
Abstract
The densities of enteroendocrine cells are abnormal in patients with irritable bowel syndrome (IBS); however, they tend to change toward normal levels in stomach, ileum, and colon following dietary guidance. The aim was to identify the types of duodenal enteroendocrine cells affected after receiving dietary guidance in the same group of patients with IBS. Fourteen patients with IBS and 14 control subjects were included. The patients received three sessions of dietary guidance. Both groups underwent gastroscopies at baseline, and again for the patients after 3–9 months (median, four months) from receiving dietary guidance. Tissue biopsies were collected from the descending part of the duodenum and were immunostained for all the types of enteroendocrine cells and were then quantified by using computerized image analysis. Using the Kruskal–Wallis non-parametric test with Dunn’s test as a post-test, the results showed a significant difference in the secretin cell densities between control subjects and patients with IBS prior to and following dietary guidance (P = 0.0001 and 0.011, respectively). The corresponding P values for cholecystokinin (CCK) cell densities were 0.03 and 0.42, respectively; gastric inhibitory peptide (GIP) cell densities were 0.06 and 0.43, respectively; serotonin cell densities were <0.0001 and 0.002, respectively; and for somatostatin cell densities were <0.0001 and 0.052, respectively. The Paired t-test showed a significant difference only in the serotonin (P = 0.03) and somatostatin (P < 0.0001) cell densities between IBS patients prior to and following dietary guidance. The changes in the cell densities of secretin, CCK, and GIP were not significant between IBS patients prior to and following dietary guidance. In conclusion, the densities of several duodenal enteroendocrine cells in IBS patients changed toward the values measured in control subjects following dietary guidance. The changes in serotonin and somatostatin cell densities may have contributed to the improvements in IBS symptoms, particularly pain and diarrhea.
Impact statement
Several contributing factors to the symptomology of irritable bowel syndrome (IBS) have been identified, such as abnormal densities of enteroendocrine cells and diet; however, the interactions between these factors have not been studied yet. The current study aims at exploring the dynamic changes between these two factors by studying the effect of using low fermentable oligo-, di-, monosaccharides and polyol (FODMAP) diet (known to improve IBS symptoms) through dietary guidance on the enteroendocrine cell densities in the duodenum. The findings showed that the densities of different enteroendocrine cells in the duodenum were abnormal before the patients received dietary guidance and tend to change/normalize after receiving guidance, which may have contributed in improving the symptoms of IBS. These findings highlight the importance of enteroendocrine cells in IBS pathophysiology and the mechanism behind the positive effect of low FODMAP dietary guidance in improving IBS symptoms and its usage as first step in the line of IBS management.
Keywords
Introduction
Irritable bowel syndrome (IBS) is a chronic disorder of the gastrointestinal (GI) tract characterized by abdominal pain or discomfort, bloating, and altered bowel movements. 1 The etiology of IBS is not known, but several factors appear to contribute to its pathophysiology, including diet, hereditary factors, low-grade inflammation, microbiota, and abnormal enteroendocrine cells.2,3
Most patients with IBS believe that certain foodstuffs trigger their IBS symptoms,4–6 mainly those that are rich with fermentable oligo-, di-, monosaccharides and polyols (FODMAPs), and insoluble fibers.7–11 Dietary guidance promoting a low-FODMAP diet along with altering the proportions of carbohydrates, protein, and fat in the diet has shown to alleviate IBS symptoms and improve the patients’ quality of life (QOL).8,12
Enteroendocrine cells play a crucial and major role in regulating several GI functions, including visceral sensitivity, secretion, absorption, motility, proliferation of epithelial and mesenchymal cells, local immune defense, and appetite. 13 Such regulation occurs through the exocytosis of hormones at the basolateral surface of the enteroendocrine cells.14–19 The enteroendocrine cells are abnormal throughout the GI tract in IBS patients20–26 and previous studies have shown that dietary guidance changes the enteroendocrine cell densities toward the values measured in control subjects in the stomach, ileum, and colon27–32 in the same group of IBS patients in the current study. Moreover, dietary guidance has normalized the densities of the duodenal chromogranin A immunoreactive cells, 31 which are considered as general marker for enteroendocrine cells.33–35 However, it is not clarified which types of enteroendocrine cells were affected. Therefore, the current study was undertaken to determine which enteroendocrine cell types are affected in IBS patients after they receive dietary guidance.
Material and methods
Study design
A total of 46 patients (35 females and 11 males with an age range 18–69 years [mean 35 years]) who were referred to gastroenterology outpatient clinic, Stord Hospital, Stord, Norway, and fulfilled Rome-III criteria for the diagnosis of IBS were included in this study. The patients have been subjected to a physical examination, blood tests (to exclude any infections, inflammations, and other organic/systemic diseases), and then received three individual sessions of dietary guidance, each for 45 min, at intervals of minimum two weeks, provided by certified nurse specialized in diet and IBS (Figure 1). The patients were also scheduled for a gastroscopy examination before the sessions of dietary guidance and again after 3–9 months (median of four months) from the last session. Fourteen subjects (nine females and five males), age range 26–70 years (mean 54 years), with no previous history of IBS were included as a control group. The inclusion and exclusion criteria for the patients and controls in the current study were previously described.
