
Abstract
Background:
Lung cancer is the leading cause of cancer-related mortality, with non-small cell lung cancer (NSCLC) accounting for 80% to 85% of cases. While surgery and chemotherapy are primary treatments, their side effects—such as nausea, vomiting, and immunosuppression—significantly impact quality of life (QoL). Acupuncture and moxibustion, commonly used in Traditional Asian Medicine (TAM), are proposed to alleviate these effects, though their efficacy in NSCLC remains uncertain. This systematic review and meta-analysis evaluated their impact on QoL, chemotherapy-induced nausea and vomiting (CINV), and immune function in NSCLC patients.
Methods:
Nine databases (PubMed, Embase, Cochrane Library, CNKI, OASIS, ScienceON, KISS, KMBASE, and RISS) were searched for randomized controlled trials (RCTs) published until April 2025. RCTs comparing acupuncture or moxibustion with standard care in NSCLC patients were included. Primary outcomes were QoL (QLQ-C30, KPS); secondary outcomes included CINV and immune markers (CD3, CD4, CD8, CD4/CD8 ratio, TNF-α). Data were analyzed using Review Manager 5.4, and risk of bias was assessed using the Cochrane RoB tool.
Results:
Thirty-nine RCTs (N = 3610) were included. Acupuncture and moxibustion significantly improved QoL (QLQ-C30 MD = 12.39; KPS MD = 8.22; both P < .00001), reduced CINV incidence (RR = 0.32, P < .00001), and enhanced symptom relief (RR = 1.16, P < .00001). Immune function markers, including CD3 (MD = 7.20, P = .0002), CD4 (MD = 4.89, P = .0003), and the CD4/CD8 ratio (MD = 0.22, P < .00001), were significantly increased, while TNF-α levels decreased (MD = −11.05, P = .04).
Conclusion:
Acupuncture and moxibustion improve QoL, reduce CINV, and modulate immune function in NSCLC, supporting their complementary role.
Keywords
Introduction
Lung cancer is one of the most common cancers globally. According to the International Agency for Research on Cancer (IARC) in 2022, there were approximately 20 million new cancer cases worldwide, with lung cancer accounting for 2.4 million (12.4%) of them. It also had the highest mortality, with 1.8 million deaths (18.7%). 1 Lung cancer is classified into small cell lung cancer (SCLC) and non-small cell lung cancer (NSCLC) based on pathological and histological criteria, such as the size and morphology of the cancer cells. NSCLC, which makes up about 80% to 85% of all cases, includes adenocarcinoma, squamous cell carcinoma, and large cell carcinoma, while SCLC is highly malignant with frequent metastasis at the time of diagnosis. 2 The distinction between NSCLC and SCLC is crucial, as they differ in clinical course and treatment. Early-stage NSCLC may be treated surgically, but SCLC is often diagnosed at an advanced stage, limiting surgical options.
NSCLC poses diagnostic and treatment challenges due to a lack of early symptoms and limited screening markers, leading to late-stage diagnoses. 3 The prognosis remains poor, with a 5-year survival rate of less than 5% for advanced NSCLC patients. 4 Treatment for NSCLC includes surgery, chemotherapy, and radiotherapy, with chemotherapy often used as adjuvant therapy.5 -7 Chemotherapy for NSCLC uses cytotoxic agents, targeted therapies, and immunotherapies, though side effects such as gastrointestinal reactions and immunosuppression significantly impact patients’ quality of life. 8
Patients undergoing surgery or chemotherapy receive standard care, which is tailored to their condition and institutional guidelines. This typically includes managing side effects such as CINV, and postoperative pain, as well as nutritional and hydration support. Additionally, complication control, infection prevention strategies, respiratory exercises, and emotional and psychological support are commonly incorporated to ensure optimal recovery.
In Traditional Chinese Medicine (TCM), a variety of treatments, including general acupuncture, auricular acupuncture, electroacupuncture, and moxibustion are used as complementary therapies to alleviate symptoms such as fatigue, nausea, and pain associated with surgery and chemotherapy, thereby enhancing patients’ quality of life. Studies suggest that electroacupuncture, in particular, significantly reduce complications related to the lungs, potentially through mechanisms involving the regulation of inflammation and a reduction in plasma levels of inflammatory markers.9,10 Additionally, acupuncture and transcutaneous electrical acupoint stimulation (TEAS) have proven effective in reducing surgery-related complications, as well as in preventing recurrence and metastasis.11,12
A recent meta-analysis reported that acupuncture and moxibustion improved immune function across various solid tumors, including lung cancer. 13 However, because the review pooled heterogeneous tumor types and focused mainly on immunologic markers, its findings provide limited cancer-specific insight for non-small cell lung cancer (NSCLC). To address this gap, the present study focuses exclusively on NSCLC and evaluates a broader range of clinically relevant outcomes. This systematic review and meta-analysis aims to assess the efficacy of acupuncture and moxibustion in enhancing quality of life (QoL), reducing chemotherapy-related adverse effects such as nausea and vomiting (CINV), and improving immune responses in patients with NSCLC. Through this approach, the study seeks to clarify the potential role of acupuncture and moxibustion as a clinically meaningful therapeutic option in the management of NSCLC.
Methods
Study Registration
The protocol for this review was registered in PROSPERO (registration number CRD 42024523418). This review was conducted in accordance with the registered protocol. Any methodological updates, dates, or rationale for amendments were tracked through the PROSPERO record. PROSPERO allows multiple derivative publications to arise from a single protocol when they share the same overarching framework but address distinct analytic questions. Our project was prospectively planned as 3 related reviews (herbal medicine, 14 acupuncture/moxibustion, and breathing rehabilitation) under 1 protocol. For the current analysis, we focused specifically on acupuncture and moxibustion, evaluating patient-centered outcomes such as quality of life (QLQ-C30, KPS) and incidence of nausea and vomiting. While these outcomes differ somewhat from those initially registered, the analysis remains within the overarching scope of the original protocol, and these differences have been clarified in the Methods section without modifying the original PROSPERO record.
