
Abstract
How naming a medical malady can be both horrifying for new parents and a key to unlocking resources and care.

Following an ambulance down Route 2 toward Boston was not the way I envisioned my day would go. That morning I pictured my wife and me bringing home our second daughter. Now, our newborn lay strapped in an ambulance as we tailed behind, her new car seat empty. Our destination was not home, but the NICU at Massachusetts General Hospital (MGH). In the span of two days, we had gone from being “parents of two children” to members of another club: parents whose newborn is suffering from an unidentified condition.
Hailey as a toddler.
Courtesy Gary David.
You do your time in the NICU waiting for something to happen, passing the hours in rooms intended to be as comfortable and comforting as possible, but are never really either. Tests are conducted, monitors go off, nurses weigh diapers, residents come through on rounds, parents eat meals in shifts. You wait for pieces of the medical puzzle to become a finished picture, still cautious about what that clarity might reveal. Sometimes not knowing is better, but knowing is the reason you are there. A diagnosis is needed, the puzzle needs to be solved. Uncertainty percolates. You anticipate a sense of the future that will arrive in the form of a diagnosis. For better or worse, it will define your child, your family, and your life.
The Sociology of Diagnosis
Diagnosis is the instrument through which questions of medical condition are answered. Mildred Blaxter, in her key 1978 piece “Diagnosis as Category and Process” succinctly noted that, even though “The activity known as ‘diagnosis’ is central to the practice of medicine,” researchers have not given it adequate attention. A sociology of diagnosis has emerged to fill this gap, exploring the importance that diagnosis has in medicine and among people and society.
Sometimes the presence of a condition is projected by a change in a person’s physical state. A lump might appear, something starts to hurt, a feeling of being “not quite right” results in the decision to seek clinical analysis and guidance. Other times, the diagnosis is a blind-side attack. There was no indication of a condition to be discovered. A narrative report titled “The Road to Diagnosis: Stories from Patients with Rare Diseases,” from the website Inspire, relates the experience of getting a diagnosis. Most of the stories describe the impact the moment of diagnosis had on the authors’ lives. Perhaps the most unfortunate, though, are those without a diagnosis. Problems exist in the absence of identification, a kind of conditional anonymity. You know you are no longer yourself, but don’t know who you now are.
Hailey, the author’s daughter, at birth.
Courtesy Gary David

Annemarie Jutel describes her own experience in Putting a Name to It: Diagnosis in Contemporary Society. “Receiving a diagnosis is like being handed a road map in the middle of a forest. It shows the way—but not necessarily the way out.”
Sometimes there is no way out. Rather than showing you how to get back to where you came, the map simply shows where you now reside, what the neighborhood is like, who your new neighbors are going to be, and maybe how long you are going to live there. There is no way out. Nothing to be conquered, nothing to be cured, nothing that can be “fixed.”
Harold Garfinkel, the founder of ethnomethodology, calls for direct observation of social action, in some instances going so far as enacting the practices of those being studied. Essentially, Garfinkel sought to understand how activity is coordinated through interaction and out of which meaning and context are achieved. The goal of the researcher, then, is meeting the unique adequacy requirement, a level of competence such that s/he could be recognizable as a member of the group being studied. I quickly fulfilled this requirement, but not by choice.
Being simultaneously the parent of a child in the NICU and a sociologist created a field experience that I did not seek out, a research project I didn’t sign up for.
Being simultaneously the parent of a child in the NICU and a sociologist created a field experience that I did not seek out, a research project I didn’t sign up for. Achieving an analytic sociological orientation can be challenging when you are also the parent talking to the specialists, whose child is attached to monitors and whose questions need answering.
Developing the Diagnosis
Under “Chief Complaint” and “Principal Diagnosis”, my daughter’s medical record listed the reason for her admission as “multiple congenital anomalies.” This included difficulty feeding, low oxygen saturation, polydactyly (the presence of extra digits), and other morphological features that came together as an unrecognized pattern of symptoms. These anomalies by themselves might not be cause for alarm. Upon finding polydactyly on a pre-natal ultrasound, the technician joked that such a feature used to be evidence of special powers and was prized among royalty. Nothing to worry about. Now this feature was perhaps a clue of something more significant.