31
Study flowchart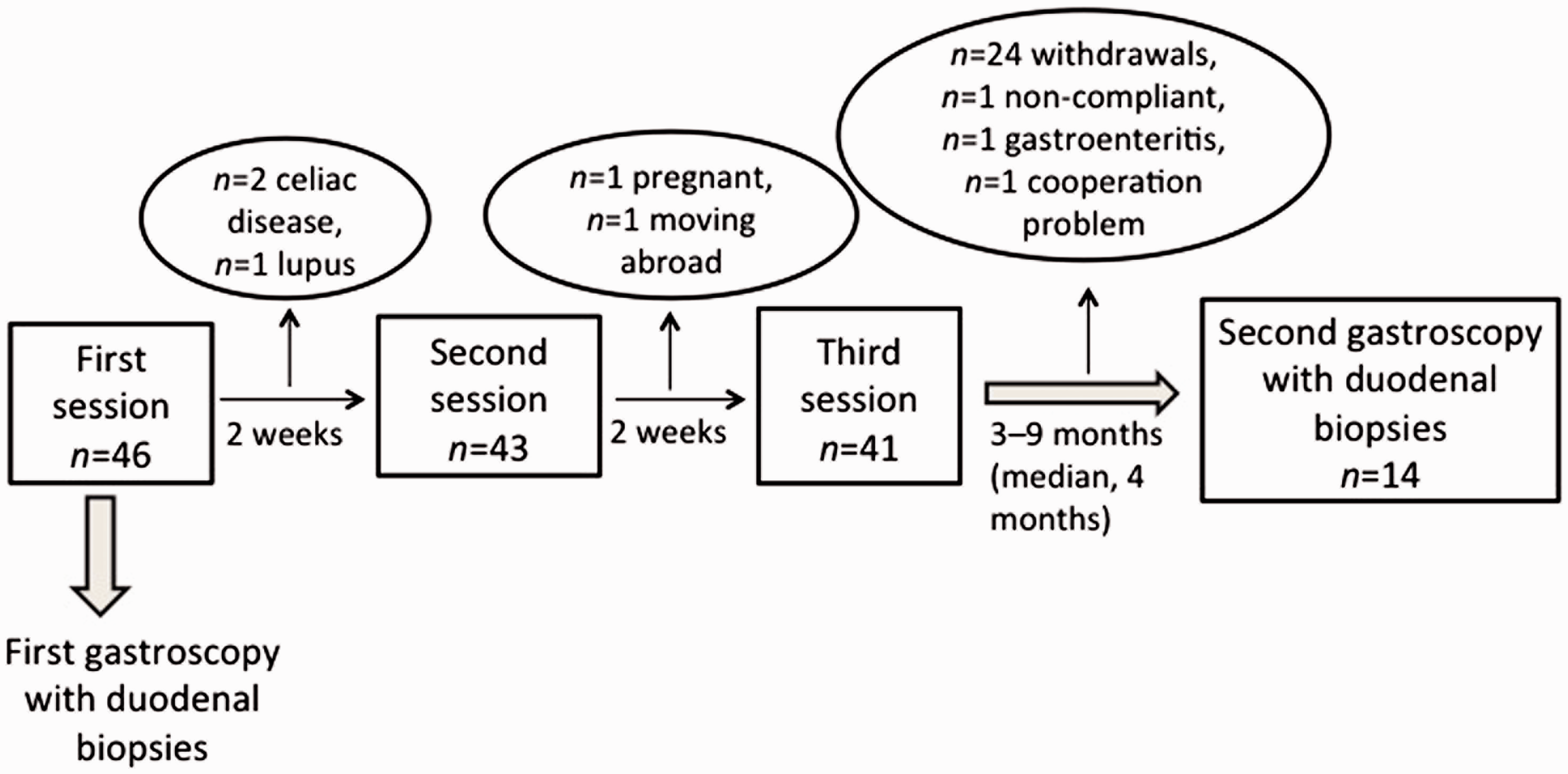
The Regional Committees for Medical and Health Research Ethics of western Norway, Bergen, Norway approved the study (number 2010/2650-2). The current study was performed in accordance with the Declaration of Helsinki. All of the participants consented (orally and in written forms) to participate in this study.
Sessions of dietary guidance
Advisory list of foods for patients with IBS
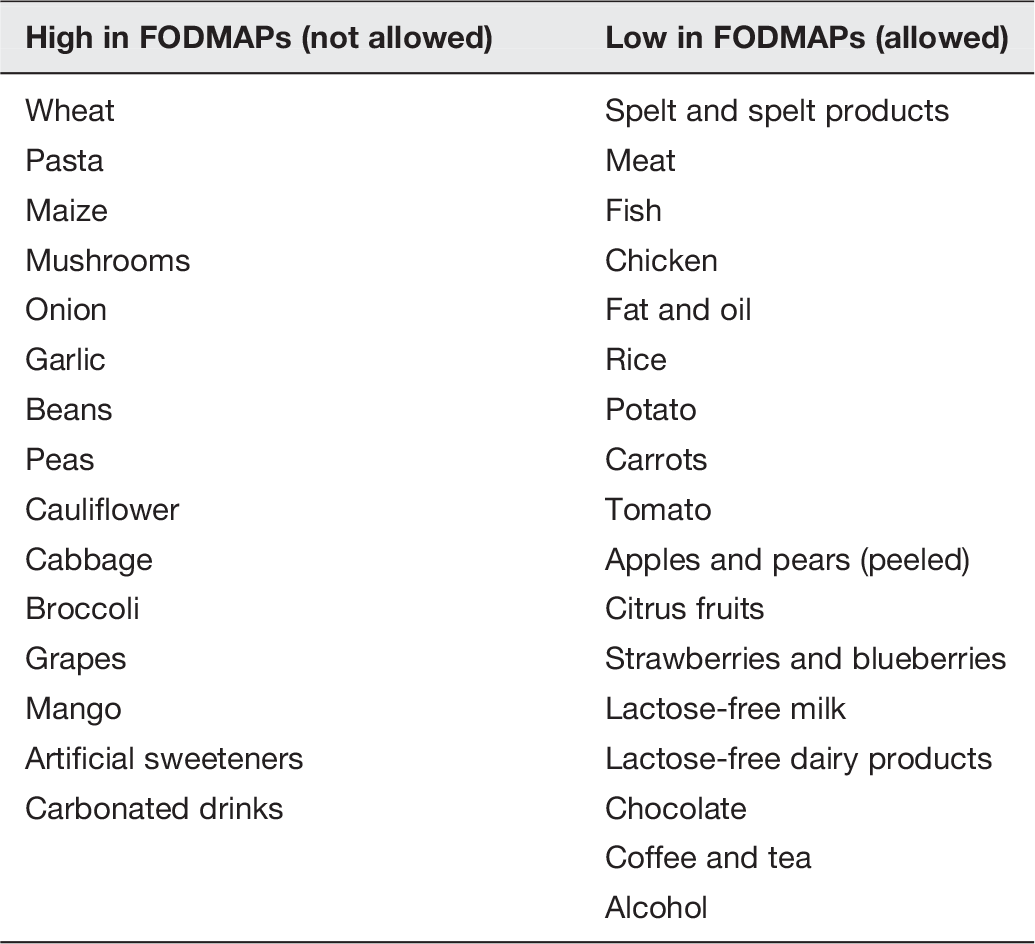
FODMAP: fermentable oligo-, di-, monosaccharides and polyol; IBS: irritable bowel syndrome.
