
Abstract
Objective. Measure Yourself Concerns and Wellbeing (MYCaW) is a patient-centered questionnaire that allows cancer patients to identify and quantify the severity of their “concerns” and “wellbeing,” as opposed to using a predetermined list. MYCaW administration is brief and aids in prioritizing treatment approaches. Our goal was to assess the convergent validity and responsiveness of MYCaW scores over time, the generalizability of the existing qualitative coding framework in different complementary and integrative oncology settings and content validity. Methods. Baseline and 6-week follow-up data (n = 82) from MYCaW and FACIT-SpEx questionnaires were collected for a service evaluation of the Living Well with the Impact of Cancer course at Penny Brohn Cance Care. MYCaW convergent validity was determined using Spearman’s rank correlation test, and responsiveness indices assessed score changes over time. The existing qualitative coding framework was reviewed using a new data set (n = 158) and coverage of concern categories compared with items of existing outcome measures. Results. Good correlation between MYCaW and FACIT-SpEx score changes were achieved (r = −0.57, P ≥ .01). MYCaW Profile and Concern scores were highly responsive to change: standardized response mean = 1.02 and 1.08; effect size = 1.26 and 1.22. MYCaW change scores showed the anticipated gradient of change according to clinically relevant degrees of change. Categories, including “spirituality,” “weight change,” and “practical concerns” were added to the coding framework to improve generalizability. Conclusions. MYCaW scores were highly responsive to change, allowing personalized patient outcomes to be quantified; the qualitative coding framework appears generalizable across different integrative oncology settings and has broader coverage of patient-identified concerns compared with existing cancer-related patient-reported outcome measures.
Introduction
Developments in complementary and integrative medicine (CIM), particularly in relation to cancer treatment, have led to a steady growth in the number of health care centers that are providing complementary therapy–based supportive care for people with cancer and their supporters/carers. For example, in the United States and Canada, 57 of the most highly esteemed academic medical centers and affiliated centers have integrative medicine clinics. 1
The use of complementary and integrative approaches to cancer treatment and patient care acknowledges the importance of treating the whole person as opposed to just the physical disease. 2 Often, modalities such as massage therapy, counseling, nutrition, acupuncture, or herbal therapy are used to support people through their treatment, recovery, and prevention of recurrence, and to improve their quality of life. This shift in the health paradigm means there is a need to capture all outcome data that is relevant to patients, including psychological, social, and spiritual outcome data in addition to data such as recurrence, survival, and tumor size.3-5 The focus on the individual within the whole person framework also underlines the importance of understanding what concerns are most important for the patient, to inform clinical practice and to accurately and effectively document how a patient benefits from complementary and integrative cancer care. 6 The increased use of patient-reported outcome measures (PROMs) represents a shift toward documenting outcomes from the patients’ perspective versus that of a clinician or researcher. Most PROMs used in cancer research, however, do not list all items deemed important to patients, or use variations in descriptions of items.7,8 Inclusion of PROMs in routine clinical practice therefore requires careful consideration. 9 The BraveNet Collaboration has conducted extensive work to develop PROMs that reflect the patients’ experience of integrative medicine; 10 however, there is no validated PROM specific to complementary and integrative cancer care.
The Measure Yourself Concerns and Wellbeing (MYCaW) PROM was developed in the United Kingdom, is appropriate for use with patients with all types of cancer diagnosis, and can also be used with supporters/carers. 11 It is used by integrative cancer centers and cancer support centers in the United Kingdom, the United States, Canada, and Israel12-16 and takes approximately 2 minutes to complete.
MYCaW allows people to identify and score the severity of up to 2 of their most pressing concerns, at the time of their first consultation. This is in contrast to most other measures, which ask people to score a predetermined list of items. The patient also rates their overall Wellbeing. After a set number of treatments or a set period of time, people independently rescore their initial Concerns and Wellbeing on the follow-up MYCaW form. The difference in scores describes the degree of improvement or deterioration. Open-ended questions on the follow-up form also capture qualitative data on what people feel is most important about the center/service and anything they have done in addition to receiving complementary care which they feel has influenced their health. A key advantage of the MYCaW tool is that it ensures whatever is relevant to the patient is captured in an evaluation, in a way that is not possible with a predetermined list of items. MYCaW can easily be integrated within an existing documentation system and ongoing collection of MYCaW data has been shown to help a center/service provider to audit or evaluate its service and capture the patients’ perspective.13,15,17-19
MYCaW also captures qualitative data and has an accompanying qualitative coding framework, which was validated to allow for standardized analysis of MYCaW data. 20 This is important for developing the evidence base in this area. MYCaW data can be analyzed to identify other variables that are relevant in statistical analysis of quantitative data, which is important in the development of comparative effectiveness research. 21 Discussion on how to report and combine the change scores and qualitative MYCaW data is reported in Seers et al. 17
While extensive effort was previously put into developing a comprehensive coding framework, the framework is only based on UK data and therefore the generalizability of this framework within different CIM settings is unclear. Furthermore, the responsiveness of the MYCaW Concern and Wellbeing scores has not yet been analyzed. It is therefore important to determine the extent to which the MYCaW questionnaire can respond to a patient’s perceived change in severity of their Concerns and Wellbeing.