Search Method for Identifying the Studies
The studies included in the research were published up until April 2025, with no language restriction. The research was conducted exclusively using online databases, including PubMed, Ovid Medline, Embase, Cochrane Library, CNKI, OASIS, ScienceON, KISS, KMBASE, and RISS. A detailed search strategy is provided in the Supplemental material. This study focused only on articles available online.
Study Inclusion Criteria
Studies were included based on the following PICOS criteria:
Population (P)
Patients diagnosed with non–small cell lung cancer (NSCLC), regardless of age, sex, ethnicity, disease duration, or cancer stage. All participants were receiving standard oncologic treatment (eg, surgery, chemotherapy).
Intervention (I)
Standard care combined with acupuncture or moxibustion. Among the included trials, the most commonly applied modalities were manual acupuncture, electroacupuncture, auricular acupuncture, and forms of moxibustion such as indirect or warm moxibustion.
Comparator (C)
Standard treatment alone (eg, chemotherapy-based regimens, antiemetic therapy, analgesics, gastrointestinal prophylactic medications), or standard treatment combined with sham transcutaneous electrical acupoint stimulation (TEAS) in sham-controlled trials.
Outcomes (O)
Quality of life (QoL), chemotherapy-induced nausea and vomiting (CINV), and immune function outcomes.
Primary Outcomes
Quality of Life Questionnaire-Core 30 (QLQ-C30), and Karnofsky Performance Status (KPS). Both tools are standardized instruments widely used to evaluate changes in the quality of life of cancer patients following treatment. The QLQ-C30 score includes both functional and symptom assessments, evaluating various domains related to quality of life, whereas the KPS score focuses on assessing the patient’s functional abilities and performance in daily activities.
Secondary Outcomes
Incidence and efficacy rates of nausea and vomiting. To determine the clinical utility of acupuncture and moxibustion in patients with lung cancer, both the incidence and efficacy rates of nausea and vomiting were evaluated.
Tertiary Outcomes
T lymphocytes (CD3, CD4, CD8, CD4/CD8 ratio), and plasma levels of TNF-α. T lymphocytes play a crucial role in the immune system, with distinct functions for each subtype. This study utilized CD3, CD4, CD8 counts, and the CD4/CD8 ratio to assess immune status. CD3⁺ represents total T cells, CD4⁺ (helper T cells) reflects immune activation, and CD8⁺ (cytotoxic T cells) are involved in recognizing and eliminating cancer cells, indicating their capacity to suppress tumors and infections. 15 The CD4/CD8 ratio evaluates immune balance, and serves as a prognostic marker. Additionally, TNF-α, a key cytokine, regulates immune and inflammatory responses. These indicators were used to assess the immunological effects and clinical utility of acupuncture and moxibustion in lung cancer patients.
Study Design (S)
Randomized controlled trials (RCTs) published in peer-reviewed journals.
Study Exclusion Criteria
Studies were excluded if they were off-topic, duplicate literature, non-randomized trials (such as protocol papers, case reports, or review articles), in order to ensure a high level of evidence and homogeneity within the analyzed data.
Literature Screening and Data Extraction
Selection of Studies
Search results were imported into reference management software (EndNote 21), and duplicate studies were removed using the built-in duplicate removal function. 16 The first screening was conducted by 3 researchers (MSP, JHK and DHK) by reviewing titles, abstracts, and, if necessary, full texts. The second screening was performed by one researcher (MSP), who classified studies based on 3 specific outcome variables: (1) quality of life, (2) nausea and vomiting, and (3) immune response. Studies that did not match the topic or include at least one of the outcome variables were excluded. Any issues were discussed among the researchers.
Data Extraction
A full-text review was conducted on the selected studies, and data were extracted regarding the first author, study period, year of publication, participants, comparisons, interventions in treatment and control groups, outcomes, and adverse events. Study outcomes were categorized as continuous or binary, based on the outcome variables. This process was performed independently by 3 researchers (MSP, JHW, and DHK). In cases of missing data or discrepancies, the researchers consulted each other and contacted the first author for clarification.
Risk of Bias Assessment
The Cochrane Risk of Bias (RoB) Assessment Tool was used to assess the quality of the selected studies. Two researchers (MSP and JHK) participated the RoB assessment, and any disagreements were resolved through discussion with a third researcher (DHK). The assessment included 7 items: (1) random allocation implementation, (2) description of the randomization method, (3) blinding performance, (4) impact of blinding on outcomes, (5) dropouts reporting, (6) selective reporting, and (7) other influencing factors. The quality of evidence was then assessed using the GRADE system, which categorizes evidence as high (H), uncertain (U), or low (L). RCTs initially provide high-quality evidence, but this can be downgraded due to significant issues such as bias, inconsistency, indirect evidence, or imprecision, as well as publication bias. Conversely, evidence can be upgraded based on substantial effect sizes or a dose-response relationship. The quality of evidence for each outcome was summarized using a GRADE evidence profile, which offers a systematic evaluation of the evidence’s strength and highlights areas requiring further investigation.
Statistical Analysis
Review Manager Software 5.4 was used to analyze the data. 17 The risk ratio (RR) with a 95% confidence interval (CI) was used to measure dichotomous data. For continuous data, the mean differences (MD) with 95% CI were used to measure treatment outcomes on the same scale.
