
Abstract
Research on the relationship between integrative oncology (IO) programs and dispensing of chemotherapy agents and supportive care drugs, and hospitalization rates is limited. The present study examined these outcomes in chemotherapy-treated patients with cancer, comparing patients highly adherent to integrative care (high-AIC) to those with low adherence (low-AIC). Data from patients with cancer treated with taxane and/or platinum-based agents participating in an ongoing prospective, controlled pragmatic trial were examined retrospectively. Patients were referred to an IO consultation and weekly treatments at 3 medical centers in Northern Israel, with high-AIC defined as attending ≥4 sessions at 6 weeks; low-AIC, 0-3 sessions. Cancer-related parameters; dispensing of medication (chemotherapy agents, analgesics, anxiolytics and opioids); rates of hospitalizations and emergency room visits were analyzed using generalized linear regression models. Of 615 patients attending the IO consultation, 367 (59.7%) were high-AIC, with both groups having mostly similar baseline characteristics. Dispensing rates for taxanes (P = .336), platinum agents (P = .403), non-opioid analgesics (P = .201), and anxiolytics (P = .350), and number of emergency room visits were similar in both groups at 12 weeks. However, high-AIC patients had fewer dispensed opioid prescriptions (RR = 0.50, 95% CI = 0.30-0.85, P = .010); lower rates of hospitalization (OR = 0.59, 95% CI = 0.39-0.88, P = .010); and fewer hospitalization days (RR = 0.53, 95% CI = 0.31-0.90, P = .019). In conclusion, dispensing of chemotherapy drugs was similar between groups, though high-AIC patients used less opioids and had fewer hospitalizations at 12 weeks. Further research is needed with randomized and prospective studies exploring the relationship between adherence to IO care; adherence to chemotherapy; quality of life; opioid use; and hospitalization.
Introduction
Cancer centers across the globe are increasing providing their patients with evidence-based integrative oncology (IO) care to address health-related quality of life (HRQoL)-related concerns unmet by supportive and palliative cancer care. 1 Clinical practice guidelines published jointly by the American Society of Clinical Oncology (ASCO) and Society for Integrative Oncology (SIO) recommend IO treatments for cancer-related pain, 2 anxiety and depression, 3 and cancer-related fatigue. 4 Implementation of these guidelines in real-life clinical practice remains limited on both national and professional levels, 5 requiring resources and research examining the impact of IO on healthcare utilization. 6
Studies employing a pragmatic methodology examining patient-tailored IO consultations and treatment programs are showing a significantly beneficial effect on both subjective patient-reported HRQoL and objectively-measured oncology treatment-related outcomes. 7 Further studies are still needed to examine the utilization of IO consultations and treatments; their impact on use of conventional medications and rates of hospitalizations, with the research to date inconclusive. 8 Still, most of this research has found IO services associated with reduced costs from medication use. 9
The findings of research examining economic aspects of IO programs remain unclear. In a study by Thronicke et al using the Network Oncology Clinical Registry in Germany, injections with the herb mistletoe (Viscum album) during chemotherapy were both beneficial and relatively cost-effective in patients with stage IV non-small cell lung cancer. 10 In a study by Shalom-Sharabi et al from Israel, chemotherapy-treated patients with breast and gynecological cancers who adhered to an IO program used significantly fewer non-opioid analgesic drugs. 11 In the U.S., Ng et al found that breast cancer survivors receiving acupuncture for pain reported using fewer analgesic (opioid and NSAID) drugs, and incurred lower healthcare costs. 12 However, studies from Canada and China comparing group versus individual acupuncture for cancer-related pain, or acupuncture versus usual care for chemotherapy-induced peripheral neuropathy, found no significant differences in quality-adjusted life years (QALYs) between groups.13,14 In China, Cao et al reported that IO rehabilitation promotes postoperative gastrointestinal function recovery in patients undergoing laparoscopic surgery for colorectal cancer, with no significant decrease in hospitalization costs. 15 Still, while acupuncture and other traditional medicine modalities are prevalent in cancer care in China, and considered to be cost-effective, 16 the research on their true economic impact is limited.
