
Abstract
On June 24, 2022, Dobbs vs Jackson Women’s Health Organization was decided by the Supreme Court effectively overturning the former precedent of Roe v. Wade. This ruling has direct consequences for the care of persons with epilepsy of childbearing potential. Now more than ever we need to provide informed and comprehensive care to our patients with epilepsy who are particularly vulnerable to the impact of this legislation on their reproductive decision-making. Important areas to understand include (1) the current state of affairs on abortion in the United States; (2) contraception options, their effectiveness, and interactions with anti-seizure medications (ASM); (3) teratogenic effects and adverse neurocognitive outcomes of ASMs; (4) folic acid supplementation; (5) the effect on perinatal and pediatric care; and (6) unique issues related to people of color.
Introduction
A half-century ago, Roe v. Wade was decided by the Supreme Court when Texas lawyer Sarah Weddington argued the case that women had the right to privacy under the 14th Amendment to determine whether to pursue a safe and legal abortion. 1 That same year, Henri Gastaut, along with World Health Organization collaborators, published the Dictionary of Epilepsy where he defined older terms such as “falling sickness” and “fit” as “obsolete,” engaging the medical community to embrace new terms that took on a data-driven view of epilepsy, a need that he described as “increasingly urgent.” 2 Changes throughout the medical community were occurring as new viewpoints of age-old problems emerged.
On June 24, 2022, Dobbs vs Jackson Women’s Health Organization was decided by the Supreme Court effectively overturning the former precedent of Roe v. Wade. Many national and international medical organizations took to their platforms to state their opinion on this landmark decision including the American Epilepsy Society (AES) which stated that the goal of AES is “equitable access to quality health care for all people. Further, we stand firm in our responsibility to deliver evidence-based medical care consistent with the best interests of our patients and against any interference into the practice of medicine that undermines the integrity of the physician-patient relationship.” 3 It was acknowledged that although not all may share the same opinion on abortion, “it is critically important that medical decisions are made by qualified practitioners” and that this be done based on evidence with respect for the individual patient. 3
In caring for persons with epilepsy, maintaining the highest standard of evidence-based care is our goal. The consequences of caring for people who can become pregnant without such knowledge regarding the intersection of epilepsy and reproductive health bears a greater weight for these individuals who may have fewer reproductive options since Dobbs v. Jackson. The goal of this article is to review key information to equip the epilepsy practitioner in caring effectively and compassionately for persons who may be affected by this ruling. In this context, this article will review (1) the current state of affairs on abortion in the United States; (2) contraception options, their effectiveness, and interactions with anti-seizure medications (ASM); (3) teratogenic effects and adverse neurocognitive outcomes of ASMs; (4) folic acid supplementation; (5) the effect on perinatal and pediatric care; and (6) unique issues related to people of color (POC).
Current State of Affairs on Abortion
Abortion is common in the United States; about 25% of people who can become pregnant have at least one. Most abortions (85%) occur early in pregnancy within the first trimester. Young age, being in school, difficult economic circumstances, lack of social support, and previously completing a family comprise common reasons. Black Americans, who face higher risks in pregnancy and worse economic circumstances than white Americans, more often end their pregnancies with abortion. People with epilepsy of childbearing potential (PWECP) experience as many, perhaps more, unplanned pregnancies than their healthy peers. 4,5 About 50% of these unplanned pregnancies end in abortion.
Two methods are used for abortion early in pregnancy: dilation and suction curettage (D&C) and medications. Dilation and suction aspiration can be accomplished safely with local cervical anesthesia and nonsteroidal anti-inflammatory drugs, as well as moderate or deep sedation. Most sedation for abortion includes a benzodiazepine which is helpful to patients with epilepsy by decreasing the risk of a seizure. Most abortions by D&C occur in free-standing facilities outside of hospitals which is also safe for patients with well-controlled seizures. As of 2020, medications are used for about 50% of early abortions. Medication abortion includes oral mifepristone, a potent progesterone antagonist, followed by the prostaglandin misoprostol. Telehealth services are a safe and effective way to provide medication abortion. Using these medications, patients experience bleeding and cramping and expel the pregnancy at home. Patients report high satisfaction rates with both approaches. Safety of early abortion is high—less than 1% experience a serious complication. The risk of complications increases with advancing gestational age (GA). Uncomplicated abortion preserves future fertility.