Heterogeneity was assessed using the I2 statistic, with values <50% considered low heterogeneity; in such cases, a fixed-effect model was used. When I2 ≥ 50%, indicating substantial heterogeneity, a random-effects model was applied. Because the included trials used several modality-specific forms of acupuncture and moxibustion, a certain degree of clinical heterogeneity was anticipated a priori. In cases of substantial heterogeneity (I2 ≥ 50%), sensitivity analyses were performed based on predefined study characteristics such as acupuncture or moxibustion, and chemotherapy regimens. If substantial heterogeneity remained unexplained, findings were cautiously interpreted, and a narrative synthesis was provided to discuss plausible reasons for discrepancies.
Results
Study Selection
We searched 9 online databases and initially identified 166 research papers published before April 2025. After excluding duplicates, we screened the titles and abstracts of the remaining 113 studies. This process led to the exclusion of 34 articles, leaving 77 for full-text review. Based on the selection criteria registered in PROSPERO, 38 studies were excluded for the following reasons: 9 did not target the appropriate population, 8 were not RCTs or were protocol studies, 12 involved inappropriate interventions, 9 reported irrelevant outcomes. Ultimately, 39 studies were included in the final review and analysis (Figure 1).

PRISMA 2020 flow diagram for systematic reviews which included searches of database and registers only.
Study Characteristics
In this study, we analyzed 39 RCTs published up to April 2025. The analysis included a total of 3610 patients who received acupuncture or moxibustion (including combined acupuncture and moxibustion treatment). In the experimental groups, Western medical treatments in the selected studies combined such as standard care, chemotherapy (including NP, TP, DP, GP, PC, etc.), and medication (eg, opioids, glucocorticoids, and antiemetic therapy) were combined with acupuncture and moxibustion interventions. The control groups primarily received only Western medical treatments. Additionally, 2 studies24,40 included sham-TEAS as an intervention in the control groups. The study duration ranged from 2 to 180 days, with detailed information provided in Table 1.
Characteristics of the Included Trials.
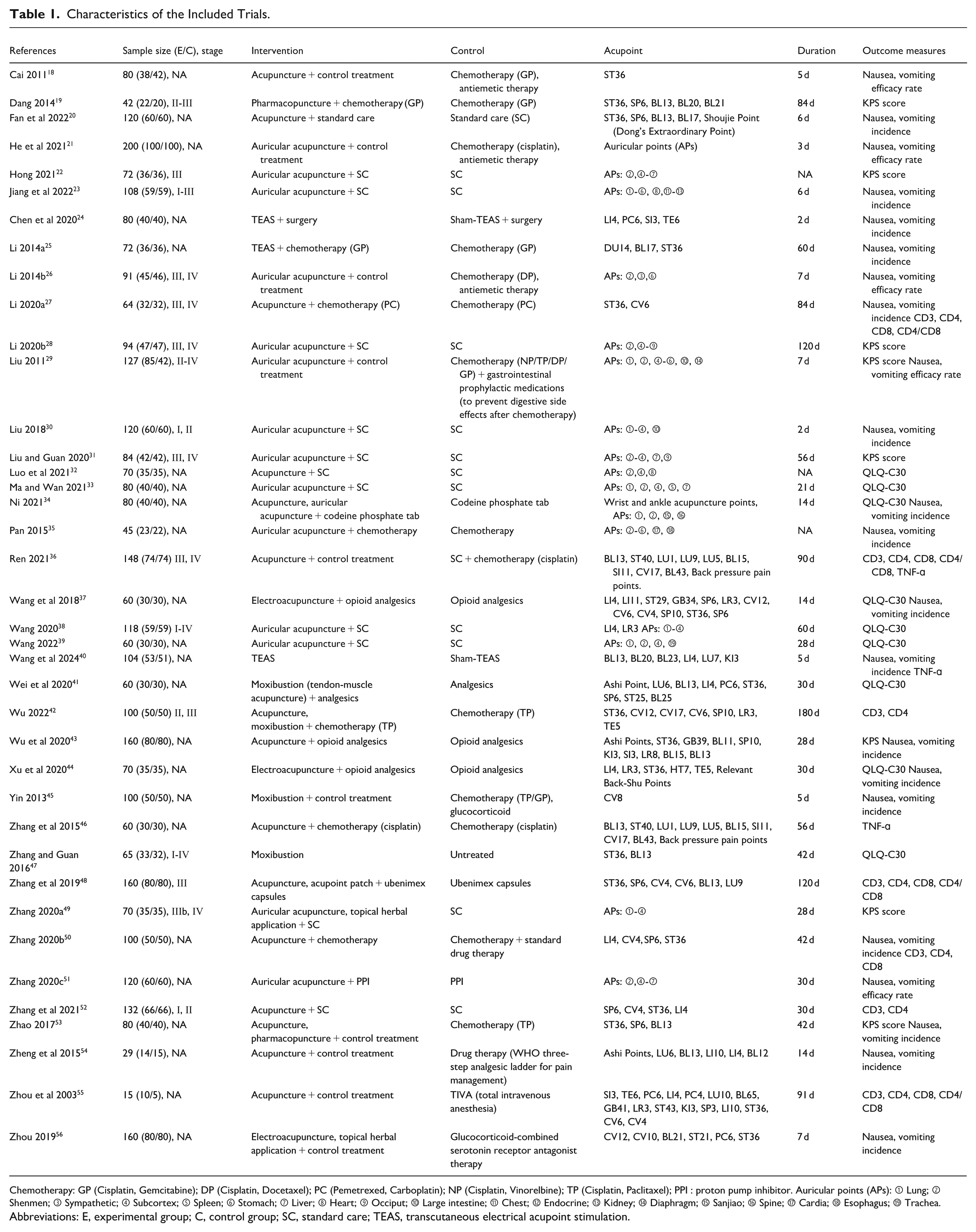
Chemotherapy: GP (Cisplatin, Gemcitabine); DP (Cisplatin, Docetaxel); PC (Pemetrexed, Carboplatin); NP (Cisplatin, Vinorelbine); TP (Cisplatin, Paclitaxel); PPI : proton pump inhibitor. Auricular points (APs): ① Lung; ② Shenmen; ③ Sympathetic; ④ Subcortex; ⑤ Spleen; ⑥ Stomach; ⑦ Liver; ⑧ Heart; ⑨ Occiput; ⑩ Large intestine; ⑪ Chest; ⑫ Endocrine; ⑬ Kidney; ⑭ Diaphragm; ⑮ Sanjiao; ⑯ Spine; ⑰ Cardia; ⑱ Esophagus; ⑲ Trachea.