The present study explored a real-life setting of IO care, which characterizes many of the IO programs currently operating within 11 oncology centers in Israel. These programs include IO consultations and treatments which are provided within conventional oncology or hemato-oncology departments, though not covered by the National Health Insurance Institute in Israel. 17 The present study purposed to identify an association between adherence to the program and use of chemotherapy agents, analgesic (opioid and non-opioid) and anxiolytic drugs; rates of hospitalization and emergency room visits; and number of consultations in primary care and oncology clinics in patients undergoing taxane and/or platinum-based chemotherapy.
Methods
Study Design, Population, and Setting
Chemotherapy-treated patients with cancer were recruited to a prospective, controlled pragmatic trial, and referred to the study IO program by their oncology provider from July 2009 to December 2021 to 1 of 3 participating oncology medical centers (Carmel, Lin, and Zebulon) operated by Clalit Health Services (CHS) in northern Israel CHS. The centers are part of the Integrative Oncology Program which provides chemotherapy-treated patients with evidence-based IO modalities addressing HRQoL-related concerns. 18 Records of patients were examined. Study data were derived from electronic medical records (EMRs) and CHS claims data (ie, administrative information collected during healthcare, available for research and public health analysis) of the oncology patients participating in the prospective pragmatic trial, and which was analyzed retrospectively. Inclusion criteria for study participation included age ≥21 years; referral to the IO consultation by the patient’s oncology healthcare providers (oncologists, oncology nurses, or psycho-oncologists); undergoing adjuvant, neo-adjuvant, or palliative chemotherapy with taxane- and/or platinum-based agents for solid tumors; and presenting within 12 weeks from the index date (the date of the initial IO consultation). Patients who were not referred to the IO consultation, or were referred but did not attend the consultation; were not undergoing treatment with by taxane- and/or platinum-based agents; or did not fulfill the other criteria were excluded from the study.
IO Consultation and Treatments
Patients are referred to the IO Program by oncology healthcare providers (eg, oncologists, oncology nurses, psycho-oncologists), specifying at least 1 leading HRQoL-related concern. Referral to the IO program and IO consultations are available as part of the study centers’ supportive cancer care, without cost. Patients are asked to provide informed consent to allow for researching the effects of the IO consultations and treatments on HRQoL-related concerns. A consultation with an IO-trained physician (integrative physician, IP) addresses patient expectations and health beliefs, including affinity and experience with traditional and complementary medicine; and identifies leading HRQoL-related physical, emotional, and spiritual concerns. The IP and patient then co-define HRQoL-directed treatment goals, co-designing weekly IO treatments (6-12 weeks), provided without charge.
The choice of IO modalities is based on safety-related considerations (eg, risk for bleeding with acupuncture; herb-drug interactions); evidence-based recommendations, such as those in the SIO-ASCO guidelines; and personal preferences of the patient, to increase adherence to the IO treatment regimen. Treatments last approximately 30 minutes, often combining IO modalities such as acupuncture, manual and mind-body therapies. Treatments are provided by a team of 25 healthcare providers (physicians, nurses, paramedical practitioners, and therapists) with extensive IO training and experience. 19
Study Objectives
The primary study outcome was the number of dispensed taxane and/or platinum agent and opioid/non-opioid analgesic drugs during the 6 to 12-week treatment period, comparing high- to low-adherence to integrative care (AIC) groups. High-AIC was defined as attending ≥4 IO treatments during the first 6 weeks of the study; low-AIC as attending 0-3 sessions during this period. Secondary objectives included the number and length of hospitalizations; emergency room visits; dispensed prescriptions for anxiolytic drugs; and visits to outpatient primary and oncology clinics at 6- and 12-weeks.