Research consistently indicates PWECP lack understanding about fertility, teratogenicity of ASMs, contraception and related drug interactions. Providers caring for PWECP must understand how to provide either an effective contraception or an appropriate referral. The consequences of unplanned pregnancy can be severe: patients face a higher risk of morbidity and mortality which is complicated by the lack of specialized obstetric providers for persons who have epilepsy. In states with the most extreme bans, neither a medical condition such as epilepsy nor a fetal anomaly due to ASM exposure constitute eligible exceptions for an abortion. Persons with epilepsy can obtain information on how to access safe and affordable abortion care through the National Abortion Federation Hotline.
Contraception in Persons With Epilepsy of Childbearing Potential
Persons with epilepsy of childbearing potential, like those in the general population, have better maternal and fetal outcomes if the pregnancy is planned. Effective contraception is necessary and integral to planning pregnancy and reducing maternal and fetal adverse consequences including fetal malformations, intra-uterine growth restriction, and adverse cognitive outcomes. 6 -11 Multiple contraceptive methods with variable effectiveness are available (Table 1). The most effective contraceptive methods include vasectomy, tubal ligation, intrauterine devices (IUDs), and implants. Together, IUDs and implants are classified as long-acting reversible contraception (LARC). Studies find that PWECP are not using methods considered to be highly effective. 4,12,13 Sixty-three percent of PWECP in a nationwide health care claims database either used no contraception or contraception other than tubal ligation, LARC, or hormonal contraception, a higher percentage than in persons with 21 other medical conditions. 13 There is an increased risk of unplanned pregnancy with ineffective contraception use, a finding demonstrated among PWECP. 4,5 Barriers to effective contraception include confusion among health care providers about potential interactions of contraception particularly hormonal contraception with ASMs. 14 Bidirectional interactions between ASMs and hormonal contraception exist (Tables 1 and 2). Cytochrome P450 enzyme inducers increase the metabolism of reproductive hormones in hormonal contraception, increasing risk of contraceptive failure and pregnancy. In contrast, estrogen-containing hormonal contraception accelerates the glucuronidation pathway, the main metabolic pathway for lamotrigine and to a lesser extent valproic acid resulting in lower concentrations of these ASMs and a potential increased seizure risk. Notably, there are no reported interactions between IUDs and ASMs. 15 In the current climate, it is increasingly important that we as neurologists know about effective contraceptive methods and the potential interactions between these methods and the ASMs we prescribe. Counseling PWECP about effective contraception should be an integral part of the care we provide.
Birth Control Methods and Potential Interactions With ASMs.