IBS symptom assessment
The Birmingham IBS symptom questionnaire (Birmingham questionnaire) measures the symptoms of IBS patients, namely pain, diarrhea, and constipation. 36
QOL assessments
The quality of life (QOL) in IBS patients was assessed by the Irritable Bowel Syndrome-Quality of Life questionnaire (IBS-QOL) and the Short-Form of Nepean Dyspepsia Index (SF-NDI) questionnaire. The IBS-QOL questionnaire is IBS specific that assesses the patients’ physical and psychosocial functioning.37,38 The SF-NDI measures the health-related quality of life and was constructed and validated originally for dyspeptic patients 39 ; however, a Norwegian translation of the questionnaire was validated for IBS patients. 40
Dietary assessment
The Norwegian Mother and Child Study food frequency questionnaire (MoBa FFQ) (www.fhi.no/dokumenter/011fbd699d.pdf) 41 was used to assess the dietary intake of each patient. This questionnaire reported the frequency and the portion size of the meals and beverages that were consumed during the study. The nutrient content was calculated using FoodCalc. 42 The MoBa FFQ was developed and validated by the Institute of Public Health in Oslo, Norway.43,44 It inquires about the consumption of more than 200 different foods and identifies the participant’s dietary habits according to the patterns of Norwegian meals.
The patients completed and returned the forms of Birmingham questionnaire, IBS-QOL, SF-NDI, and MoBa FFQ at baseline before the first session and again, on the day of control gastroscopy, at least three months after the last session of dietary guidance. 12
Gastroscopy and immunohistochemistry
The participants of both groups fasted overnight prior to undergoing a gastroscopy. During the gastroscopy, four tissue biopsies were collected from the descending part of the duodenum, distal to major duodenal papilla. The preparation of the slides was previously described in details. 31 The sections were stained with hematoxylin (Harris Hematoxylin satin [Ortho], Ref.: RBA-4213-00A, Cellpath Ltd, Newtown, Powys, UK)-eosin (Eosin Y, Ref: 1.15935.0100, CAS.no: 17372-87-1, Merck KGaA, 64271 Darmstadt, Germany) and immunostained with an ultraView Universal DAB Detection Kit (cat.no. 760-500, Ventana Medical Systems, Basal, Switzerland). 45 The sections were then incubated with primary antibodies, diluted according to the suppliers’ recommendations as previously described, for the detection of secretin (code sc-20938, Santa Cruz Biotechnology, Santa Cruz, CA, United States), cholecystokinin (CCK; code A0568, Dako, Glostrup, Denmark), gastric inhibitory peptide (GIP; code no. sc-57162, Santa Cruz Biotechnology), somatostatin (code A0566, Dako), 45 and serotonin (code R87104 B56-1, Dako). 26
Computerized image analysis
Image analysis was performed using ×40 objective on the light microscope and a computer software (Cell^B, Olympus, Tokyo, Japan). The number of immunoreactive enteroendocrine cells was quantified in 10 randomly chosen fields with epithelial cell area measured at 0.09 mm2 per slide. The density of each enteroendocrine cell type was expressed as the number of cells/mm2 of epithelium. By keeping the identity of the slides concealed, the quantifications of all the slides were conducted by the same person (TM).
Statistical analysis
Fisher’s exact test is used for sex comparisons between control subjects and patients, while the Mann–Whitney U test is used to compare between the ages of both groups. The Kruskal–Wallis non-parametric test with Dunn’s test as a post-test is used to compare between the enteroendocrine densities of the control subjects and patients before dietary guidance and also between the enteroendocrine densities of control subjects and patients after dietary guidance. The paired t-test is used to compare the enteroendocrine densities of the patients between before and after receiving dietary guidance. The data are presented as mean ± SEM values. P < 0.05 are considered to be statistically significant.
Results
Patients and control subjects
The study initially included 46 patients who were planned to receive three sessions of dietary guidance. However, many of these patients were excluded/dropped out of the study due to different reasons, including newly diagnosed with celiac disease (following first gastroscopy) or lupus, cooperation problems, non-compliance, pregnancy, moving abroad, being treated with antibiotics because of gastroenteritis or withdrawing their consent, as shown in the flowchart (Figure 1). These dropouts meant that only 14 patients (nine females and five males) with an age range 21–44 years (mean 33 years) completed the study. There was a significant difference between the patient and control groups in age (P = 0.0002) but not in sex (P = 1).
Changes in IBS symptoms and QOL
The changes in symptoms and QOL in IBS patients in the current study have been described previously. 12 Briefly, IBS symptoms as assessed by Birmingham questionnaire showed significant improvements particularly in the domains of pain (P < 0.001) and diarrhea (P < 0.05) but not in constipation, after receiving dietary guidance. The total scores for QOL as assessed by the IBS-QOL and SF-NDI showed significant improvements in the QOL in IBS patients after they have received dietary guidance (P = 0.003 and 0.002, respectively). 12
Dietary assessment
The changes in diet implemented in the present study have been described previously. 12 In brief, the patients’ daily total consumption of FODMAPs decreased significantly between before (16.2 ± 5.3 g) and after (9.2 ± 3.2 g) receiving dietary guidance (P = 0.02). However, the daily consumption of fiber did not significantly change (27.4 ± 2.5 g versus 23.1 ± 2.2 g, P = 0.09). 12
Gastroscopy and immunohistochemistry
The gastroscopies showed that the duodenal mucosa was macroscopically normal in both patients and control subjects. Histopathological examinations of the duodenal biopsies from patients and control subjects were also normal. Immunoreactive enteroendocrine cells were found among the epithelial cells both in patients and control subjects; they were either basket- or flask-shaped and sometimes with a long basal cytoplasmic process.