Abbreviations: E, experimental group; C, control group; SC, standard care; TEAS, transcutaneous electrical acupoint stimulation.
Risk of Bias in Included Trials
Using the Cochrane Risk of Bias Assessment Tool, we found that all but 7 studies explicitly reported performing randomization, resulting in an overall low risk of bias. Most studies used random number tables for randomization, while others employed sealed envelopes or computer-generated randomization techniques. However, 5 studies that claimed to use randomization did not provide methodological details, leading to an unclear risk assessment for this aspect.
Blinding was generally not feasible in most studies, leading to a high risk of performance bias. This was primarily because acupuncture or moxibustion was applied only in the experimental group. However, 2 studies employed a sham-TEAS to achieve blinding, resulting in a low-risk of bias for those cases.
Several studies exhibited a high risk of bias due to discrepancies in participant numbers between the experimental and control groups caused by dropouts. In cases where there were no dropouts, but the initial study design assigned different numbers of participants to the experimental and control groups, the risk was rated as unclear. Additionally, all included studies were assessed as having an unclear risk due to the absence of protocol papers.
All but one study were assessed as having a low risk of attrition and other biases. However, selective reporting bias was rated as unclear for all studies due to the lack of protocol documentation.
Overall, while most studies had a low risk of bias in randomization and outcome assessment, significant concerns remained regarding performance bias and allocation concealment, which could affect the overall reliability of these studies (Figures 2 and 3).
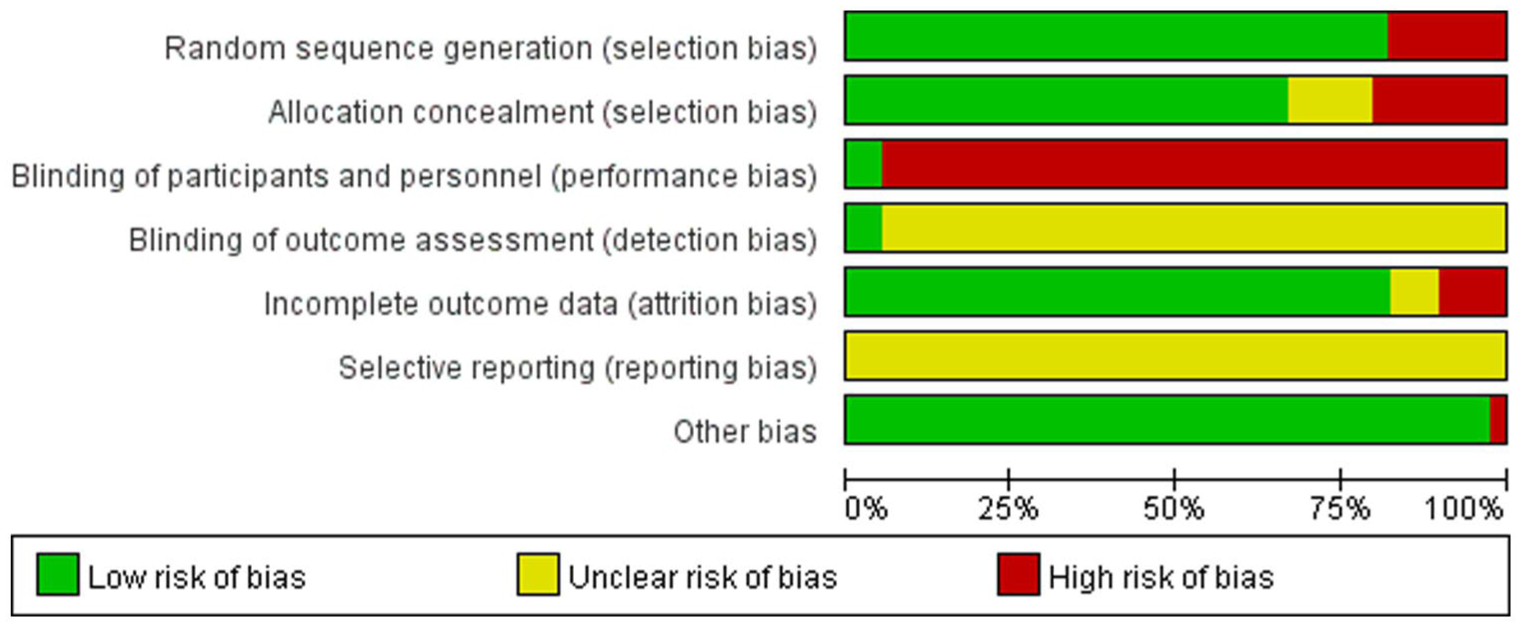
Risk of bias graph of the included studies.

Risk of bias summary of the included studies.
