
Abstract
Bongkrekic acid (BKA) poisoning is a rare but highly lethal foodborne illness caused by the mitochondrial toxin produced by Burkholderia gladioli pv. cocovenenans. Historically concentrated in Indonesia and China, recent outbreaks in Africa and North America underscore its global public health relevance. A comprehensive literature search was conducted in PubMed and China National Knowledge Infrastructure, supplemented by manual searches. A total of 91 studies were included. Outbreaks are mainly linked to traditional fermented foods such as tempe bongkrek, rice noodles, and corn products, with case fatality rates ranging from 30% to 100%. BKA irreversibly inhibits adenine nucleotide translocase, leading to profound mitochondrial dysfunction and multiorgan failure. Clinically, poisoning progresses rapidly from gastrointestinal symptoms to severe hepatic, renal, and neurological damage. Liquid chromatography–tandem mass spectrometry remains the gold standard for confirmation, while immunoassays and molecular tools provide rapid screening in outbreak settings. Despite advances in detection and mechanistic understanding, prevention is hindered by the toxin’s heat stability and its association with traditional food practices. Enhanced surveillance, point-of-care diagnostics, and targeted public education in high-risk regions are urgently needed.
Introduction
Bongkrekic acid (BKA) is a lethal foodborne toxin first identified in the late 19th century in Indonesia (Anwar et al., 2017), when fatal outbreaks were linked to the consumption of tempe bongkrek, a traditional fermented coconut-based product contaminated by Burkholderia gladioli pv. cocovenenans (Garcia et al., 1999). Since then, BKA poisoning has been documented predominantly in Indonesia and China. Although improved regulations have reduced outbreak frequency, BKA poisoning remains a significant global public health threat, particularly in rural communities where traditional food practices persist, as evidenced by outbreaks linked to tempe bongkrek, fermented corn products, rice noodles, black fungus, and traditional homemade beer (Hu et al., 1989; Gudo et al., 2018; Su, 2024).
The clinical and public health significance of BKA poisoning lies in its extremely high case fatality rate (CFR), which varies across outbreaks and is dependent on the efficacy of the health care response (Han et al., 2023; Chen XL et al., 2025; Su, 2024). Unlike many other foodborne illnesses, BKA intoxication has no specific antidote, progresses rapidly, and frequently results in multiple organ dysfunction syndrome (Hu et al., 2025).
In recent years, multiple analytical and immunological methods have been developed for the detection of BKA in food and biological samples. High-performance liquid chromatography (HPLC) and liquid chromatography–tandem mass spectrometry (LC–MS/MS) remain the gold standards due to their high sensitivity and specificity for quantitative determination. Immunoassay-based techniques, such as enzyme-linked immunosorbent assay (ELISA) and colloidal gold immunochromatographic strips, enable rapid screening in field settings (Gao et al., 2025). These advances have significantly improved diagnostic capacity, although their application in routine surveillance remains limited.
Given its high fatality and the ongoing challenges in management and prevention, the purpose of this review is to provide a comprehensive synthesis of BKA poisoning pathophysiology, clinical features, epidemiology, and highlight recent advances in toxin detection and public health interventions.
Materials and Methods
This review was conducted in accordance with Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. A comprehensive literature search was performed using PubMed database and the China National Knowledge Infrastructure to identify studies published between 1950 and 2025, the period during which most documented outbreaks of BKA poisoning have been reported. In addition, Google was used as a supplementary source for manual website and citation searching to identify relevant reports and publications not indexed in the above databases.
The search strategy combined the following keywords and Medical Subject Headings terms: “bongkrekic acid,” “Burkholderia gladioli,” “foodborne toxin,” “poisoning,” “epidemiology,” “case report,” “management,” “toxicology,” and “outbreak,” using Boolean operators (AND, OR) as appropriate.
Eligible articles included original studies (case reports, outbreak investigations, epidemiological analyses, toxicological studies, and clinical trials where available), as well as authoritative surveillance reports relevant to BKA poisoning. Reports in both English and Chinese were considered to capture the largest number of outbreak investigations, particularly from China and Indonesia, where most cases occurred.
Titles and abstracts were screened, and full-text articles were assessed for eligibility. Data were extracted on epidemiology, food sources, pathogenesis, toxicokinetics, clinical manifestations, diagnostic approaches, treatment, and prevention strategies.