Computerized image analysis
Densities of immunoreactive enteroendocrine cells in the duodenum of control subjects and of IBS patients before and after receiving dietary guidance

CCK: cholecystokinin; GIP: gastric inhibitory peptide; IBS: irritable bowel syndrome.
Data are mean ± SEM values. *P: control versus before guidance, **P: control versus after guidance, ***P: before versus after guidance.
P < 0.001.
P < 0.05.
P < 0.0001.
P < 0.01.
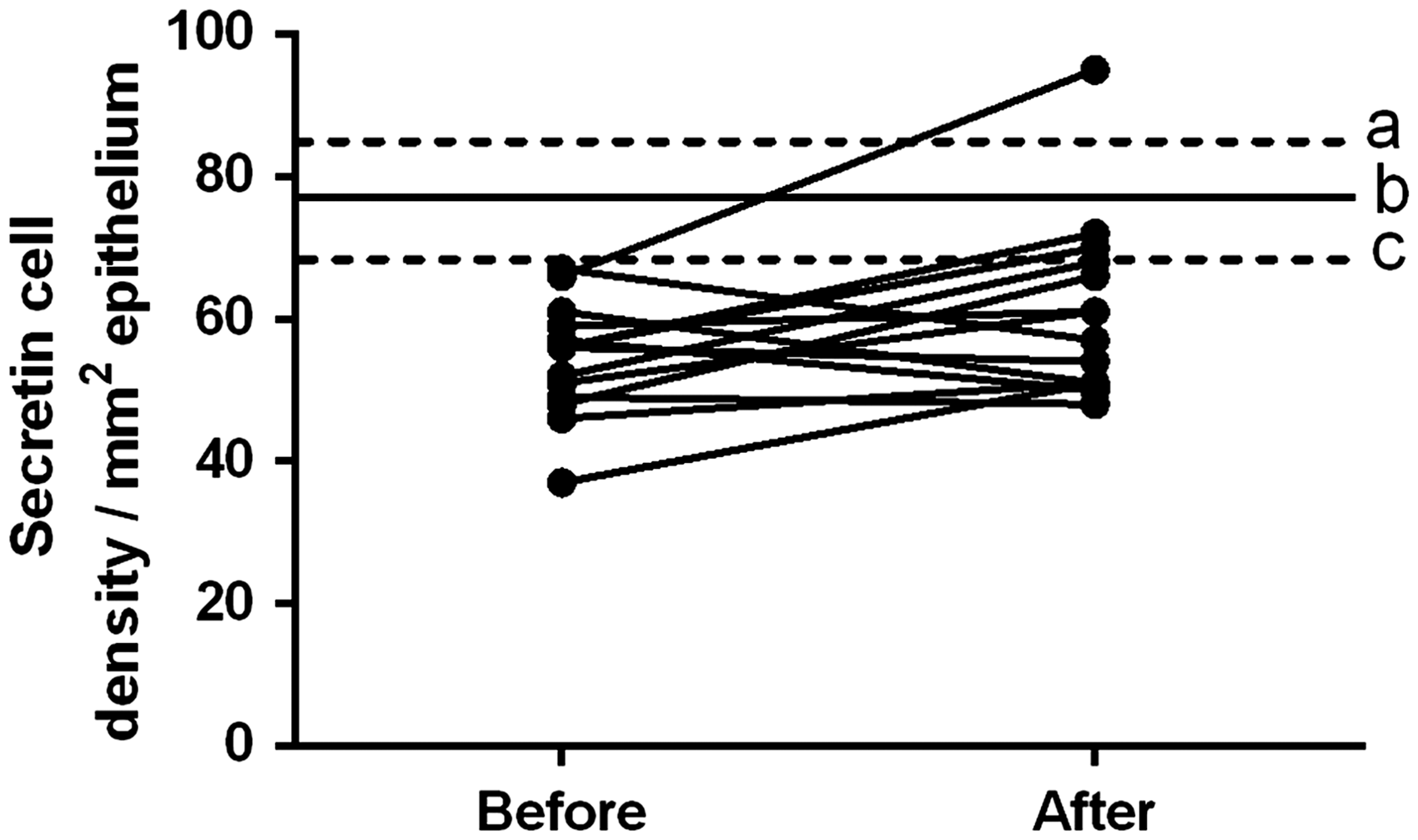
Secretin cell densities in the duodenum of IBS patients before and after receiving dietary guidance. The dashed lines labeled ‘a’ and ‘c’ indicate the upper and lower limits of the 95% confidence interval of the secretin cell density in control subjects, respectively, while line ‘b’ indicates the mean density. IBS: irritable bowel syndrome
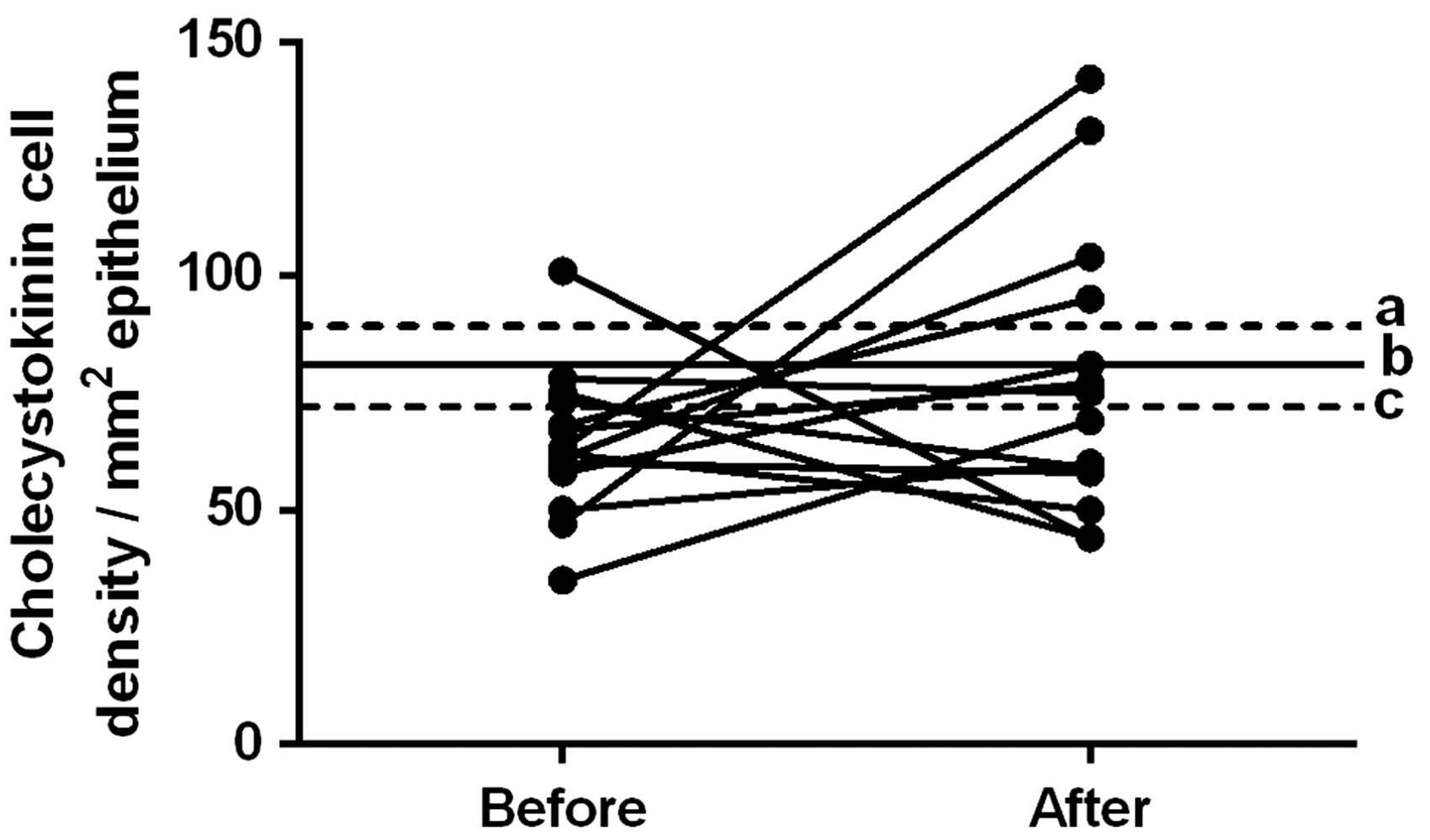
CCK cell densities in the duodenum of IBS patients before and after receiving dietary guidance. The dashed lines labeled ‘a’ and ‘c’ indicate the upper and lower limits of the 95% confidence interval of the CCK cell density in control subjects, respectively, while line ‘b’ indicates the mean density. CCK: cholecystokinin; IBS: irritable bowel syndrome
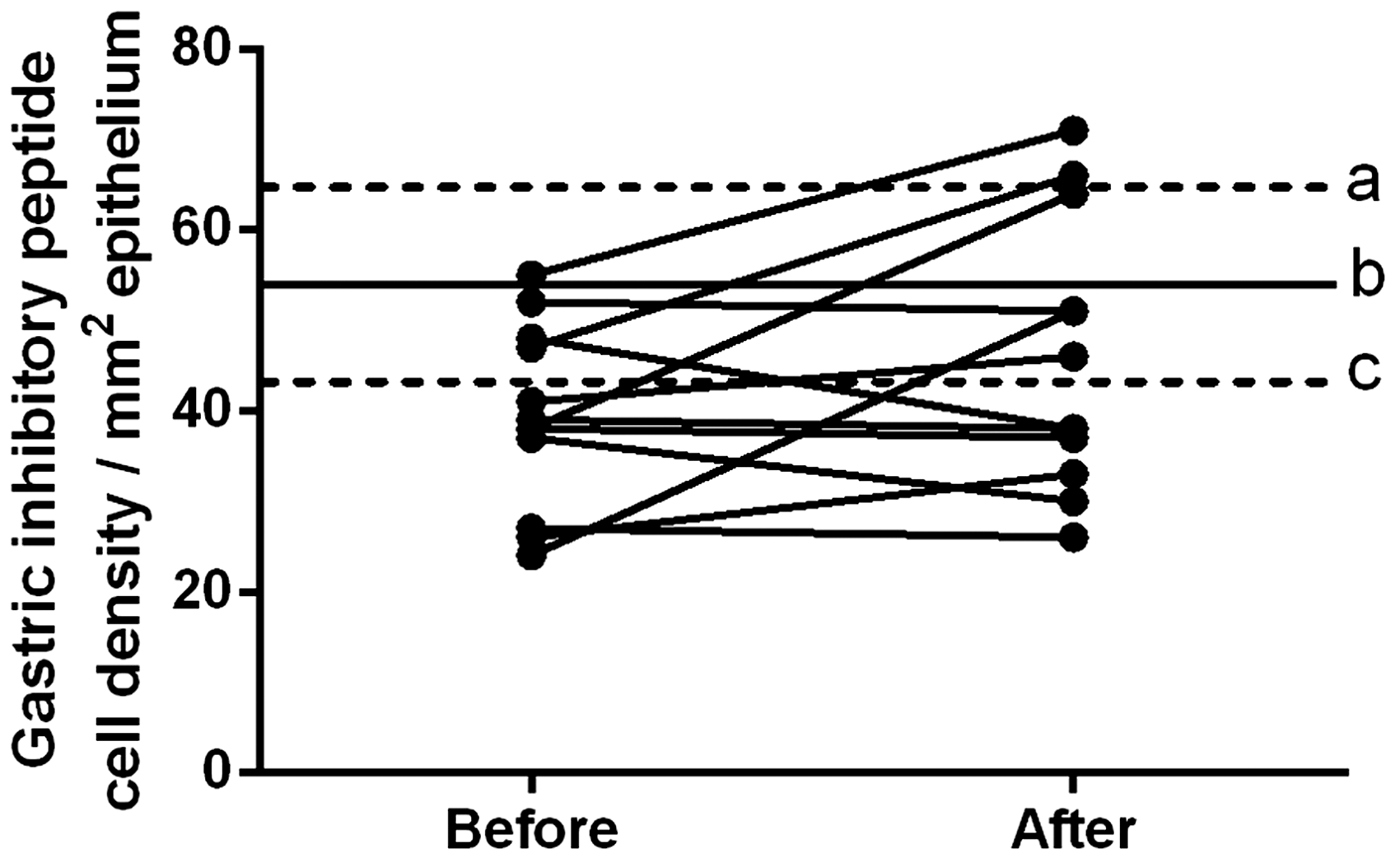
GIP cell densities in the duodenum of IBS patients before and after receiving dietary guidance. The dashed lines labeled ‘a’ and ‘c’ indicate the upper and lower limits of the 95% confidence interval of the GIP cell density in control subjects, respectively, while line ‘b’ indicates the mean density. GIP: gastric inhibitory peptide; IBS: irritable bowel syndrome
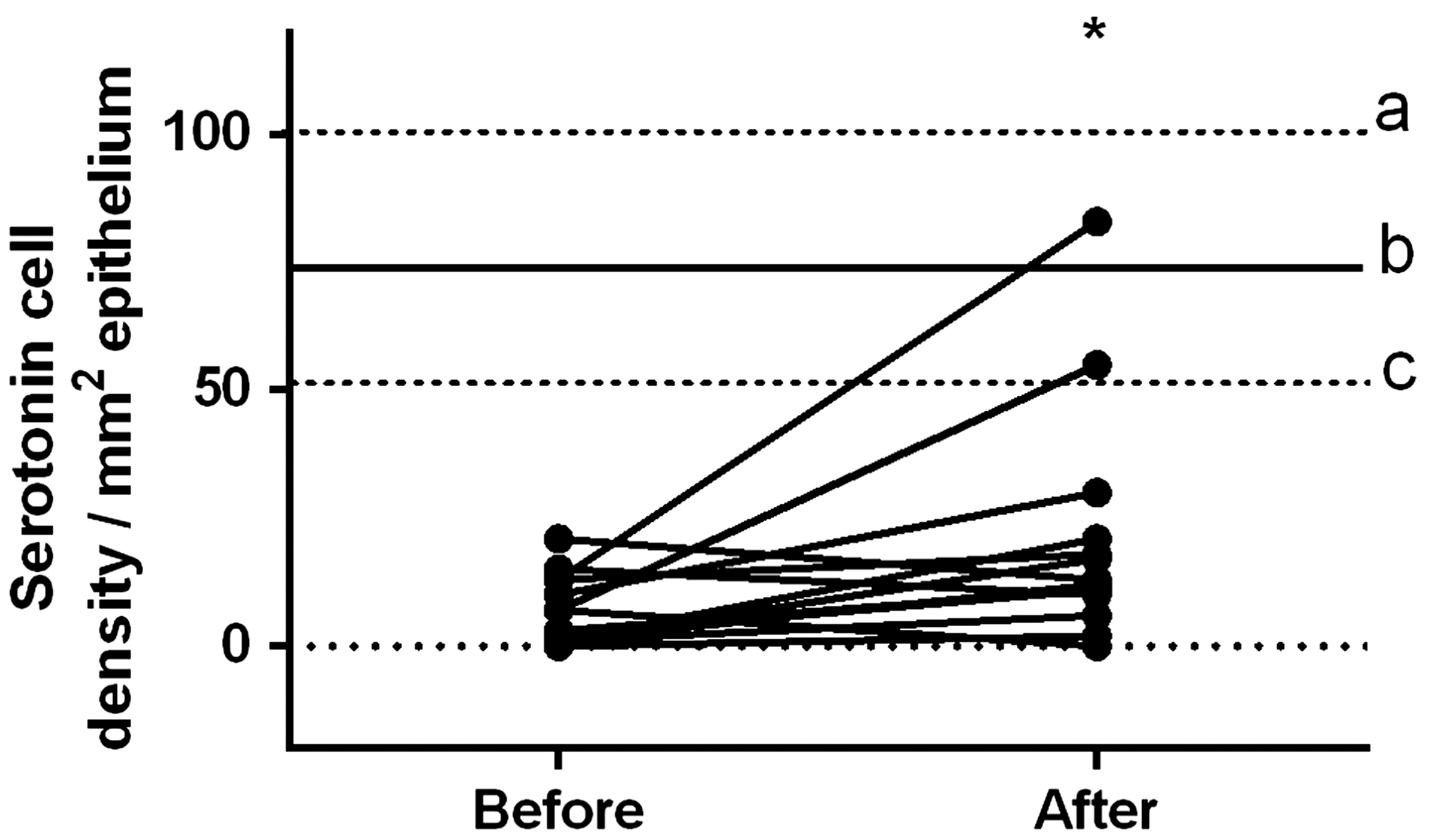