Outcomes
Primary Outcomes: Quality of Life (QoL) Assessment
Treatment combining acupuncture or moxibustion with standard care showed a statistically significant improvement compared to standard care alone, as did standalone acupuncture or moxibustion treatment. The Quality of Life (QoL) assessment was conducted using the QLQ-C30 and KPS scores. The number of studies included in the QLQ-C30 analysis varied by subdomain, with 6 to 8 studies for the functional domains and 2 to 3 studies for the symptom domains. For the KPS score, 2 types of data were analyzed: continuous variable and efficacy rates. Seven studies were included in the continuous variable analysis, while 2 studies were included for efficacy rate analysis.
Functional Assessment Using QLQ-C30
Statistically significant improvements were observed across all 5 functional assessment categories.
For Physical Functioning, 7 studies32 -34,38,39,41,47 were included. The initial analysis showed (MD = 11.50; 95% CI: [10.48, 12.51]; P = .004; I2 = 59%, n = 593), indicating high heterogeneity and a wide confidence interval. Sensitivity analysis identified one study 37 contributing to heterogeneity, and its exclusion reduced I2 to 20%, yielding more stable results (MD = 11.73; 95% CI: [10.51, 12.95]; P < .00001, n = 533).
In the Role Functioning category, 6 studies32,33,37 -39,41 were included, yielding (MD = 9.86; 95% CI: [5.07, 14.65]; P < .00001, I2 = 95%, n = 448).
For Emotional Functioning, 8 studies32 -34,37 -39,41,47 were included, with results showing (MD = 8.47; 95% CI: [5.87, 11.07]; P < .00001, I2 = 80%, n = 593).
For Cognitive Functioning, 5 studies32,33,37,39,41 were included, with results showing (MD = 7.26; 95% CI: [4.84, 9.69]; P < .00001, I2 = 67%, n = 330). The initial analysis showed (MD = 4.71; 95% CI: [1.48, 7.95]; P = .004; I2 = 87%, n = 528), but after excluding 2 studies34,38 identified as potential sources of heterogeneity, I2 was reduced to 67%, though heterogeneity remained moderate.
For Social Functioning, 6 studies32,33,37,39,41 were included, yielding (MD = 7.89; 95% CI: [4.14, 11.65]; P < .00001, I2 = 83%, n = 448).
Although sensitivity analyses were conducted across all categories to explore sources of heterogeneity, only the Physical Functioning domain showed a notable reduction in I2. Heterogeneity in the other domains remained high or only marginally improved, limiting the impact of such adjustments (Figure 4).

Forest plot of QLQ-C30 functional domains.
Similarly, the Global Health Status demonstrated a statistically significant improvement. The initial analysis showed (MD = 8.99; 95% CI: [4.58, 13.41]; P < .00001, I2 = 93%, n = 753), with substantial high heterogeneity and wide confidence intervals. To address this, one study 44 which reported a negative MD value likely due to an alternative interpretation of the global health status, was excluded. After this adjustment, a total of 7 studies32,33,37 -39,41,47 were analyzed, yielding (MD = 12.39; 95% CI: [8.49, 16.29]; P < .00001, I2 = 87%, n = 523). Although this led to a modest reduction in heterogeneity, the I2 value remained high, suggesting that variability among studies persisted despite adjustments (Figure 5).
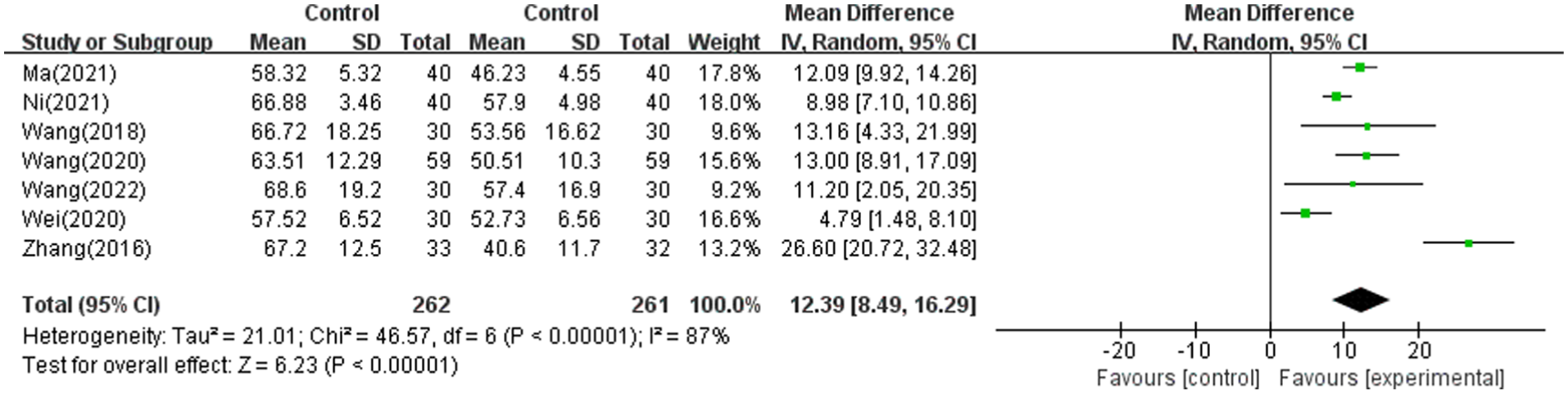
Forest plot of QLQ-C30 global health status.
Supplementary funnel plots for the QLQ-C30 functional domains and global health status are provided in the Supplemental materials (Supplemental Figure 1A and 1B).
Symptom Assessment Using QLQ-C30
In the symptom assessment, statistically significant improvements were observed in 6 of the 9 symptom domains, including fatigue, pain, nausea/vomiting, insomnia, appetite loss, and constipation. In contrast, dyspnea, diarrhea, and financial difficulties showed no significant differences between groups with P-values greater than .05 in all cases.
For dyspnea, an exploratory fixed-effect model was applied despite moderate heterogeneity, which yielded a statistically significant difference; however, this finding was not consistent with the random-effects model and should therefore be interpreted with caution.
