
Abstract
Sudden unexpected death in epilepsy (SUDEP) is the leading cause of death in patients with refractory epilepsy. Likely pathophysiological mechanisms include seizure-induced cardiac and respiratory dysregulation. A frequently identified feature in SUDEP cases is that they occur at night. This raises the question of a role for sleep state in regulating of SUDEP. An association with sleep has been identified in a number of studies with patients and in animal models. The focus of this section of the Sleep and Epilepsy Workshop was on identifying and understanding the role for sleep and time of day in the pathophysiology of SUDEP.
Introduction
Sudden unexpected death in epilepsy (SUDEP) is defined as the sudden, unexpected, witnessed or unwitnessed, nondrowning death of a person with epilepsy with or without evidence of a seizure and in whom postmortem examination does not reveal a structural, infectious, or toxicological explanation for the death. 1 Sudden unexpected death in epilepsy is the leading cause of mortality in patients with refractory epilepsy. 2 Sudden unexpected death in epilepsy is second only to stroke in years of potential life lost to neurological disease, making it an important public health problem. 3 A consistent feature among SUDEP cases is that it frequently happens at night. 4 This has led to it being associated with sleep, since humans sleep during the night. 5 Indeed, a recent large meta-analysis has demonstrated across a number of studies in many different settings that SUDEP happens most often during the night and likely during sleep. 6 The purpose of this portion of the Sleep and Epilepsy Workshop (SEW) was to review associations between SUDEP and sleep, to identify gaps in knowledge (Table 1), and determine pathways forward for research and prevention (Table 2).
Gaps.
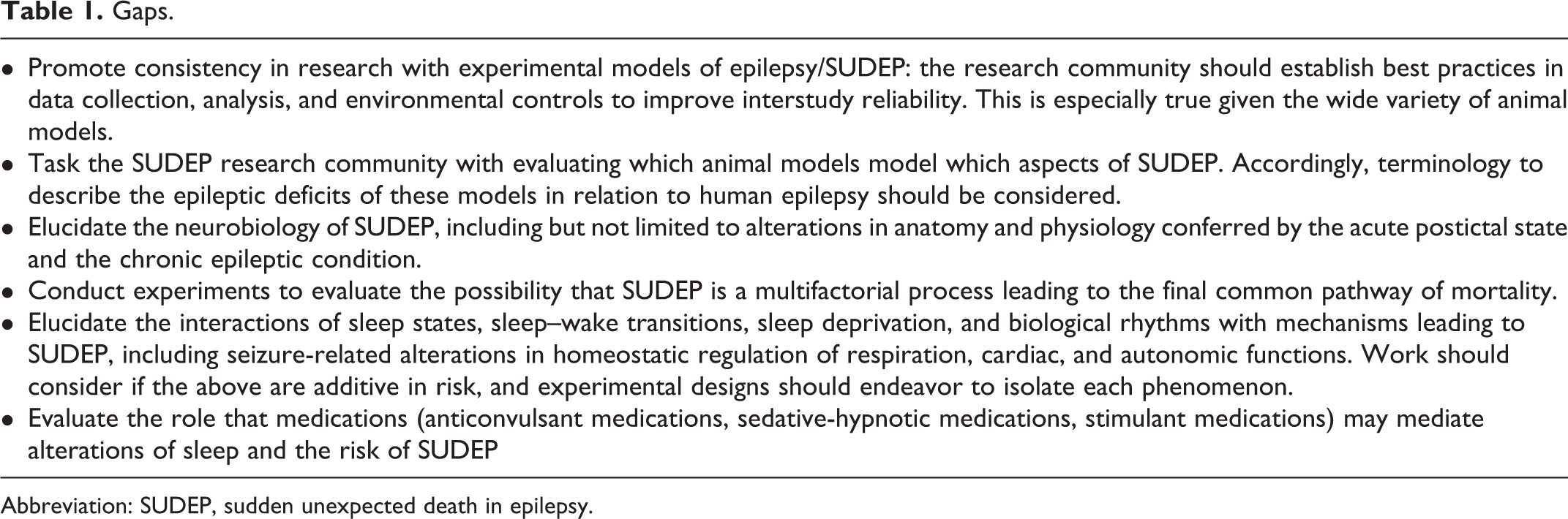
Abbreviation: SUDEP, sudden unexpected death in epilepsy.
Barriers.
