
Abstract
Despite disproportionate mortality rates for Black skin cancer patients, medical education and practice guidelines center White bodies and fair skin. How did dark skin become such a deadly dermatological blind spot?
Following a soccer injury in 1975, reggae legend Bob Marley attributed the dark discoloration under his toenail to bruising. After all, his physician’s advice upon evaluating him had simply been to stay off his right foot while it healed. As reported by Rolling Stone journalist Mikal Gilmore, it wasn’t until 1977, when Marley reinjured the same toe and lost the toenail, that the progressively growing lesion was accurately diagnosed as acral lentiginous melanoma (ALM)—the skin cancer that would ultimately metastasize to form tumors in his lungs, brain, and liver, claiming his life at the age of 36.
It is true—as the better-known part of the story—that Marley declined an amputation for spiritual reasons, even when advised that it might stop the spread of the disease to other parts of his body after his late diagnosis. The lesser-known part of his story, however, is that earlier detection, diagnosis, and treatment also might have saved his life before an amputation ever became necessary.
Marley’s story illustrates several important points about skin cancer in Black patients. First, it serves as a reminder that—contrary to popular myth—people of color, including Black people, can develop skin cancer. It also demonstrates the differential location of melanoma, the deadliest form of skin cancer, on those with dark skin compared to those with less pigmentation. Finally, as was the case for Marley, a Black-identified man of multi-racial descent, melanoma is frequently diagnosed far later in the disease progression for Black patients than it is for White patients.
Dermatologist Shasa Hu and colleagues studied the timing of patient diagnoses to see whether race affected stage at diagnosis. They found that 52% of Black patients were first diagnosed at the advanced stage, as compared to only 16% of White patients. Because of these and other factors, Black melanoma patients have disproportionately high mortality rates. In fact, as recently as 2019, the CDC reported that Black melanoma patients had only a 66% five-year survival rate from time of diagnosis as compared to a 90% survival rate for non-Hispanic White patients.
Despite all of this, current guidelines from the United States Preventive Services Task Force (USPSTF) regarding behavioral health counseling to prevent skin cancer recommend physicians only provide skin cancer prevention counseling to patients with “fair skin types.” The guidelines are situated within a history of medical knowledge production that has centered White bodies, leading to an incomplete understanding of skin cancer across the range of skin tones and insufficient medical training regarding dark skin.
Deconstructing the USPSTF Recommendation
The USPSTF is a panel of healthcare professionals with expertise in disease prevention and evidence-based medicine. They review existing medical materials and make recommendations to health care workers and organizations about preventive care and health promotion for patients in primary care settings. The USPSTF’s 2018 recommendation for preventing skin cancer concludes that clinicians should counsel adults, teens, children, and parents of young children, specifically those with “fair skin types,” about minimizing their exposure to ultraviolet radiation to prevent skin cancer. Its mention of those without fair skin types includes only that there is not enough evidence about such persons to include them in the recommendations.