The three David sisters: Cailin, Hailey, and Amelia (from left).

As our NICU stay lengthened, so did the list of specialists. We would get visits from the radiologist (giving our daughter the top-to-bottom once-over), nephrologist (hydro-nephrosis), cardiologist (ASD and bicuspid aortic valve), orthopedist (polydactyly and syndactyly on hands and feet), nutritionists and lactation consultants (low tone and difficulty feeding), and social workers (to help manage it all).
While each dealt with issues related to their separate areas of expertise, one specialist loomed large: the geneticist. The geneticist was the central figure, hoped to unify all of the “multiple congenital anomalies” into a coherent theme. The separate medical issues that had been uncovered could be treated, but genetics would answer the overarching question of a diagnosis at the root of all the disparate problems. Other specialists might be able to describe what was happening in parts of our child, but the geneticist would attempt to describe what she “was”. In many ways, this might lead to answering what, if anything, could and should be done.
When seeing someone’s new baby, it’s customary to coo “how cute,” “isn’t she adorable,” and “she looks just like you.” This was not the case when the geneticist entered the room. When Foucault wrote of “the clinical gaze,” this must be the look he meant. The process of dissection began as the geneticist walked in and viewed my daughter in my wife’s arms. After a long pause and with a tilt of the head, her assessment started:
“Her ears are a little low. Her eyes are somewhat far apart. Her palette is high. She has epicanthal folds.”
No congratulations were given. The geneticist did not smile or comment on how cute our daughter was. Instead, the placid listing of atypical morphological features conveyed what we had come to learn over three days: our baby was not like other babies. In other words, “Your child is not ‘normal,’ and it is written all over her face.”
The geneticist believed she knew what was wrong, but it would not be confirmed until the FISH test (flourescence in situ hybridization) and karyotype results, used to see into our daughter’s chromosomes, came back. She warned, “I’m going to tell you what I think it is, and I’m going to tell you not to look it up online. You’re going to do it anyway, so keep in mind that what you see online are the extreme cases.” The geneticist was clearly familiar with the parental freak-out that ensues from even a casual WebMD or Google Image search. This warning was our first indication that our daughter’s condition was potentially severe.
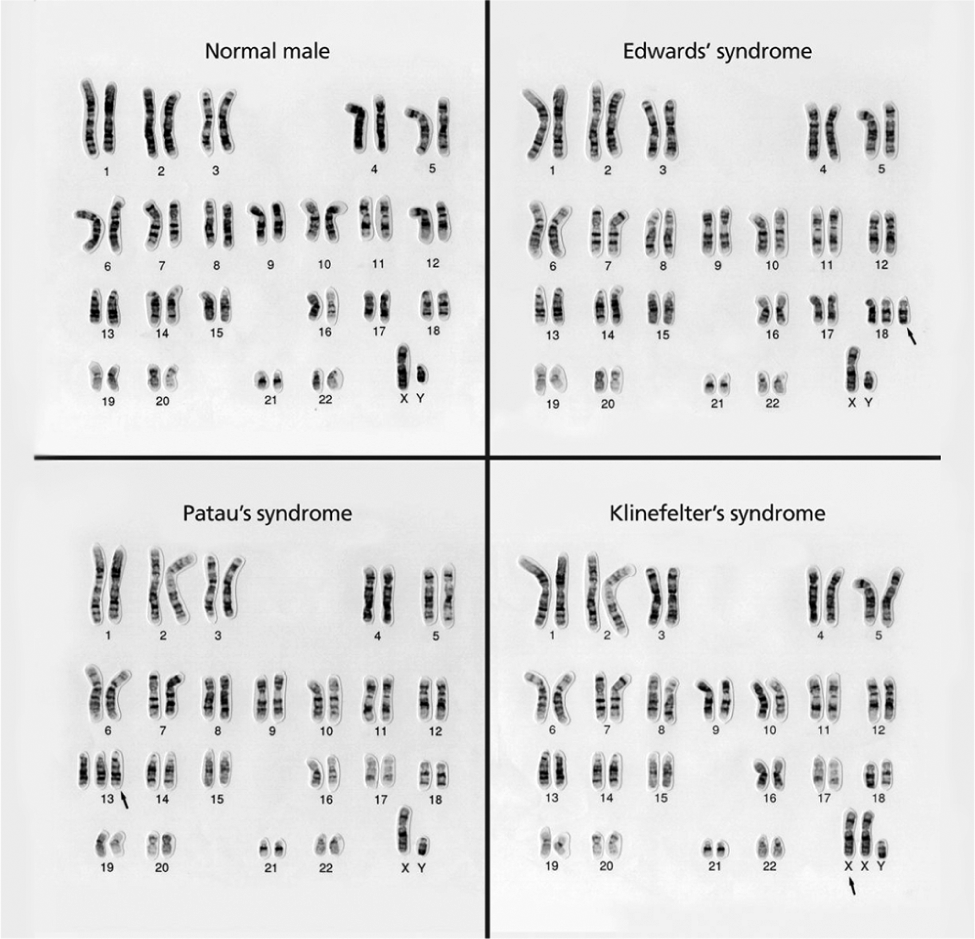
The genetic specialist’s initial thoughts would be confirmed: Trisomy 13 Mosacism. “Hard” findings tend to have a quantitative nature. In this case it was: “8 of 20 cells with three copies of chromosome 13.” This simply means that some of our daughter’s cells had an extra 13th chromosome. Full Trisomy 13 (or Patau Syndrome) is the presence of an extra 13th chromosome in all cells (just as Down’s Syndrome is the presence of an extra 21st chromosome). Trisomy 13 is reported to occur in 1 in 10,000 births, with mosaicism accounting for 5% of those births. Other than a random error during mitosis (the dividing of the embryonic cells), there’s no known cause, and the prognosis for children with full Trisomy 13 is bad. First-year mortality rates are over 90%. Though Patau is often considered “incompatible with life,” it is clearly not true—children with Trisomy 13 do live, even if for a short time. What kind of life is entirely another question, depending on individual circumstances and who is asked to judge.