Results
A total of 217 records were identified from databases, of which 91 remained after duplicate removal. Following screening and full-text assessment, 49 English-language and 37 Chinese-language studies were included in the final synthesis. Additional 5 references were identified through manual website and citation searching (Fig. 1).

PRISMA flowchart.
Among the English-language literature on Burkholderia gladioli and BKA poisoning, research was distributed across several domains: case analyses (n = 4), epidemiological investigations (n = 3), detection methods (n = 12), genomic studies (n = 7), toxicity mechanisms (n = 6), contamination surveys and risk assessments (n = 10), and others (n = 7).
The Chinese-language publications primarily addressed applied and methodological aspects. These included case analyses (n = 3), epidemiological investigations (n = 4), detection methods (n = 21), and contamination surveys and risk assessments (n = 9).
Pathophysiology
Toxin origin, biosynthesis, and toxicological properties
BKA is produced by Burkholderia gladioli pv. cocovenenans, a Gram-negative bacterium first reclassified from Pseudomonas cocovenenans in the 1980s (Jiao et al., 2003). Its molecular formula is C28H38O7 (molecular weight 486.61), and it is odorless and tasteless (Hu et al., 1989). The bongkrekic acid biosynthetic gene cluster (bon BGC) encodes enzymes responsible for BKA biosynthesis, with genomic studies revealing significant variability across strains (Peng et al., 2021). Strains harboring the complete cluster are capable of producing lethal amounts of BKA, while others may lack or carry incomplete clusters and are nontoxigenic (Chen J et al., 2025).
BKA production is highly substrate-dependent. Coconut press cake, corn flour, and rice noodles provide favorable growth environments. Lipid-rich substrates, such as coconut, enhance toxin synthesis (Garcia et al., 1999). Environmental conditions, including warm temperatures (25–30°C), neutral to slightly acidic pH, and prolonged storage facilitate bacterial proliferation and toxin accumulation (Huang et al., 2025).
BKA is heat-stable and resistant to boiling, frying, and steaming (Moebius et al., 2012). Cooking does not inactivate the toxin, making prevention dependent on eliminating contamination rather than culinary practices. BKA is also chemically stable under acidic and alkaline conditions, and thus persists in diverse food environments (Zhao et al., 2025).
Molecular mechanism of toxicity
The pathophysiological severity of BKA intoxication is profoundly potentiated by its pronounced stability. The heat-stable and chemically inert nature of the toxin allows it to traverse the gastrointestinal tract unscathed, ensuring its full bioactivity is delivered to cellular targets (Anwar et al., 2017).
BKA primarily targets the mitochondria. It binds irreversibly to the adenine nucleotide translocase (ANT) located in the inner mitochondrial membrane. ANT is responsible for exchanging ADP and ATP between mitochondria and the cytosol, an essential step in oxidative phosphorylation (Kiranadi et al., 1991). By inhibiting this transport, BKA causes a collapse of ATP synthesis, profound cellular energy depletion, inhibition of mitochondrial respiration, increased reactive oxygen species generation, and mitochondrial swelling and rupture that trigger necrosis and apoptosis (Li H et al., 2023). Consequently, the collapse of oxidative phosphorylation and the ensuing energetic failure are not transient but relentless, driving the progression of multiorgan damage (Shi et al., 2019). Additionally, BKA can inhibit the decoupling of mitochondrial oxidative phosphorylation caused by ATP-dependent potassium channel opening (Moebius et al., 2012). Animal models and cellular experiments further reveal that BKA exposure triggers neutrophil extracellular trap formation and autophagy dysregulation, amplifying tissue injury (Zhou et al., 2025). These mechanisms explain the toxin’s multiorgan tropism, with the liver, kidneys, heart, and central nervous system being most vulnerable due to their high energy demands.
Detection
Gold-standard detection: LC-MS/MS and sample preparation
Reliable detection of BKA and its producer (Burkholderia gladioli pv. cocovenenans) is central to outbreak confirmation, clinical management and forensic attribution. Instrumental chromatographic methods, particularly LC-MS/MS/UPLC-MS/MS, currently represent the laboratory gold standard for quantitative confirmation of BKA in food and biological specimens due to their high sensitivity, selectivity and ability to resolve BKA from its isomer IBKA and complex food matrices (Han et al., 2023; Gao et al., 2025).