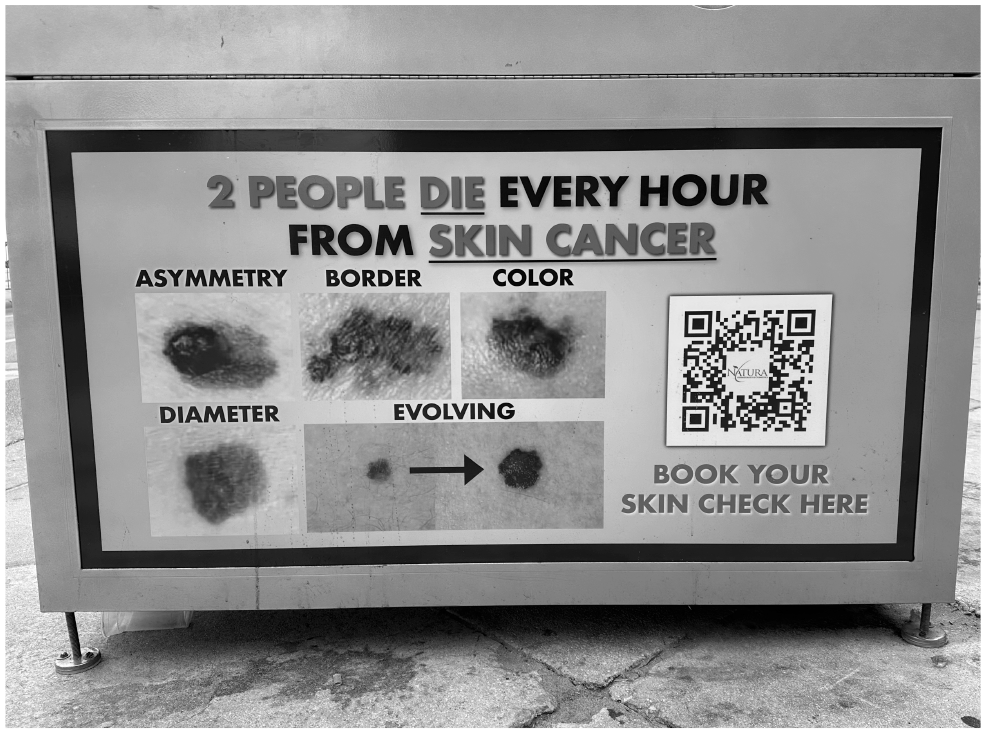
During Spring Break 2023, a Fort Lauderdale, FL dermatological practice posted these health education posters on recycling bins. Notably, each image depicts symptoms of skin cancer, but none shows what symptoms look like on dark skin.
Courtesy Ashley C. Rondini
This statement is problematic for a few reasons. First, it says that physicians and scientists don’t know enough about skin cancer in dark-skinned individuals to provide behavioral counseling—meaning clinician-recommended changes in behavior that can decrease the risk of disease. Essentially, the USPSTF has found that research about risk for skin cancer in patients with dark skin has not been prioritized or undertaken, so there are no studies from which to draw solid guidelines.
Second, the recommendations assume that behavioral counseling is comprised completely of cautioning patients to avoid sun or artificial UV light exposure. We know that sun exposure is an important risk factor for people with “fair” skin, but is it also important for dark-skinned patients? Or are there other risk factors they should be counseled about? We will discuss this issue further below.
When we deconstruct the recommendations, it is clear that their to-the-letter implementation can negatively impact patients with dark skin. As noted, Black patients diagnosed with skin cancer in the United States are less likely to survive the disease than are their White counterparts. In part, this is because skin cancer in Black patients is disproportionately detected at later stages. The recommendations, as written, exacerbate this problem. Since they systematically exclude dark-skinned patients from prevention efforts, it becomes predictable that these patients will be diagnosed at later points in the disease progression. This exclusion may also reinforce the popular notion that people with dark skin cannot develop skin cancer and therefore need not worry about taking steps to prevent it or seek screening for it—again delaying early detection and care.
Black bodies are rendered invisible within the milieu of relevant medical knowledge about skin cancer prevention. This erasure obscures the fact that disproportionate mortality rates could be mitigated through appropriate medical interventions. Consequently, inequitable outcomes appear somehow inexplicably or “inevitably” beyond the bounds of medical expertise—a self-fulfilling prophecy, of sorts. But this problem goes much deeper than the USPSTF recommendations—it must be traced through the erasures that have occurred throughout the history of medicine, the evolution of dermatology as a field, and the training of dermatologists in medical schools. Our ongoing exploration of these topics in the medical literature is supplemented by our conversations with a small pilot group of practicing dermatologists.