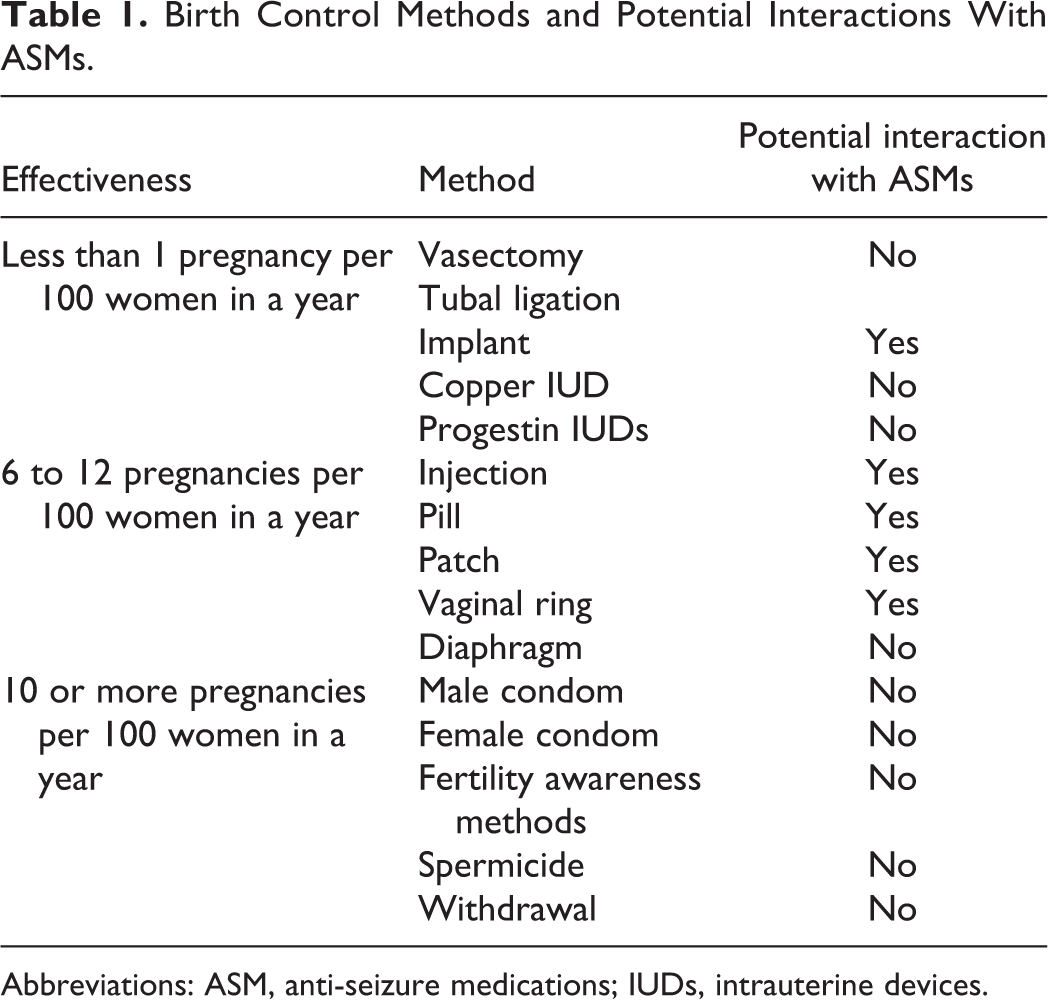
Abbreviations: ASM, anti-seizure medications; IUDs, intrauterine devices.
Interactions Between ASMs and Combined Oral Contraception (COC).
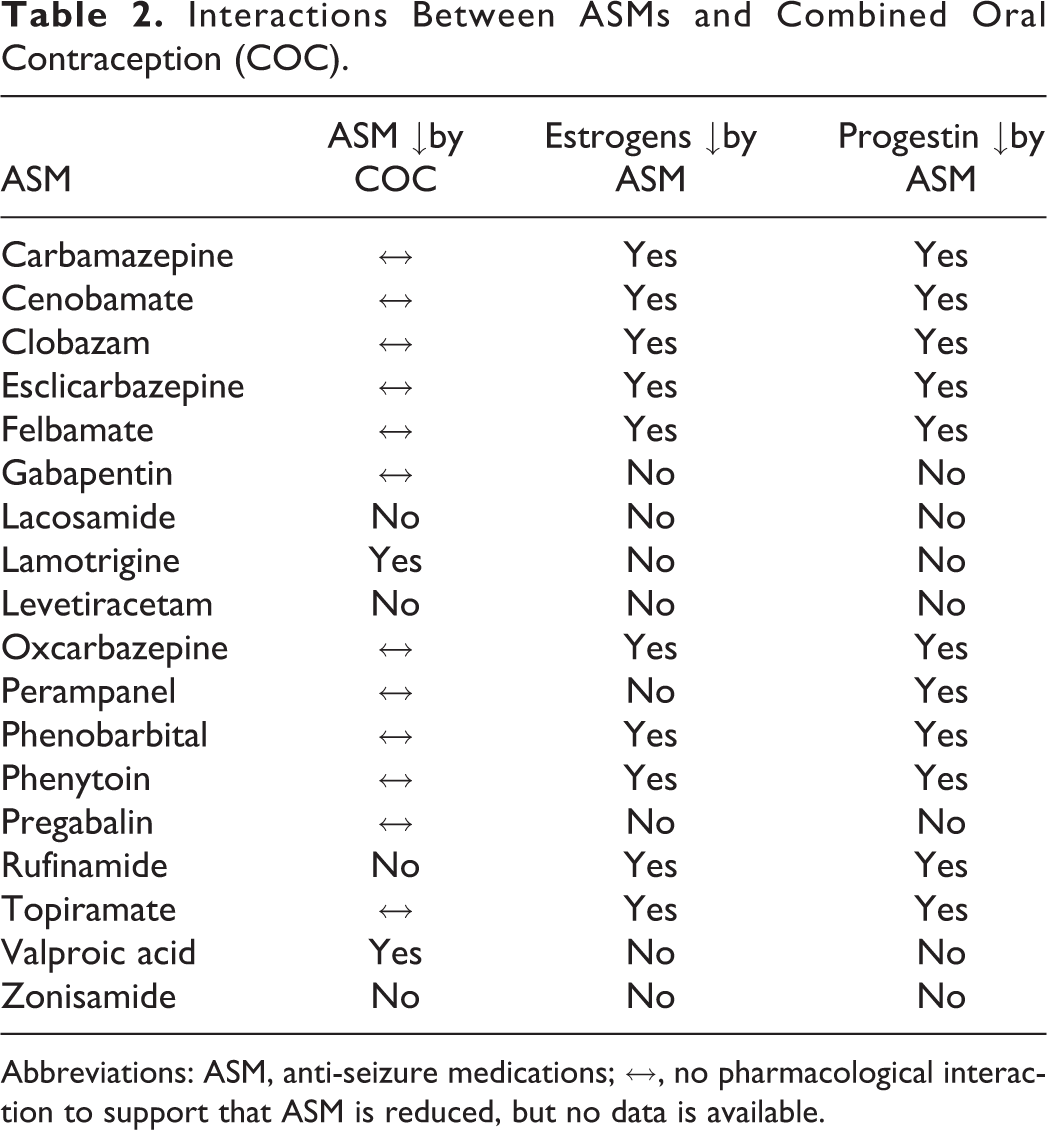
Abbreviations: ASM, anti-seizure medications; ↔, no pharmacological interaction to support that ASM is reduced, but no data is available.
Impact of Anti-Seizure Medications on Teratogenicity and Adverse Neurodevelopmental Outcomes
The risk of major congenital malformations (including neural tube, cardiac, and urogenital defects) among children born to PWECP is increased by many ASMs. 16 This risk is greatest with valproic acid. 9,17 -19 The risks associated with valproic acid are dose-dependent. The risk of major congenital malformations with 500 to 700 mg or less per day of valproic acid approach the risk seen with high doses of lamotrigine (i.e., at least 300-300 mg per day). 17,18,20 Levetiracetam, lamotrigine, and oxcarbazepine are associated with the lowest risk of major congenital malformations. 9,18,19
More recent data shows that ASMs can impact neurodevelopmental outcomes (including intellectual quotient and traits for autism spectrum disorders) in the children of PWECP. This is most evident for valproic acid 8 but there is evidence for similar effects with topiramate. 21
Despite these risks, there are circumstances where valproic acid remains an unavoidable ASM choice in some PWECP. The SANAD I and II trials have demonstrated that on average valproic acid is the most effective ASM in treating generalized epilepsy, superior to lamotrigine, topiramate, and levetiracetam. 22,23 Withdrawal of valproic acid, or changing to another ASM, after the onset of pregnancy is associated with an increased probability of recurrence of generalized tonic–clonic seizures, a risk that may be greater than 30%. 24
Folic acid may protect against some of the risks associated with gestational exposure to ASMs. An older randomized clinical trial (RCT) of people of female sex from the general population demonstrated that folic acid decreases the live-birth prevalence of neural tube defects by 50%. 25 These benefits have never been shown in PWECP. 9,17,26 There is evidence that periconception folic acid is associated with a mean 5.9 point increase in the full scale intellectual quotient at age 6 years among children born to PWECP. 27 Another study of 335 pregnancies with exposure to an ASM reported an 8-fold increased odds of autistic traits at age 36 months among children to exposed to folic acid supplementation during pregnancy, and that this effect was greatest with greater plasma concentrations of folic acid in the pregnant person. 28 A recent analysis of more than 27 000 pregnancies among PWECP, on the other hand, demonstrated that folic acid supplementation greater than 1 mg per day was associated with a close to 3-fold increase in the instantaneous risk of childhood cancer (although the absolute risk remained less than 2%). 29
Recognizing that some ASMs, notably valproic acid may have increased negative pregnancy outcomes is necessary to consider when treating PWECP. Many PWECP in the United States will now have limited options should they be faced with adverse consequences of ASM treatment in pregnancy.