Various LC-MS/MS-based methods have been developed and applied to diverse matrices, with multiple studies reporting limits of detection (LOD) in the low µg/kg to sub-µg/kg range and acceptable recoveries when appropriate extraction and cleanup are applied (Hu et al., 2022). For instance, Zhao et al. (2025) established a UPLC-MS/MS method for the simultaneous detection of BKA and dehydroacetic acid, while Hu et al. (2022) developed a PRiME purification-based UHPLC-MS/MS method for the concurrent determination of BKA and multiple aflatoxins. For specific food matrices like fresh Tremella fuciformis, methods employing isotope internal standard-UPLC-MS/MS have been developed for the simultaneous determination of BKA and its isomer Iso-BA (Xia et al., 2024). The application extends to clinical settings, where isotope dilution-based LC-MS/MS methods enable rapid and sensitive determination of BKA and Iso-BA in human plasma and urine (Fang and Qiu, 2022). High-resolution mass spectrometry (HRMS) techniques such as UPLC-Q-Orbitrap-HRMS (Han et al., 2021) and liquid chromatography electrospray ionization time-of-flight mass spectrometry (LC-ESI-TOF/MS) (Li et al., 2018) have been utilized for the rapid screening and confirmation of BKA, offering powerful qualitative capabilities through the provision of accurate mass numbers for parent and fragment ions.
The success of these methods heavily relies on efficient sample preparation, which is essential for reducing matrix interference and improving analyte recovery. These include not only conventional approaches such as liquid–liquid extraction, solid-phase extraction (SPE), but also more advanced methodologies such as Quick, Easy, Cheap, Effective, Rugged and Safe (QuEChERS), various dispersive-SPE formats (e.g., using enhanced matrix removal-lipid or magnetic composites like Fe3O4/HNTs) (Zhao et al., 2025; Hu et al., 2022; Liang et al., 2021; Fang et al., 2023), as well as techniques like dispersive liquid–liquid microextraction based on solidification of floating organic drop (DLLME-SFO) (Huang et al., 2022a) and mixed-mode weak anion exchange SPE (Li et al., 2016). Comparative method papers show recoveries typically 80–105% across rice noodles, cornmeal, white-fungus, and related matrices when optimized procedures are used (Liang et al., 2021; Zou et al., 2021). However, viscous or colloidal samples, such as Auricularia auricula, often result in lower recoveries or larger matrix effects unless additional cleanup or tailored pretreatment is applied (e.g., optimized adsorbent type, extractant composition) to reduce analyte loss and improve accuracy (Huang et al., 2022b).
For clinical matrices (blood, gastric contents, liver, urine, vomitus), LC-MS/MS methods have been established and shown to detect BKA in postmortem and antemortem samples; however, several practical challenges remain: (1) plasma exchange or extracorporeal therapies can markedly reduce circulating BKA and produce false negatives; (2) sample stability and matrix effects require validated extraction procedures for each tissue type; (3) delayed sampling or disposal of implicated food hampers outbreak confirmation.
Immunoassay-based rapid screening and molecular approaches
Given that traditional instrumental analyses are time-consuming and require centralized laboratories, researchers have prioritized rapid on-site assays for outbreak triage. A range of immunoassay-based rapid detection methods, including ELISA (Wu et al., 2024), colloidal gold lateral flow immunochromatographic assays (Cao et al., 2023b; Lin et al., 2023), fluorescent immunochromatographic assays (Lin et al., 2024), and immunoassays (IA) (Xuan et al., 2024), have been developed and validated in China for on-site screening. Time-resolved fluorescent immunochromatography, which achieves a LOD of 1.0 µg/kg and shows strong correlation with LC-MS/MS results (R2 = 0.99) (Chen YJ et al., 2025); flow cytometry fluorescence immunoassay, with a LOD of 0.56 µg/kg and cross-reactivity rates of less than 0.1% with other mycotoxins (Lu et al., 2025); a dual-modular immunosensor for BKA was constructed based on a specific monoclonal antibody, integrating both colorimetric and fluorescent readouts, demonstrating good sensitivity (IC50 = 17.9 ng/mL in ELISA) and reproducibility in food samples (Cao et al., 2023a). These methods demonstrate detection limits suitable for a variety of food matrices, typically in the low µg/kg range, along with acceptable recovery rates. However, they are prone to matrix interference and cross-reactivity and exhibit lower absolute sensitivity compared with LC-MS/MS. Thus, they should be primarily employed for preliminary screening, with positive results confirmed via LC-MS/MS.