Racial Myths in Medicine
As people of color have long described, their bodies are often mischaracterized, erased, or pathologized at the intersection of modern medicine and historical conceptions of race. Myths about innate biological differences have often presented Black bodies as invulnerable to pain or to particular illnesses. Such myths result in inequitable access to medical interventions for Black patients, because they create the false assumption that medications or testing comparable to those offered White patients are unnecessary. As sociologist Ashley Rondini and physician Rachel Kowalsky have noted previously, when racial invulnerability myths inform the creation of clinical practice guidelines with which physicians are expected to comply, they codify meso-level structural inequities, meaning inequities at the level of institutions or organizations. These inequities include differential access to screening for illnesses to which Black patients are assumed to be “immune.” In this case, the myth embodied within the recommendations of the USPSTF is that Black people are invulnerable to skin cancer.
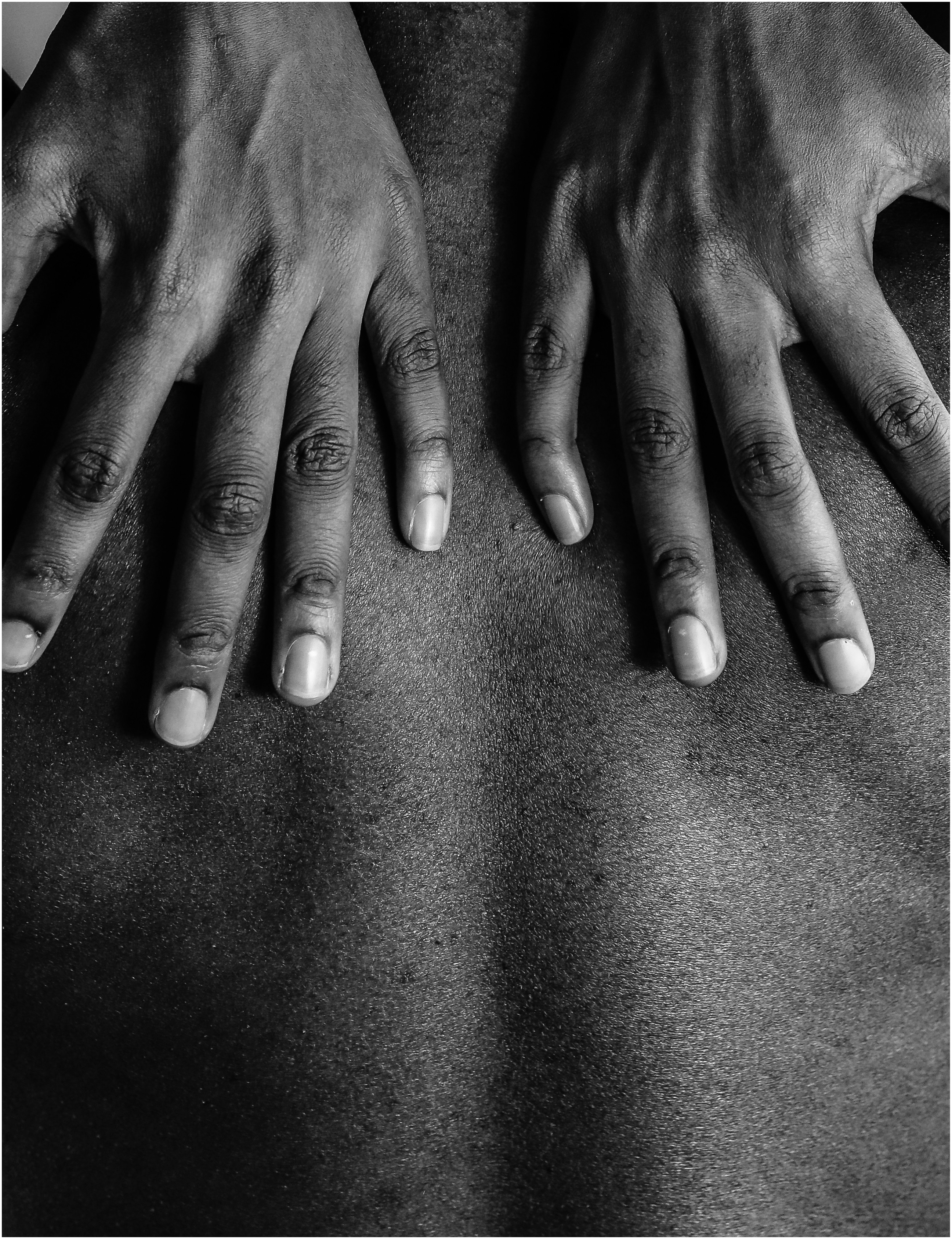
Black individuals can indeed develop skin cancer. The most common forms in Black patients are squamous cell carcinoma (SCC), followed by basal cell carcinoma (BCC) and then melanoma. Of the three forms, melanoma is the deadliest. It is associated with shorter survival and higher mortality rates than SCC and BCC. Returning to Bob Marley’s melanoma, recall that he had ALM. ALM is a particularly aggressive form of melanoma, occurring more commonly in Black patients than White patients. It is typically found on the non-exposed, least pigmented skin on the body: under the nails, on the palms of the hands, and on the soles of the feet. In comparison to BCC and SCC—which are likely to spread more superficially—ALM carries far more danger when left untreated, due to the greater likelihood that it will quickly spread to other organs. Because ALM is more common in Black patients, found in less obvious sites on the body, and particularly aggressive, physicians’ expertise in and familiarity with cancer in Black patients are critically important to patient survival.
A histological examination will determine whether tumor samples are cancerous.
iStockPhoto.com // Leonid Eremeychuk
White Normativity in Dermatology