The aim of this article is to report a preliminary assessment of the responsiveness, generalizability, content, and convergent validity of MYCaW, including (a) an analysis of the responsiveness of MYCaW score changes as compared with a widely used and validated tool, (b) generalizability via an analysis of the use of MYCaW across different CIM health care settings in different countries, and (c) content validity via a literature search to determine any outcomes that are being captured as MYCaW Concerns but are not commonly represented within other Health-Related Quality of Life (HRQL) PROM tools and vice versa.
Methods
Sample
Data were collected as part of a service evaluation of 171 cancer patients and their supporters/carers attending Living Well with the Impact of Cancer courses at Penny Brohn Cancer Care (PBCC), between August 2011 and January 2012. MYCaW was administered before patients started their course and again 6 weeks later. Patients were asked to write down their 2 main Concerns and score these on a scale of 0 (best it could be) to 6 (worst it could be). Patients also rated their Wellbeing using the same scale. MYCaW takes approximately 3 to 5 minutes to complete at baseline and 5 to 7 minutes to complete at follow-up. More details on MYCaW administration can be found in other studies.19,20 These data were used to assess the responsiveness of the change in MYCaW scores and to review the categories of the qualitative coding framework. Ethical approval was gained from the University of Westminster Research Ethics Committee.
Assessment of Responsiveness of MYCaW
MYCaW score changes from eligible participants (n = 82) who had data recorded at baseline and at the 6-week follow-up time point, for both MYCaW and Functional Assessment of Chronic Illness Therapy Questionnaire with an additional spiritual subscale (FACIT-SpEx) 22 were analyzed. FACIT-SpEx is a HRQL PROM specific to cancer patients; it is responsive to change, valid and reliable in clinical and observational settings. 23 A core of 27 questions measure Physical, Social/Family, Emotional and Functional Wellbeing relating to cancer therapy. The Extended Spiritual subscale (SpEx) encompasses a further 23 items which relate to religious and nonreligious aspects of Spiritual Wellbeing. Hence, a total of 50 items assess HRQL. For each item participants can select “Not at all,” “A little bit,” “Somewhat,” “Quite a bit,” or “Very much” and the higher the score, the better the HRQL of the patient.
Validity and responsiveness were measured using a similar approach employed in the validation of the Measure Yourself Medical Outcomes Profile (MYMOP), a sister questionnaire developed for general practice.24,25 To determine convergent validity, MYCaW scores were compared to FACIT-SpEx scores. MYCaW Profile scores and FACIT-SpEx total scores at baseline were analyzed using Spearman’s rank correlation (based on nonparametric distribution of scores at baseline), with the aim of achieving a negative correlation coefficient of r ≥ 0.3 (based on data from Paterson 24 ). MYCaW Profile scores are the calculated mean of the Concerns and Wellbeing scores combined. Profile scores are only calculated for those participants who have provided at least 1 Concern score and a Wellbeing score.
A combination of distribution- and anchor-based methods has been used to determine clinically important change in FACIT scores. 26 Thus FACIT-SpEx was a good candidate to use as an anchor to determine when a clinically relevant change had occurred. The minimal important difference for FACIT-SpEx scores were calculated based on a change of between 0.15 and 0.25 points per item, 26 hence clinically relevant improvement was set at 7.5 to 12.5 points. A substantial clinically relevant change was deemed any score change of 12.6 points or greater. Change could be improvement or deterioration, hence 5 mutually exclusive change categories were developed for the purpose of analysis: substantial improvement (≥+12.6); clinically relevant improvement (+7.5 to +12.5); stable (−7.4 to +7.4); clinically relevant deterioration (−7.5 to −12.5); substantial deterioration (≤ −12.6).
Mean change scores for MYCaW and FACIT-SpEx were calculated by subtracting the baseline score from the 6-week follow-up score. Standardized response mean (SRM) and the effect size (ES) were calculated for MYCaW and FACIT-SpEx data as a whole group.
Participant data were then grouped using the change categories determined by the FACIT-SpEx (described above). Responsiveness indices, including T-statistic, Guyatt’s responsiveness statistic (GRS), SRM, and the ES were then calculated for MYCaW data in each change category. Because of the small number of participants with clinically relevant deterioration (n = 2), meaningful analysis could not be carried out for this category.