Molecular detection of the pathogen (BGC) complements toxin analysis. Real-time fluorescent PCR can specifically detect B. gladioli pv. cocovenenans in about 1 h, with an LOD of 650 colony forming unit (CFU)/mL for bacterial suspensions (Wang et al., 2022); Droplet digital PCR (ddPCR) significantly shortens detection time compared with the plate counting method, achieving an LOD of 361 CFU/mL in contaminated glutinous rice soup (Li HJ et al., 2023). Furthermore, fluorescent probe-based loop-mediated isothermal amplification enables visual detection within 30 min, with LODs of 1.98 pg/μL for genomic DNA and 270 CFU/mL for bacterial suspensions, providing a powerful tool for rapid on-site detection (Yao et al., 2023). Clustered Regularly Interspaced Short Palindromic Repeats (CRISPR)/Cas12a system combined with recombinant enzyme polymerase amplification (RPA-CRISPR/Cas12a) (Zheng et al., 2023) and targeted sequencing (Wang et al., 2024), permits rapid, culture-independent identification of toxigenic strains and the bon BGC. These methods are valuable when toxin levels are low or when plasma exchange/clinical interventions have reduced measurable BKA in patient samples. However, they cannot differentiate between viable and nonviable pathogens or directly quantify functional toxins, potentially leading to false positives. Despite their technical requirements and cost, these techniques remain essential complements to direct toxin analysis in outbreak investigations and food safety monitoring.
Clinical Features
Symptoms and signs of BKA poisoning
The symptoms and signs of BKA poisoning are broadly consistent with those caused by other mitochondrial toxins, but the severity and rapid clinical progression distinguish it as a uniquely lethal foodborne disease. The initial manifestations typically occur within 0.5–24 h of ingestion of contaminated food. Early symptoms are dominated by gastrointestinal distress, including nausea, vomiting, abdominal discomfort, bloating, diarrhea, and in some cases, bloody stools (Li et al., 2019). These nonspecific features often lead to initial misdiagnosis as viral gastroenteritis or foodborne bacterial infection.
As poisoning progresses, systemic toxicity rapidly emerges, manifesting as hepatic injury (hepatomegaly, ascites, jaundice, subcutaneous hemorrhage, and in severe cases, hepatic encephalopathy), renal involvement (hematuria, oliguria or anuria, and acute kidney failure), neurological complications (dizziness, drowsiness, headache, progressing to seizures, convulsions, or coma) (Shi et al., 2019). In advanced stages, multiorgan dysfunction involving the liver, kidneys, and central nervous system leads to rapid deterioration and often death from respiratory or circulatory failure (Hu et al., 2024). Based on the synthesized evidence, several factors can serve as predictors of severity. These include a short latency period (especially < 6 h) from ingestion to symptom onset, suggesting a large toxin dose; early and profound metabolic acidosis and hypoglycemia in laboratory findings; a rapid rise in liver transaminases and bilirubin; and the early development of oliguria or anuria. The presence of these features should alert clinicians to a high risk of mortality and necessitate aggressive supportive interventions. Limited human toxicokinetic data indicate that BKA is metabolized slowly, with a long half-life and high peak plasma concentration, resulting in sustained toxicity (Hu et al., 2024; Rivera Blanco et al., 2024; Lv et al., 2023).
Pathological changes
The earliest pathological changes occur in the gastrointestinal mucosa, with congestion and edema. Following absorption, BKA induces acute hepatocellular injury, characterized by liver atrophy, widespread hepatocyte necrosis, and destruction of the lobular architecture (Hu et al., 2024). With systemic dissemination, multiorgan damage becomes evident, including renal tubular necrosis with casts, pulmonary edema, cerebral edema, and, in some cases, brain herniation. Forensic autopsies frequently reveal hepatocyte necrosis, disorganized hepatic lobules, multiorgan congestion, and hemorrhage, supporting the pathological evidence of BKA’s systemic toxicity (Chen XL et al., 2025).
