
Abstract
Immunologic thrombocytopenic purpura (ITP) is a condition that affects four to 18 per 100 000 children every year. In most cases, spontaneous remission occurs, but splenectomy may be proposed. Exploring the site of platelet sequestration can help to better predict potential poor responders to splenectomy, but 111In-radiolabeled platelet scintigraphy (IPS) can be difficult to perform in children with very few platelets. A 12-year-old boy suffering from refractory ITP was referred for evaluation of platelet survival and sequestration and consideration of splenectomy. His platelet count consistently remained below 10 000/mm3. An exceptional procedure was set up to use homologous platelets to perform the IPS. Splenectomy was ruled out based on the results of 111In-radiolabeled homologous platelet scintigraphy. The attending pediatrician intensified medical treatments, resulting in a significant improvement in platelet count. This increase in platelet levels allowed for 111In-radiolabeled autologous platelet scintigraphy, which confirmed the absence of splenic sequestration. This allowed us to reject splenectomy in this child. Homologous IPS could help clinicians to choose splenectomy as a treatment option for ITP in children with a very low platelet count, and its use should be promoted after failed thrombopoietin receptor agonist (TPO-RA) treatment. More systematic studies are needed to confirm the predictive response to splenectomy of homologous IPS.
Keywords
Introduction
111In-radiolabeled platelet scintigraphy (IPS) has demonstrated its utility in the study of platelet survival, enabling the investigation of the thrombocytopenia mechanism, and in the identification of a potential splenic sequestration.1-4 Immunologic thrombocytopenic purpura is a rare autoimmune disorder defined by an isolated thrombocytopenia under 100 000/mm3 caused by autoantibodies directed against platelets. Most children will resolve spontaneously in a matter of weeks to months, but occasionally chronic ITP may develop, necessitating therapeutic intervention. For patients who are not responding to medication, a splenectomy can be proposed for resolving ITP.5-7 Splenectomy is an interventional procedure that carries some inherent risk, thus its benefit-risk balance must be established before it is performed. Investigating the location of platelet sequestration could help in the prediction of individuals who may not respond well to splenectomy.4,8 Unfortunately, routine use is limited to those individuals with an adequate platelet count since the patient's own platelets are used as a marker in this investigation (autologous platelets). A minimum number of platelets is required for the test to be carried out correctly. When platelet levels are insufficient, it becomes necessary to carry out this examination using homologous platelets (from donors).
In theory, radiolabeling homologous platelets should not present difficulties, especially because platelet isolation processes are not required and radiolabeling techniques are efficient. Nevertheless, procedures must be adapted to thrombocyte conditioning—that is, formulation and packaging—and homologous platelet administration must follow good transfusion practices. Homologous IPS appears to be a safe and efficient technique for patients with a very low platelet count, and it has indeed been performed for many years.9,10 Its use in infants and children remains uncommon, essentially for rare diseases or chronic thrombopenia.11,12 Isolation of platelets from whole blood is not needed, given that they come from donors, and this make the specific labeling much easier as the lipophilic complex used is not platelet-specific. 13 Moreover, it is not necessary to collect a sample from the patient, which may be challenging with young children and infants.
Here, we discuss the case of a child suffering from chronic ITP who was unresponsive to thrombopoietin receptor agonist (TPO-RA), with very low platelet count and for whom splenectomy was being considered. To address this matter, we performed a homologous IPS, the results of which we then validated by performing an autologous IPS that ruled out splenectomy in this child.
Case Presentation
A 12-year-old male patient with ITP was referred to the Nuclear Medicine Department of Montpellier University Hospital for assessment of platelet lifespan and sequestration, with the potential consideration of splenectomy as a therapeutic option. The patient was refractory to therapies—corticosteroids, immunosuppressive agents, immunoglobulins and TPO-RA—and his platelet count consistently remained below 10 000/mm3 on romiplostim up to 400 μg per week (44 kg). Below this threshold, the number of platelets required for correct radiolabeling could not be obtained with a sample volume that was tolerable for his morphology. Two autologous IPS in two different hospitals failed due to the low platelet count, leading us to perform an IPS using homologous platelets. To confirm the results, an autologous IPS was performed remotely thereafter. A platelet count of approximately 33 000/mm3 was obtained after romiplostim treatment with progressive intensification up to the maximum recommended dose of 450 μg per week (10 μg/kg/week for 45 kg) following a 4-days pretreatment by intravenous immunoglobulins (1 g/kg) and prednisolone (4 mg/kg/day) 10 days prior. A summary of the patient's history is shown in Figure 1. He had been diagnosed with ITP in August 2020. He suffers from a moderate hemorrhagic syndrome, which affects both his parents’ mental health and his own quality of life. An anti-platelet antibody search revealed anti-glycoprotein IIb-IIIa and Ib-IX autoantibodies. The patient has A RH1 (D+) blood group phenotype, anti-HLA class I antibodies, and no irregular antibodies.