Study Measures
The date of the initial IP consultation was designated as the date of study entry (index date). Adherence (AIC) following the initial IP consultation was derived from the database of a currently ongoing prospective registry protocol study, at 6- and 12-weeks. Data for dependent variables derived from CHS claims data (at 6 and 12 weeks from index date) included the number of dispensed prescriptions for taxane- and/or platinum-based agents, according Anatomical Therapeutic Chemical (ATC) classification system 20 for taxane (L01CD) and platinum-based agents (L01XA); anxiolytics (N05B, N05C); anti-inflammatory and anti-rheumatics, including non-steroidal anti-inflammatory drugs (M01A), opioids (N02A and N01AH, excluding N02AJ); and non-opioid analgesics (salicylic acid and derivatives, N02BA; paracetamol/acetaminophen, N02BE01 & N02BE51; and pyrazolones, N02BB). The number and duration of hospitalizations included departments of oncology, general surgery, gynecology, urology, and internal medicine. Emergency room visits (without hospitalization), primary care and outpatient oncology visits were examined as well.
Independent variables included demographics (age, sex, primary language); supplementary health insurance coverage; and socioeconomic status, based on area of residence. 21 Other variables included clinical cancer-related parameters (primary tumor site; treatment setting (adjuvant/neo-adjuvant/palliative end-of-life care); tumor stage (TNM classification); co-morbidities, based on the Charlson comorbidity index (CCI), including chronic disease such as diabetes mellitus, renal, liver, pulmonary and cardiovascular disease.
Statistical Analysis
Data were stored and managed using Microsoft Excel 2016 and Microsoft Access 2016 (Microsoft Corporation), and analyzed using RStudio software (version 2022.07.1; RStudio, PBC, Boston, MA). Continuous variables were presented using mean ± standard deviation, median, and interquartile range (IQR), with categorical variables presented as proportions. Between-group comparisons of continuous and categorical variables were conducted using the Mann-Whitney U test and a chi-squared test, respectively.
A multivariable generalized linear model (GLM) assuming log link function and negative binomial distribution was used to analyze the number of dispensed opioid drugs and hospitalization days. We have specified 2 types of GLMs: The first, for count data (ie, the number of dispensed opioid drugs and hospitalization days), using a rate ratio (RR) for this purpose. The second, for dichotomous variables (ie, hospitalized, yes/no), using an odds ratio (OR). A logistic regression model was used to analyze the likelihood of being hospitalized. Core independent variable in all models was high- versus low-AIC. All models were adjusted for potential confounders, including age, sex, supplementary health insurance, socioeconomic status, clinical oncology parameters, and comorbidity burden. P-values of <.050 were used to determine statistical significance in all analyses.
Ethical Considerations
The protocol of this retrospective study was based on a secondary analysis of an anonymous dataset, approved by the Ethics Review Board (Helsinki Committee) at the Carmel Medical Center in Haifa, Israel (CMC-17-0091). This is part of an ongoing prospective study of the Integrative Oncology Program registry protocol, approved by the Ethics Review Board at the Carmel Medical Center in Haifa, Israel (CMC-09-0024). Patients were recruited to the prospective study after signing an informed consent form during the IP consultation. Both referral and IO treatments were available as part of routine supportive cancer care, and without cost to the patient.
Results
Characteristics of Study Groups
Of 615 patients eligible for study inclusion, 367 (59.7%) were high-AIC and 248 (40.3%) low-AIC (Table 1) . The 2 groups shared mostly similar demographic and cancer-related characteristics and co-morbidities, with the exception of a lower prevalence of chronic pulmonary disease in the high-AIC group (P = .001); significantly more Hebrew language speakers (P < .001); and a trend for higher socioeconomic status and supplementary health insurance, both with borderline significance (P = .054; P = .064, respectively).
Comparison of Patient Characteristics According to Adherence to Integrative Care (AIC) in an IO Program.