Perinatal Counseling
Pediatric epileptologists may encounter a unique situation as it relates to fetal evaluations. Many prenatal neurologic genetic and structural abnormalities, such as tuberous sclerosis complex or hemimegalencephaly, are highly comorbid with epilepsy. Pediatric epileptologists and neurologists who participate in prenatal counseling must be aware of their specific state’s regulations and that options for pregnant persons may be limited. With advances in prenatal genetic screening, genetic anomalies such as aneuploidies can be detected earlier at 14 week GA although false negatives are still possible. 30,31 However, microarray abnormalities and single gene disorders will not arise on more routine testing and only be discovered once structural abnormalities appear on fetal ultrasound in the second trimester prompting further genetic evaluation. 32
In addition, most significant structural abnormalities are still not detected until after 20-weeks’ gestation. Of these structural causes, neurologic etiologies are the most common. 30 Due to the inherent technical and timing limitations for these to appear on fetal imaging, termination is not an option for many pregnant persons based on their state of residence. Eighteen states have an abortion ban at or before 20 weeks’ gestation. Of these, 13 have a complete ban at any GA, and 4 have an exception for lethal-only fetal anomalies. 33 Additionally, this sensitive window of time of detecting a fetal abnormality must account for the time required for parents to schedule this consultation, undergo additional testing and then make informed decisions. Thus, families in some states will find the window of time to make a decision has ended. 31
Despite earlier genetic testing, many pregnancies affected by a significant genetic or structural abnormality occurring in states with complete bans will restrict the options of the pregnant person as to continuation or termination. Epileptologists along with their pediatric colleagues who partner in the care of children with complex medical needs—orthopedic surgeons, neurosurgeons, and many others—must prepare for an increased need in the wake of a preexistent protracted time to evaluation. 34,35
Unique Issues for People of Color