Determining Generalizability of the Qualitative Analysis Framework for MYCaW
The existing qualitative coding framework was developed using data from patients in 3 locations in the United Kingdom who were using the National Health Service (NHS) as their primary health care provider. 20 For this study, MYCaW Concerns data from a further 171 participants in the PBCC Living Well with the Impact of Cancer course evaluation 19 and 158 participants cared for at the Ottawa Integrative Cancer Centre (OICC), were analyzed to determine the generalizability of the framework and whether any new concerns had emerged that warranted inclusion. The OICC is a not-for-profit treatment and research centre in Canada offering CIM care to anyone affected by cancer. All people receiving care at the OICC are asked to complete the MYCaW questionnaire as part of an outcomes evaluation. Concerns data collected at PBCC and OICC were coded using the existing framework. Through a constant comparative method potential new concern categories and amendments to existing categories were suggested by either MP, RJ, HS or LW. Changes to the established framework were only made if consensus of opinion was reached, which were accompanied by corresponding changes to the description of the concern categories. (Go to http://www.pennybrohncancercare.org/previous-research to download the qualitative analysis guidelines.)
To assess if any concerns captured on MYCaW were not represented on FACIT-SpEx and vice versa, an in-depth comparison was carried out between each item from FACIT-SpEx and each category listed in the MYCaW qualitative analysis framework. MYCaW Concerns that were not covered on FACIT-SpEx were then searched for on other HRQL PROMs. An electronic literature search of MEDLINE, Cochrane Database of Systematic Reviews, and CINAHL databases, from 2000 to September 2013 was conducted. The search strategy included the following keywords or their combinations: “quality of life questionnaires,” “cancer patients,” “cancer survivors,” “measures,” and “scales.” The search was limited to studies in English and Spanish languages. Instruments were included in the review if they were validated, used in cancer studies and their description and psychometric properties were reported in a cancer population with a varying number of cancer survivor years. Each instrument identified was searched for items that matched the outstanding MYCaW Concerns.
Results
Assessment of Responsiveness