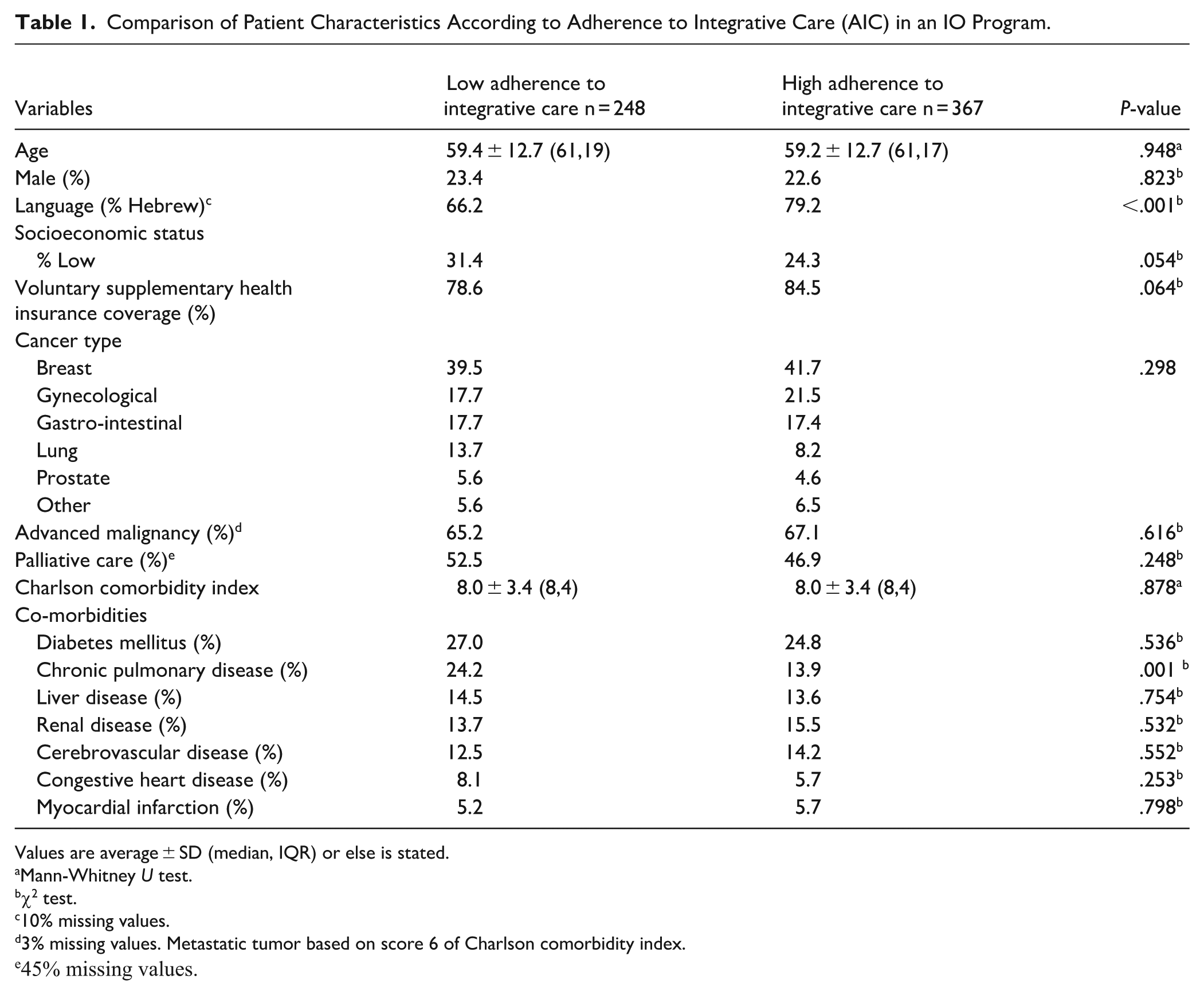
Values are average ± SD (median, IQR) or else is stated.
Mann-Whitney U test.
χ2 test.
10% missing values.
3% missing values. Metastatic tumor based on score 6 of Charlson comorbidity index.
45% missing values.