Flowchart of patient's history.
The radiolabeling process followed the French good preparation practices. 14 Platelets are isolated from blood after sampling for an autologous process or concentrated for a homologous process into a pellet. [111In]In-oxinate solution is used for platelet radiolabeling. [111In]In3+ has good radiopharmaceutical characteristics such as medium gamma energies (171-245 keV) and a radioactive period of 2.8 days, which allows for several days of monitoring. 15 As a metal cation in the +3 oxidation state, indium(III) oxine can easily coordinate with species that are abundant in electrons. The present radiolabeling process was simple and not specific, and it was validated quite some time ago: after buffering to pH 6, the [111In]In-oxinate complex can pass through cell membranes. It then dissociates and [111In]In3+ forms a bond with intracellular proteins.13,16
The platelet concentrate (PC) used in the homologous technique must be obtained by apheresis, irradiated, and strictly ABO/RH1 grouped and HLA compatible. The donor's platelets were collected, processed by filtration, quantified, and tagged the day before radiolabeling by the French Blood Establishment (EFS). Conformity and security controls upon receipt of the PC and pre-transfusion controls were carried out by the Hemovigilance Department. The use of PC for this technique is subject to an authorization issued by the French National Agency for the Safety of Medicines and Health Products (ANSM). This agency recommends that the PC be untreated with amotosalen, which could impact viability results. 17 Radiolabeling tests were carried out beforehand by radiopharmacists to validate the process and set up the procedure. Good transfusion practices were followed, and an infusion set with a 200-µm filter was used to block any small aggregates that may have been present in the PC, as required for classic platelet transfusion. 18
Radiolabeled platelets were injected by a catheter at the elbow crease, 15 MBq and 6 MBq for the homologous and autologous IPS, respectively. Since the first exam results were good, we decided to halve the dose for the second exam in order to minimize the child's radiation exposure. The patient received ongoing monitoring of his clinical parameters, as well as pharmacovigilance and hemovigilance follow-up in case of any adverse event.
The same data collection and data analysis procedures were carried out for the IPS in both homologous and autologous settings. Blood samplings were performed from the contralateral arm at 0.5, 1, 3, 24, 48, 72 h post-injection (an additional 96-h sample for the autologous IPS). Radioactivity measures were performed with a gamma counter (Wizard 1480®, Perkin Elmer) to evaluate platelet lifespan. The platelet half-life was determined graphically. Static acquisitions in anterior and posterior views of the thoraco-abdominal region were performed 0.75, 1, 4, 24, 48, 72 h post-injection using a dual-head NM/CT 870-DR gamma camera equipped with middle-energy, general-purpose, parallel-hole collimators (GE Healthcare, Tirat Carmel, Israel) (an additional 96-h image for the autologous exam). Anterior and posterior images were acquired simultaneously and geometrically averaged. Platelet sequestration was determined from a radioactivity count in a region of interest (ROI) traced around an organ and normalized by the activity measured in that organ 45 min after administration of radiolabeled platelets. Late sequestration was defined as splenic or hepatic if the ratio exceeded 1.2. 3
Case Outcome
The activity measured in the blood samples decreased exponentially between 30 min and 72 h. A significantly reduced homologous and autologous platelet lifespan was observed in the two exams. Homologous and autologous platelet half-life was calculated after an exponential fit at 1.80 and 4.70 h, respectively (Figure 2), for an expected lifespan of around 9 days ± 1 day in healthy subjects with a threshold for test negativity estimated at 6 days.19,20

Same patient's blood activity after homologous (left) and autologous (right) 111In-radiolabeled platelet injection.
The splenic and hepatic ratios remained below 1.2 at all time points for both the homologous and autologous tests. Only the splenic uptake ratio at 24 h appeared at the level of the upper threshold—that is, 1.2, for the autologous test. Other ratios were under 1.2 (Figure 3).