The detailed results for all symptom domains are presented in Table 2, and the corresponding forest and funnel plots are provided in the Supplemental materials (Supplemental Figures 1C and 2).
Summary of QLQ-C30 Symptom Domain Outcomes.

KPS (Karnofsky Performance Status)
To evaluate the effectiveness of acupuncture or moxibustion treatments, 7 studies16,22,28,31,43,49,53 were included in the analysis of KPS score as a continuous variable. These studies showed a statistically significant improvement in KPS compared with standard care alone, yielding (MD = 8.22; 95% CI: [7.07, 9.37]; P < .00001, I2 = 0%, n = 608) (Figure 6).

Forest plot of KPS scores.
For studies where the KPS score was described as a binary variable, 2 studies19,29 were included. A significantly higher clinical improvement rate (CR + PR) was observed in the acupuncture or moxibustion group compared with the control group, with the pooled effect of (MD = 1.36; 95% CI: [1.12, 1.64]; P = .002, I2 = 0%, n = 169; Figure 7).

Forest plot of KPS efficacy rate.
Funnel plots for both continuous and binary KPS outcomes demonstrated symmetrical distributions, suggesting no evidence of publication bias. The corresponding funnel plots are provided in the Supplemental materials (Supplemental Figure 3A and 3B).
Secondary Outcomes ; Nausea and Vomiting Assessment
Incidence of CINV
After excluding duplicates, 18 studies were included in a meta-analysis assessing the incidence of nausea, vomiting, and combined nausea and vomiting Specifically, for the incidence of nausea, 8 studies20,24,27,29,30,50,54 showed a RR of 0.30 (95% CI: [0.21, 0.44]; P < .00001, I2 = 0%, n = 720), for vomiting, 8 studies20,24,27,30,50,56 showed a RR of 0.30 (95% CI: [0.20, 0.46]; P < .00001, I2 = 37%, n = 800), and for the combined incidence of nausea and vomiting, 10 studies19,23,25,35,37,40,43 -45,53 showed a RR of 0.34 (95% CI: [0.23, 0.52]; P < .00001, I2 = 0%, n = 817). The overall result showed a RR of 0.32 (95% CI: [0.25, 0.40]; P < .00001, I2 = 0%, n = 2337), indicating a significant reduction in the incidence of nausea and vomiting in the acupuncture or moxibustion treatment group compared to the standard care group (Figure 8).

Forest plot of CINV incidence.
The corresponding funnel plots for CINV incidence are provided in the Supplemental materials (Supplemental Figure 4A).
Efficacy Rate of CINV
A meta-analysis of 5 studies18,21,26,29,51 evaluating the response rate of nausea and vomiting showed a statistically significant improvement in the experimental group. The RR was 1.16 (95% CI: 1.08, 1.25; P < .00001, I2 = 0%, n = 618), suggesting that acupuncture or moxibustion treatment significantly improved the efficacy rate for managing nausea and vomiting compared to standard care (Figure 9). The corresponding funnel plots for CINV efficacy rate are provided in the Supplemental materials (Supplemental Figure 4B).

Forest plot of CINV efficacy rate.
Tertiary Outcomes; Immune Response Assessment
T Lymphocyte
The meta-analysis of studies assessing CD3, CD4, CD8 counts, and CD4/CD8 ratio revealed a significant improvement in T lymphocyte counts in the experimental group compared to the control group. 7 studies27,36,42,48,50,52,55 reported a MD of 7.20 for CD3 counts (95% CI: [3.40, 11.00]; P = .0002, I2 = 95%, n = 719), and 7 studies27,36,42,48,50,52,55 reported a MD of 4.89 for CD4 counts (95% CI: [2.27, 7.51]; P = .0003, I2 = 91%, n = 719).
In contrast, 5 studies36,37,48,50,52,55 on CD8 counts showed no statistically significant improvement (MD = –1.00; 95% CI: [−3.09, 1.08]; P = .35, I2 = 82%, n = 487). However, 3 studies36,48,55 on the CD4/CD8 ratio showed a MD of 0.22 (95% CI: [0.05, 0.39]; P < .00001, I2 = 0%, n = 312). Although CD8 counts did not improve significantly, CD3, CD4 counts, and the CD4/CD8 ratio showed marked improvements, suggesting potential benefits of acupuncture or moxibustion for enhancing immune function in lung cancer patients (Figures 10 and 11). Funnel plots for all T-lymphocyte outcomes (CD3, CD4, CD8, and CD4/CD8 ratio) are provided in the Supplemental materials (Supplemental Figure 5A and 5B).

Forest plot of CD3, CD4, CD8 counts.

Forest plot of CD4/CD8 ratio.
TNF-α (ng/L)
Three studies36,40,46 assessing TNF-α (ng/L) showed a significant reduction in TNF-α levels in patients receiving acupuncture or moxibustion, with a MD of −11.05 (95% CI: [−13.44, −8.66]; P = .04, I2 = 0%, n = 312). This suggest that acupuncture or moxibustion may help modulate immune and inflammatory responses in lung cancer patients (Figure 12). Funnel plots for the TNF-α analysis showed symmetrical distributions with no apparent publication bias and are provided in the Supplemental materials (Supplemental Figure 6).

Forest plot of TNF-α levels.
Discussion
This systematic review and meta-analysis evaluated 39 RCTs involving 3610 patients with NSCLC. This study evaluated the effectiveness of acupuncture and moxibustion in alleviating chemotherapy-induced adverse effects, including nausea, vomiting, and immunosuppression, and in improving QoL. Additionally, the risk of bias in the included studies was assessed using the RoB tool.
