysis and ongoing adverse effects for several months, but there was no mention of any increase in birth defects. Most of the world continued to ignore Zika.
That changed in 2015 when Brazil was in the midst of an outbreak and news outlets started showing footage of babies with abnormally small heads. These infants were born with microcephaly and due to their extensive neurological impairments will be severely impacted for life. Some survive no more than a few days or months. While the normal microcephaly rate is 200 per year, Brazil already had nearly 2,000 confirmed Zika-related cases by the end of 2016 and another few thousand were suspected but had yet to be investigated. Brazil’s spike in birth defects spurred a flurry of international research. Today, medical researchers are confident that infection in pregnant women is linked to microcephaly and other impairments, that Zika is a danger beyond the first trimester of pregnancy, and that the virus is not just caused by mosquitos but can also be sexually transmitted.
Why was this knowledge not obvious from the Asian cases? Ultimately, scientific studies retrospectively reported that Zika had caused brain damage in French Polynesia, but these cases were determined after the fact, not during the outbreak like in Brazil. This was in part because only a little more than 4,000 babies are born a year there compared to roughly three million a year in Brazil. In addition, some Zika-affected pregnancies end in miscarriages and, therefore, may not have been apparent to doctors and nurses as Zika casualties. Crucially, it is also because when women saw malformations on ultrasounds, the majority chose to terminate their pregnancies.
Pregnant women in French Polynesia could do this because French law not only allows abortion, but permits the procedure throughout all of pregnancy in cases where severe problems with the fetus are confirmed. Of the 19 cases in which Zika was suspected or established, 8 were microcephalic and another 6 had visible brain lesions; 11 of these fetuses were aborted. Five fetuses had no visible damage on imaging but after birth their brainstem dysfunction was readily apparent. Those born had problems breathing and eating as well as irregular heartbeats and epilepsy. Two babies died.
Centers for Disease Control and Prevention
Courtesy Guttmacher Institute, guttmacher.org
Given the seriousness of birth outcomes and the inability to prevent mosquito bites throughout nine months of pregnancy, officials in El Salvador, Colombia, Ecuador, the Dominican Republic, and Jamaica have encouraged women to delay pregnancy. In Colombia, women are told to wait six to eight months; in El Salvador, officials are saying two years in the hopes that the outbreak will pass as the population becomes increasingly immune.
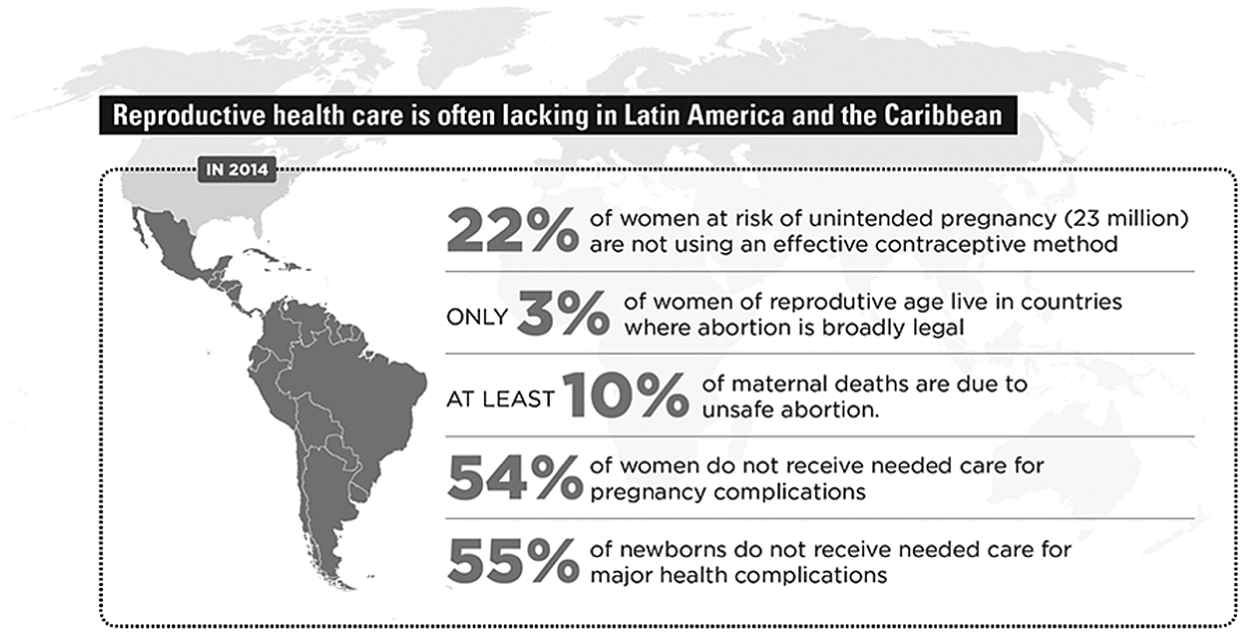
Women’s groups point out that these governments are placing all the responsibility on women—men are not being told to wear condoms. Additionally, they take governments to task for issuing advice as if all pregnancies are planned, despite the case that in some countries only half of pregnancies are intended. Contraceptive availability and rates of use vary dramatically: in some Spanish-speaking Latin-American countries, two-thirds to almost three-fourths of married women have access to birth control, but in other countries the rate drops to less than one-third. Unmarried women and teenagers have even less access to contraceptives. In situations of poverty, girls and young women may trade sex with older men for shelter or money, making negotiation of sexually transmitted infection and pregnancy protection extremely difficult. Obviously, this is true in sexual violence cases as well.
