
Abstract
Introduction:
Occupational health and safety management systems are widely used as a systematic approach to managing occupational health and safety. However, sometimes they are restrictive and underspecified to deal with dynamic workplace demands. Rasmussen used a model of boundaries to conceptualize this dynamic model of safety, where the space of possibilities lay within 3 boundaries and workers used various means to stay within the boundaries to remain both productive and safe at work.
Methods:
This study applied the Rasmussen model of boundaries to understand the factors that formed the boundaries, the gradients, and countergradients in a biomedical laboratory.
Results:
The most central goal was to be the first to publish, and this formed the boundary to scientific output failure; the boundary to unacceptable workload and boundary to functionally acceptable performance were the other 2 boundaries in line with the Rasmussen model. The workers had developed methods (mental risk assessment, teamwork, and experience and familiarity) of working, which ensured they remained productive and safe. This can be described as resilient performance, where resilience is not something that a system has but something it does to adjust their performance when faced with expected or unexpected changes.
Discussion and Conclusion:
A customized portfolio of rule-based non negotiable instructions and a risk assessment–based approach would be best suited for a biomedical laboratory. The workers have learned resilient performance on their own and unknowingly are already practicing this. It is now time to formally incorporate such practices into the safety systems of biomedical laboratories.
Occupational health and safety management systems (OHSMS) are widely used as a systematic approach to managing occupational health and safety in organizations. Such systems typically provide a framework for organizations to develop policies, processes, and procedures to ensure the health and safety of their employees. 1 -3 One of the popular OHSMS is the Occupational Health and Safety Assessment Series (OHSAS), with the British OHSAS 180001 emerging as a very popular system. According to reports in 2009, nearly 56 251 organizations had been certified to this standard, with double the number in 2006. 2,4,5 OHSMS is modeled on the concept of the plan-do-check-act cycle, which is a repetitive cycle to ensure continuous improvement in the organization’s performance—in this case, safety performance. 6,7
The OHSMS method includes prescriptive predefined elements consisting of processes, legal compliance, and standard operating procedures (SOPs), the success of which is predominantly measured by the number of accidents. 8 This adopts the approach that is referred to as the old view of safety or safety I, which is a focus on failure as opposed to the new view of safety or safety II, which looks at what goes right. 9,10 In the medical school where this research was undertaken, between 2017 and 2019, there were 24 minor injuries and no major injuries, and if plotted against the man hours of 2.7 million (approximately 400 workers, 44 hours a week for 3 years), the rate of minor injuries was extremely low. It can be seen more than 99.9% of the time things went right. This is exactly what Hollnagel 10 points out when looking at an illustrative accident rate of 1 in 10 000, where the safety I approach of focusing on accidents will be at the expense of not understating the success rate of 9999 in 10 000 times.
Key elements of the OHSMS are hazard identification, risk assessment and mitigation, and development of SOPs to ensure uniform written safety procedures throughout the organization. Such SOPs have to be aligned to the parent organization and other applicable regulations. 11 -13 While the benefits of uniform SOPs throughout an organization are certainly well recognized, 14 -17 their pitfalls, of being time-consuming and restrictive and reducing individual variation, are also known. 18 -20
Organizations often face multiple goal conflicts that pull or push them in different directions. This will certainly trickle down to the sharp end workers, 21 who, keeping in mind the goal of production, will realize that there are degrees of freedom 22 -25 available to them to perform their tasks and will use these degrees of freedom to adjust their work such that they remain productive despite other constraints such as workload, resource availability, and restrictive safety SOPs. SOPs are not always compatible with the variety of demands placed on a system because they are not created for specific situations and can be restrictive because they cannot adapt to the changing demands that workers often face. 26,27 In practice, SOPs can be found to be unsuited for every situation that practitioners are confronted with, and the diversity of the circumstances or contexts to which they are to be applied: procedures are frequently found to be underspecified in that they are not universally applicable. 27
The need to remain flexible in the face of rapid changes, in both the threat landscape and technology in the field of biological safety, has resulted in a paradigm shift in the approach to biosafety at the World Health Organization (WHO). The WHO Laboratory Biosafety Manual, which is a key resource for the practice of biosafety throughout the world, is now shifting focus to a risk-based, technology-neutral, and cost-sensitive approach in its new edition. The manual, which is to be released soon, will now adopt locally relevant and sustainable solutions with greater emphasis on human factors and worker training rather than on unsustainable and expensively engineered laboratories. The manual recommends that oversight at country and institutional levels should allow flexibility and multiple ways of mitigating risks based on the local conditions at the workplace. 28
Biomedical researchers are under extreme pressure to be the first to publish in high-impact journals, and their entire career and existence depend on this. Publication in highly respected peer-reviewed journals is a matter of prestige not only to the individuals but also for the institutions and is directly related to the amount of funding that the research team and institution can secure. 29 -31
As a result, workers and practitioners develop, through their own local rationality, strategies that sustain performance by applying workarounds and trade-offs.
A dynamic model of safety proposed by Rasmussen 23,24,32 plots this variability in performance due to workers exercising their degrees of freedom in response to the changing demands of the sociotechnical system in which they work. Rasmussen visualized work as being done in the “space of possibilities” 23 within boundaries and likened the “situation-induced variations within the work space to the ‘Brownian movements’ of the molecules of a gas.” 23 Human behavior at work is strongly controlled by goals and constraints that individuals face in their everyday work life. These constraints and goals have to be taken into account when understanding how they work. According to Rasmussen, “aiming at such productive targets, however, many degrees of freedom are left open which will have to be closed by the individual actor by an adaptive search guided by process criteria such as work load, cost effectiveness, risk of failure, joy of exploration, etc.” 23
Rasmussen’s dynamic model of safety describes a system’s operating point (OP) within a space of possibilities bounded by 3 boundaries: boundary to economic failure, boundary to unacceptable workload, and boundary of functionally acceptable performance. Crossing the boundary of functionally acceptable performance can lead to an accident. The OP is the point in the space within the boundaries where the system or person performs the work. This model is a descriptive one, and the location of the OP will shift constantly and will be difficult to locate exactly. In addition, gradients and countergradients move the OP away from or toward a boundary based on the day-to-day factors in the workplace (eg, production pressure, manpower shortage). 33 Workers must avoid crossing not only the boundary of functionally acceptable performance (crossing this may result in an accident) but also the boundary to economic failure and boundary to unacceptable workload to remain with the space, thus being productive and safe at the same time. Therefore, recognizing and understanding the boundaries and gradients will give workers the opportunity to anticipate and avoid moving past any of the boundaries, as well as to recover from an unsafe to a safe state 34 —in other words, build resilient performance.
Resilience is understood differently in different fields but generally can be defined as the reactive or proactive capacity of a system to adapt and bounce back. 35 -45 Resilience is not a characteristic relevant just to safety; it is crucial that individuals and organizations remain productive and safe, with safety being entwined with the business of the organization. Resilience is thus a characteristic that is able to cope with complexity and is able to avoid both safety and productivity failures. 45 -48
The Rasmussen model of boundaries has been applied to study resilience in the way emergency department staff adjusted to surges in patient volume. The authors explain that knowing where the OP is in relation to the boundaries, especially of the functionally acceptable performance, requires both the organizations and its workers to develop a “keen awareness of its operations and variability in performance.” 49 Nemeth et al 49 explain how emergency department staff coped by using known and newly thought-out methods in unusually difficult situations to gain control. It is through understanding the goal conflicts and methods used to address them that effective improvements can be planned.
Rasmussen’s model of boundaries has also been used to measure resilience in the Dutch railway system. 50 The authors describe 3 boundaries and related pressures (gradient) that would affect the OP as economic boundary/performance pressure, workload boundary/least effort pressure, and safety boundary/safety pressure. They have attempted to plot the location of the OP in relation to the boundaries using quantifiable data and, by viewing the model from above, have plotted a slope to measure resilience.