The original PROSPERO registration primarily aimed to evaluate the effects of traditional Korean medicine interventions on tumor response (RECIST) and survival outcomes in NSCLC patients receiving standard cancer treatments. However, during the systematic search and screening process, we found that randomized trials involving acupuncture and moxibustion rarely reported tumor response or survival endpoints. Instead, most available evidence focused on patient-centered outcomes such as quality of life, chemotherapy-induced nausea and vomiting, and immune function. Therefore, we conducted a meta-analysis focusing on these outcomes as a sub-analysis within the overarching PROSPERO protocol framework, which explains the difference between the registered primary outcomes and those reported in the current review.
According to the RoB assessment, 32 studies reported performing randomization. However, 5 of these did not specify the randomization method and were therefore rated as having an “unclear risk,” while 7 studies did not mention the allocation method and were considered to have a “high risk” of bias. Due to the nature of acupuncture and moxibustion interventions, blinding was challenging. Except for 2 studies that utilized sham-TEAS, most were rated as having a “high risk” of performance bias. Furthermore, none of the studies had a pre-registered protocol, resulting in an “unclear risk” of reporting bias.
Acupuncture and moxibustion interventions resulted in statistically significant improvements in QoL, CINV, and immune function in patients with NSCLC. After re-analyzing the data with studies exhibiting high heterogeneity excluded, the effects became more consistent and their magnitude was more clearly demonstrated.
As the primary outcome, quality of life (QoL) showed improvements in most domains of the EORTC QLQ-C30 (functional and symptom scales) and in KPS scores. Notably, KPS demonstrated significant improvements in both continuous and dichotomous analyses, indicating that acupuncture and moxibustion effectively enhance patient QoL regardless of the assessment tool employed. However, given that the QLQ-C30 relies on patient self-reports, the potential for subjective bias cannot be excluded. Further longitudinal studies are warranted to validate the long-term sustainability of these effects.
For the secondary outcome, CINV, significant improvements were observed in both incidence rates and treatment efficacy following acupuncture and moxibustion interventions. This indicates that these interventions can effectively address common gastrointestinal side effects during chemotherapy. The Society for Integrative Oncology (SIO) and the American Cancer Society (ACS) have also acknowledged, through integrative therapy guidelines, that acupuncture may help alleviate chemotherapy-induced nausea and vomiting.
McKeon et al conducted a meta-analysis evaluating the efficacy of acupuncture and acupressure for alleviating acute and delayed chemotherapy-induced nausea and vomiting, analyzing 13 randomized controlled trials (7 on acupuncture and 6 on acupressure). 57 In all included studies, standard antiemetic medications were co-administered. 57 The main findings indicated that acupuncture significantly reduced the frequency of acute vomiting and the need for rescue medication, while acupressure was effective in decreasing the frequency of nausea. 57
In comparison, the present study assessed CINV across a broader range of research conditions, including a more diverse set of clinical scenarios. Clear improvements were observed in both the incidence and effective rate of nausea and vomiting. Notably, acupuncture and moxibustion demonstrated efficacy in improving overall CINV regardless of the timing (acute or delayed) or the concomitant use of antiemetics. These findings suggest a wide range of clinical applicability for acupuncture interventions and further strengthen the evidence supporting their use as complementary therapies for the management of CINV.
As the tertiary outcome, immune responses showed statistically significant increases in CD3, CD4, and the CD4/CD8 ratio, while CD8 levels remained unchanged. These findings are partly consistent with the results reported by Wang et al (2025), who reported increased CD3, CD4, CD4/CD8 ratios and a reduction in CD8 levels across heterogeneous solid tumors. 13 However, the absence of a CD8 reduction in our analysis may reflect NSCLC-specific immune characteristics, particularly the high prevalence of exhausted CD8⁺ T cells in this population. Supporting this interpretation, Sanmamed et al (2021) identified a distinct “burned-out” CD8⁺ T-cell subset (Ebo) in NSCLC using a humanized patient-derived xenograft model, demonstrating that these cells exhibit proliferative hyperactivation, impaired effector function, and an apoptotic trajectory—features that may limit their numerical responsiveness to therapeutic modulation. 58
The lack of change in CD8 levels also suggests that immunoregulation was predominantly mediated by helper T-cell activation rather than cytotoxic T-cell depletion. This pattern indicates that immune homeostasis was preserved without the intervention inducing cytotoxic overactivation or immune imbalance. The observed increase in the CD4/CD8 ratio suggests that acupuncture and moxibustion may enhance helper T cell activity while maintaining cytotoxic T cell balance, thereby promoting immune activation. Clinically, this modulation of immune function is meaningful, as it indicates the potential to restore immune balance without provoking excessive inflammatory responses. Such restoration may be particularly beneficial for immunocompromised cancer patients, potentially contributing to improved immune resilience and overall clinical outcomes.
Levels of the pro-inflammatory cytokine TNF-α significantly decreased following the intervention. As TNF-α is a key mediator of chronic inflammation and plays a critical role in promoting tumor growth, angiogenesis, and metastasis within the tumor microenvironment, this reduction may have important immunological implications. 59 Recent evidence indicates that TNF-α exhibits dual roles within the TME, contributing to tumor immune evasion by driving immunosuppressive pathways—such as regulatory T-cell expansion and stabilization of PD-L1 expression—while exerting antitumor apoptotic effects through TNFR1 under specific acute inflammatory conditions. 60 Given that chronic TNF-α elevation in cancer is predominantly linked to inflammatory and immunosuppressive TME signaling, the observed reduction following acupuncture and moxibustion likely reflects an improvement in TME immune balance, thereby potentially supporting the efficacy of anticancer treatments.