A total of 171 participants were recruited into the PBCC service evaluation and provided baseline data. Of these, 82 participants had complete data at baseline and 6 week follow-up for MYCaW and FACIT-SpEx and were included in the calculations of responsiveness. Seventy-seven percent of participants were female, 33% were male Ages ranged from 18 to >80 years and the majority were aged between 51 and 60 years (35%). A range of cancer types were represented, including breast (54%), bowel (10%), and gynecological (7%). Fifty-one percent of participants were undergoing primary treatment, 21% had completed treatment, and 19% had metastatic cancer.
Convergent Validity
There was a high correlation coefficient of baseline MYCaW Profile scores and the total FACIT-SpEx scores (r = −0.57, P ≥ .01), hence making FACIT-SpEx a suitable HRQL measure to use as an anchor when assessing responsiveness of MYCaW.
Responsiveness
The Concerns and Profile change scores of MYCaW all showed a high SRM and ES (Table 1). The MYCaW Wellbeing score was not as sensitive to change as the other MYCaW scores, although still showed a moderate level of sensitivity to change. The SRMs for MYCaW are highly comparable to those of MYMOP.24,25 Overall, the FACIT-SpEx scores were not as responsive as the MYCaW scores. The highest responsiveness scores on FACIT-SpEx were for Emotional Wellbeing, Spiritual Wellbeing, and the total score.
Scores, Score Changes, SRMs, and Effect Size for All MYCaW and FACIT-SpEx Scores.
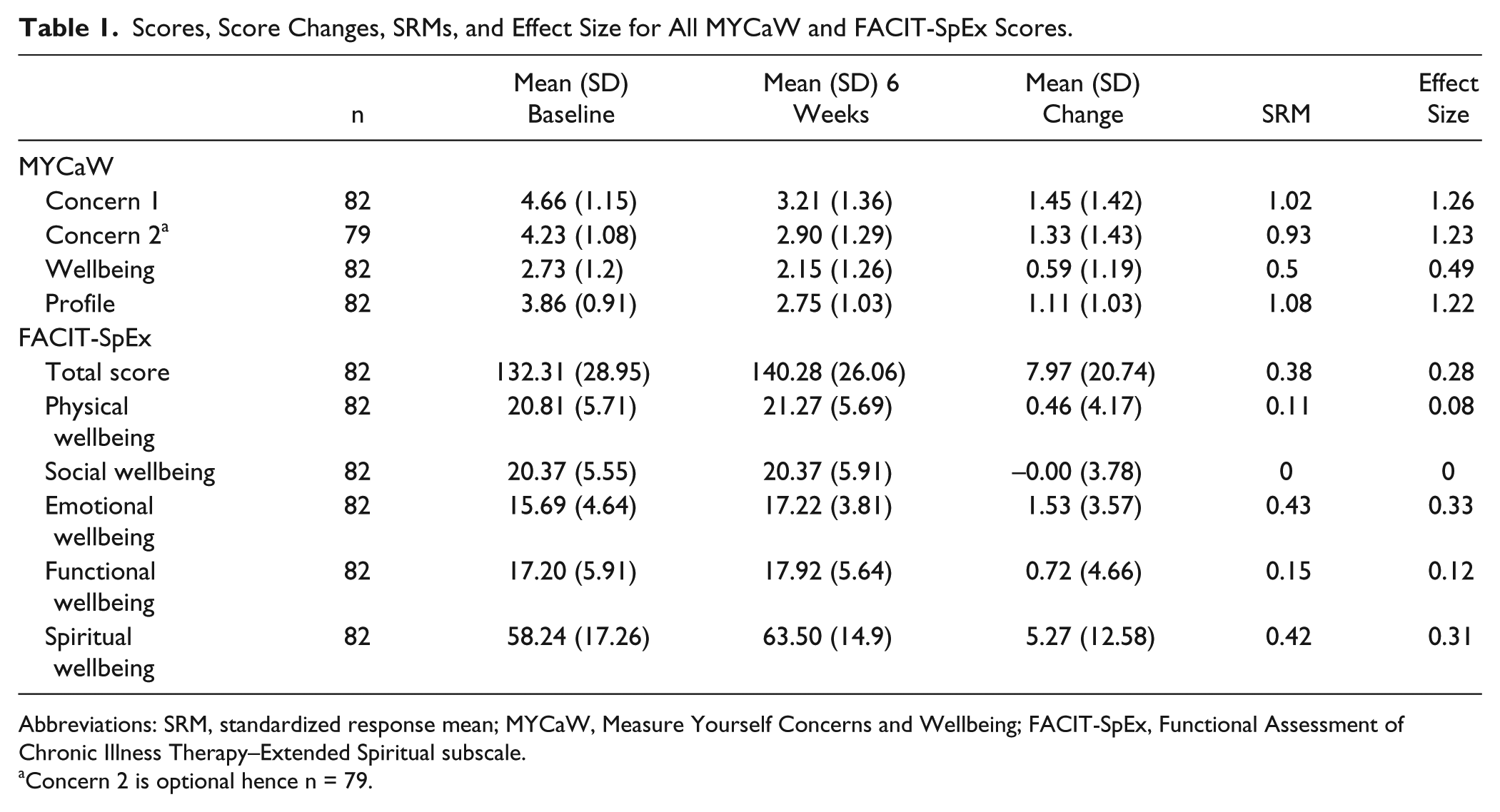
Abbreviations: SRM, standardized response mean; MYCaW, Measure Yourself Concerns and Wellbeing; FACIT-SpEx, Functional Assessment of Chronic Illness Therapy–Extended Spiritual subscale.
Concern 2 is optional hence n = 79.
When the MYCaW data are stratified according to degree of change on the FACIT-SpEx (see Table 2), there is an anticipated gradient of change for the Wellbeing score and to a lesser degree the Concern scores as well. When there was a substantial improvement on the FACIT-SpEx, the highest score changes were seen in each of the MYCaW questions. The MYCaW scores tended to decrease as the degree of change in FACIT-SpEx scores decreased, but did not always follow a smooth gradient.
Mean Change Scores for MYCaW Concern 1, Concern 2, Wellbeing, and Profile Score, Stratified by Degree of Change on FACIT-SpEx.
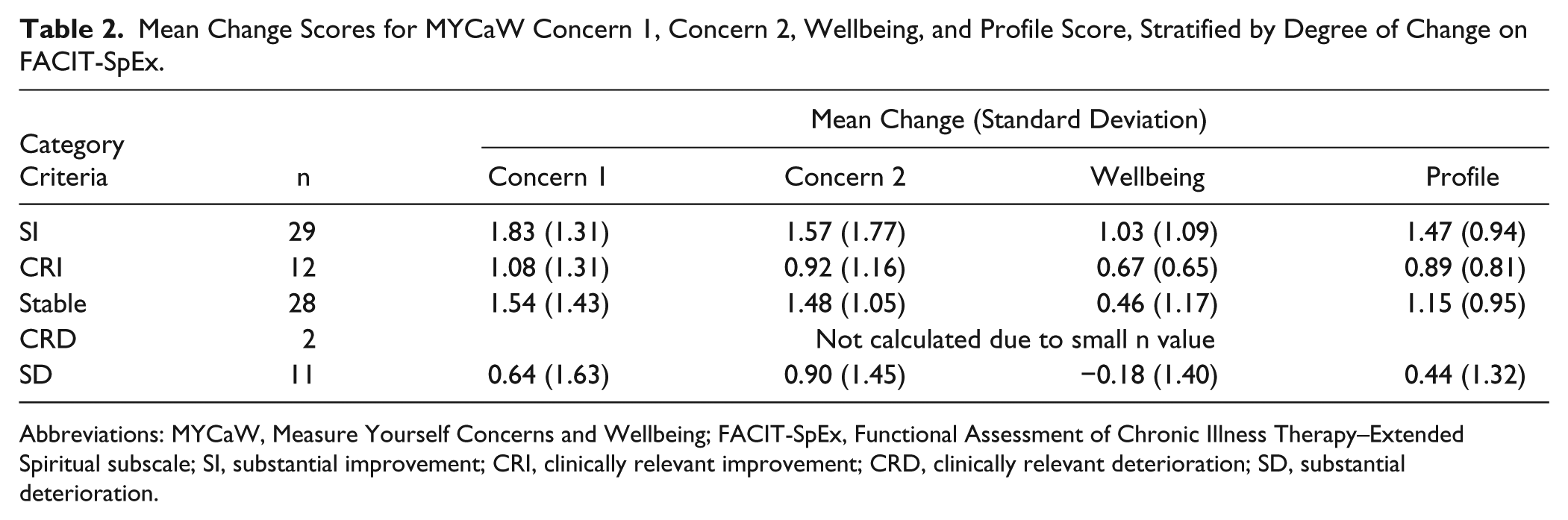
Abbreviations: MYCaW, Measure Yourself Concerns and Wellbeing; FACIT-SpEx, Functional Assessment of Chronic Illness Therapy–Extended Spiritual subscale; SI, substantial improvement; CRI, clinically relevant improvement; CRD, clinically relevant deterioration; SD, substantial deterioration.