While the idea of projecting the definition of resilience onto Rasmussen’s model of boundaries has been attempted, as shown in the examples above, this has not been attempted in a university biomedical laboratory. Research teams are most challenged with production pressure when working with novel ideas and material, because they want to be the first to publish. While publications are the main indicators of performance, safety is something that they have to bear in mind constantly, because 1 major lapse can end their careers. A good example of such an occurrence is at the University of California, Los Angeles, where a 23-year-old research assistant died as a result of severe burns while working with a liquid called tert-butyllithium. The principal investigator’s (PI’s) stellar career suffered a great blow and the university spent US$4.5 million defending him. 51 (Principal investigator refers to the head of the laboratory or research team who is responsible for proper and ethical conduct of the research and is the holder of research grants and the lead researcher for the research project.)
Today, in a biomedical laboratory, competence is not dependent entirely on formally acquired knowledge but also on heuristic know-how and practical skills acquired through experience, which allows workers to act quickly and effectively to prevent a harmful incident. Do the degrees of freedom available to biomedical workers allow them to anticipate and avoid failure, thus making them resilient? In an attempt to answer this question, this project turns to Rasmussen 23 , who pointed out, in 1997, that the workplace is very dynamic with changing risks and that the behavior of workers is inseparable from their working context. Biomedical researchers constantly face new challenges through new viruses, new technology, and new applications, many of which have not even been characterized enough to understand the risk they pose. This study is therefore aimed at applying Rasmussen’s model of boundaries to a biomedical laboratory in order to (1) identify the factors that contribute to the 3 boundaries, (2) identify the gradients that move the OP close to any of the boundaries with the possibility of crossing them, and (3) identify the countergradients that move the OP away from the boundaries toward the safe working space that enhances resilient performance. This has not yet been attempted in a biomedical laboratory, and the information obtained can be used to supplement and strengthen the existing OHSMS approach.
Materials and Methods
Research Setting
This study was undertaken in a medical school with a strong biomedical research emphasis as evidenced by research grants of more than US$530 million and over 5000 publications in international peer-reviewed journals. The school has established a schoolwide OHSMS to oversee all aspects of safety in the school and its activities, which is modeled on the elements of the internationally accepted OHSAS 18001 standard. The school has successfully obtained OHSAS 18001 certification for the past 5 years.
Research in the school is organized into research programs, each of which has several PIs working within a common field of research. As part of the schoolwide OHSMS, each PI is also required to develop an OHSMS for his or her own laboratory, based on the OHSAS 18001 elements. The school has a safety, health, and emergency management department that works closely with the PI and his or her team members to ensure that the laboratory has developed and implemented a robust OHSMS. This includes identifying hazards, assessing risk, and implementing control measures and SOPs, training programs, and other requirements in compliance with applicable regulations and laws. Fifteen researchers from 4 research teams were invited to take part in this study, which has been approved by the university’s institutional review board to ensure that ethical considerations are in accordance with applicable regulations.
Data Collection
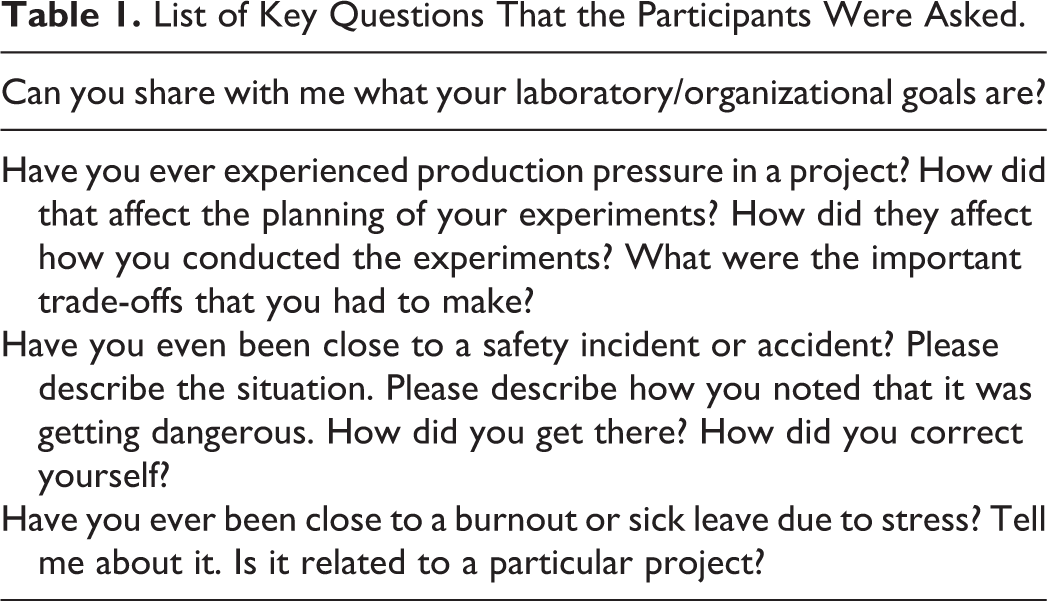
This study used the one-on-one semistructured interview method using some key questions and topics (Table 1) to understand and explore the participants’ opinions and experiences. This method allowed the interviewer to pursue the key topics related to this study while providing the flexibility to diverge and pursue points of interest as they arose during the interview. It also allowed the discovery of information that may be important to the participant but was not known to the interviewer prior to the interview. 52 Each response from the participant was used as an opportunity by the interviewer to probe further and to get in-depth information about the participant’s views. Participants were asked to draw from their entire biomedical work experience, regardless of country or institution, and not to limit their answers to the current laboratory. This method was used to uncover the diverse and rich experiences that all participants have had in their entire biomedical career.
List of Key Questions That the Participants Were Asked.
The participants were interviewed for between 45 and 60 minutes each between the months of May and June 2017. Each participant was interviewed only once, except for 1 participant who on his own accord came back the following day to add to the interview data. All the interviews were electronically recorded with the participant’s permission and transcribed into text. Second-order analysis was conducted by using thematic analysis, exploring all the responses and identifying common themes and subthemes. 53,54 The text was then coded into themes based on the response received from the participants, and subthemes were identified within each theme. All the participants were not asked the exact same questions; therefore, some responses do not total to 100%, because all the participants may not have provided an answer to every question. On the other hand, some questions (eg, the goal conflict of publication failure) had answers from all the participants, and the response totaled 100%.
Identification of Themes
The aim of this study is to apply Rasmussen’s model of boundaries to a biomedical laboratory; therefore, the transcribed data was examined to identify patterns or themes that were observed and then mapped onto the model. This was done by reviewing the data several times and then coding them such that patterns became discernible by using the following methods
53
: Repetitions such as repeated words or phrases in the same participant’s responses as well as across participants. This was done by reading through the text and looking for words or phrases that had the same meaning. The repetitions need not always be in response to the same interview question or situation. Similarities and differences in the way the participants responded to the same interview question or situation. This was done by comparing responses by the participants and assessing if there was 1 or multiple themes or subthemes in the responses. Repetition in the participant’s behavior patterns in response to similar situations either in the same participant at different times or across participants. The behavior patterns of the participants were used to assign themes or subthemes.
The coded data was used to identify and characterize the factors that formed the boundaries, gradients, and countergradients.
Results
Demographics of the Participants
The current positions held by the participants ranged from research assistant, PhD student, and postdoctoral fellow, with biomedical laboratory experience ranging from 3 to 20 years with an average of 9. Figure 1 provides the breakdown of the demographics.
