
Abstract
The cost-effectiveness and benefit of many diagnostic tests used in the presurgical evaluation for persons with epilepsy is for the most part uncertain as is their influence on decision-making. The options we have at our disposal are ever increasing. Advanced imaging modalities aim to improve surgical candidacy by helping us better define the epileptogenic zone and optimize surgical planning. However, judicious use is important. Randomized controlled trials delineating which mode of investigation is superior are lacking. Presurgical tests do have incremental value by increasing surgical candidacy and refining surgical planning. The yield of additional imaging will increase with complex localization. However, every case must be tailored by hypothesis, cost, and accessibility. Future studies using a quantitative cost–benefit framework are needed to determine the cost-effectiveness of advanced diagnostic tests (beyond magnetic resonance imaging) in the presurgical evaluation of those with epilepsy.
Introduction
This review is a recount of the debate at the Annual Course at the American Epilepsy Society 2018 Meeting in New Orleans, Louisiana. This symposium aimed to examine the cost-effectiveness of advanced diagnostic technologies as well as discuss the knowledge gaps and future directions in the presurgical evaluation of those with epilepsy. The focus of this narrative review is on the cost-effectiveness of these tools in those undergoing a presurgical evaluation rather than their accuracy or concordance with other clinical data. The challenges related to determining the cost-effectiveness of various diagnostic technologies for epilepsy surgery are also discussed.
Discussion
The etiology of epilepsy is multifaceted and, in many patients, remains unclear. Identifying the cause of epilepsy is a fundamental component in the clinical management of such patients. In recent years, new diagnostic modalities have revolutionized our capacity to investigate and identify the underlying causes of epilepsy. Classically, imaging along with electroencephalography (EEG) has been the fundamental tool in the workup of those with epilepsy, as successful treatment of epilepsy, particularly drug-resistant epilepsy, is governed by how accurately the epileptogenic zone is identified. 1 All patients with epilepsy should undergo magnetic resonance imaging (MRI) as a first step to assist in establishing the cause of their epilepsy and to attempt to determine whether there is a lesion associated with their epilepsy, since the identification of an associated lesion is associated with greater odds of seizure freedom after surgery. 2
Resective surgery is the gold standard for the treatment of focal drug-resistant epilepsy in appropriately selected patients. 3 -5 Seizure freedom can be achieved for significant proportion of patients; the number needed to treat with surgery for 1 additional patient to become seizure-free is 2. A randomized controlled trial (RCT) comparing medical treatment to early surgery in those with temporal lobe epilepsy (TLE) found 64% of patients in the surgical arm were seizure-free in the first year of follow-up versus 8% in the medically treated arm. 3 Long-term outcomes are also good with 10-year follow-up studies showing that 50% to 60% of those who undergo TLE resection, and 30% to 40% of those who undergo frontal lobe resection remain seizure-free. 6 -8 Thus, it is critical to identify ideal surgical candidates. The success of surgical resection is dependent on localization of the epileptogenic zone and complete resection of known epileptogenic cortex. Surgical failure is more common in cases of contralateral hippocampal sclerosis, remnant ipsilateral hippocampus, or temporal-plus epilepsy (extension to insula, orbitofrontal region, operculum, and temporoparietal junction, even extension into extratemporal components of the limbic network and thalamus). 9 -11 Advanced imaging is performed in order to help determine surgical candidacy and improve the presurgical identification of the epileptogenic zone. Such processes ultimately aid in surgical planning to guide the placement of intracranial electroencephalography (iEEG) electrodes, the extent of resection needed, placement of responsive neurostimulation device, or determine whether other surgical approaches may also be considered (eg, later interstitial thermal therapy [LITT] and deep brain stimulation [DBS]). The benefit of advanced diagnostic technology depends not only on its diagnostic accuracy but also on how the results impact subsequent treatment decisions as well as the final clinical outcomes (eg, seizure control and safety) and economic benefits. 12 The RCTs delineating which mode of investigation is superior are lacking. A recent meta-analysis using epilepsy surgical data from the 3 RCTs on TLE in adults as well as class II data from prospective studies found remarkable concordance at approximately 70% seizure freedom across studies. 13 As future RCTs with TLE will continue to have recruitment challenges, this may act as a reasonable historical control for future surgical therapies (eg, LITT).
