
Abstract
Lamberta LK, Asmar M, Fredwall MM, Ahrens SM, Bai S, Eisner M, Lado FA, Schuele SU, Clarke DF, Abdelmoity AT, Davis KA, Hopp JL, Koubeissi MZ, Bensalem Owen MK, Herman ST, Ostendorf AP; NAEC Center Director Study Group. Neurology. 2025; Jun 10;104(11):e213689. doi: 10.1212/WNL.0000000000213689. Epub 2025 May 16. PMID: 40378375; PMCID: PMC12089659. Objectives: Status epilepticus (SE) is a neurologic emergency that requires urgent recognition and medical management. SE management remains heterogeneous across centers. Methods: We analyzed SE treatment protocols from level 3 and level 4 epilepsy centers. Discrete data including stabilization measures, timing of treatment phases, medications, doses, and routes of administration were collected from each protocol and described using frequency for categorical variables and median for continuous variables. The distribution of treatment times and dosing were compared with the AES guideline. Results: A total of 256 SE treatment protocols were included. Only 66% of SE protocols detailed treatment times. Doses below recommendations occurred in 4% of protocols for initial benzodiazepine (BZD) and 14% for first non-BZD medications. Infusion therapy was outlined in 61% of protocols. Discussion: Despite the importance of timeliness in SE management, one third of institutional protocols did not specify treatment times. This analysis of US hospital inpatient SE protocols provides expert opinion regarding infusion therapy management and highlights gaps and targets for improvement in SE treatment.
Commentary
Status epilepticus (SE) demands rapid recognition and targeted therapy to improve patient outcomes. The recent analysis by Lamberta et al provides crucial insights into the current state of SE management. They reviewed 256 SE protocols submitted by Level 3 and Level 4 epilepsy centers in 2022 to the National Association of Epilepsy Centers (NAEC) as part of their accreditation process. 1 The authors compared the SE management protocols to the AES's 2016 SE Guideline. 2 The AES guideline recommends a timed, staged approach. After the first 5 min of patient stabilization, benzodiazepines (BZDs) are administered within 5–20 min, followed by second-line non-BZD IV anti-seizure medications (ASMs) in the next 20 min, and anesthetic or repeat IV ASMs if needed, for managing refractory SE (RSE). Continuous EEG should support the latter phase. The AES SE guidelines conform to the highest quality evidence until the RSE stage.
Before jumping into the specifics of the findings, it is critical to take in the bigger picture and consider the following:
- Treatment protocols are idealized, aspirational documents backed by the best available scientific evidence. They are a tool for translating evidence into action and help standardize care. They must meet the highest standards and lay strong foundations for SE readiness and management to offset inevitable bedside deviations. - Studies show that up to 75% of SE cases are managed outside of the hospital by the emergency medical services (EMS) or the emergency department (ED).
3
The protocols analyzed were submitted by NAEC centers, which likely means by the epilepsy division or the neurology department. Therefore, it is possible that the sphere of influence of the analyzed SE protocols may not even impact most SE patients. - Protocols don’t often translate into real-world practices. Multiple prospective and retrospective studies, including analyses of randomized controlled trials (RCTs), show median times to first BZD use of ∼30 min, second-line use after 70 min, and sub-therapeutic dosing in more than three-quarters of patients (Table 1). The existence of a protocol, therefore, does not guarantee timely or adequate treatment. The late and light dosing of ASMs in RCTs shows that overcoming entrenched practices is incredibly difficult, even in a controlled research environment. Additionally, it is humbling to realize that these deviations in SE management are observed in tertiary academic centers, and lower-level centers are unlikely to perform better.
Studies Reporting on ASM Use for SE Management in Real-World Settings.