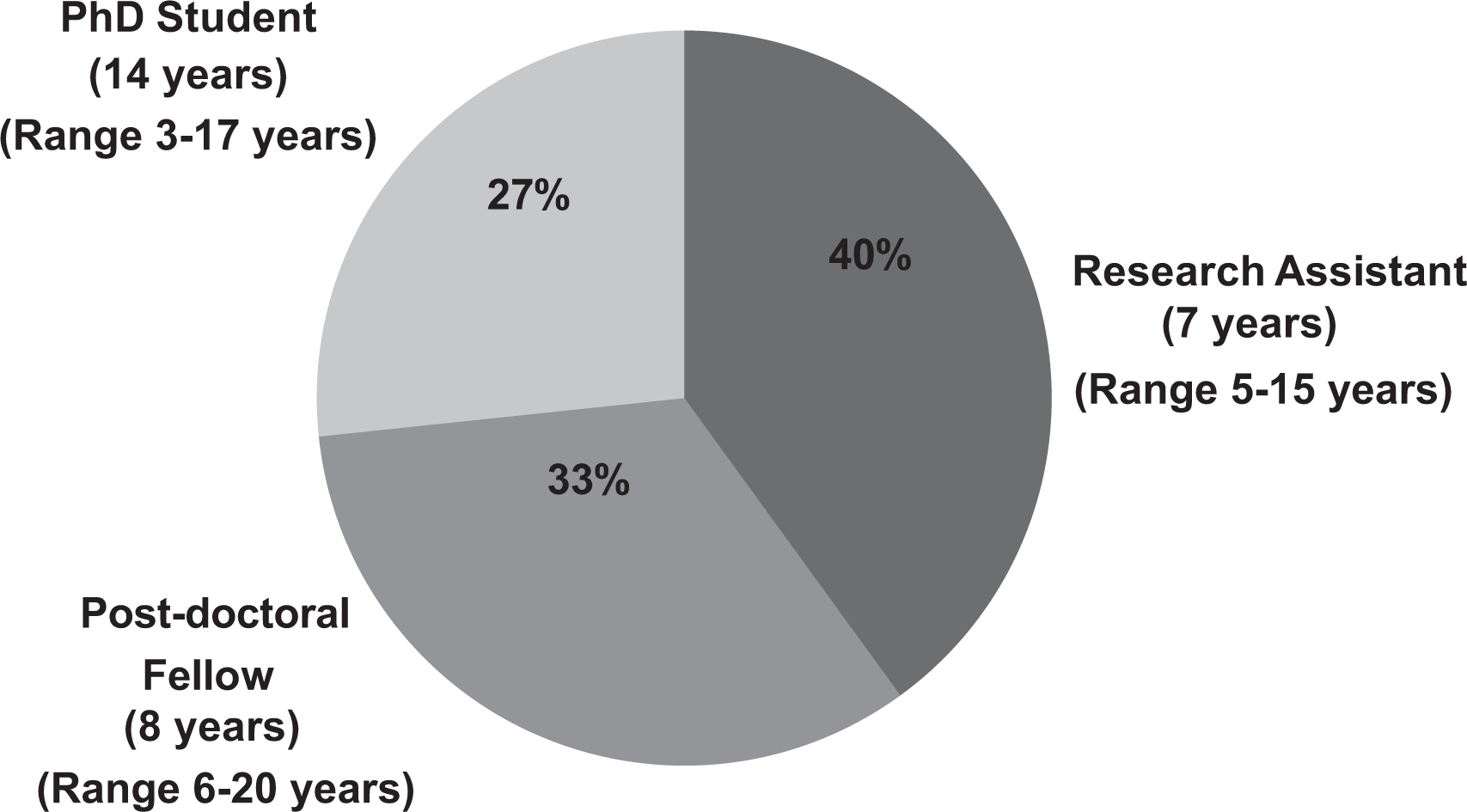
Demographics of participants: the current positions of the participants and the average (and range) number of years of biomedical experience for each group.
In biomedical laboratories, workers often face and deal with several types of hazards concurrently, each requiring a completely different set of skills and experience. Therefore, participants were asked about the different types of hazards that they had encountered in their laboratory experience. Five main types of hazard were identified: biological (infective agents), chemical, radioactive, laboratory animals, and animals in the wild. All participants encountered biological and chemical hazards; in addition, some laboratories worked with radioactive materials, laboratory animals, and animals in the wild. All participants except 2 had encountered at least 1 incident during their time working in a biomedical laboratory. An incident is defined as a work-related event(s) in which an injury or ill health or fatality occurred or could have occurred (https://oshwiki.eu/wiki/Accidents_and_incidents). All participants who described such an incident said that it happened to themselves or to coworkers.
Defining the Boundaries of the Rasmussen Model
Figure 2a shows Rasmussen’s model of boundaries plotted for a biomedical laboratory based on the interview information. The key measure of success of research teams is publications in leading scientific journals, with academic research often adopting the publish-or-perish culture. In line with this, failure to publish was a factor that all participants were very concerned about. Publication, in turn, depended on getting good, consistent, and reproducible experimental results. It therefore followed that experimental results were the immediate outcome that concerned the participants the most. Scientific output, which in turn depended on the experimental results, was a key measure of success. Thus, boundary to scientific output failure, formed one of the boundaries corresponding to Rasmussen’s boundary to economic failure. Table 2 shows the different factors that could lead to crossing of this boundary.
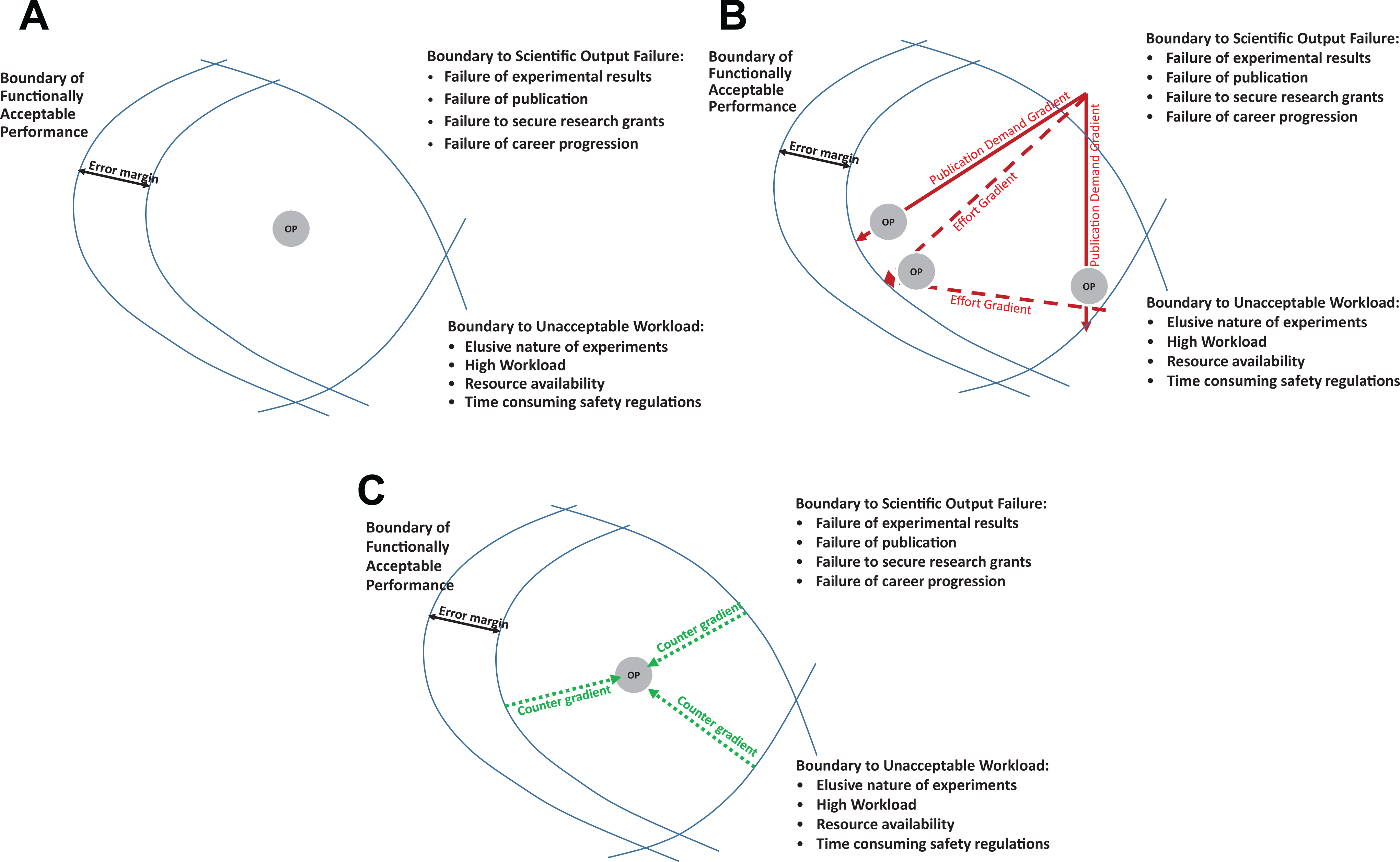