Serotonin cell densities in the duodenum of IBS patients before and after receiving dietary guidance. The dashed lines labeled ‘a’ and ‘c’ indicate the upper and lower limits of the 95% confidence interval of the serotonin cell density in control subjects, respectively, while line ‘b’ indicates the mean density. *P < 0.05. IBS: irritable bowel syndrome
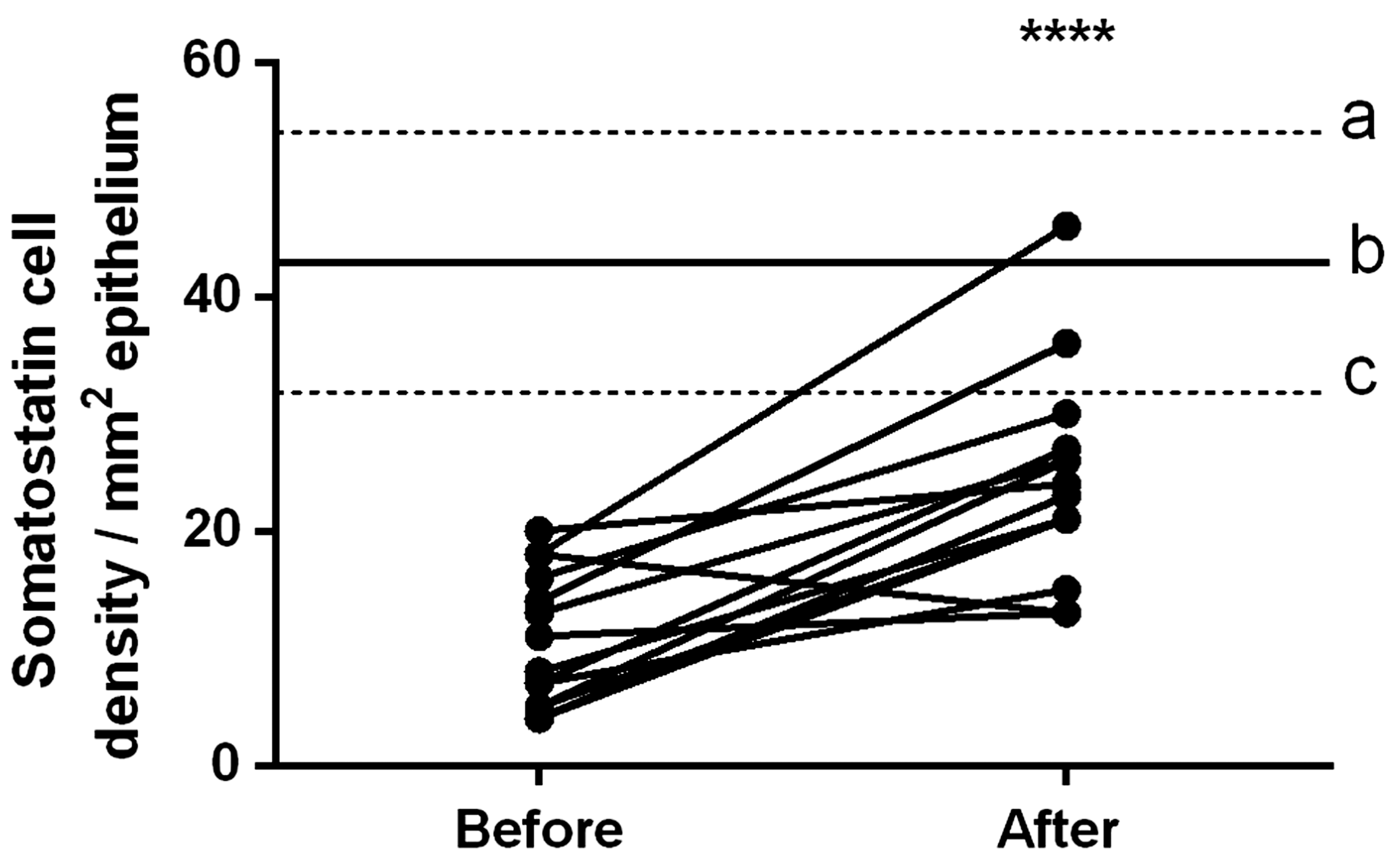
Somatostatin cell densities in the duodenum of IBS patients before and after receiving dietary guidance. The dashed lines labeled ‘a’ and ‘c’ indicate the upper and lower limits of the 95% confidence interval of the somatostatin cell density in control subjects, respectively, while line ‘b’ indicates the mean density. ****P < 0.0001. IBS: irritable bowel syndrome
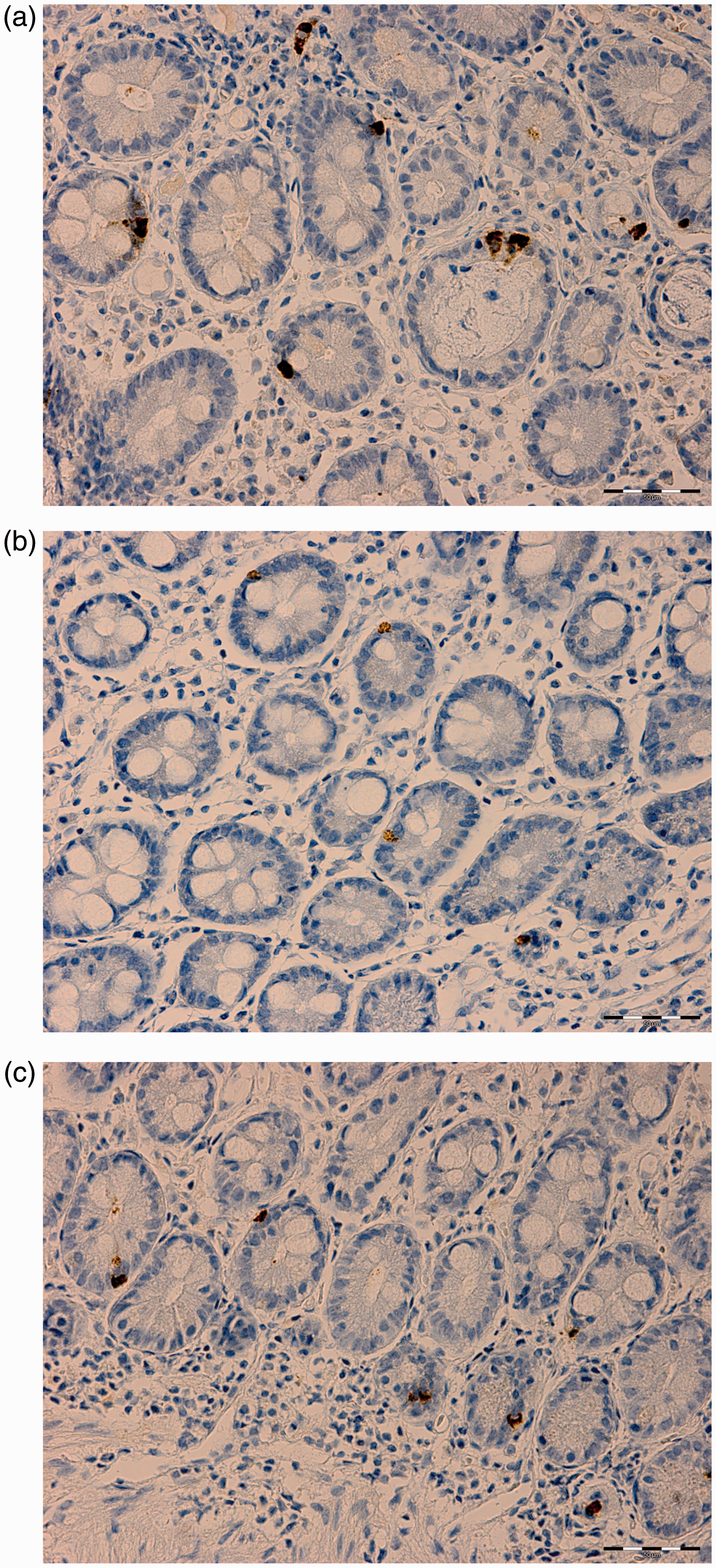
Somatostatin cells in the duodenum of a control subject (a) and of an IBS patient before (b) and after (c) receiving dietary guidance. IBS: irritable bowel syndrome
Discussion
This study was characterized by a high dropout rate, which is consistent with previous studies involving IBS patients.8,46–49 The dropout rate was 72%, which could be due to the demanding study design that required the patients to undergo two invasive procedures (gastroscopies) and to follow a strict diet for at least three consecutive months. Most (52%) of these dropouts were due to the patients withdrawing their consent after they received dietary guidance and their symptoms had improved, in addition to their unwillingness to undergo a second gastroscopy. The remaining 20% of the dropouts were due to exclusion factors such as being diagnosed with organic diseases (celiac disease or lupus), pregnancy, moving abroad, or receiving antibiotics