The concept of White normativity refers to the ideas and practices through which White people are positioned as the normative standard for all human beings, while people of color are seen as inherently divergent. Race scholar George Yancy discusses the “insidiousness” of Whiteness operating as “unseen, unmarked, unnamed, unraced”; “invisible” in its normativity because of how it is positioned as the center of human experience.
White normativity is deeply embedded within the history of medical science. In the United States, mandates to include people of color (and women) in clinical research studies were not implemented until Congress passed the National Institutes of Health (NIH) Revitalization Act of 1993 (Public Law 103-43), interrupting the long history of solely using White male research subjects as a proxy for all human bodies. As historian Harriet Washington documents, when Black participants have been included in medical studies, it has often been in the absence of their informed consent, under abusive conditions, and in ways that exploit their vulnerable socio-political positionality—rather than as voluntary participants in clinical trials from which Black communities would benefit.
The field of dermatologic oncology—the study of cancers that affect the skin—developed in a context that centered White normativity. Most original 20th-century medical studies about risk factors for skin cancer were conducted in regions of Western Europe with predominantly fair-skinned general populations, such as England, Scotland, and northern Italy. Later studies, conducted in multiethnic regions of the world, like the United States and Australia, systematically excluded those with dark skin, assuming that these populations had lower prevalence rates and did not require study.
New medical studies typically rely upon older studies for theoretical frameworks and concepts about disease. This means the modern body of literature on skin cancer draws from a body of “knowledge” focused on the types of cancers most commonly occurring in fair skin types. This circular process of knowledge production, in which Black patients were initially excluded, then excluded again from derivative studies, has created a situation in which most knowledge about skin cancer is actually only knowledge about skin cancer in fair-skinned people. Medical professionals who rely upon this “knowledge” to make clinical decisions may unknowingly reinforce the original misconceptions about racial differences within the general population.