Rasmussen’s model of boundaries plotted for a biomedical laboratory. (a) Factors that form the 3 boundaries: boundary to scientific output failure, boundary to unacceptable workload, and boundary of functionally acceptable performance and the ideal location of the operating point (OP) in the space of possibilities within the boundaries. (b) Gradients that can shift the location of the OP. Publication demand gradient (solid lines) are measures taken to prevent the OP from crossing the boundary to scientific output failure and are mainly due to the pressure to publish. This gradient can push the OP toward the boundary to unacceptable workload and boundary of functionally acceptable performance. Effort gradient (dashed lines) are measures taken to follow the path of least effort in an attempt to avoid crossing the boundary to scientific output failure and boundary to unacceptable workload boundaries. (c) Countergradients (measures that achieve resilient performance) drawn as dotted lines. These comprise mainly the 3 methods of mental risk assessment, teamwork, and experience and familiarity that help to keep the OP within the space of possibilities. These measures are very important as they work collectively to keep the OP from crossing all 3 boundaries.
Factors that Could Lead to the OP Crossing the Boundary to Scientific Output Failure.
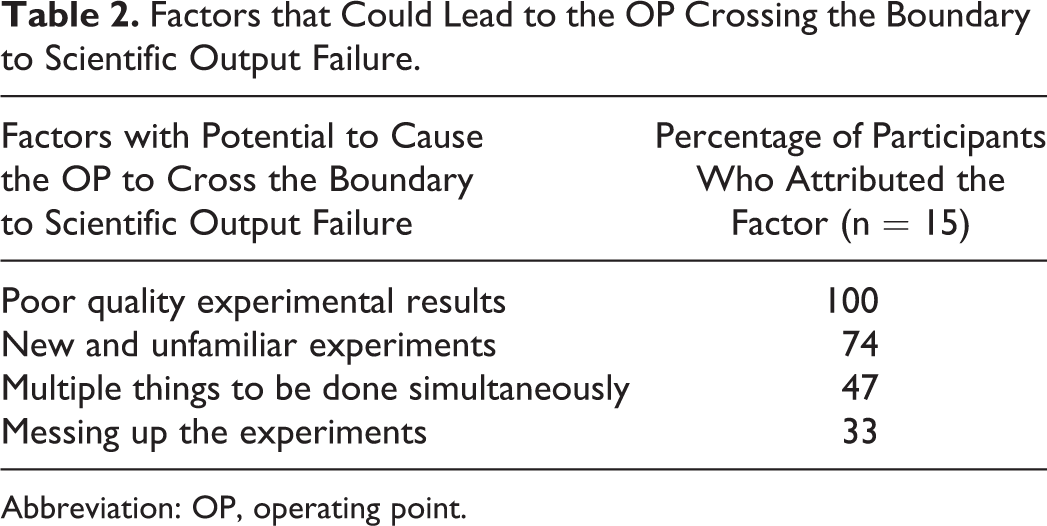
Abbreviation: OP, operating point.
The second boundary was identified by looking at the challenges faced by the participants to achieve the scientific output. Work overload, especially when the experiments were time dependent and urgent, was mentioned by the participants as a key challenge. Work overload being a key challenge formed the boundary to unacceptable workload in line with Rasmussen. Table 3 shows the different types of factors that could lead to crossing of this boundary. The last boundary was termed the boundary of functionally acceptable performance, in line with Rasmussen.
Factors That Could Lead to the OP Crossing Boundary to Unacceptable Workload.
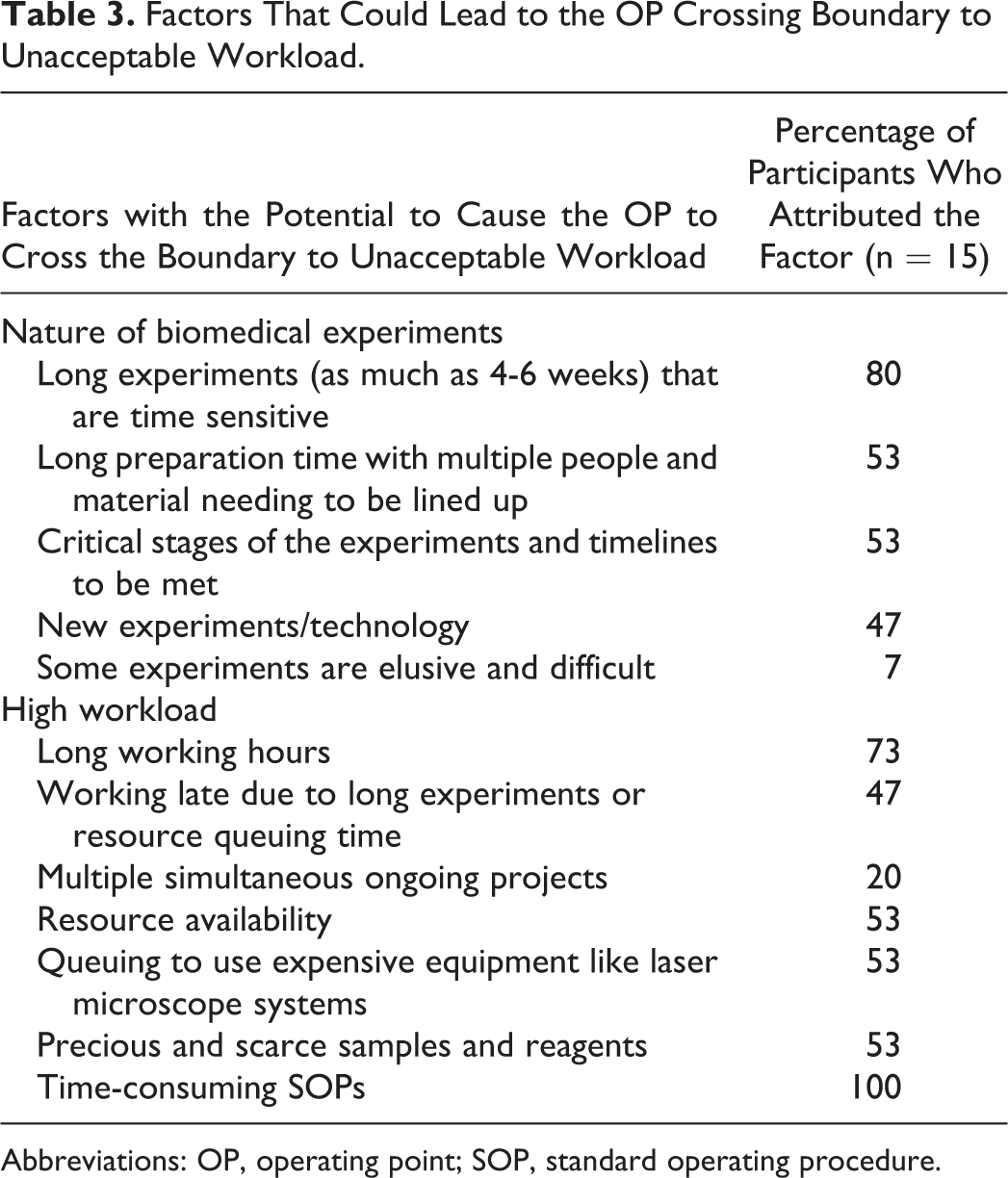
Abbreviations: OP, operating point; SOP, standard operating procedure.