Same patient's spleen and liver ratios after homologous (left) and autologous (right) 111In-radiolabeled platelet injection (spleen at t / (spleen t = 0) and liver at t / (liver t = 0)).
The images obtained with the two techniques were visually comparable. A lower count rate (and higher background noise) was noted for the examination with autologous platelets. This was consistent with the lower rate of marked platelets in the case of the autologous exam. Figure 4 shows imaging results of the homologous and autologous 111In-radiolabeled platelet injections immediately after injection and 3 days later.
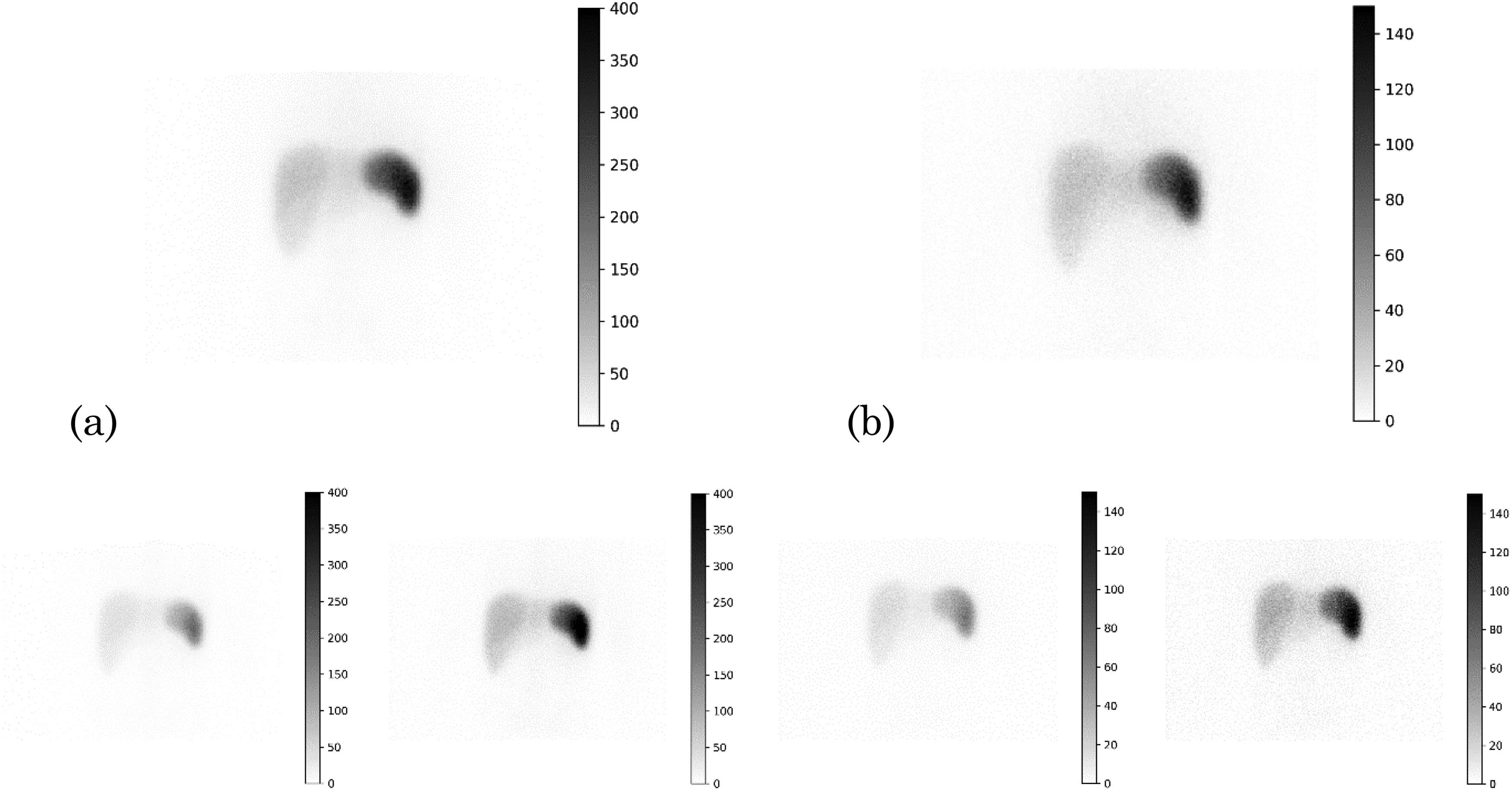
Same patient's acquisition after (a) homologous and (b) autologous 111In-radiolabeled platelet injection. Top image: t = 0.5-h geometrical means (decay corrected), bottom images: t = 72-h geometrical means (with decay uncorrected on the left and decay corrected on the right).