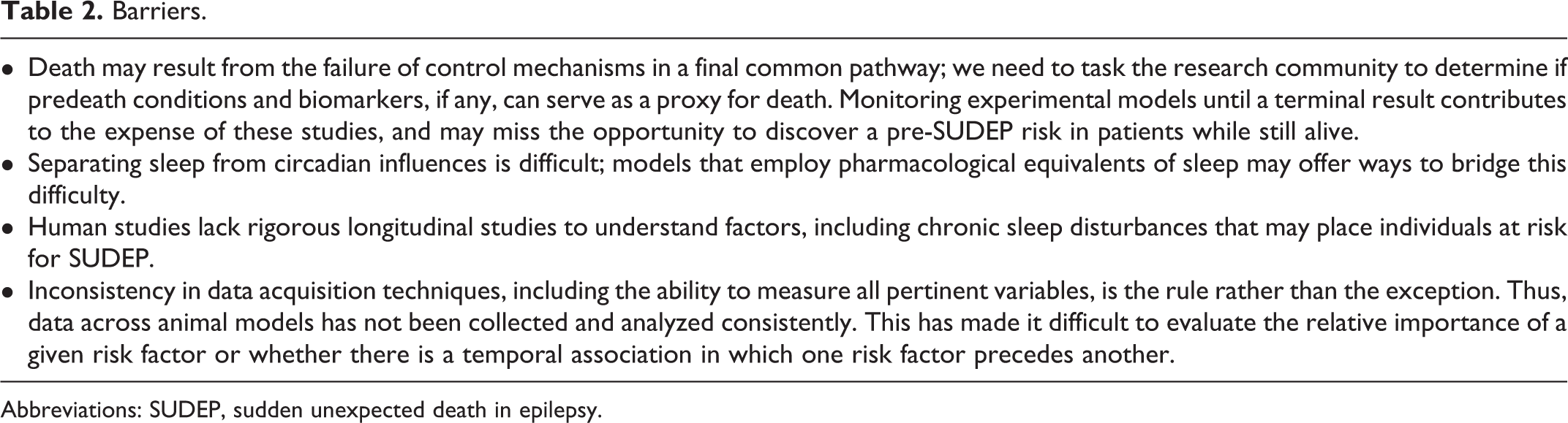
Abbreviations: SUDEP, sudden unexpected death in epilepsy.
Clinical Perspectives on SUDEP and Sleep–Wake State
Clinical interactions between sleep and SUDEP have been largely gleaned from retrospective case accumulations that unfortunately lack direct evidence of sleep status at the moment of SUDEP, and in most of these, the location of the deceased stands as a proxy for sleep. For example, in one of the first reports, 42 of 140 deaths in one epilepsy center were probable (no autopsy) or definite (with autopsy) SUDEP. 7 Of the 42 deaths, many of those that were presumed to have occurred during sleep were simply found in bed. 7 Other reports confirmed that more cases of SUDEP occur in bed again surmising that SUDEP occurred during sleep. 8,9
Nighttime occurrence has been thought to be a proxy for sleep as well. 10 A refinement designated cases that occurred during the night in which the victim was found in or near bed to have occurred during sleep. 10 For instance, death occurring near beds during the night was associated with the death occurring during sleep in a large, recent meta-analysis in which 69% of 1025 cases gathered from 67 studies were said to have occurred during sleep. 6 It is notable to consider that such a high percentage of SUDEP occurs during sleep, when only about a third of a 24 hour day is spent asleep.
In addition to occurring more often during sleep, the majority of SUDEP patients are found in the prone position. 6,11 Many feel that one of the factors contributing to SUDEP risk during sleep is sleeping position, analogous to risk in sudden infant death syndrome that has led to recommendations to mitigate risk with supine sleep. 12,13
To better evaluate the circumstances of death in epilepsy patients, the Mortality in Epilepsy Monitoring Units Study (MORTEMUS) consortium was formed to retrospectively evaluate SUDEP cases that occurred in epilepsy monitoring units. 14 In this study, 14 of the 16 deaths occurred during the night. Of the 10 for which there was adequate data to determine sleep–wake state, 7 occurred during sleep. In all cases for which there was sufficient physiological monitoring, respiratory activity (which, in these cases, was assessed via post hoc video review) ceased prior to cessation of cardiac activity. 14
The importance of respiratory compromise during sleep is supported by the occurrence of acute peri-ictal apnea. Apneas can be ictal or postconvulsive. The latter can be seen in association with post-ictal generalized EEG suppression and had been implicated as a contributing factor to SUDEP. 15 Although little evidence has linked comorbid sleep apnea with SUDEP in patients with epilepsy, it is well established that seizures frequently lead to obstructive and central apneas. Respiratory arrest is a major putative etiological mechanism for SUDEP. 15 Not only may position and ictal rictus cause respiratory compromise, ictal involvement of key supratentorial regions—namely amygdala—may be an important contributor of respiratory arrest leading to SUDEP during sleep. Two studies in awake patients with epilepsy demonstrate that amygdala stimulation causes respiratory cessation that is not noticed by the patient. 16 -19
Basic Science Perspective: Links Between Death, Seizures, Sleep–Wake State, and Circadian Rhythms
Several experimental animal models of epilepsy, in which animals often experience high rates of death, feature sleep, or circadian disruptions. 20 No particular mechanistic links have been elucidated, but the phenomenology of interactions between death, seizures, and abnormalities in sleep and circadian behaviors forms a fascinating and rich collection which we summarize below.