As women’s rights groups have argued, women can and do die from illegal abortions.
Many Latin American countries have very restrictive abortion laws (with the exceptions of Uruguay and countries with colonial ties to France). In El Salvador and Paraguay, recent cases of young minors who have been raped and forced to carry resulting pregnancies to term have elicited an international outcry. El Salvador provides no exemptions at all, even to save the life of the pregnant woman or girl. Women can even be prosecuted for miscarriages if they are suspected of having induced them. Religious groups continue to influence laws concerning reproductive rights, yet the tide is already turning. When asked point-blank about the Zika epidemic, abortion, and contraception, Pope Francis responded that while abortion is “an absolute evil,” “avoiding pregnancy is not an absolute evil” and referenced Pope Paul VI permitting nuns in the Belgian Congo to use oral contraceptives to prevent pregnancy in the case of rape in the 1960s. Thus, the Zika outbreak is the first event in 50 years to compel a pope to sanction contraception and on a much broader scale. Supporters of reproductive rights are hopeful that a door has been opened by the Pope’s comments, but others are more cautious about how this will translate into access for women in Latin American countries.
Meanwhile, pregnant women concerned about their offspring’s condition agonize about their financial and emotional ability to provide for very ill children as well as who will care for them when they no longer can. The lifetime costs of care for a seriously disabled child can run from the tens of thousands to millions. This presents a cost not only to individual families but also to governments.
Thalidomide, Rubella, and American Abortion
These issues surfaced in the 1960s in the United States. In the late 1950s and early ‘60s, it was becoming apparent that a drug prescribed in Europe to help people sleep—Thalidomide—was causing babies to be born with terrible anomalies including missing limbs. The type and level of complications were correlated with the point during pregnancy when the woman took Thalidomide. Relatively few American women were impacted because the FDA had not yet approved the drug in the U.S., but some doctors had handed it out anyway and other women took pills they or others got abroad. This was the case for Sherri Finkbine, a married mother of four expecting her fifth child. She was originally approved for a therapeutic abortion in the U.S., but fearing legal reprisals, doctors backed out. Instead, she flew to Sweden to obtain an abortion. Her very public case, in addition to pictures of “Thalidomide babies” from Europe, led to rising empathy for mothers, especially married, intentionally pregnant ones who faced serious birth defects.
At the same time Thalidomide was revolutionizing people’s understandings of both the effects of teratogens on developing fetuses and moral choices during pregnancy, a Rubella (German Measles) outbreak struck the U.S. in 1964. Rubella is not usually a very serious disease, but when a pregnant woman is infected during the first or second trimester, 40% to 90% of pregnancies will be affected. Babies born with Congenital Rubella Syndrome (CRS) can be blind, deaf, neurologically impaired, or all three, along with other problems. At the time there was no vaccine for Rubella, and fear gripped women of childbearing age. Twenty thousand children were born with CRS, and an additional 11,000 pregnancies ended either by miscarriage or abortion. Another 2,000 babies died at or shortly after birth.
The press related stories of women who had abortions and those of women whose children suffered the effects of CRS. This garnered tremendous sympathy from the American public. That these women were married and supported by their husbands, and often also by their physicians, lent credibility and made room for empathy. Unlike stories of unwed teenagers seeking back-alley abortions, the Thalidomide and Rubella cases extended respectability to the demand for abortion.
As awareness increased, attitudes toward termination for fetal defects became more favorable. An American Institute for Public Opinion poll in January of 1966 showed that 54% approved of abortion in the case of “deformity”; by May of 1969, in a California poll, 77% of respondents were supportive. Various advocacy groups including doctors, social workers, and even over 1,000 clergy members in the case of California’s Human Abortion Act (HAA), began to push for a loosening of states’ abortion laws to allow for terminations in cases of fetal abnormalities. In her book, Dangerous Pregnancies, Leslie J. Reagan relates that when the California Junior Chamber of Congress passed a resolution with 80% voting to support the HAA, a Jaycees representative explained that the Thalidomide crisis influenced the vote.