White normativity factors into the USPSTF recommendations in another important way. Indoor tanning beds, and behavioral counseling about avoiding them, have been thoroughly studied in the skin cancer prevention literature, and they are mentioned several times in the USPSTF recommendations. This concentrated attention primarily reflects the values and behavior of fair-skinned patients, for whom a tan may represent tropical vacations, an outdoor lifestyle, and physical fitness. In contrast, the prevalence of colorism confronted by many communities of color in the United States and beyond socially privileges light skin tones over dark skin tones. Perhaps unsurprisingly, BIPOC-identified individuals do not practice indoor tanning as frequently as do their White-identified counterparts, even across the wide range of skin tones that exist within BIPOC communities. Juxtaposed with the innumerable studies on UV exposure risks, comparatively scant research has been conducted regarding the effects of derma bleaching—a skin-related risk behavior more commonly practiced in communities of color around the world. Studies are needed to establish a comprehensive understanding of the medical risks associated with this practice.
Decolonizing Dermatology
White normativity in dermatology is also reflected in insufficient physician training with respect to dark skin. The movement to “decolonize dermatology” aims to disrupt White normative bias, including the lack of diverse skin tones represented in medical textbooks and academic curricula.
Dermatology, as one dermatologist told us in an interview, “is a very visual field,” meaning that the diagnostic indicators for most conditions that dermatologists are trained to identify manifest as observable changes to the skin. Thus, physicians are trained to recognize conditions in their patients by first engaging with textbook images—a seemingly straightforward pedagogical practice. Or, it would be, if those textbooks provided reference images depicting those conditions on a wide range of skin tones.
In reality, dark skin tones are systematically under-represented in diagnostic atlases used for medical education. Sociologists Patricia Louie and Rima Wilkes conducted a review of images from the most commonly assigned preclinical anatomy textbooks in U.S. medical schools, finding that none of 4,146 images depicted the six most common forms of skin cancer on dark skin tones. This underrepresentation in images depicting skin cancer—from which physicians derive their earliest understandings of the disease—reinforces White normativity in preventive and diagnostic care. This is not inconsequential. If depictions of skin cancer in medical educational materials are limited to fair skin tones, the odds that a given physician will recognize cancer on darker skin at an early stage—conferring the highest likelihood of survival—are likely reduced. For example, a 2020 study by Anne Fenton and colleagues in the Journal of the American Academy of Dermatology found that students at two well-known U.S. medical schools were nearly 30% less accurate in diagnosing SCC in the skin of patients of color than in the skin of White patients.
If depictions of skin cancer in medical educational materials are limited to fair skin tones, the odds that a given physician will recognize cancer on darker skin at an early stage are likely reduced.
There is one area of medical research that is well-resourced with images of medical conditions on dark skin. Another medical textbook image study, conducted in 2019 by Jenna Lester and colleagues, found that while skin of color only appeared in 22%-32% of overall images, that proportion doubled to 47%-58% among images depicting symptoms of sexually transmitted infections (STIs). During our interviews with a pilot group of practicing dermatologists, several referred to historical ties between dermatology and colonialism through the field of tropical medicine, which focuses on skin conditions in the tropics, including “dermatovenereology,” a term which relates “venereal disease” (considered an outdated term in the United States) to skin. Because of its position within colonized regions populated by dark-skinned individuals, the lens of tropical medicine often exotified and sexualized colonized populations, leading to a focus on STIs. One dermatologist specializing in skin of color emphasized this historic point in our interview, noting that “the study of dermatology was a study of sexually transmitted infections and syphilis.” The term dermatovenereology is still in use today in Europe.