Comparable to the change scores in Table 2, the responsiveness indices for MYCaW were also influenced by the FACIT-SpEx categories of change (see Table 3). All the indices were larger for participants who had a “substantial improvement” on FACIT-SpEx than those who had a “substantial deterioration.” For example, the Guyatt response score for MYCaW Concern 1, was 1.28 for the “substantial improvement” category, compared with just 0.45 for the “substantial deterioration” category. The gradient was consistent across the other categories apart from those participants who were “stable” on FACIT-SpEx, with the responsiveness indices being consistently higher, rather than lower, than those in the “clinically relevant improvement” category. There were not enough participants in the “clinically relevant deterioration” category to carry out meaningful analysis. Responsiveness scores for Wellbeing were consistently smaller than for the Concern scores across all of the responsiveness indices used. This is comparable to the responsiveness scores for MYMOP.24,25
T Statistics, Effect Size, Guyatt Response Score, and SRM for MYCaW According to Degree of Change on FACIT-SpEx.
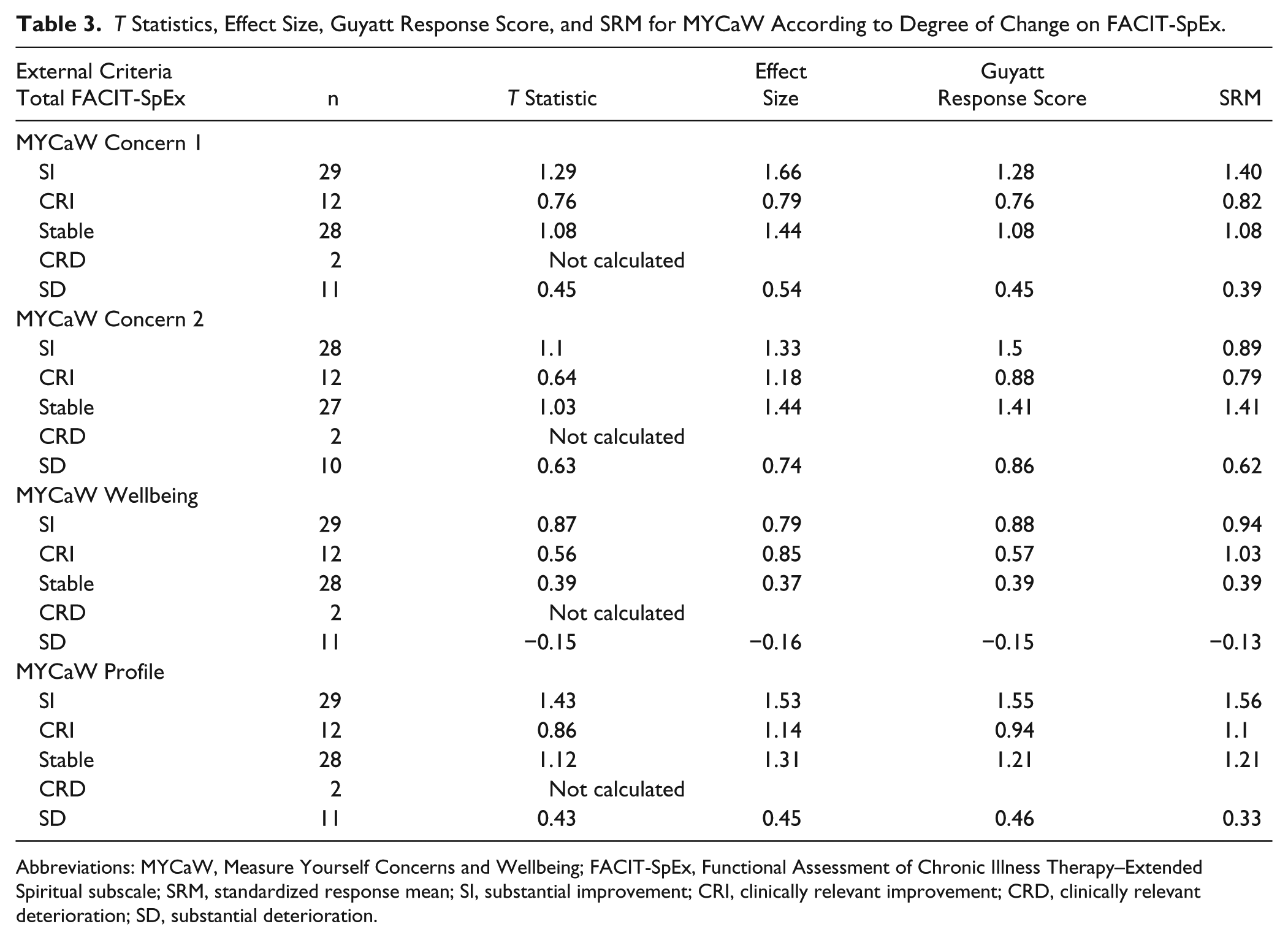
Abbreviations: MYCaW, Measure Yourself Concerns and Wellbeing; FACIT-SpEx, Functional Assessment of Chronic Illness Therapy–Extended Spiritual subscale; SRM, standardized response mean; SI, substantial improvement; CRI, clinically relevant improvement; CRD, clinically relevant deterioration; SD, substantial deterioration.