Despite opposition by Catholic organizations and some politicians, by the late 1960s and early 1970s, 13 states had liberalized their abortion laws to include therapeutic abortions for rape, incest, and fetal defects. Four states—Alaska, Hawaii, New York, and Washington—decriminalized abortions altogether in 1970. Amid the general outpouring of support, abortion was no longer a dirty word in the U.S., and the empathy extended to mothers suffering with illness-affected pregnancies had mushroomed into broader approval of abortion for a variety of reasons. The majority of states never passed laws to allow terminations for abnormalities, but only because Roe v. Wade beat them to it.
The Thalidomide and Rubella cases extended respectability to the demand for abortion.
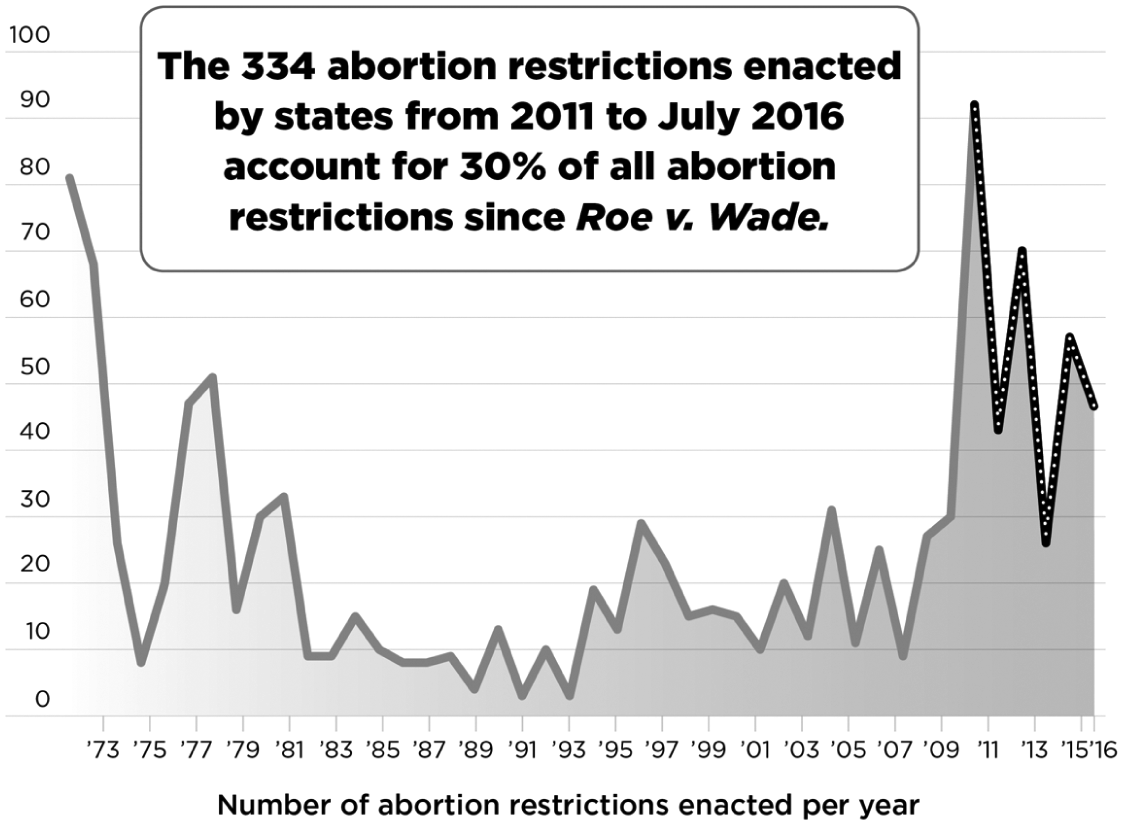
Almost 50 years later, abortion is more hotly contested than most people in the early 1970s would have predicted. Despite the fact that between one-fourth and one-third of American women have an abortion at some point during their reproductive lives, according to the Guttmacher Institute, 57% of American women today live in states with numerous restrictions on abortion. A slew of laws limiting women’s right to abortion have passed at the state level in recent years. Since 2010, state legislatures have proposed over 400 provisions attempting to reduce access to abortion, and many have passed. Some create waiting periods between a woman’s first abortion consultation appointment and the procedure, others mandate what information doctors are supposed to tell patients, and still others place restrictions on the types of facilities where abortions may be performed. New attempts at legislation mandate that aborted tissue must be cremated or buried (generally, this stipulation applies to the abortion provider, not the patient).