treatment because of a bout of gastroenteritis. Nonetheless, despite the small number of patients who completed the entire study, the dietary guidance that was delivered to these patients still significantly affected their duodenal enteroendocrine cells, as it reportedly did in other segments of the GI tract.27–31 The age distribution differed between the present patients and control subjects; however, a previous study found that age did not affect the densities of duodenal enteroendocrine cells. 50
A previous study that included the same group of IBS patients as in the current study found that the total number of duodenal enteroendocrine cells (as detected by chromogranin A) tended to normalize after they had received dietary guidance. 31 The finding of the present study showed that these changes occurred due to the significant changes in the duodenal serotonin and somatostatin cells and also changes in secretin, CCK, and GIP cells (though not significant).
Secretin stimulates pancreatic exocrine secretion, 51 regulates the homeostasis of body water,52,53 and inhibits gastric emptying and intestinal motility.54,55 CCK delays gastric emptying, 56 stimulates gallbladder contraction,57,58 results in the release of pancreatic enzymes,59,60 and suppresses food intake.56,59
Since GIP belongs to the incretins family, 61 it increases insulin release from the pancreas61,62 and inhibits gastric acid secretion.62,63 The cell densities of secretin and CCK in the duodenum were significantly lower in our IBS patients while consuming the standard Norwegian diet and before receiving dietary guidance than in our control subjects, which is in accordance with the previous findings.26,45 