Dispensed Prescriptions
Rates of dispensed taxane and platinum agents were similar in the 2 groups (Table 2 : taxanes, P = .336; platinum, P = .403), as was the percentage of patients using these agents (taxanes, P = .982; platinum, P = .642) at 12 weeks. Similar results were noted at 6 weeks for rates of dispensed taxane and platinum agents (taxanes, P = .635; platinum, P = .245), and for the percentage of patients using these agents (taxanes, P = .674; platinum, P = .983). The number of opioid prescriptions dispensed was significantly lower in the high-AIC group at 12 weeks, for both total number of prescriptions (0.64 ± 2.18 vs 1.33 ± 3.55, P = .014) and percentage of patients using these medications (16.3% vs 23.4%, P = .030). Table 3 presents a multivariable model, with high-AIC patients showing significantly lower numbers of dispensed opiate prescriptions at 12 weeks (RR = 0.50, CI = 0.30-0.85, P = .010), with a similar finding at 6 weeks, and a trend with borderline significance for dispensing of opioid prescriptions (0.45 ± 1.46 vs 0.86 ± 2.19, P = .065) and percentage of patients using these drugs (16.7% vs 22.8%, P = .095) (figures for 6-week time point are not shown).
Between-Group Comparison of Healthcare Utilization During the 12 Weeks.
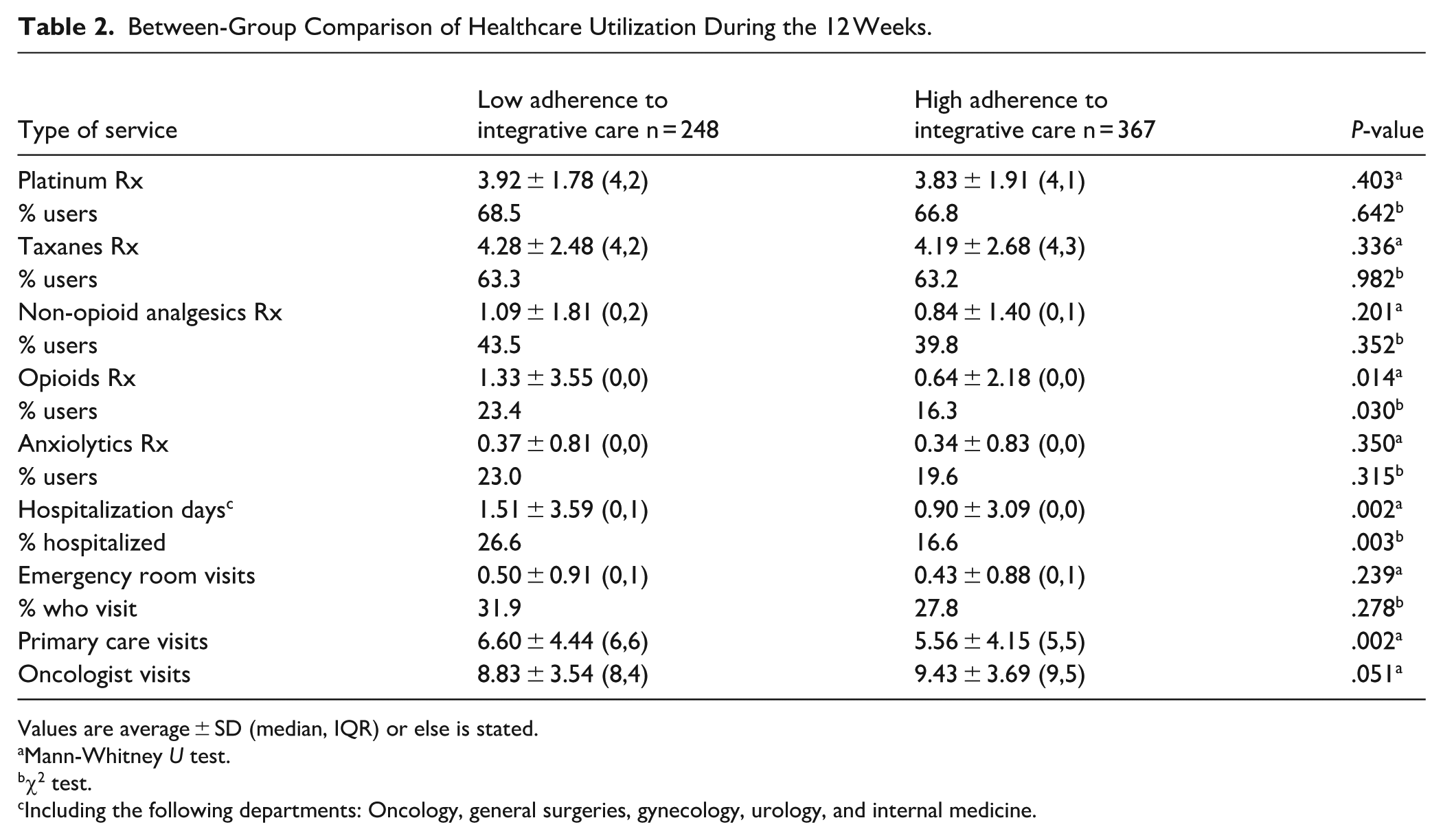
Values are average ± SD (median, IQR) or else is stated.