The options we have at our disposal are ever increasing. Nuclear medicine techniques that determine metabolic, in vivo perfusion, and neurotransmission changes associated with a seizure, although not used in the primary diagnosis of new-onset epilepsy, have afforded essential functional data in the presurgical evaluation of drug-resistant epilepsy. Nuclear medicine imaging modalities are particularly beneficial if the MRI is nonlesional or exhibits multiple lesions or if EEG changes are discordant with structural imaging. Positron emission tomography (PET) and single photon emission computed tomography (SPECT) are also helpful when interrogating the remaining functional integrity of the brain in these patients. Other noninvasive imaging techniques such as simultaneous recording of functional magnetic resonance imaging and EEG (EEG-fMRI), magnetic source imaging (MSI), and magnetoencephalography (MEG) can be useful in defining the epileptogenic zone. 14,15 These investigations however are expensive (eg, high equipment costs) and typically labor-intense with much expertise needed.
The Challenges of Evaluating the Cost of Epilepsy Diagnostic Technologies
There are challenges in evaluating the cost of epilepsy technologies. It is important to keep in mind that >85% of the world’s 50 million people with epilepsy live in low-resource countries, where many diagnostic and therapeutic options are not available. There are limited facilities and personnel, implementation of new technologies in these regions may not be financially or practically feasible, and competition for resources and allocation is often based on political decisions. A Health Technology Assessment report on neuroimaging modalities used to identify a seizure focus in drug-resistant epilepsy was first published in 2006 and updated in 2010. These reports identified that there remained a lack of accuracy and cost-effectiveness studies linking test results, management, and clinical outcomes in the presurgical evaluation of those with epilepsy. 16,17 Limitations of existing studies include the fact that most studies only include operated patients, the follow-up is often short with small sample sizes, and there is a lack of detailed cost analysis (eg, direct, indirect, and intangible costs).
Do we know the true cost-effectiveness of diagnostic technologies for epilepsy surgery? Not really. An ideal pathway in the presurgical workup for epilepsy that weighs the benefits, risks, and costs associated with advanced diagnostic technologies is necessary. Limited research has been conducted investigating the clinical effectiveness and cost-effectiveness of advanced imaging studies used to visualize the seizure focus in people being considered for epilepsy surgery. 18 This may be partly due to the challenges of assessing the cost of an additional mode of imaging with minimal consensus on analytical techniques. It is also difficult to attribute the benefit of an additional diagnostic test to long-term outcomes. As there are levels of evidence for therapeutic studies, a hierarchy in diagnostic research has been proposed. 19 -21 At the lower end of the hierarchy, studies tend to evaluate diagnostic performance, while at the higher end clinical- and cost-effectiveness are appraised. 22 The following elements have been proposed when evaluating the cost-effectiveness of diagnostic tests (Table 1): (1) the test characteristics, that is, the parameters that determine the accuracy, sensitivity, specificity, and predictive values of the tests; (2) a robust knowledge about the clinical value of the test, that is, additional information from the test in sequence, rather than in isolation is required; (3) the clinical outcome is vital to the overall evaluation that is, the justification to do it is not for direct test results but potential access to surgery; and (4) the cost-effectiveness analysis is the only appropriate way to be able to combine all the information collected in the first 3 steps. 21