Plotting the Gradients for the Rasmussen Model
In the Rasmussen model, gradients are production demands (cost effort) imposed by the organization and path of least effort (effort gradient) identified and adopted by the workers. These gradients, while preventing the OP from crossing the boundary to scientific output failure and the boundary to unacceptable workload, respectively, have the potential to move the OP beyond the boundary of functionally acceptable performance, thus causing an accident. The 2 gradients in a biomedical laboratory based on the results of this study are publication demand gradient and effort gradient.
Publication demand gradient
The pressure to publish was the most critical factor for all the participants, and to avoid crossing the boundary to scientific output failure, they worked closer to the other 2 boundaries, and this pressure formed the publication demand gradient. Figure 2b shows this gradient, which can move the OP toward both the boundary to unacceptable workload and the boundary to functionally acceptable performance (solid line in Figure 2b).
The tedious nature of biomedical experiments was cited as a factor by most participants, and 1 participant explained that during the critical and exploratory stages, they have to be very attentive to make sure that all the planning is not wasted and to get the maximum out of the experiments, especially when they have been planning the experiments for a long time. Some experiments may need to use core equipment that is only available through a booking system, and this can cause long waiting times. One participant explained that they had to use a machine at the hospital so they had to wait until routine patient work was complete before they could use the machine.
Effort gradient
Figure 2b shows the effort gradient, which are measures taken to follow the path of least effort in an attempt to avoid crossing the boundary to scientific output failure and the boundary to unacceptable workload that could move the OP toward the boundary of functionally acceptable performance (dashed line). To understand this gradient, it was necessary to find a marker to which all participants could relate. For the purpose of this study, deviations from SOPs (both safety and experiment related) was chosen as the marker. Deviation from SOPs are not uncommon in laboratories, and the emphasis on deviations from SOPs in this study also allowed the authors to understand which methods of assessments the participants used to identify the risk in such deviations, because such deviation with improper assessment of the risk could lead to crossing the boundary of functionally acceptable performance.
All participants felt that to follow the safety SOPs fully was sometimes time-consuming. They felt that the SOPs were sometimes impractical and probably written by those who did not know how laboratories worked: “People who make the rules should understand how a lab works; when something happens, they impose some rules that are very impractical. They don’t know how a lab works and they will think it’s just one step why can’t you do it. It will affect all our day-to-day work and procedures. I think SOP is very useful, of course it will minimize the risk but a lot of things are redundant and troublesome.”
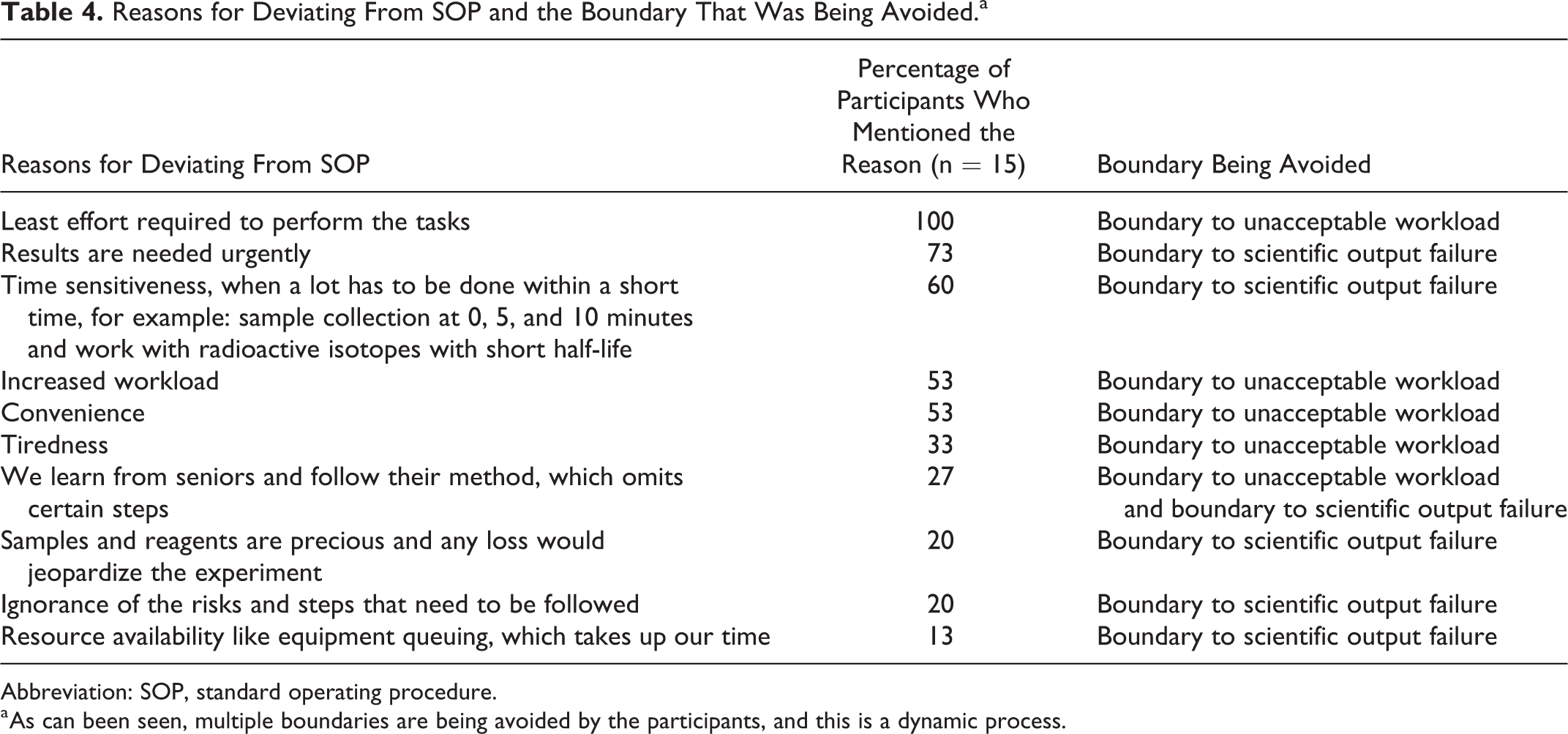
Reasons for deviating from SOPs
The participants were asked what caused them to deviate from the SOPs. The most common reason for deviating from the SOPs is to ensure that the experiment was not jeopardized, especially in time-sensitive experiments with precious samples and reagents (Table 4). In this case, the worker is trying to stay away from all 3 boundaries, as explained by 1 participant: “If it is the final result, then you are more stressed depending on how thirsty you are for this result.…Also, it has to do with planning experiments in terms of cost, you cannot just keep on buying animals or reagents so you have to be conscious of the tools you have and how precious they are. The more precious they are, the more stressed you are because you don’t want to use it up wastefully. You cannot just play with that so this is critical. If you have only 500 micrograms of a protein, you have to be mindful and cannot make too many trials.”