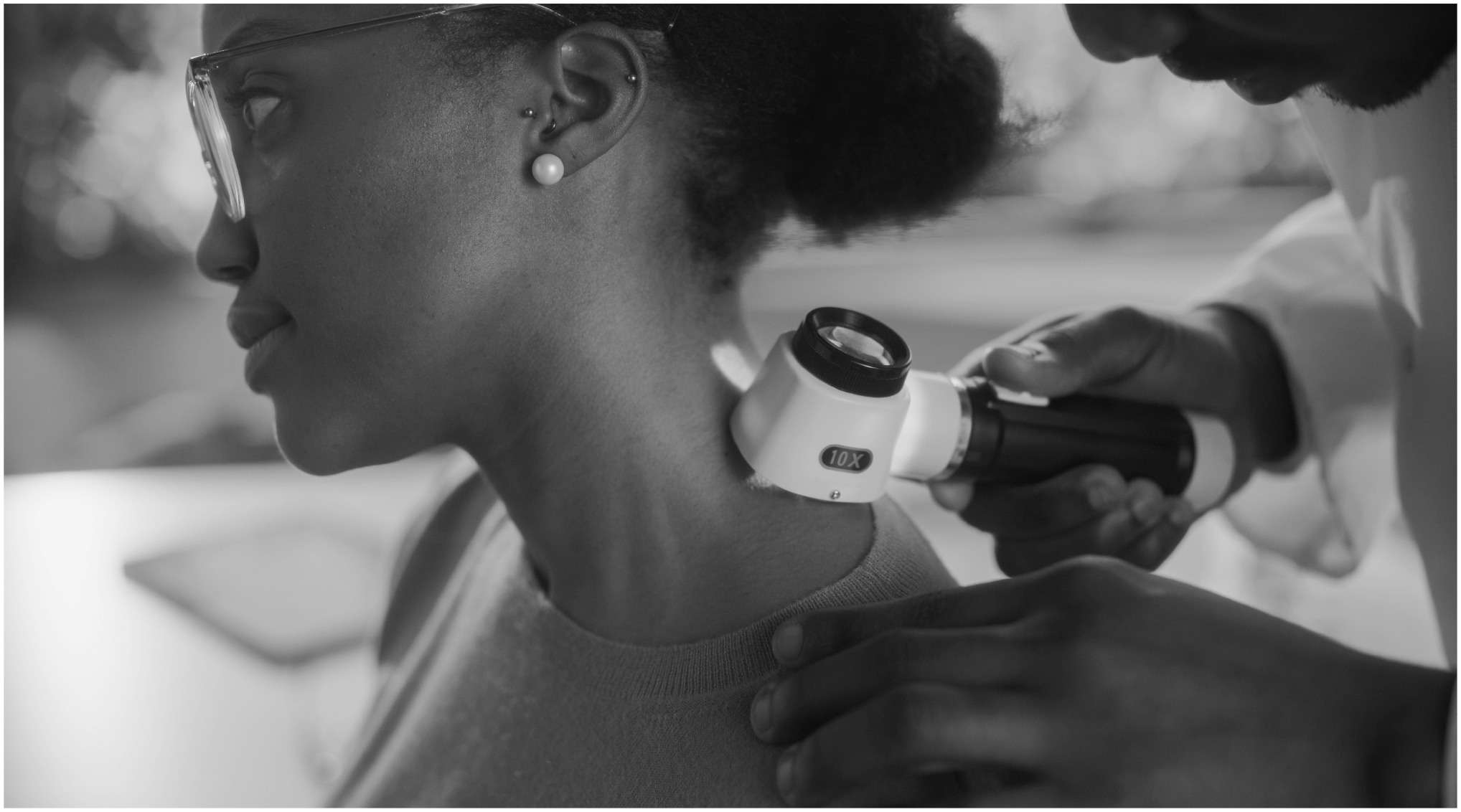
Early detection is key to successful skin cancer treatment, but studies find more than half of Black patients are diagnosed at advanced stages.
iStockPhoto.com // gorodenkoff
Textbooks aren’t the only educational vehicle through which dermatologists may (or may not) gain exposure to skin of color. During a physician’s residency period—a period of focused post-graduate experiential training after medical school—the geographic location of one’s assigned placement can inform the relative diversity of patient demographics and, by extension, physicians’ exposure to different skin tones. Our interviewees noted that residency placements in communities of color sometimes provide the first introduction that physicians receive to identifying dermatological conditions on dark skin, given the dearth of textbook models from which to draw reference. Of course, this also means few trainees bring the same degree of preparation to encounters with dark-skinned patients that they bring to the care of their fair-skinned patients, yet another compounded dimension of inequitable care.