Hierarchy in Diagnostic Research.a
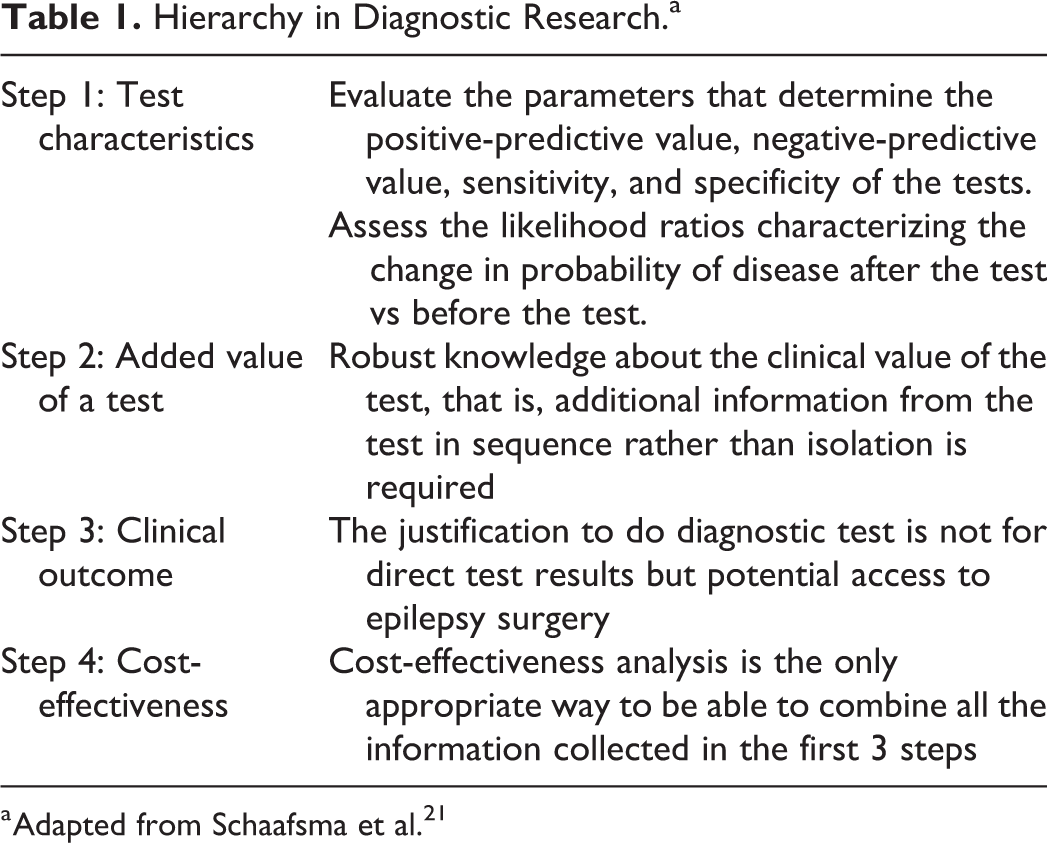
a Adapted from Schaafsma et al. 21
Positron Emission Tomography
The abovementioned framework was applied to PET in a systematic review on clinical and economic benefits of diagnostic testing for TLE surgery, when video-EEG (vEEG) and MRI are non-localizing or discordant. Fluorodeoxyglucose (FDG)-PET + iEEG after discordant or nonlocalizing vEEG and MRI “appear” cost-effective but only if the benefits are sustained in the long term. 12 Added value is inextricably linked to the decision to proceed to surgery and cost-effectiveness, particularly when used in patients with nonlocalizing or nonconcordant vEEG/MRI. 23,24 Limitations to this study include the limited assessment to vEEG and MRI alone, use of FDG-PET alone, and use of FDG-PET and iEEG. Although showing promise, this study is still an oversimplification of the wide range of diagnostic modalities available to clinicians. 12 Another FDG-PET study examined whether FDG-PET substantially altered decision-making in drug-resistant epilepsy and found that there was greater concordance with TLE than with extra-TLE (78.0% vs 28.6%, P < .001). One-third of the patients were selected for resective surgery based on PET, and associated costs escalated by 13.0% when PET was used (unless iEEG was avoided). Positron emission tomography when applied judiciously remained a supplementary tool in the surgical selection of one-third of patients with drug-resistant partial epilepsy; however, its application as a separate tool was not as promising. 25
Single Photon Emission Computed Tomography
Cost-effectiveness data about additional diagnostic modalities (eg, SPECT or MEG) in the presurgical evaluation of epilepsy are scarce. This explains partially why these tests are not ordered at once but rather serially, since the added value diminishes with each test, especially if one already gives reasonable localizing information. A recent study from the United Kingdom looked at the relationship between MRI, EEG, and SPECT and the probability of a child being offered epilepsy surgery. 26 The study included 353 children discussed at presurgical multidisciplinary rounds of which 236 were offered surgery. It showed that MRI and EEG were independently useful in identifying children with localized seizure onset. The proportion of children offered surgery with a single lesion on MRI was 92% (95% confidence interval [CI]: 88%-95%), and EEG did not modify decision-making in such cases (P < .001). In children who had bilateral MRI changes or normal scans, surgery was offered in 78% of those with localized EEG onset versus 9% with nonlocalized onset (P < .001). Magnetic resonance imaging provided the most powerful data for surgical planning, while SPECT did not appear to systematically influence decision-making in any group. 26 In a Spanish study that looked at 34 consecutive patients with interictal brain SPECT abnormalities when the seizure focus was identified with vEEG or MRI brain, SPECT did not offer any additional information regarding surgical decision-making. 27 Although unlikely to provide additional information in some patients, SPECT can be useful in selected groups of patients, especially in those with lesional TLE with nonlocalizing ictal data and in those with dual pathologies. 28 Single photon emission computed tomography is costly with radiotracers having short half-lives and the fact that multiple fillings are usually needed for a successful SPECT completion. One also requires the presence of an EEG technologist and/or a trained nurse to ensure timely injection of radiotracer.