Reasons for Deviating From SOP and the Boundary That Was Being Avoided.a
Abbreviation: SOP, standard operating procedure.
a As can been seen, multiple boundaries are being avoided by the participants, and this is a dynamic process.
Example of deviation from SOPs
Biological samples are stored in large liquid nitrogen tanks because of liquid nitrogen’s extremely low temperature of –196°C. SOP says that when taking samples out of liquid nitrogen tanks, workers must wear cold-resistant cryogenic gloves to prevent frostbite. Cryogenic gloves are thick and heavy and do not give the dexterity required to handle the small vial of extremely precious biological material (Figure 3). The participants do not wear the cryogenic gloves in both hands and instead allow the liquid nitrogen to drain off before handling the vial so that nitrogen in the liquid state does not touch their hands. As one participant explained, if the vial fell into the tank, they know not to use their hands but to use tongs to retrieve them.
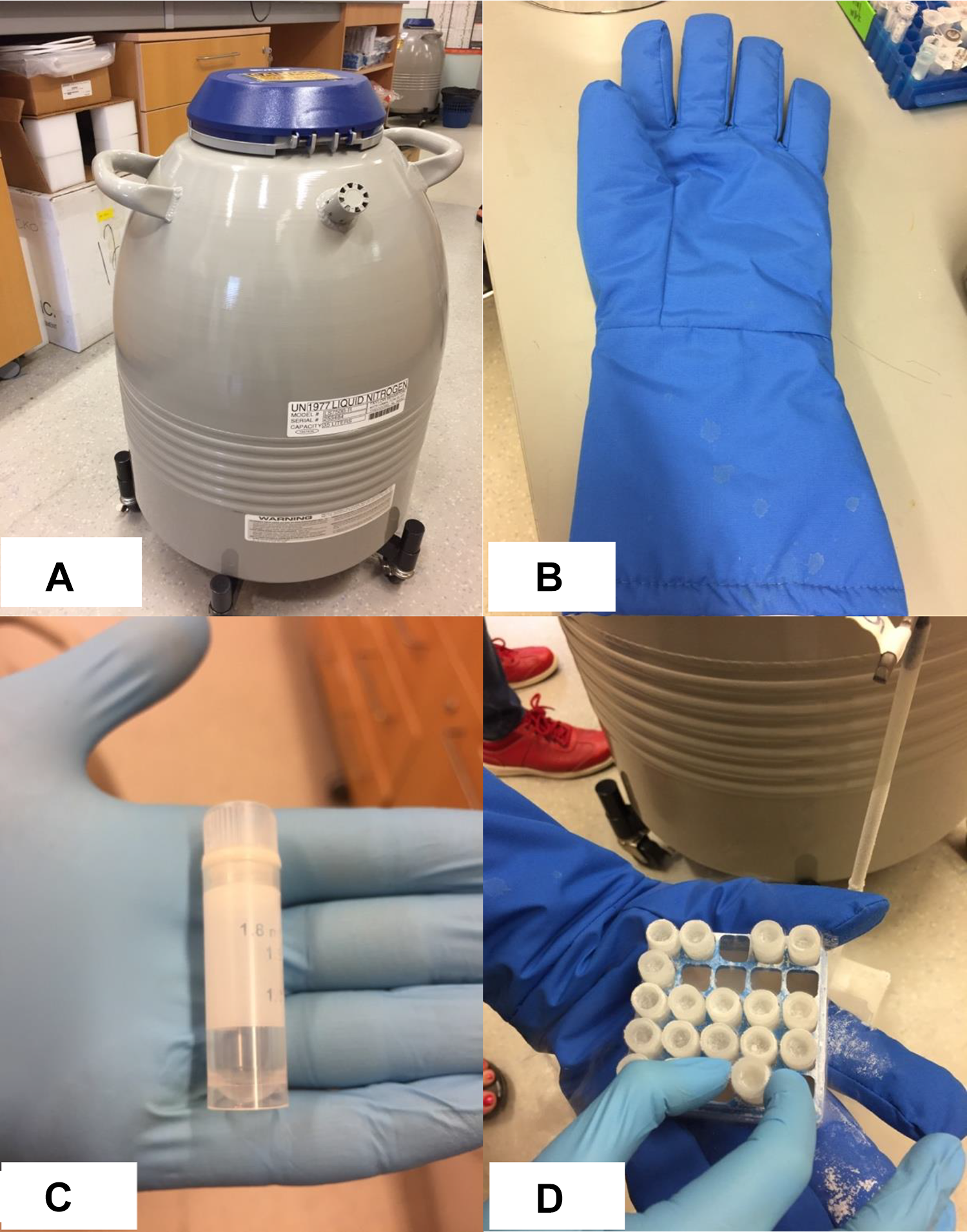
Examples of deviation from standard operating procedures (SOPs). (a) A liquid nitrogen tank that is used to store biological material for long term. (b) Thick cryogenic gloves that need to be worn according to the SOP to take any samples out of the liquid nitrogen. The samples, which are extremely precious and may be the result of several decades of research work, are in a small vial (c). (d) How the workers used nitrile gloves to allow dexterity so that they do not drop the vial of biological material.
Countergradients (resilient performance)
The measures described in this section are those used by the participants to remain within the space of possibilities described by Rasmussen as countergradients.
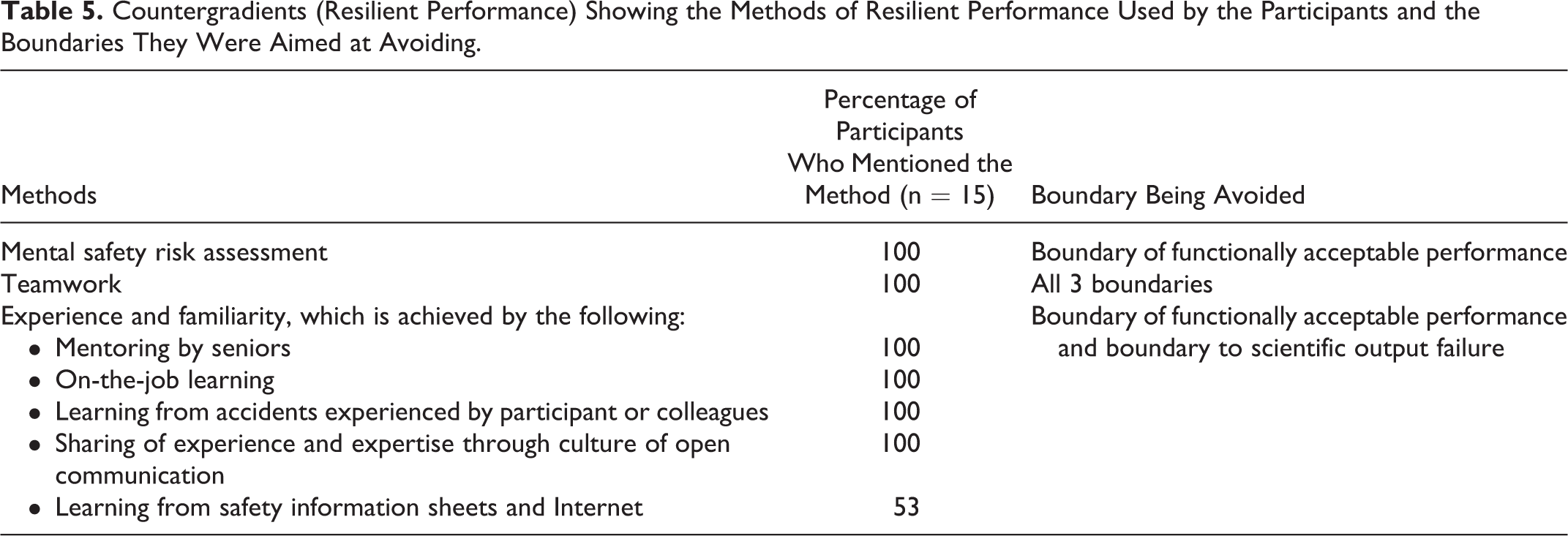
Figure 2c shows the countergradients (dotted lines) that help to keep the OP within the boundaries. The challenge in the laboratory is to ensure that experiments produce the desired results while ensuring that no accident or work overload occurs that will undo the productivity. Participants were shown the Rasmussen model of boundaries and asked how they ensured that the OP remained within the boundaries. The methods described were (a) performing mental risk assessment before they deviated from SOPs, (b) teamwork where they looked out for one another, and (c) experience and familiarity, which came through mentoring and actually performing the experiments repeatedly (Table 5).