Courtesy Guttmacher Institute, guttmacher.org
Courtesy Guttmacher Institute, guttmacher.org
When he was the governor of Indiana, Vice President Mike Pence signed into legislation a 2016 bill, held up by the courts, that prohibits women from having abortion specifically because of fetal abnormalities—the very type of abortion that many Americans support and that helped lead to decriminalization of abortion in general. Like El Salvador, Indiana has imprisoned at least one woman for allegedly having caused her own miscarriage.
Several of the state law initiatives ban abortion after a certain number of weeks, but many birth defects are not detected until an ultrasound scan at 18 weeks or later. This leaves women subject to 20-week abortion bans little time to decide what to do. Zika’s congenital effects are not seen in fetal brains until these second-trimester ultrasounds (and may not be seen until even later). In French Polynesia, the median gestational age for termination due to microcephaly during the Zika outbreak was 30 weeks.
As Zika hit Miami, Florida senator and former presidential candidate Marco Rubio stated that he does not believe in abortion for rape, incest, or Zika cases, but when polled, the majority of Americans do. When asked specifically about abortion after 24 weeks in a recent Harvard-STAT poll, 61% of respondents initially disapproved and 23% were in support, but when microcephaly in fetuses was added to the question, the numbers reversed, with 59% in support and only 28% disagreeing. Zika is clearly seen by many as a legitimate reason for abortion, even late-term abortion, just as Thalidomide and Rubella were in the mid-20th century. Reproductive rights advocates can also use this ripe time to point out that many late-term abortions are performed in cases of health issues, the mother’s or the fetus’s.
As people draw connections between Zika, abortion, and women’s right to make their own choices about their families, and as the question goes from a hypothetical one to an actual one for the women of Florida, Texas, and elsewhere across the U.S., will voters turn away from restrictive abortion measures such as Indiana’s? As the examples from the 1960s show, when the American public began to discuss “respectable” reasons for ending a pregnancy, it opened the door for a deeper understanding of the numerous reasons (beyond health concerns) that compel women to have abortions. Could another summer of the Zika epidemic similarly stem the tide of restrictions on reproductive rights in the U.S.? Could it expand access to contraceptives and abortion in Latin America?
The UN High Commissioner on Human Rights has asked countries affected by the virus to suspend laws denying women reproductive choices. Human rights lawyers are preparing to try their case in Brazil, but they face opposition from some politicians and church groups. Currently, Mexican, Colombian, and Panamanian women can abort in cases of fetal defects. Will more of their neighbors pass laws to allow the same? Or even more expansive laws like Uruguay’s? As the new administration in the U.S. threatens abortion rights, Americans are donating in droves to organizations such as Planned Parenthood and demonstrating in Washington and other cities. Such protests can be effective, as in Poland in October 2016. When the government there moved to make already restrictive abortion laws draconian, tens of thousands of black-clad Poles demonstrated across the country and caused politicians to stand down. Many other Catholic countries in Europe have more liberal abortion laws, although Ireland, where a 31-year-old dentist was left to die from an incomplete miscarriage rather than being given an abortion, is a notable exception. This last example highlights the very real risks to pregnant women in countries that put undue restrictions on abortion. Women can and do die from pregnancy complications when fetus’s lives, in some cases even doomed fetus’s lives, are privileged above theirs. And as women’s rights groups have argued for decades, women can and do die from illegal abortions when the state will not grant them.
Social media scoffed at the CDC’s advice for pregnant women: “Don’t let mosquitoes bite you.”
Centers for Disease Control and Prevention
These realities, so often ignored by the public, politicians, and the press, are being forced back into the limelight by the terrible sequelae of the Zika virus. Trying to force women to bear children they know they will have trouble caring for, usually without adequate support from the very government that denies them control over these decisions, is likely to lead to a higher rate of illicit abortions and ultimately more health problems and deaths. President Trump’s reinstatement of the Mexico City policy, or global gag rule, will contribute to Zika-affected pregnancies worldwide by limiting both contraceptive access and abortions due to cuts in funding to non-governmental organizations that provide or even discuss abortions. On the other hand, states may use this health crisis to rethink their policies. In addition to working on a vaccine, governments have the opportunity to respond to the epidemic by promoting reproductive rights that will help all women, not just those affected by Zika. In the end, as Mills’ “personal troubles” create conversations in a larger social context, the pain suffered by families today may help expand women’s control over their bodies and their futures and help the families of tomorrow.