Mann-Whitney U test.
χ2 test.
Including the following departments: Oncology, general surgeries, gynecology, urology, and internal medicine.
Multivariable Model of Determinants for the Number of Dispensed Opioid Prescriptions at 12 Weeks (n = 615).

Abbreviation: AIC, adherence to integrative care.
No between-group differences were found for the number of non-opioid analgesics dispensed (P = .227, P = .201) or percentage of patients using these drugs (P = .213, P = .352) at both 6 and 12 weeks, respectively. Use of anxiolytics was also similar in both groups regarding number of prescriptions dispensed (6 weeks, P = .699; 12 weeks: P = .350) and percentage of patients using these drugs (6 weeks, P = .614; at 12 weeks: P = .315).
Hospitalizations and Emergency Room Visits
The percentage of hospitalized patients at 12 weeks was significantly lower in the high-AIC group (16.6% vs 26.6%, P = .003), with a lower number of hospitalization days (0.90 ± 3.09 vs 1.51 ± 3.59, P = .002). Similar results were found in both groups at 6-weeks, with the high-AIC group less likely to be hospitalized (9.6% vs 16.8%, P = .020), and with fewer hospitalization days (0.43 ± 2.10 vs 0.92 ± 2.87, P = .016).
Table 4 presents a multivariable model demonstrating a lower probability for hospitalization at 12 weeks in the high-AIC group (OR = .59, CI = 0.39-0.88, P = .010); additional multivariable analysis showed fewer hospitalization days in this group (RR = .53, 95% CI = 0.31-0.90, P = .019). Patients in the high-AIC group also had fewer emergency room visits at 6 weeks, though with borderline significance (0.26 ± 0.58 visits vs 0.38 ± 0.73, P = .086); with no statistically significant difference found at 12 weeks (P = .239).
Multivariable Model of the Likelihood for Hospitalization (at 12 Weeks, n = 584).

Abbreviation: AIC, adherence to integrative care.
Oncology and Primary Healthcare Visits
The number of oncologist visits was similar in both groups at 6 weeks (P = .209), and greater (though with borderline significance) in the high-AIC group at 12 weeks (9.43 ± 3.69 vs 8.83 ± 3.54, P = .051). In contrast, patients in the low-AIC group had more primary care visits at 6 weeks (P = .001), as well as at 12 weeks of follow-up (6.60 ± 4.44 vs 5.56 ± 4.15, P = .002).
Discussion
This study explored the relationship between adherence to a real-life IO program and health care utilization, measured by the number of dispensed prescriptions for taxane and/or platinum-based chemotherapy agents, as well as analgesic (opioid and non-opioid) and anxiolytic drugs; rates of hospitalization and emergency room visits; and number of consultations in primary care and oncology clinics. Patients highly adherent to weekly IO treatments (high-AIC group) had a similar number of dispensed taxane/platinum prescriptions as those with low adherence (low-AIC group), at both 6 and 12 weeks. However, patients in the high-AIC group had a lower number of dispensed opioid drugs at 12 weeks, and lower rates of hospitalizations at both 6 and 12 weeks.