Epidemiology
Historical data highlight that BKA poisoning caused significant mass casualties in Indonesia and China throughout the 20th century, with CFRs often exceeding 30%. From the 1950s to the 1980s, Indonesia documented several outbreaks involving hundreds to thousands of cases, such as the 1975 outbreak in Java that affected over 1000 individuals and resulted in 125 deaths. Similarly, China experienced severe outbreaks in its northeastern provinces (Heilongjiang, Jilin, and Liaoning) between the 1950s and 1970s, with outbreaks linked to contaminated fermented corn and sorghum products leading to over 700 deaths (Anwar et al., 2017).
While this historical pattern is well-established, this review focuses its subsequent detailed analysis on outbreaks from the 21st century (Table 1) to underscore recent trends and the persistent threat of BKA poisoning.
Summary of Outbreaks, Year, Number Affected, and Deaths Related to Bongkrekic Acid Poisoning, 2000–2025
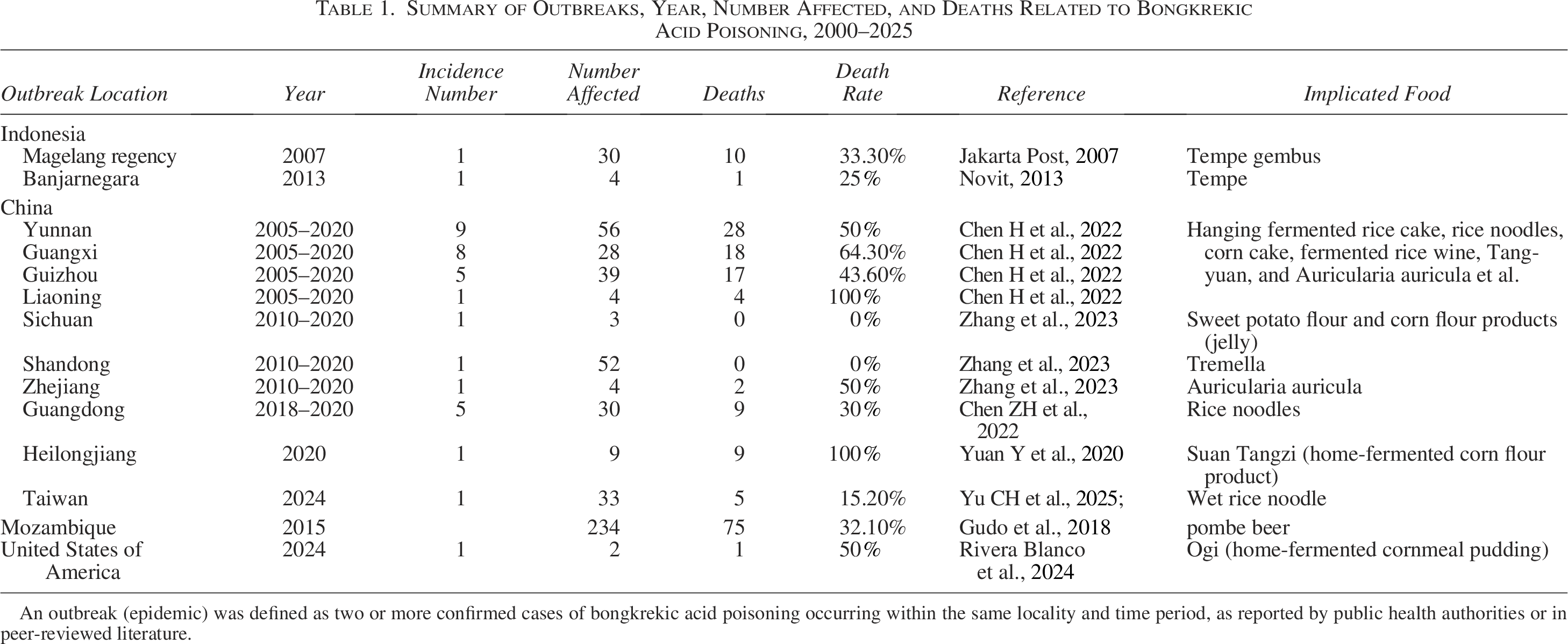
An outbreak (epidemic) was defined as two or more confirmed cases of bongkrekic acid poisoning occurring within the same locality and time period, as reported by public health authorities or in peer-reviewed literature.