Countergradients (Resilient Performance) Showing the Methods of Resilient Performance Used by the Participants and the Boundaries They Were Aimed at Avoiding.
Mental risk assessment
All participants, when interviewed, stated that they performed a mental risk assessment before deciding to deviate from a process in the SOPs. Five participants did not realize that they were performing a mental risk assessment until it was pointed out to them at the interview. Sometimes they would make sacrifices to reduce the higher-risk work (in this case, taking blood from animals) and continue with the lower-risk procedures (eg, taking swabs) when they were tired. Sometimes, if they were not as experienced in the procedure, they would ask a more experienced person to do it for them.
Teamwork
The nature of biomedical research is such that many things (eg, animals at precise weights and ages, sample collection, equipment availability, reagents with extremely short shelf-life [sometimes minutes as in radiochemistry]) have to be lined up before work can commence, and when everything is lined up, making mistakes will mean starting all over again and losing time, money, and precious samples. The participants said they worked in teams with a more experienced person leading the rest. The projects were divided among the teams and the workers had independence and responsibility to plan the work to ensure that it went smoothly, and they coordinated within their team to plan the work. Several participants said that they planned like “choreographing” a “drama production.”
Participants explained that when they performed complex work, they planned for days ahead before the work could commence. One participant described that they have both formal and informal “chit-chats” to plan the work. They worked in teams and “watched over each other” to “catch the balls so that none fell to the ground.” Participants said that when things went well, they all would benefit from that and share the success, so they planned such that they could divide the workload among each other so that the workload was reduced to a “doable amount for each person.” When they did complex, time-consuming, and risky work, they would build in redundancies in the form of asking colleagues to stand by in case of any problems or asking colleagues to watch over them to see if any issues were developing that the one performing the work was not able to see.
Experience and familiarity
Participants felt that the best way to learn was through a good mentor and by doing the work for themselves. All participants felt very strongly that mistakes, accidents, and incidents, whether they happened to themselves or colleagues, were the best teacher. One participant felt that open communication and a no-blame culture could go a long way in learning from mistakes: “A mistake is always considered as a personal failure, but I appreciate a more open policy with no blame and no consequences. No one does it on purpose. If something goes wrong, do you discuss it or do you cover it up?”
All participants said that when they learned a new procedure or used new material, they would be very careful and follow the SOPs. Once they became familiar, they would deviate from the SOPs based on mental risk assessment and their familiarity with the procedure.
One participant said that before attempting work that was risky, like working with infective agents, they practiced the procedures by going through the entire procedure without the virus and only doing the real work when they were very familiar with the procedure. This helps to stay away from both the boundary to scientific output failure and the boundary to functionally acceptable performance, because they do not want to use up the precious samples and also do not want to have an accident.
All participants said that they learned from their seniors who mentored them and told them about risk and safety at each step of the procedure and what to look out for. Only 20% relied on the SOPs to learn the safety aspects of the work, and about half of them got additional information from the Internet or safety information sheets. One participant said that when, as juniors, they learned from a good senior, and they also learned how to be good mentors when it was their turn.
Participants felt that SOPs were long and difficult to read; most of them did not read them, and they just learned from the senior who was mentoring them. In one of the participants’ previous workplace, they used a lot of scenario training, which the participant found very useful. When asked how safety training could be improved, participants said that mental risk assessment methods should be taught as part of the training. Participants felt that explanation was very important; if a risk and the control measure was explained to them, they would be more able to accept it. These countergradient methods prevented them from crossing not only the functionally acceptable performance boundary but also other boundaries, revealing that it was a dynamic process.
Discussion
In 1997, Rasmussen asked a very basic question: “Do we actually have adequate models of accident causation in the present dynamic society?” 23 In trying to determine a good model to study accident causation, he explained that while stable systems could be modeled by decomposition into structural elements, dynamic systems would have to take into consideration changing demands, risks, and competition in the workplace. In other words, while safety traditionally was managed by laws, rules, and SOPs, these were not adequate in a dynamic workplace. 55,56 Such rules and SOPs are not followed to the letter even in highly regulated industries, and workers often deviate from SOPs to meet other demands like production pressure. 27,57 -60 Workers will realize that they have degrees of freedom 61,62 to perform their tasks, and as they get more experienced in the tasks, they will have more choices in performing them based on practice and know-how. They will exercise these choices to deal with the workplace demands. 23
To perform their work successfully, workers will use the degrees of freedom to strategize and adjust the way they work when faced with production, workload, and other pressures. In doing so, Rasmussen explains that there will be a “natural migration of activities toward the boundary of acceptable performance,” 23 and he used a model of boundaries to illustrate the mechanism underlying this migration. In this descriptive model, the OP, the location where work is performed, constantly moves around in the space of possibilities bounded by 3 boundaries. In addition, there are gradients that push the OP toward the boundary of functionally acceptable performance and countergradients that push it away from all the boundaries to keep it within the space of possibilities. 23,24,33
The results show that in a biomedical laboratory, the factors contributing to the 3 boundaries (Figure 3a) are the boundary to scientific output failure, the boundary to unacceptable workload, and the boundary of functionally acceptable performance; the last 2 boundaries are similar to what is described by Rasmussen. The results also show that a key gradient (publication demand gradient), which has the potential to move the OP toward the boundary to unacceptable workload and the boundary of functionally acceptable performance, was the fear of failure to publish in reputable journals. This, in turn, prompted the workers to follow the path of least effort, which formed the second gradient (effort gradient) and had the potential to move the OP closer to the boundary of functionally acceptable performance. In addition to the gradients, the study aimed to identify countergradients that allowed the OP to remain within the workspace and prevent crossing any of the boundaries. These countergradients took the form of mental risk assessment, teamwork, and experience and familiarity.
The nature of biomedical research is in itself tedious because of inherent uncertainties and elusiveness in obtaining reproducible results.
30,31
Scientific output was the all-important goal expressed by every participant, and this required that they got good and reproducible experimental results. Therefore, to avoid crossing the boundary to scientific output failure, participants used their degrees of freedom to navigate within the space and sometimes worked closer to the other 2 boundaries. They seemed to be aware of the hazards and managed the tensions and trade-offs by using the following methods in various combinations to keep the OP within the space of possibilities: Performing mental risk assessment to omit certain steps and deviate from SOPs Working in teams and planning and coordinating the work processes well in advance Using their experience and familiarity with the work processes, which in turn were developed through mentoring, on-the-job training, and learning from accidents and incidents Making trade-offs and sacrificial decisions to stay within the space and not cross any boundaries
Hollnagel 63 explains that resilience is not something that a system has but something it does, and that becomes evident in the way that people and teams deal with everyday situations by adjusting their performance when faced with expected or unexpected changes, opportunities, and challenges. He also describes 4 potentials that are required for resilient performance as the potential to respond, monitor, learn, and anticipate. The results of this study show that workers are already showing evidence, albeit unknowingly, of resilient performance in the way they work by rarely crossing any of the boundaries while at the same time working close to the functionally acceptable performance and unacceptable workload boundaries in an attempt to remain productive and avoid crossing the boundary to scientific output failure. The workers not only are aware that they are working close to the boundaries but also use methods that sustain resilient performance that enables them to anticipate the boundaries and avoid crossing them.