Determining the Generalizability of the MYCaW Qualitative Coding Categories
Overall, the MYCaW coding framework was deemed representative of Concerns data collected across PBCC and OICC, however, consensus of opinion was reached on several amendments, which reflect new categories to report specific concerns, or clarifications to the names and descriptions of categories to make the framework generalizable to other health care settings. Table 4 presents the changes made to the qualitative analysis guidelines for MYCaW.
Changes Made to Qualitative Analysis Guidelines for MYCaW. a
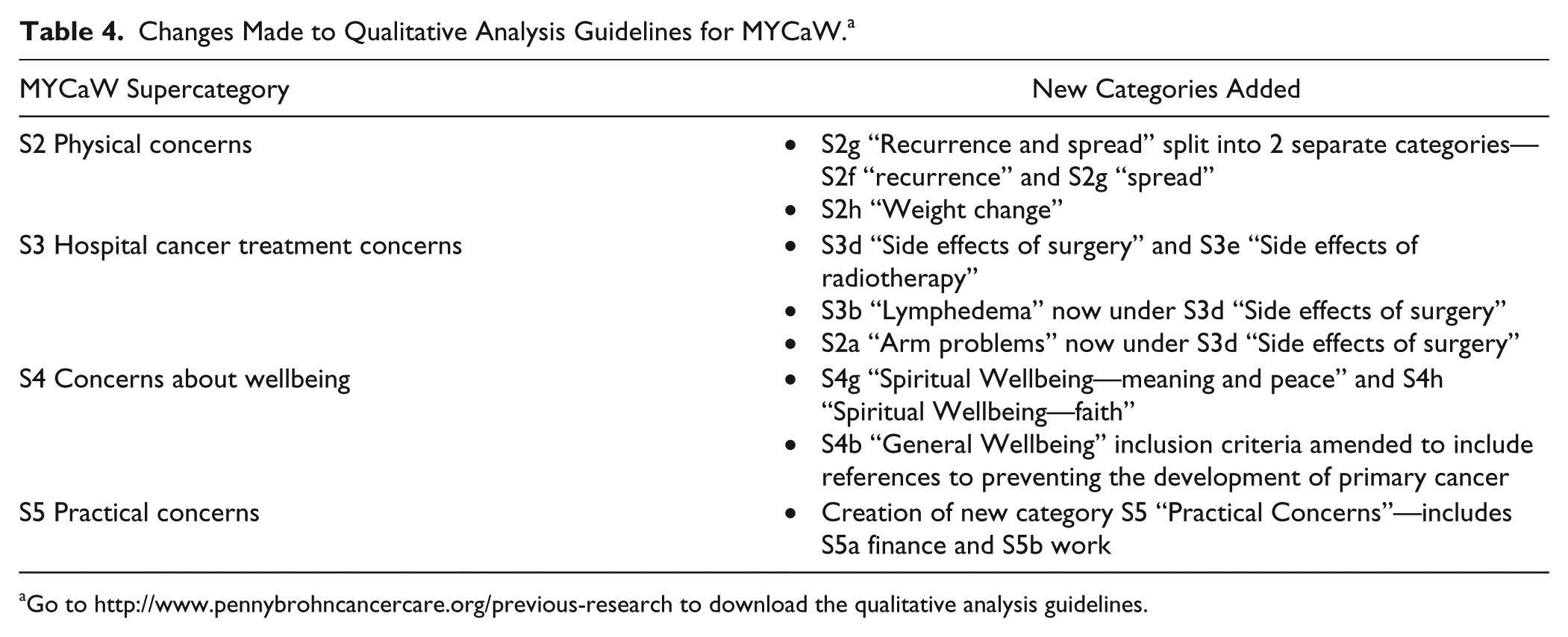
Go to http://www.pennybrohncancercare.org/previous-research to download the qualitative analysis guidelines.