The tumor microenvironment (TME), composed of immune cells, vasculature, and stromal cells, plays a critical role in tumor growth and metastasis. 61 Tumor cells promote inflammation within the TME, activating the NF-κB pathway and enhancing immunosuppressive signaling through increased production of TNF-α and ROS, thereby creating a tumor-favorable environment. 62 The observed reduction in TNF-α levels in this study may indicate an improvement in the TME.
Further mechanistic studies involving key cytokines such as IL-6, IL-10, and IFN-γ are warranted, as IL-10 promotes immunosuppression via Tregs, Bregs, and TAMs,15,63,64 and IL-6 facilitates tumor growth and inhibits adaptive immunity through the JAK/STAT3 pathway.65 -68 Additionally, prospective clinical studies are needed to determine the extent to which TNF-α reduction correlates with long-term outcomes.
Wang et al (2023) conducted a meta-analysis and network analysis of 14 RCTs involving patients with stage III/IV NSCLC, evaluating the treatment efficacy (ORR), KPS scores, and safety of acupuncture, moxibustion, and their combination with chemotherapy. 69 The study differentiated between manual acupuncture, auricular acupuncture, fire needling, and moxibustion, and compared both their standalone and combined effects with chemotherapy. 69 According to the SUCRA ranking, the combination of acupuncture and chemotherapy demonstrated the highest treatment efficacy and the most significant improvement in KPS scores, followed by fire needling plus chemotherapy, and moxibustion plus chemotherapy. 69
Taken together with the findings of the present study, these results suggest that combining chemotherapy with acupuncture or moxibustion may effectively enhance treatment outcomes, improve QoL, and alleviate adverse effects in NSCLC patients. In particular, the combination of acupuncture and chemotherapy appears to offer the most favorable therapeutic benefits, supporting its potential as a complementary approach in clinical practice.
This study demonstrates that acupuncture and moxibustion effectively alleviate symptoms, enhance quality of life, and support immune balance in NSCLC patients, underscoring their potential as integrative therapies in clinical practice. They may serve as valuable options for post-chemotherapy or postoperative care, contributing to the holistic management of NSCLC.
Limitation
This study comprehensively analyzed the effects of acupuncture and moxibustion on quality of life and immune function in NSCLC patients; however, several limitations should be noted.
First, blinding was not feasible in most included studies, and control groups were often not placebo-controlled, introducing potential observer and participant bias, particularly in subjective outcomes such as QoL and KPS.
Second, few studies provided detailed intervention protocols in accordance with the STRICTA guidelines, which are designed to ensure the reproducibility and reliability of acupuncture research. 70 As a result, standardization and comparison of treatment components—such as acupoints, techniques, stimulation intensity, and practitioner expertise—were limited, potentially affecting the generalizability of the findings.
Third, considerable heterogeneity existed among the included studies, partly due to the use of various modality-specific forms of acupuncture and moxibustion. Although these techniques differ in their procedural details, they are all regarded as subtypes of the same core therapeutic approaches in routine clinical practice, and the additional supportive measures reflect real-world treatment conditions. To address this variability, we applied predefined sensitivity analyses as well as appropriate fixed- or random-effects models, as described in the Methods. Nevertheless, residual heterogeneity may limit the consistency of the pooled estimates and should be interpreted with caution.
Fourth, most studies assessed only short-term effects, leaving the long-term sustainability of acupuncture and moxibustion, as well as their impact on recurrence and survival, unconfirmed.
Lastly, limited and heterogeneous data on certain immune markers (eg, CD8, NK cells, cytokines) restricted detailed interpretation of the immunomodulatory mechanisms.
Future research should adopt rigorous randomization and blinding, standardized reporting of interventions, long-term follow-up, and integration of biological mechanism studies to strengthen the reliability and clinical applicability of acupuncture and moxibustion in NSCLC care.
Conclusion
This systematic review and meta-analysis suggests that acupuncture and moxibustion may effectively improve quality of life (QoL), alleviate chemotherapy-induced nausea and vomiting (CINV), and enhance immune function in patients with NSCLC. Although heterogeneity was observed due to insufficient standardization of treatment protocols and the short-term nature of immune assessments, the overall findings indicate meaningful complementary benefits of these interventions. Future trials with standardized methodologies and long-term immunological and clinical evaluations are warranted to better establish their therapeutic value in integrative NSCLC care.
Supplemental Material
sj-docx-1-ict-10.1177_15347354261419716 – Supplemental material for Effectiveness of Acupuncture and Moxibustion for Non–Small Cell Lung Cancer (NSCLC) Patients Undergoing Standard Treatment: A Systematic Review and Meta-Analysis
Supplemental material, sj-docx-1-ict-10.1177_15347354261419716 for Effectiveness of Acupuncture and Moxibustion for Non–Small Cell Lung Cancer (NSCLC) Patients Undergoing Standard Treatment: A Systematic Review and Meta-Analysis by Dong-Hyeon Kim, Mi-Sun Park, Keon-Jun Lee, Jong-Ha Kwon, Ye-Jin Jin and So-Jung Park in Integrative Cancer Therapies
Footnotes
Acknowledgements
The authors thank all researchers and supporters involved in this study.
Ethical Considerations
No ethical approval was required as this study did not involve human participants or laboratory animals.
Author Contributions
DHK and MSP contributed to the study conception and design and drafted and wrote the manuscript. MSP, JHK, KJL and YJJ performed data collection, data extraction, and quality assessment. DHK and SJP contributed to the methodology and to the manuscript’s review and critical revision. SJP supervised the project, managed project administration, and acquired funding. All authors reviewed and approved the final version of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by a grant of the Korea Health Technology R&D Project through the Korea Health Industry Development Institute (KHIDI), funded by the Ministry of Health & Welfare, Republic of Korea (grant number:
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data and materials included in this study are included in this published article and supplementary material.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.