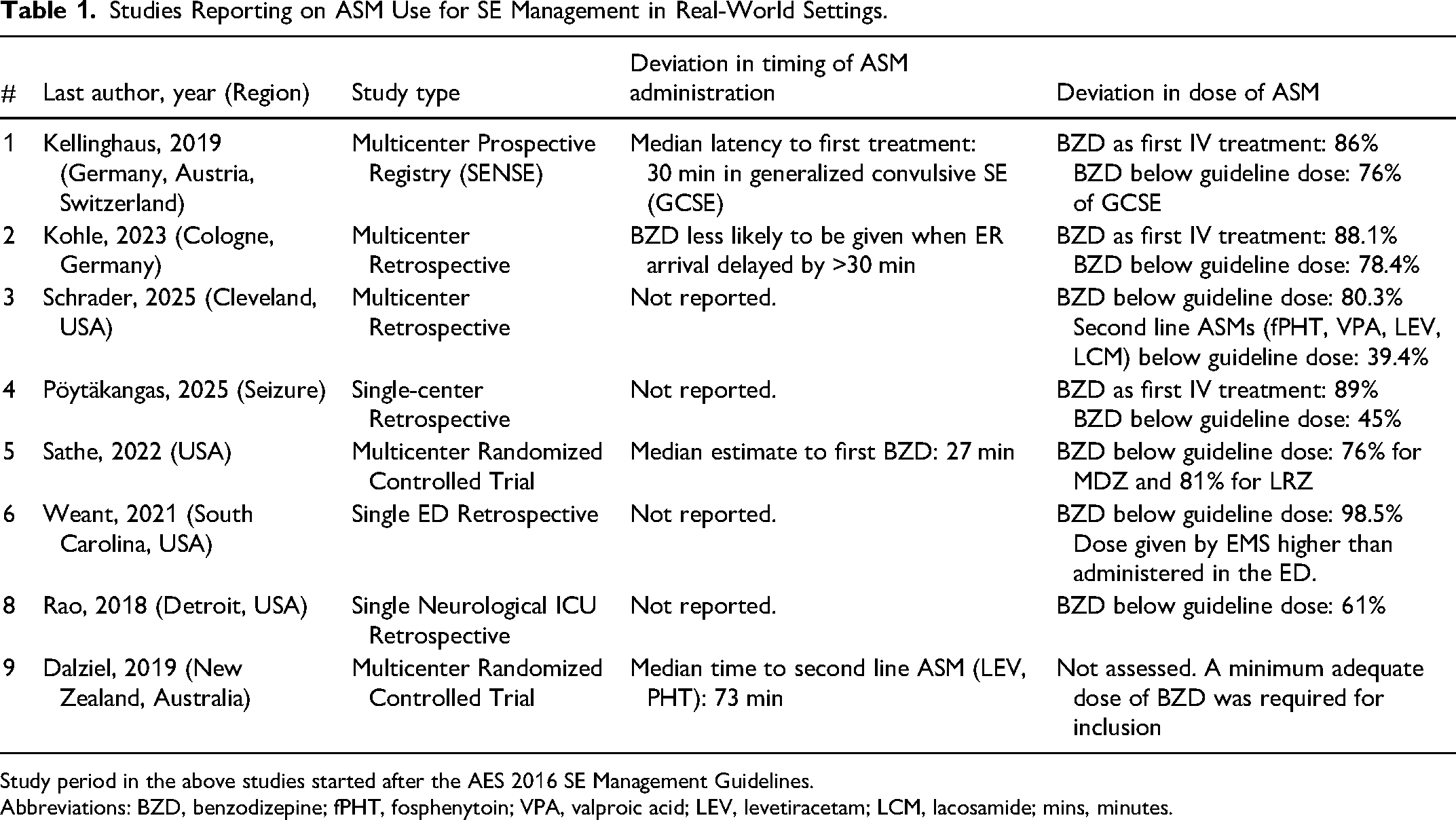
Study period in the above studies started after the AES 2016 SE Management Guidelines.
Abbreviations: BZD, benzodizepine; fPHT, fosphenytoin; VPA, valproic acid; LEV, levetiracetam; LCM, lacosamide; mins, minutes.