MYCaW qualitative codes were compared with FACIT-SpEx to map similarities. Eleven codes were remaining after mapping to FACIT-SpEx, these were mostly practical-based concerns, that is, “information and guidance on complementary therapies,” “relaxation,” “nutrition,” and “exercise,” and specific physical concerns, that is, “fertility,” “lymphedema,” and “hot flushes and night sweats.”
MYCaW Concern items that could not be found on FACIT-SpEx were searched for on other cancer-related PROMs. There was no instrument identified that contained all the MYCaW Concern categories. Nine instruments were identified that measured one or more aspects of quality of life (eg, physical, psychological, social, and spiritual) and contained one or more of the outstanding MYCaW Concerns: POMS, 27 SF-36, 28 CARES-SF, 29 EORTC QLQ-C30, 30 QLI-CV, 31 FACIT-SpEx, 22 EQ-5D, 32 QoL-CSV, 33 QLACS. 34 One tool, the Distress Thermometer, 35 was also identified that represented some outstanding MYCaW Concerns; however, this tool may be classed more as a consultation aid.
Discussion
This article reports on the first type of validity assessment of MYCaW, which specifically included the responsiveness, generalizability, and content and convergent validity of MYCaW. The data set(s) used for this study represents the experiences of cancer patients who seek complementary and integrative cancer care, the target population for this outcome measure. The analysis has demonstrated that MYCaW scores are highly responsive to change, the qualitative coding framework is generalizable across 2 different CIM oncology settings and MYCaW has the ability to capture a wider range of patient-identified concerns as compared to existing cancer-related PROMs.
Validation of MYCaW Score Changes
FACIT is a well-validated and commonly used tool for measuring HRQL in people with cancer and already has the minimally important difference in score changes defined. 26 For these reasons, FACIT-SpEx was used as a suitable tool against which to validate the responsiveness of MYCaW scores. There was a high degree of correlation of baseline scores on the FACIT-SpEx and MYCaW questionnaires, highlighting good convergent validity of MYCaW. As shown in Table 1, MYCaW score changes for Concern 1, Concern 2, and Profile scores are extremely responsive to capturing the person’s experience of how their concerns change, and more so than FACIT-SpEx. This may be because the participants define their own items - the Concerns - for MYCaW, hence participants know exactly what the concern means to them and perhaps score it more accurately than a predetermined item. The MYCaW Wellbeing score was less responsive to change, but the effect size still indicated a medium effect. The Wellbeing score is arguably more comparable to the total FACIT-SpEx score in how a person perceives their Wellbeing as a total concept and interestingly the respective SRM and effect size scores highlight this (Table 1). The MYCaW SRMs were very similar to those achieved in the sister questionnaire, MYMOP, which was developed for general practice.24,25
To further understand the responsiveness of MYCaW scores, 4 different distribution based analyses were carried out, using the FACIT-SpEx questionnaire as an anchor (Table 3). The raw MYCaW scores and the responsiveness scores followed the expected gradient when compared across the highest and lowest FACIT-SpEx categories of clinical change. By splitting the sample into categories of clinical change, the authors acknowledge that the numbers in each group are much smaller and that the standard deviation is larger, which may affect the accuracy of the responsiveness calculations.36,37 Also there were not enough participants with clinically relevant deterioration to carry out meaningful analysis.
Generalizability of the Qualitative Analysis Framework
The original MYCaW qualitative analysis frameworks were devised using UK data from 3 geographical locations and where participants were using the NHS as their primary treatment provider. MYCaW is used in many complementary and integrative cancer centers internationally, which incorporate a range of healthcare models. Therefore, it was important to determine whether any amendments to the analysis framework would be necessary to accommodate a different integrated model of care and different patient populations across centers. The OICC provides cancer treatment using an integrated model of care led by naturopathic doctors. Patients are primarily female, with a range of diagnoses of advanced cancer. Data collected at the OICC may therefore represent different types of patient concerns than data collected in the United Kingdom as part of MYCaW development. The generalizability analysis demonstrated that the majority of categories within the prior qualitative analysis framework were transferable to the OICC, although additional categories were added, including ones for spiritual Wellbeing, weight change, specific side effects from hospital treatment relating to surgery and radiotherapy, and practical concerns relating to finances and work (Table 4). Levels of spiritual Wellbeing are known to correlate to total Wellbeing 38 and as the use of holistic models of care increases, measuring the effect of CIM on spiritual Wellbeing is very important. Similarly there is a growing acknowledgement of the financial burden of cancer and how diagnosis and treatment has a profound effect of practical issues for many members of the family. 39 The assessment of generalizability across a total of 4 different CIM centers, including resultant refinements to the qualitative analysis framework, suggests that MYCaW is broadly applicable across different settings. People seeking care at the OICC and PBCC are representative of the broader population of people seeking complementary and integrative cancer care, who are more commonly female, of middle age with advanced diagnoses. While the MYCaW coding framework appears generalizable across these centers, the authors acknowledge the need for similar generalizability assessments across a greater range of countries, cultures, and models of CIM care. The authors would welcome collaborations with other CIM centers who use MYCaW and would like to contribute to such analyses.