Mosaicism is different. We were told our daughter would live, “somewhere in between normal functioning and severely disabled.” As the diagnosis became clearer, our future, ironically, became less knowable. Our initial uncertainty was amplified. Sure, all new parents wonder what their child’s future will be. The difference is most parents start with the expectation that things will be normal. We started on the opposite end of the spectrum. We needed to expect the worst while trying to find normal.
Karyotype charts show the markers for different conditions, including Trisomy 13 or Patau Syndrome.
Courtesy Wessex Regional Genetics Centre, Wellcome Images
Before leaving the hospital, a doctor told us he was sorry. He encouraged us to enjoy the time that we had with our daughter. With that, we were finally able to take that car ride home from the hospital.
The Good and The Bad News
It is strange to think of diagnosis as a gift. Typically, a diagnosis of illness or condition is unwelcome information. No parents want to hear their child has a condition that will impact his or her quality of life (let alone their own). On the other hand, the diagnosis makes other things possible. Medical treatment might be available, and children with qualifying diagnoses can get educational and therapeutic services more readily than those without. Looking back, our daughter’s diagnosis was actually one of the first baby gifts we received.
Looking back, our daughter’s diagnosis was actually one of the first baby gifts we received.
Oddly enough, as I have found in my own research on medical records, it is not uncommon for doctors to not provide a diagnosis. The symptom(s) and treatment(s) are seen as enough clinical information that any competent practitioner will know what the diagnosis is. For doctors, this may be understandable. If you document that “Patient complains of a pain in his head” and that “Aspirin were prescribed which resolved the problem,” the next doctor will likely infer that that the person was suffering from a headache. However, because that diagnosis was not written down, it cannot be coded, may not be submitted for billing, and might not be counted in other metrics. As medical professionals say, “If it isn’t written down, it didn’t happen.” We might add that, “if it isn’t diagnosed, the condition isn’t there.”
Hailey David
Courtesy Gary David.
A diagnosis can thus be treasured for parents seeking services for their child. Our child’s genetic testing provided institutionally valid confirmation of a condition that would qualify us for services, a kind of “key to the treatment kingdom” presented through the karyotype. For parents whose child has no diagnosis, but needs extra assistance, the absence of a confirmed, scientific label is frustrating, to say the least. It can also lead to conflict with various local, state, and even federal agencies. One parent reports that an application for respite care was rejected with the phrase, “No diagnosis of intellectual disability.” The parent noted, “No one had ever officially stated the obvious.” No parents want to hear that their child is “developmentally disabled,” except when it officially confirms what the parents already know, in order to get the help they need.