The pilocarpine temporal lobe epilepsy model has a high incidence of death from seizures 21 and displays dysregulated circadian rhythms. 22,23 Similarly, another spontaneous seizing mouse model with a high incidence of seizure-related death, the Kcna1-/- mouse, also displays dysregulated circadian rhythms. 24
Many animal models of epilepsy have impaired sleep architecture, marked by more time awake and less time in non-rapid eye movement (NREM) and rapid eye movement (REM) sleep than normal, or unstable, interrupted sleep, and possibly leading to overall chronic sleep deprivation. 24 -27 These differences are more profound in the absence of light-dark cues. 23,24,27 -29
In most of the above models, circadian abnormalities, especially in behavioral activity, have been observed. Seizures can even reset circadian rhythms. 30 Circadian function is important, as it facilitates or inhibits sleep depending on the biological clock’s “time of day.” In this light, the growing literature exploring the genetic components of the biological clock shows that clock abnormalities are common in experimental epileptic animals. For example, Clock gene expression is reduced in rats subjected to pilocarpine status epilepticus 22 and in Kcna1-/- and Scn1a-/- 25 mice, a model of Dravet syndrome that has a high incidence of SUDEP. Notably, in the pilocarpine treated rats, clock expression does not decrease until the animals display spontaneous seizures. 22 Taken together, this suggests that reduced clock expression contributes to hyperexcitability. Indeed, reducing clock expression in excitatory neurons increases behavioral activity and leads to spontaneous seizures. 31 Notably, there is reduced expression of several circadian clock genes, including clock and period, in brains of patients with tuberous sclerosis. 31
Outside the field of epilepsy, partial chronic sleep deficiency is associated with cardiovascular problems, respiratory problems, and early mortality. 28 Interestingly Kcna1-/- mice display a progressive cumulative sleep deficiency that increases just before death, 28,29 suggesting a role for sleep deprivation in contributing to fatality risk. This suggests chronic sleep deficiency may contribute to a pre-SUDEP pathophysiology that increases the likelihood of death. 32
Sleep itself affects seizure occurrence in that NREM can promote and REM sleep can inhibit seizures. 33,34 Although rarer, seizures during REM sleep may confer disproportionate mortality. Acute seizures induced via maximal electroshock are associated with seizure-induced respiratory arrest 35 ; all seizures induced during REM sleep were fatal in this model. 36,37 While it is generally thought that seizures during REM sleep occur infrequently in humans and many rodent epilepsy models, they are frequent in some rat models. 38,39 There are differences in EEG theta activity between humans and rodents which may confer some of the differences in assigning seizure propensity to a given sleep state. Several lines of evidence indicate that changes in theta are important in gating seizures. 39 -41 Given that several induced and genetic epilepsy models that have high mortality also demonstrate impaired sleep architecture, perhaps disruption of the natural gating mechanisms provided by sleep contributes to seizure-induced death.
Center for SUDEP Research
In 2015, the NIH/NINDS funded the Center for SUDEP Research (PIs Samden Lhatoo and Jeffrey Noebels), a multidisciplinary “center without walls” that supported 9 projects spanning 14 institutions, aimed at understanding SUDEP from both a basic science and clinical perspective. The Center not only evaluated the role for sleep and circadian rhythms in epilepsy-related mortality but also provided a valuable demonstration of how a multicenter collaborative network fostered cross collaboration from individual centers that otherwise may have competed and withheld collaboration. From a clinical perspective, the Center facilitated the capture of physiologically monitored epilepsy cases in the EMU that showed autonomic instability, as well as near-SUDEP and postmortem SUDEP cases for genetic, pathological, histochemical, anatomical, and imaging studies. Basic science projects using genetically defined mouse models, and human induced pluripotent stem cells derived from patients with Dravet syndrome focused on excitability mechanisms in heart and brain that predispose to SUDEP. The infrastructure required consistent collection, curation, and analysis of patient data and shared approaches to model development and testing. Valuable insights into SUDEP pathophenomenology and potential mechanisms were gained, including the role of brainstem spreading depolarization, 42 peri-ictal breathing dysfunction, 15,43,44 imaging biomarkers of risk, 45 -48 and neuropathological evidence of brainstem serotonergic neuronal depletion. 49
It is the SEW participants’ experience with the Center’s consistency in research definitions and techniques that drove many of the SEW’s recommendations for future research. Future proposals for “centers without walls”—especially those that may be proposed for sleep and epilepsy—may draw heavily from this collaborative research scheme.
Summary/Conclusions
The physiological activity that initiates and supports sleep may open chinks in the variety of homeostatic processes sustained by the autonomic nervous system that armor patients against catastrophic failure of these processes. Sleep mechanisms provide a valuable window through which the causes and risks of SUDEP can be evaluated. We hope that the momentum initiated by the SEW promotes research, raises awareness, and improves education in the potential mortal interactions of sleep, biological rhythms, and epilepsy.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Sleep and Epilepsy Workshop was supported in part by a grant from the BAND Foundation.