Comparing patients with high versus low-AIC has been shown to reflect the impact of IO on patient care, which has been shown to be most significant when a continuum of care is ensured for between 6 and 12 weeks.22,23 Studies employing a pragmatic methodology have shown a significantly greater effect of IO interventions among high-AIC (vs low-AIC) chemotherapy-treated patients, as assessed using patient-reported outcomes (eg, pain, 24 insomnia, 25 anxiety/depression 26 ). Adherence to the IO program has also been associated with increased adherence to the patient’s chemotherapy regimen. In a pragmatic study of chemotherapy-treated female patients with breast and gynecological cancers, the relative dose intensity (RDI) calculation was significantly closer to 1.0 in high-AIC patients for paclitaxel and carboplatin at 6 weeks, though this was not the case with chemotherapy agents such as cyclophosphamide and doxorubicin. 27 In a second study of that cohort, high-AIC patients reported lower severity scores for fatigue, despite a greater reduction in hemoglobin levels, most likely due to greater adherence to the chemotherapy protocol (ie, RDI closer to 1.0). 28 Finally, in a study of patients with advanced gynecological cancer, high-AIC at 6 weeks was associated with better adherence to taxane-based regimens, though not for platinum-based agents. 29 The present study did not find a correlation between adherence to integrative care and dispensing of taxane/platinum-based agents, or the percentage of patients using these drugs. This may be due to the retrospective search for dispensed prescriptions as a measure of adherence. A more accurate method is the RDI calculation, which prospectively measures drug dosage and time intervals between chemotherapy cycles.
The present study found lower rates of dispensing opioid drug prescriptions in the high-AIC group, which may reflect a reduction in pain severity in the cohort of patients with metastatic cancer. The SIO-ASCO guideline for treating cancer-related pain recommends modalities such as acupuncture for general or musculoskeletal pain (recommendation 1.3); reflexology or acupressure for pain during systemic therapy for cancer treatment (recommendation 1.4); and massage for pain in patients undergoing palliative care (recommendation 1.13). 2 Real-world pragmatic research has indicated that high-AIC may be associated with greater pain relief at 6 weeks in patients undergoing chemotherapy and/or palliative care. 22
Earlier research on economic aspects of IO programs in supportive and palliative care services has shown reduced costs related to medication use.8,9 However, only a small number of studies have examined economic implications of adherence to IO interventions, finding no correlation with use of non-opioid and opioid analgesics and anxiolytics.11,12 In the present study, the lower opioid use observed is likely to result in lower medication costs. A number of methodological differences between the present and former studies may explain this discrepancy, such as different periods of follow-up; use of different IO modalities; and characteristics of patient populations being studied. In the present study, 60% of patients had a diagnosis of breast or gynecological cancer, in contrast to earlier studies where the cohorts were more diverse. Still, a correlation between adherence to integrative care and reduced costs has been observed in an earlier study in which patients with advanced non-small cell lung cancer or mesothelioma suffering from dyspnea who were treated with acupuncture, resulting in reduced doses of opioids. 30 A similar effect was observed with electro-acupuncture, which was associated with a reduced need for opioid drugs during the early postoperative period in patients scheduled for gynecologic abdominal surgery. 31
The lower rates of hospitalization and number of hospitalizations observed in the high-AIC group may reflect a correlational (rather than causal) relationship. It is possible that high-AIC (vs low-AIC) led to greater improvement in HRQoL-related concerns, and thus a lesser likelihood for hospitalization. At the same time, it is also possible that higher rates of hospitalization led to reduced attendance at IO sessions, though most patients in the low-AIC group were hospitalized for less than 6 days. In any case, both groups of patients had similar rates of dispensing both taxane and platinum-based agents; and the greater improvement in HRQoL-related concerns observed in the high-AIC group supports a causal role of the IO intervention in lowering rates of hospitalization and emergency room visits, as shown in prior pragmatic research of this setting.32,33