In Indonesia, the commercial production and sale of tempe bongkrek have been officially banned since the 1980s due to its association with fatal food poisoning outbreaks. The traditional preparation involves fermenting coconut press cake (bungkil kelapa) with the mold Rhizopus oligosporus, a process during which the bacterium Burkholderia gladioli pv. cocovenenans can contaminate the substrate and produce lethal toxins (Garcia et al., 1999; Buckle and Kartadarma, 1990). Despite the official prohibition, sporadic outbreaks linked to homemade products persist in rural areas of Indonesia, underscoring the challenges in regulating traditional food practices. More broadly, other traditional fermented foods, particularly tempe gembus (made from okara) and other types of tempe, have also been implicated in outbreaks. This highlights that the safety risk is not confined to a single banned product but is a broader issue within informal food production systems. Outbreaks include incidents in Magelang regency in 2007 (30 cases, 10 deaths) and in Banjarnegara in 2013 (4 cases, 1 death), highlighting its ongoing public health risk (Jakarta Post, 2007; Novit, 2013).
In China, numerous smaller outbreaks were reported across multiple provinces, including Yunnan (56 cases, 28 deaths), Guangxi (28 cases, 18 deaths), Guizhou (39 cases, 17 deaths), Liaoning (4 cases, 4 deaths), Sichuan (3 cases, 0 deaths), Shandong (52 cases, 0 deaths), and Zhejiang (4 cases, 2 deaths). These incidents were associated with a variety of contaminated foods such as hanging fermented rice cake, rice noodles, corn cake, fermented rice wine, Tang-yuan, Auricularia auricula and other fermented corn flour products. (Chen H et al., 2022; Zhang et al., 2023). A particularly severe outbreak took place in Heilongjiang Province in 2020, linked to contaminated homemade fermented corn noodles (suan tangzi), which resulted in 9 deaths among 9 cases (100% CFR) (Yuan et al., 2020). Further cases were reported in Guangdong Province from 2018 to 2020 (30 cases, 9 deaths) and in Taiwan in 2024 (33 cases, 5 deaths), all associated with rice noodle products (Chen ZH et al., 2022; Yu et al., 2025; Zhang et al., 2023).
The first African outbreak occurred in Mozambique in 2015, led to 234 cases and 75 deaths, was linked to the consumption of traditional pombe beer, a traditional homemade alcoholic beverage brewed from corn flour (Gudo et al., 2018).
The first North American case of fatal BKA poisoning occurred in the United States (2 cases, 1 death), linked to the consumption of ogi, a traditional home-fermented cornmeal pudding (Rivera Blanco et al., 2024).
Conclusions
This review synthesizes the current, albeit fragmented, evidence on BKA poisoning. We now know that BKA is a potent mitochondrial toxin, consistently linked to the consumption of traditionally fermented foods like tempe bongkrek and corn-based products in regions of Asia and Africa. Its disruption of oxidative phosphorylation underpins the rapid progression to severe, often fatal, multiorgan failure. Although advances in analytical chemistry have improved the detection of BKA in food and biological samples, with methods ranging from gold-standard LC-MS/MS for confirmation to rapid IA and innovative molecular techniques for on-site screening, diagnostic and therapeutic options remain limited. Currently, no specific antidote is available, and treatment is mainly supportive.
Future efforts should more closely align with the foodborne nature of this toxin and target key stages in its transmission and control. Specifically, priorities should include: (1) development of affordable, field-deployable diagnostic tools for rapid detection of Burkholderia gladioli and BKA in fermented or starch-based foods, (2) strengthening food safety education and hygiene management among producers and consumers in high-risk settings, particularly in tropical and rural areas; and (3) integrating international collaboration into a coordinated foodborne disease surveillance and early-warning framework. Addressing these gaps through a food system-based approach will enhance prevention, early detection, and response capacity, ultimately reducing the global burden of BKA poisoning.
Authors’ Contributions
Y.H. performed the literature search, data extraction, and wrote the original draft of the article. Z.L., L.S., R.J., D.M., and W.B. assessed the risk of bias and quality. B.Y. and S.M. were responsible for supervision and the final content. All authors have read and agreed to the published version of the article.
Footnotes
Acknowledgments
The authors are grateful to the Foodborne Pathogens and Disease editorial team and the reviewers for their helpful suggestions that improved this article.
Funding Information
No funding was received for this article.
Disclosure Statement
The authors declare no conflicts of interest.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.