Within this broader context, Lamberta et al identified several specific gaps. The inconsistent inclusion of basic stabilization measures at the start of the protocol is quite surprising. Only 65% to 70% of protocols mention oxygen use and getting an ECG or oxygen monitoring. Fewer than one in four specify calling a response team. To be charitable, it may be because the basics of airway, breathing, and circulation management in any medical emergency, including seizures, are so deeply ingrained in us that adding them to the protocol seemed unnecessary. On the flip side, the absence of such fundamentals from a sizable fraction of SE protocols underscores the risk of treatment “tunnel vision,” focusing on SE aborting drugs while neglecting the physiological environment in which they are delivered. SE readiness is not only about timing and drugs but also about embedding a complete resuscitation framework. Also notable is that, despite SE management being a battle against time, one-third of protocols omit explicit time-based escalation, thereby inviting a “wait and watch” approach. Additionally, only half list a revision date, and nearly a quarter still predate the 2016 AES guideline.
The study found that the protocol's alignment with guideline-recommended dosing is higher when it is based on level 1 evidence. Most protocols included recommendations on dosages of BZD, IV ASMs, and IV anesthetics. Nearly all centers matched AES BZD doses, but ∼14% diverged on second-line IV ASM dosing, and about one-quarter underdosed levetiracetam (LEV) or valproate (VPA). It is worth noting that the ESETT trial's finding that fosphenytoin, VPA, and LEV have comparable efficacy in aborting SE is only valid when the administered loading doses are 20, 40, or 60 mg/kg (maximum 4500 mg), respectively. 4
In contrast to the first- and second-line therapies, RSE management exhibited extreme variability. Only 61% reported infusion therapy, and 18% specified ketamine dosing, despite its growing role in RSE. 5 Three-quarters mentioned continuous EEG, yet only 14% specified infusion tapering (not part of the AES guidelines). It suggests cEEG is often ordered perfunctorily rather than used to guide anesthetic weaning in RSE. A global study linked prolonged EEG use to shorter IV anesthetic courses. 6 With IV anesthetics’ use potentially associated with worse outcomes, cEEG use must be part of SE protocol implementation.6–8 A systematic review likewise found that cEEG monitoring goals are often unclear. 5 Incorporating cEEG-based titration rules informed by literature and expertise into SE protocols could harmonize practice and standardize care.
Addressing many of the above protocol deficits and poor adherence to evidence in routine practice requires structured implementation, not more guidelines. Implementation science suggests that making changes in several key areas is essential for incorporating guidelines into routine practice. 9 In the context of SE management, at the professional level, epilepsy teams should develop and disseminate protocols with buy-in from all stakeholders. Even low-tech tools, such as laminated pocket cards for caregivers, can improve adherence to the SE protocol. 10 Institutions can embed weight-based order sets and clinical decision support into electronic medical records. At the regulatory level, the NAEC accreditation could require a “minimum elements” checklist endorsed by all key departments (ER, Hospital Medicine, Surgical, and Neurology services) to ensure content quality, not just document presence. Ultimately, ensuring optimal SE management requires a multi-pronged approach that extends beyond protocol creation to ensure system-wide implementation and adherence.
In conclusion, the study by Lamberta et al has a clear message that the existence of guidelines is insufficient without implementation scaffolding. It shows that even in top-tier epilepsy centers, many protocols lack explicit timing, adequate dosing for some second-line agents, and structured RSE management, with the latter still lacking high-quality evidence. When these results are evaluated in the context of real-world practice data, they should serve as a call to action for ensuring consistent implementation of guideline-adherent SE management across all levels of care. SE outcomes will improve only when every center owns its protocol. If you guide SE care, make it a priority to examine your institution's documents for alignment with guidelines. To turn the written protocols into better SE outcomes, all stakeholders, from EMS to ER and inpatient teams, must be engaged and educated. Quality-improvement initiatives should then be launched to ensure these guidelines are consistently applied in everyday care.