Parenting a child with a disability is a constant battle between thinking “what might have been” in the face of what is.
When we have told other parents of developmentally disabled children that we received our diagnosis three days post-partum, we have been told, “Oh, you’re so lucky!” Clearly not in terms of drawing the cosmic short-straw in having a child with a syndrome whose frequency is over 1 in 10,000 births, the luck refers to the institutional recognition that a condition exists, which then makes you eligible for services and care. There will not be questions about qualification or arguments over criteria. We can walk into a meeting, slap down our daughter’s test results of—“Trisomy 13 Mosacism”—and we are eligible. The key works.
I also have been told by parents that they were glad not to have a diagnosis right away, especially when the eventual diagnosis was a terminal one. These parents fondly recall the time when they could enjoy their newborn without any diagnostic cloud. My wife and I had no such time. Looking back, it is hard to say which situation is preferable. My wife and I would also wonder why our daughter’s condition wasn’t found in all of the pre-natal testing. What we would have done if it was found? What would we have done if we knew, if we had a diagnosis with no definite prognosis? What if we’d known the syndrome before we got to know our daughter? We never answered these questions. The answers were unknowable.
Dealing with the Diagnosis
In the end, everyone has to deal with a diagnosis. While traditionally thought of as the identification of a disease or disorder, every person gets assessed in the sense that they are or are not diagnosed. They either have a condition or are free from one. A healthy person, in essence, has a treatment plan: routine checkups. As one healthcare professional put it, “Everyone gets an ICD-9 code,” every instance of medical examination is an assessment.
Still, diagnoses differ in the degree to which they put us on a new life trajectory, whether they shake our foundations or future expectations, call us to question the certainty we once had before symptoms appeared and the diagnosis was delivered. Armand Marie Leroi, in his book Mutants, writes, “Mutation is a game of chance, one we must all play, and at which we all lose. But some of us lose more heavily than others.” Within us all is some alteration as yet unnamed, unidentified.
Parenting a child with a disability is a constant battle between thinking “what might have been” in the face of what is. It can be hard to appreciate what you have when you are preoccupied with “it was not supposed to be like this.” Relatively minor developmental milestones are less expected and more joyous, given the uncertainty about whether they would ever be reached. One parent described it as dealing with “what if” moments, where a routine observation of other “normal” children playing can hit you with the feelings of loss. Your “sick” child will never be able to do what the other kids are doing. It can be difficult not to let the diagnosis define the child and, instead, see the child in terms of deficits rather than abilities. The diagnosis becomes the shorthand for those limitations, and as a parent, your instinct is to fight against it. At the same time, you need the diagnosis. Parenting is always uncertain, but dealing with the diagnosis is unsettling at every level.
23andMe helps interested people see the secrets their DNA may hold.
Nathan Siemers via Flickr Creative Commons

My child may belong to a certain syndrome, but she is so much more than that. Today, she is an active 8-year-old who goes to school, fights and plays with her two sisters, attends birthday parties and inclusive summer camps, has the ability to remember anyone’s name, memorizes song lyrics, and forms friendships. The diagnosis doesn’t begin to say anything about her as a person. It never will. What the diagnosis has done is make much of her development possible through the services received, the dedication of her teachers and aides, and programs aimed at children with special needs. From Early Intervention before she was 3 years old to the one-on-one assistance when she started school, the diagnosis on her medical records gave us access.
I’d rather not have to deal with my daughter’s diagnosis at all. I’d rather a situation in which my knowledge of genetics was limited to 9th grade biology class. I’d rather not know that 23 pairs of chromosomes is the optimal number, and more or less than 23 is trouble. But this is the world we have, in which we continue to have challenges and triumphs, in which humor and irreverence are required to make the days manageable. We, like many parents, have a diagnosis. The moment of our daughter’s diagnosis is that life-changing moment that we will never forget. We were fortunate enough to have it.
When Foucault wrote of “the clinical gaze,” this must be the look he meant.