The idea of applying Rasmussen’s model of boundaries to study resilience is not new and has been attempted by others. A study on the Dutch railways has attempted to find quantifiable parameters to study resilience 50 using the model of boundaries. The authors use the angle of the slope when the model is viewed from above to measure resilience, with a gradual slope denoting brittleness and a steep one resilience. Such measurements are not easy to devise, and this study has not attempted to do that but simply to understand the factors that form the boundaries and the gradients and countergradients employed by the workers. Knowing the boundaries and the location of the OP within the space for both organizations and individuals is essential to sustain resilient performance and avoid failure. 49 In the current study, by working in teams and “watching out” for each other, the workers were ensuring that the experimental results were of good quality, that they were not doing anything that could result in an accident, and that they were dividing the work among themselves such that the amount of work was “doable.” The countergradients described in this article are more local and applicable within the research team. In addition to this, there are several organizational initiatives such as occupational health checks, training, provision of adequate resources like personal protective equipment (PPE), and provision of safe working laboratories, which were not studied or addressed in this study.
In a community pharmacy setting when workers found the tension between working efficiently and safely challenging, often efficiency was favored with deviations from procedures to ensure productivity. 64 Workers often make deviations or adaptations from procedure to remain productive, and these need to be considered based on the context of the situation faced by the workers. A combination of a safety I approach, where performance resulted in incidents, and a safety II approach, which is resilient performance (ie, typical daily work), can be studied and used as an opportunity to gain understanding and learn how resilient performance is sustained. This can then be developed into corresponding meaningful improvements. Sharing of how they dealt with different situations makes a significant contribution to the learning that takes place. 65
Deviations from SOPs are seen in all industries and do not always lead to unsuccessful outcomes, but they can contribute to successful outcomes. SOPs cannot predict every possible scenario; in this respect, they are underspecified. It is the skill and experience of the workers rather than following SOPs that have led to a safe outcome in some situations, and this has been encountered in many industries. 57,58 Are the SOPs too stringent and therefore what appears to be a deviation is not really unsafe at all and could even be beneficial? In health care, such deviations are sometimes known to have beneficial outcomes in saving time and adjusting to the local situation. 64,66,67 However, it is essential to know which informal procedures are being adopted or discarded and to understand the circumstances that lead to this. Such deviations may, over time, modify the behavior of the workers to such an extent that the deviations will become normalized and lead to an accident. 68,69 Deviations from SOPs should be addressed principally by examining the SOPs and revising them based on how laboratory work is done in consultation with the workers 8 or by structural changes to the work system where these have been identified. This was correctly pointed out by 1 participant who said that people who make the SOPs (usually safety personnel) feel it is just 1 more step, so why cannot the laboratory worker just do it? In reality, that 1 step can delay the work throughout the day, and hence the laboratory workers will deviate from it.
Once the SOPs are written commensurate with sustaining resilient performance, taking into consideration how the laboratory works, workers can share and contribute to these in practice (eg, how they influence their risk assessments for different situations and how they influence the ability to exercise their degrees of freedom in a cautious and well-informed manner). 58 Amalberti et al 67 have described the use of Rasmussen’s model to study violations in aviation, train drivers, and rotary press and explain 3 stages in the progress of a deviation to a dangerous level. Initially, it is still a (1) safe action, moving to (2) borderline tolerated condition of use (BTCU) and (3) normalization of deviance and reckless individuals. Managing deviations is not an easy task and requires in-depth analysis and monitoring of the situation and will perhaps form the topic of further research.
Borrowing from studies in other health care settings, 70 human work can be understood in 4 varieties: work-as-imagined, work-as-prescribed, work-as-done, and work-as-disclosed. Work-as-imagined is what is written by policy makers, senior management, middle management, and others in SOPs and work procedures with a mental image of how work should be done. Work-as-prescribed is formal laws, regulations, rules, and so on, and these are the rules by which the correctness of work done is often judged. Work-as-done is the way in which work is really done, and work-as-disclosed is what the workers are willing to describe about the way work was done. Work-as-done is characterized by the trade-offs and compromises that the workers make all the time. As 1 participant talked about sacrificing 1 goal to achieve another goal: “If it was late at night and they were tired, they would still work but do the less risky tasks and leave the risky tasks for the morning when they were rested.” This is a sacrifice judgment where the group collectively sacrifices 1 goal for another—in this case, productivity vs safety. Such sacrifice judgments happen all the time and should be encouraged in a resilient organization. 38,47 Work-as-done is very dependent on the local situation, and if nothing goes wrong, these gaps are not even visible and the productivity is rewarded. When something goes wrong, these gaps between work-as-imagined and work-as-done become glaringly visible, and investigations often blame the fact that written rules are not followed exactly so additional rules are made. This in and of itself can create conditions that are new threats to safe production.
The participants in this study placed great emphasis on teamwork combined with experience and familiarity with the work process to remain both productive and safe. The workers already use these methods informally, and tailored training can assist in developing this further where both safety and productivity are given emphasis through strategic approaches, employee empowerment, and continual improvement. 8 This recognizes implicitly that sustaining performance is more than safety alone, or safety first, but that safety is but one concern. Hollnagel 63 asserts that resilience engineering looks at everything that an organisation does, at its functioning (on a broad scale of outcomes) and not only at what goes wrong. Safety is neither the only nor the primary concern, but just one among several. Saurin et al 71 have looked at the compatibility of lean production with complex systems theory to identify learning opportunities. Among the several ideas described, the one that is applicable to this study is the creation of an environment that supports resilient performance and teamwork and with a team formed by workers with a variety of complementary skills. This idea should be built into the approach to managing safety.
It has been pointed out that biomedical laboratories have been slow in learning and incorporating newer safety concepts and training modalities from other industries. 72 Our study is the first undertaken in a biomedical laboratory, and the results clearly align with the results from other industries showing that a combination of safety I and safety II approaches is necessary because in reality, this is how safety is managed in the workplace. It is time to incorporate newer concepts and training methods into the conventional safety concepts in a biomedical laboratory.
Conclusion
Resilient performance cannot be achieved by adding more rules to deal with every situation but by giving the right tools and knowledge to deal with and monitor the expected and unexpected situations that workers face every day. 73 The Rasmussen model of boundaries helped to understand the trade-offs and tensions in the laboratory and to appraise the methods that the workers used to manage them to remain productive and safe at the same time. This study already shows that the workers have developed the art of resilient performance on their own; it is now time to adopt a more modern approach to safety by incorporating resilient performance as part of safety training and everyday operations. 74 One approach is a hybrid model of rule-based non negotiable instructions and risk assessment–based practice in their everyday work. The rule-based organization-wide instructions will invite compliance when they are correct (commensurate on risk) and rewarding. These will always lack the requisite variety needed to deal with constantly changing work demands that need to be dealt with using local risk-based resilient performance.
Footnotes
Authors’ Note
All authors contributed equally to this work.
Ethical Approval Statement
Approval was sought from the University’s IRB to conduct this study and the study was conducted as per the approved protocol: IRB Reference Number: S-17-042E.
Statement of Human and Animal Rights
Not applicable to this study.
Statement of Informed Consent
Informed consent was obtained from all participants as per the IRB approved protocol.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.