Further research needs to expand its understanding of this relationship. Most studies published to date have compared IO programs to standard care for rates of hospitalization, without examining adherence to integrative care as an influencing factor. In addition, the research has been examining specific IO modalities, and not the program as a whole; and addressing varying characteristics (eg, patient demographics, co-morbidities, etc.) and periods of follow-up. These and other factors may explain the differences between the findings of the present study with those of earlier research.8,10,12 An example of this is a study which examined the impact of acupuncture on survivors of breast cancer, finding no relationship between AIC and rates of hospitalization at 12 months. 12
The present study has several methodological limitations. Although patients were recruited prospectively to the ongoing pragmatic trial, data analysis was performed retrospectively. In addition, the number of dispensed prescriptions of chemotherapy agents, analgesics (opioid and non-opioid) and anxiolytics may not correlate directly with actual administration of these drugs. This can be assessed far more accurately using RDI calculations, which include chemotherapy drug doses and intervals between cycles. Finally, only files of patients referred to the IO program by their oncology healthcare providers were included, and not of patients not referred to or not attending the initial IP consultation and subsequent treatments. In a previous study with a cohort of nearly 5000 oncology patients in northern Israel, significant disparities in accessing IO services were identified, leading to lower rates of referral to and attendance of consultations and treatments. 34
In addition to the above, the present study defines adherence to IO care according to attendance during the first 6 weeks, and not from weeks 6 to 12. It is therefore possible that patients with low-AIC during the first 6 weeks of treatment may have had higher adherence between 6 and 12 weeks, or vice versa. While acknowledging this limitation, this definition of AIC is more reflective of real-life IO care, which is most challenging during the first 6 weeks. Another study limitation is the focus on the number of IO interventions, as opposed to the various IO modalities provided (eg, massage vs acupuncture, or yoga vs reflexology, etc.). Future studies need to expand the definition of adherence, to include the entire 12-week period of the intervention; the “total dose” of IO interventions provided; and the use of specific IO modalities.
In addition to the above, a number of barriers to accessing IO care have been identified, include ethno-national factors (ie, primary language), gender and age, all relevant to the present study. While patients in both high- and low-AIC had similar demographic, co-morbidity and cancer-related parameters, the high-AIC group had a larger percentage of primarily Hebrew speakers and higher socioeconomic status. Finally, the study took place in an IO program in northern Israel, which precludes reaching any conclusions regarding the generalizability of the findings for similar programs in other parts of Israel or other countries. Nevertheless, and despite these limitations, this study presents a unique perspective in that it explores the relationship between adherence to integrative oncology care, chemotherapy and analgesic (opioid and non-opioid) drug and healthcare utilization in a real-life IO clinical setting, which is increasingly becoming part of conventional supportive and palliative cancer care.
In conclusion, the present retrospective study found that while both patients with high and low adherence to integrative care had a similar number of dispensed taxane/platinum prescriptions, the high-AIC group required fewer opioid prescriptions and had fewer hospitalizations at 12 weeks. These findings need to be confirmed in large, prospective and multi-centered studies in order to better understand the association between adherence to integrative care, within the context of an IO program addressing HRQoL-related concerns, and the use of opioid analgesics and rates of hospitalization.
Footnotes
Ethical Considerations
The protocol of this retrospective study was based on a secondary analysis of an anonymous dataset, approved by the Ethics Review Board (Helsinki Committee) at the Carmel Medical Center in Haifa, Israel (CMC-17-0091). This is part of an ongoing prospective study of the Integrative Oncology Program registry protocol, approved by the Ethics Review Board at the Carmel Medical Center in Haifa, Israel (CMC-09-0024)
Author Contributions
EBA and TST organized and designed the trial and collected the data analyzed in this study. EBA, TST, DG, and NS planned the study. TST carried out the analysis. EBA, TST, AML, and NS wrote a draft manuscript. All authors participated in the revision of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.