Serotonin modulates the visceral sensitivity and conveys sensation from the GI tract to the central nervous system by activating Meissner’s plexus (submucosal sensory branch).20,64,65 In addition, serotonin stimulates the intestinal motility and accelerates the intestinal transit.65–67 Somatostatin inhibits intestinal contractions as well as gut exocrine and neuroendocrine secretion.13,68 The density of somatostatin cells in the duodenum was previously found to be lower in IBS patients than in control subjects.26,45 After the IBS patients in the current study received dietary guidance, the densities of secretin, CCK, and GIP cells increased toward the values measured in control subjects, but this increase was insignificant between before and after receiving dietary guidance. On the other hand, serotonin and somatostatin cell densities increased significantly toward the values measured in control subjects. The insignificant changes in secretin and CCK cell densities could be secondary to the significant increase in somatostatin cell density, since both secretin69,70 and CCK 70 are inhibited by somatostatin. It is possible to stipulate that the improvement observed in IBS symptoms and as assessed by the Birmingham questionnaire particularly in the pain and diarrhea domains 12 after receiving dietary guidance may be ascribed to the significant changes in the cell densities of serotonin and somatostatin following dietary guidance.
The release of GI hormones is stimulated by food intake and depends on the meal composition, that is the proportions of carbohydrates, proteins, and fats. CCK release into the bloodstream is triggered by the consumption of a fat-rich meal, 71 while GIP is released after consuming carbohydrate- and fat-rich meals.72,73 The main trigger for enteroendocrine cells is the GI luminal content, especially the nutrients.13,74 Stem cells differentiate rapidly (within 2–6 days) into mature enteroendocrine cells.75,76 The densities of duodenal stem cells, expressing Musashi and endocrine cell progenitor Neurogenin 3 proteins were lower in IBS patients than in healthy control subjects. 45 The interactions between food and enteroendocrine cells are dynamic. 68 The changes in the densities of duodenal enteroendocrine cells may be caused by changes in clonogenic factors and/or the differentiation of stem cells.
Conclusion
The current study is the first to show that changing the diet can alter the densities of enteroendocrine cells in the duodenum, similarly to the diet-induced changes in the stomach,27,29 small intestine,31,32 and large intestine.28,30 The changes in the different enteroendocrine cell densities identified herein may have contributed to the previously reported improvement in IBS symptoms and the QOL of these IBS patients. 12 The results of the current study shed some light on the involvement of the enteroendocrine cells in the pathophysiology of IBS.
Authors’ contributions
TM planned the study, conducted the computerized image analysis, analyzed the results, and wrote the first draft of the manuscript. ME-S planned the study, recruited patients and control subjects, conducted gastroscopies, contributed to the data analysis, and commented on the manuscript.
Footnotes
Acknowledgements
This study was financially supported by a grant from Helse Fonna (project no.: 40415).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.