There was high convergent validity when correlating FACIT-SpEx scores with MYCaW scores. It was notable, however, that several MYCaW Concerns were neither represented on FACIT-SpEx nor on other commonly used HRQL tools. Concerns about healing and arm problems were not represented cancer-based HRQL tools, or tools used as clinical decision making aids. While some questionnaires have bolt-on subscales that may cover lymphedema, when evaluating a heterogeneous sample of participants, it is necessary to be able to identify all relevant concerns quickly and simply. Furthermore, Concerns data on MYCaW associated with arm problems covered issues such as restricted movement, not just lymphedema. Concerns relating to relaxation, guidance on complementary therapies, nutrition (relating to knowing what foods are best to eat, as opposed to side effects around eating problems) and lymphedema could only be found on clinical aid tools, such as the Distress Thermometer 35 and other holistic assessment tools. 40 It is noticeable that these types of concerns tended to be less about medical issues and more about what the patient could be doing to support themselves. While patients are able to access information on the internet and hear about potential avenues to support themselves, they are very vulnerable to accessing and following unevidenced approaches. It is also noteworthy that during treatment in many hospitals it is variable as to whether these areas of concerns relating to nutrition, healing, relaxation or guidance on CAM are even discussed. It is our observation that if a patient reports his or her top 2 concerns as hot flushes and access to information about complementary therapy, for instance, then it is likely that these concerns are so severe that the person needs professional support and the concerns will not just improve over time. Therefore, while a clinician may not perceive these issues as life-threatening or a priority in the patient’s treatment plan, for the patient these concerns are likely to be causing them a degree of distress or anxiety and do need discussing.
The growing use of CIM in cancer treatment and support means that tools being used for researching the effectiveness of these models of care, need to capture all the variables relevant to patients for meaningful data analysis to be performed. So while there are a plethora of tools to assess and measure patient reported outcomes, there are very few that are being used in research that fully represent all the items that are important to patients. Furthermore, failure to measure all outcomes relevant to patients will lead to a bias in the reporting in effectiveness of CIM health care models.
MYCaW to Personalize Approach
MYCaW was developed in response to the need for cancer centers offering complementary supportive care to people with cancer and their supporters/carers, to be able to document fundamental reasons why patients were using their service (as an extra to the treatment already received in the NHS), to develop a method of quickly determining the most pressing concerns to be addressed (as a clinical assessment tool to compliment the holistic medical history) and to quantify whether after a series of therapy sessions the patient felt that the severity of their concerns had decreased. Further data were collected on follow-up, to understand what else a person thought may also affect their health, and what was most important about the centre visited.
As with any organization, optimizing the service provided to best meet the needs of the users is fundamental to success of the patient outcomes.
One limitation of MYCaW is that it cannot be used solely to measure quality of life, as the tool only measures the main concerns a person has and does not compare the same list of items for each person. Therefore MYCaW is not intended to be used to replace a quality-of-life outcome measure, more as an adjunct in these circumstances, as it can capture concerns that are important to the patient that may not be listed on the quality-of-life measure.
Furthermore, this article only reports on some validity analysis of MYCaW. There are other aspects of psychometric analyses that have not yet been carried out that could further determine how well MYCaW performs.
In summary, MYCaW is fast to administer, is suitable for use with a heterogeneous group of patients, can be routinely incorporated into clinical administration processes and is responsive to change. Concerns data can determine a patient’s primary needs and facilitate a more personalized service to be offered. MYCaW data can determine why patients use a service, how they respond to treatment and what aspects of the service are beneficial. Such information can be used to inform future pathways of care and use funding efficiently. The analysis framework allows comparison of data internationally and is suitable for a range of CIM health care models. As a research tool, MYCaW is a valuable addition alongside other validated HRQL tools to ensure that all patient variables have been captured. These data can inform a more accurate design and analysis of comparative effectiveness research. Finally, as cancer treatments increasingly incorporate CIM, MYCaW allows holistic concerns to be captured where traditional research tools do not.
Footnotes
Acknowledgements
We thank the participants for taking the time to give us their data and to share their experiences in such an honest and open way. The James Tudor Foundation for supporting the Research and Evaluation Department at PBCC. We also thank Dr Catherine Zollman and Jo Durrant for their informed discussions of the data.
Authors’ Note
Raw data can be accessed by contacting any of the named authors in this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.