Dermatologic oncology is arguably the one field in which skin color itself may actually have biological implications beyond the health consequences of exposure to racism.
Brown Skin Matters
A rising movement within the field of dermatology seeks to change the status quo. In 1999, The Department of Dermatology at Mt. Sinai Hospital opened the nation’s first specialized Skin of Color Center, staffed by board-certified dermatologists with specialized training in the unique needs of patients with “pigmented skin.” The expansion of this model throughout the country has been steady, but slow. Between 1999-2020, 14 other “Skin of Color” or “Ethnic Skin” centers have opened in medical facilities throughout the United States, all of which are located in major urban centers. These centers endeavor to address the dire need for long-denied focused dermatological care in communities of color. Echoes of White normativity persist, however, in the juxtaposition of the “marked” other—providing “skin of color,” “pigmented skin,” or “ethnic skin” care—framed as an alternative to the “unmarked” normative White category, always called simply “skin” care.
In 2004, Dr. Susan C. Taylor, MD, founded the Skin of Color Society: a professional organization focused on promoting “awareness of and excellence in skin of color dermatology,” which offers educational symposia, supports applicants of color applying for dermatology residencies, and keeps an active database of practicing physicians with specialized training in skin of color. While the organization has grown to an estimated 1,200 members, it is important to note that the need for all dermatological care in the United States significantly exceeds the capacities of current providers, and this gap in care is exacerbated for communities of color. New educational resources are also in the works, and several are already available online.
Other initiatives have come from outside of the medical community. “Brown Skin Matters,” a community-sourced digital image library of dermatological conditions on various skin tones, was established in 2018 by Ellen Buchanan Weiss—not a physician, but, rather, the parent of a pediatric dermatology patient. The site’s Instagram account has 113k followers as of this writing, and its images can now be readily referenced by both parents and medical practitioners.
Following the murder of George Floyd and the focus on health equity catalyzed by the COVID-19 pandemic, the USPSTF commissioned a 2021 report to identify strategies for mitigating the effects of systemic racism on its recommendations. A central assertion underscored by the Task Force was that individuals who experience racism are also disproportionately impacted by illness conditions and premature mortality attributable to preventable causes. The report, titled “Actions to Transform U.S. Preventive Services Task Force Methods to Mitigate Systemic Racism in Clinical Preventive Services” and published in the Journal of the American Medical Association, signaled the USPSTF’s commitment to counteracting social injustices in healthcare by making changes to their methods for developing recommendations and integrating changes into selected existing topics. Even more recently, in 2023, the USPSTF issued guidance concluding that there is insufficient evidence to assess the harms and benefits of doing general skin cancer screening exams of asymptomatic adolescent and adult patients. This finding further underscores the need for behavioral health prevention counseling to compensate for the lack of clinical safeguards that universal screening practices might have created.
To date, it remains to be seen whether or when the White normative bias embedded within skin cancer prevention recommendations will be critically reevaluated by the USPSTF. We just don’t know yet whether the requisite research needed to support more inclusive recommendations will be funded and conducted any time in the near future.
What we do know is that deeply embedded racist ideologies in American medicine have attached biologized mythologies to skin color and called it “science” for centuries. Myths of race as biology—most often operationalized in terms of skin color—have long been posited to “naturalize” inequities in social hierarchies, education, labor market participation, and health outcomes across a wide range of conditions.
Racist pseudo-science has a thoroughly documented history of scouring Black bodies for some “proof” of biologic difference from White bodies—and its flawed claims have reverberated loudly within American social systems, at the cost of Black lives. Dermatologic oncology is arguably the one field in which skin color itself may actually have biological implications beyond the health consequences of exposure to racism, for which it acts as a proxy. And yet, somehow differences between groups remain too understudied to develop skin cancer prevention recommendations for patients with dark skin. Where the science on differences in skin color is needed to save Black lives, the silence is deafening.