During both exams, the patient was treated by TPO-RA and the possibility of interference with the exam was raised. One study showed that TPO-RA may overcompensate the platelet destruction in ITP and reduce the platelet destruction rate. 21 Another more recent study suggested that TPO-RA does not modify either the site of platelet destruction or the platelet survival and pointed out that the increased estimated platelet production is not sufficient to overcome the platelet destruction by the immune system. 22 As there was no difference between the results of the homologous and autologous exams, we concluded that there was no interference from TPO-RA treatment.
In this case, avoiding splenectomy, which certainly would not have improved the ITP severity, was important both physically and psychologically. An uncommon ITP phenomenon, identified as diffuse endovascular destruction of immunological cause, was then diagnosed. The splenectomy option was ruled out and the TPO-RA treatment was kept up to the maximum recommended dose. One year after the autologous IPS, the patient remained stable, on a dose of 500 μg (10 μg/kg/week for 50 kg) of romiplostim per week only, with a platelet count between 85 000 and 100 000/mm3.
Discussion
We conducted a platelet lifespan evaluation and explored a potential sequestration site in a young patient with severe thrombocytopenia associated with an ITP therapeutic escape. Homologous 111In-radiolabeled platelets were used to perform the examination with a platelet count of 9000/mm3. The results showed no significantly different in-vivo behavior between the homologous and autologous platelets, and this supports the possibility of using homologous platelets for this procedure.
There is insufficient evidence to support strong recommendations on how to manage ITP. Splenectomy is a second-line therapy, after corticosteroids, TPO-RA and rituximab, and it is generally delayed for at least 1 year after diagnosis. Older and current international recommendations do not mention platelet survival and sequestration examination prior to choosing splenectomy in ITP.5,23,24 Recent studies have demonstrated that IPS is useful to guide treatment.8,25 Platelet sequestration explorations are known to be effective predictors of a good response to splenectomy in the case of isolated splenic sequestration in ITP. Splenectomy can be avoided if no splenic sequestration, mixed sequestration, or hepatic sequestration is shown, indicating a platelet destruction mechanism unrelated to hypersplenism.3,26-28 New prospective studies using improved methodology are still required to support the interest of IPS for the indication of splenectomy in the management of ITP, even though various studies are pointing in the same direction.
Although splenectomy is considered as standard without actual recommendation for looking at platelet sequestration prior to surgery, it is important to note that some patients do not completely respond to splenectomy even with proved splenic sequestration by IPS. 29 It is advisable to avoid unnecessary splenectomies in children, as it is important for them to remain protected against infections caused by particularly encapsulated bacteria, without antibiotic prophylaxis or vaccination, especially as it is acknowledged that many children are likely to experience spontaneous remission of ITP. 24 IPS is a non-invasive investigation that can be used relatively easily to guide the decision to undergo splenectomy.
Conclusion
Results of the homologous procedure were validated remotely with an autologous IPS carried out following the intensification of TPO-RA treatment. The use of homologous platelets should remain the exception in cases where the patient's platelet count is too low for autologous radiolabeling due to transfusion issues and the difficulty of PC supply and storage with a shelf-life of 5 to 7 days. However, homologous IPS could help clinicians to choose splenectomy as a treatment option for ITP in children with a very low platelet count after failed optimized TPO-RA treatment. In addition, more systematic studies on larger populations are needed to confirm the indication and predictive response to splenectomy of homologous IPS.
Footnotes
Acknowledgements
We would like to thank Aurélie Conte and the French Blood Establishment (EFS) for their work and for allowing us to carry out the homologous test by providing the donor's platelets.
Authors’ Contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by Julien Dubois, Aurélie Bourdon, Florentin Kucharczak and Tom Paunet. The first draft of the manuscript was written by Julien Dubois and all authors commented on the successive versions of the manuscript. All authors read and approved the final manuscript.
Consent to Participate
Written information was given to the patient's parents for participate.
Consent for Publication
Written information was given to the patient's parents for publication of this case report and its accompanying images.
Data Availability
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Declaration of Conflicting Interest
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Considerations
This study was conducted in accordance with the ethical standards as laid down in the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. It was approved by the Montpellier University Hospital's local Institutional Review Board under the No. 2024-01-010 on 5 February 2024.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.