Since the 18th century, the reproductive rights of POC have been controlled by legislation that either compels or punishes childbearing (Figure 1). Of those who have had an abortion, 38% are black, 21% Hispanic, and 33% are white. 36 Black POC have higher rates of pregnancy-related deaths (RR 3.4) compared to non-Hispanic white POC. 37 Racial/ethnic minority groups are more likely to use Medicaid and thus public defunding of abortion access is most likely to target POC. 38 Abortion bans prior to 2020 affected 18.1 million people of reproductive capacity of which 43% were POC. Nearly half of all Indigenous Americans/Alaskan Natives live in a state with abortion ban laws. 38 Maternal mortality rates are higher in those states with restrictive abortion statuses among all racial groups. 39
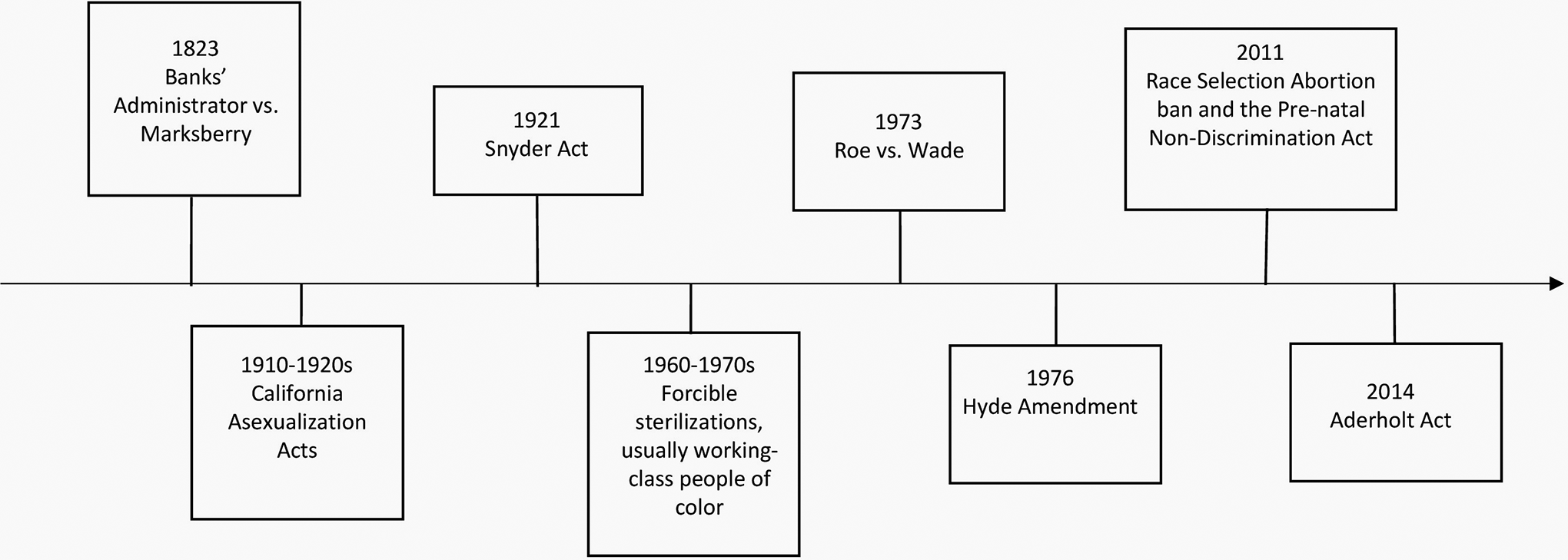
The affirmation of ownership of Black women and their future offspring was affirmed in Banks’ Administrator vs. Marksberry (1823). Eugenic movements in the 20th century to control the population of people of color (POC) included the California Asexualization Acts which targeted Blacks and Mexican peoples as well as the forced sterilization procedures in the 1960s and 1970s that targeted working class and poor people, usually POC, under threat of termination of welfare benefits or denial of medical care. Native American, indigenous POC were granted healthcare under the Snyder Act of 1921, however they were unable to obtain access to abortion due to the 1976 Hyde amendment which prohibited abortion using federal dollars despite Roe vs. Wade decision in 1973 which gave access to others. Passed in 2014, the Aderholt Act prohibits federal funding for abortion services to those people held in detention centers despite higher levels of sexual assault and limited medical care.
In other countries with prohibitive abortion laws, there are known increases in maternal mortality due to complications of self-abortion and increased reporting and prosecution of people who may present with miscarriages rather than self-induced abortions. 40 Similarly, in the United States, of the cases that have been investigated and prosecuted for self-managing or helping someone obtain an abortion, charges are more likely to be seen in POC compared to non-Hispanic whites. 41 People of color and sexual/gender minority people face greater challenges accessing reproductive healthcare. Awareness of restrictive abortion laws should be taken into clinical context when counseling people with epilepsy, regardless of race, ethnicity, and sexual/gender preference about contraception, pregnancy, and malformation rates with ASMs.
Conclusion
As the landscape of reproductive care grows increasingly complicated due to lack of federal protection for abortion, it has become more important that we provide informed and comprehensive care to our patients with epilepsy who are particularly vulnerable to the impact of this legislation on their reproductive decision-making.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.