Magnetoencephalography
When standard noninvasive diagnostic tests cannot sufficiently localize the potential epileptogenic zone, additional ancillary tests are necessary. A cost-utility study analyzed MEG use to inform intracranial electrode placement in those with drug-resistant epilepsy and found that it was not cost saving. 29 However, this study had several limitations. Although peer-reviewed literature was used to inform the model, most studies were of small sample size, and no RCTs existed. Many factors can influence surgical outcomes including the diagnostic technologies available for surgical planning, the skill and experience of the diagnostic and surgical teams, and the etiology of the epilepsy. The authors went on to acknowledge that the study likely overstated the effectiveness of MEG by attributing diagnostic yield of FDG-PET and SPECT to MEG. 29
Functional Magnetic Resonance Imaging
Other modalities are increasingly being utilized in the presurgical evaluation of epilepsy. The American Academy of Neurology published a practice guideline in 2017 on the use of fMRI for the presurgical evaluation of epilepsy. 30 A systematic review looking at the diagnostic accuracy of fMRI, amobarbital testing, MEG, functional transcranial Doppler (fTCD) sonography to predict memory and language outcomes after surgery found that the overall quality of the evidence was very low. 15 Meta-analyses of the diagnostic accuracy of fMRI, MEG, and fTCD were not feasible due to small number of studies. Only the diagnostic accuracy of amobarbital to predict memory outcome could be evaluated, yielding a sensitivity of 0.79 (95% CI: 0.67-0.92) and specificity of 0.65 (95% CI: 0.47-0.83). It was also noted that high variability existed between protocols, stimuli, neuropsychological testing, and assessments of language and memory function. 15
Conclusions
The cost-effectiveness of many diagnostic tests used in the presurgical evaluation for persons with epilepsy is for the most part uncertain as is their influence on decision-making. However, lack of high-quality evidence does not equate to lack of cost-effectiveness. There is a need to examine the cost-effectiveness of diagnostic tests in everyone who has a test, not just those who undergo surgery, as there would be an inherent selection bias. Studies examining which advanced imaging and EEG modalities effectively contribute do decision-making and improve surgical outcomes in epilepsy are also warranted. More high-quality studies addressing the cost-effectiveness of newer presurgical investigations are needed.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: EF Chang is funded by the US National Institutes of Health grants R00-NS065120, DP2-OD00862, and R01-DC012379, and the Ester A. and Joseph Klingenstein Foundation. CS Kwon is funded by the Leon Levy Fellowship. N Jette receives grant funding paid to her institution for grants unrelated to this work from NINDS (NIH U24NS107201, NIH IU54NS100064) and PCORI. She also receives an honorarium for her work as an Associate Editor of Epilepsia.