
Abstract
Purpose:
HNC poses significant health challenges globally with over 650 000 new cases annually. Studies have demonstrated the benefits of exercise for many cancer types, with several exploring the effects of exercise on various molecular biomarkers. However, no study has systematically explored these effects among HNC survivors.
Methods:
Studies published up to February 2024 were screened on PubMed, SCOPUS and Web of Science using relevant keywords yielding 838 results. Studies that explored the effect of exercise-based interventions on molecular biomarkers among HNC survivors were eligible for inclusion. Risk of bias was assessed using the Joanna Briggs Institute quality assessment tool.
Results:
Three studies were included in the review. Primary biomarkers assessed were inflammatory (eg, IL-6, TNF-α), oxidative stress (eg, 8-OHdG, MDA), and collagen fragment markers (eg, IC6, ProC3). Significant changes were observed in collagen fragment markers, specifically Pro C3, IC6 and IC6/C6M over time, although no correlation with lean body mass was found. Oxidative stress markers improved following exercise, with increases in total antioxidant capacity, decreases in 8-OHdG and carbonyl content. However, no significant changes were found in inflammatory markers or DNA methylation patterns post-intervention.
Conclusion:
Our review suggests that exercise shows potential in modulating physiological and molecular pathways’ among HNC survivors. Although only 3 studies were eligible for inclusion, these benefits might potentially translate into improvements in health-related outcomes amongst HNC survivors. Future large-scale trials with standardized exercise protocols and extended follow-up periods might improve our understanding of the long-term effects of exercise on biomarkers and survivorship outcomes in HNC.
Introduction
Each year 650 000 new HNC cases are diagnosed globally, making it a significant public health concern. 1 The location and extent of the tumor limit the available treatment options, and hence this condition is seldom associated with poor prognosis, particularly in its advanced stages. 2 Surgery, radiation therapy, and chemotherapy are examples of conventional treatment options that often lead to serious side effects. These include fatigue, pain, decreased quality of life (QOL) and sarcopenia, which is characterized by a loss of muscle mass, strength and physical performance. 3 Additionally, these treatments options may also result in long-term adverse events that negatively impact survivorship outcomes and overall, well-being.
While there is extensive evidence on the benefits of exercise, especially for cardiometabolic health in people with obesity4,5 as well as for improving psychological health for individuals with anxiety and depression,6,7 there is a growing body of evidence suggesting that exercise has numerous benefits in the management of various cancers, such as HNC, by promoting not only physical health but also improving the survivors quality of life (QOL).8,9 The physiological pathways through which exercise leads to these benefits is complex and multifaceted, possibly mediated through molecular, cellular and systemic adaptations.10,11 Various underlying mechanisms such as decreased stress response and improved metabolic and immune system functions are believed to be the complex pathways through which regular exercise might modulate cancer related outcomes. 12 In addition, amongst breast cancer survivors, exercise has been widely recognized as an effective non-pharmacological intervention to reduce levels of pro-inflammatory biomarkers, improve cardiovascular disease risk profiles, and enhance mental health as well as physical functioning.13–15
The promising role of exercise on several physiological and molecular pathways amongst cancer survivors has gained significant attention in the past decade. Literature suggests that exercise was associated with reduced levels of inflammatory markers such as interleukin-6 (IL-6) and tumor necrosis factor-alpha (TNF-α), as well as increased levels of anti-inflammatory markers like interleukin-10 (IL-10). 16 Lower levels of these respective inflammatory biomarkers have been associated with enhanced physical performance. Exercise has also been associated with inducing epigenetic changes where in, 163 differentially methylated sites were observed in gene locomotor regions. 17 These changes might contribute to the ability of exercise as an intervention to mitigate fatigue and improve various cancer related outcomes among HNC survivors. 18 For example, a recent study found that aerobic exercise was associated with reduced levels of soluble TNF receptor II (sTNFR2), although it did not significantly influence other inflammatory markers. 19 Hence, these findings highlight the potential of exercise to positively influence various inflammatory and complex genomic pathways among HNC survivors.
There is paucity of evidence underlining the effects of exercise-based interventions on biomarkers in HNC survivors. Investigating links between exercise and biomarkers relevant to HNC may further our understanding of the disease and its relationship to exercise as an adjuvant treatment to cancer.
Hence this review investigates the existing evidence on the impact of exercise-based interventions on molecular biomarkers among HNC survivors. Better insights of how these biomarkers interact and/or respond to exercise could lead to development of tailored exercise protocols and thus improve survivorship outcomes in the long run.
Methods
Registration
The systematic review was conducted in accordance with The Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA) statement. 20 An initial search was conducted to identify systematic reviews and/or meta-analyses conducted on a similar topic and identify any ongoing or previously registered studies. Accordingly, the current review protocol was submitted to PROSPERO and was registered on 12th February 2024. (registration number CRD42024508084, available at https://www.crd.york.ac.uk/prospero/#recordDetails).
Research Question and Search Strategy
Studies regarding the effectiveness of exercise on biomarkers amongst head and neck survivors were selected based on a pre-set PICOS format:
“PICOS”
P (population) = adult head and neck cancer survivors (aged 18 years and older) with a histologically proven squamous cell carcinoma of head and neck regions. Any clinical stage with no distant metastasis and receiving or completed anti-cancer treatments (adjuvant or neo-adjuvant chemotherapy and/or radiotherapy and/or surgery [pre/post medical management]).
I (intervention) = Structured exercise program as a rehabilitation administered pre-, during or post cancer treatment.
C (Comparison) = Any comparator including pharmacological, non-pharmacological, or no intervention.
O (Outcome) = Potential modifications in biomarker levels assessed using blood samples or tissue biopsies.
S (Study Design) = Clinical Studies
Studies were excluded during full-text screening if: (a) the study population did not include patients diagnosed with head and neck cancer; (b) did not include a structured exercise-based intervention; (c) did not assess molecular biomarkers as an outcome; (d) were review articles, editorials, or protocols; (e) full text not in English language.
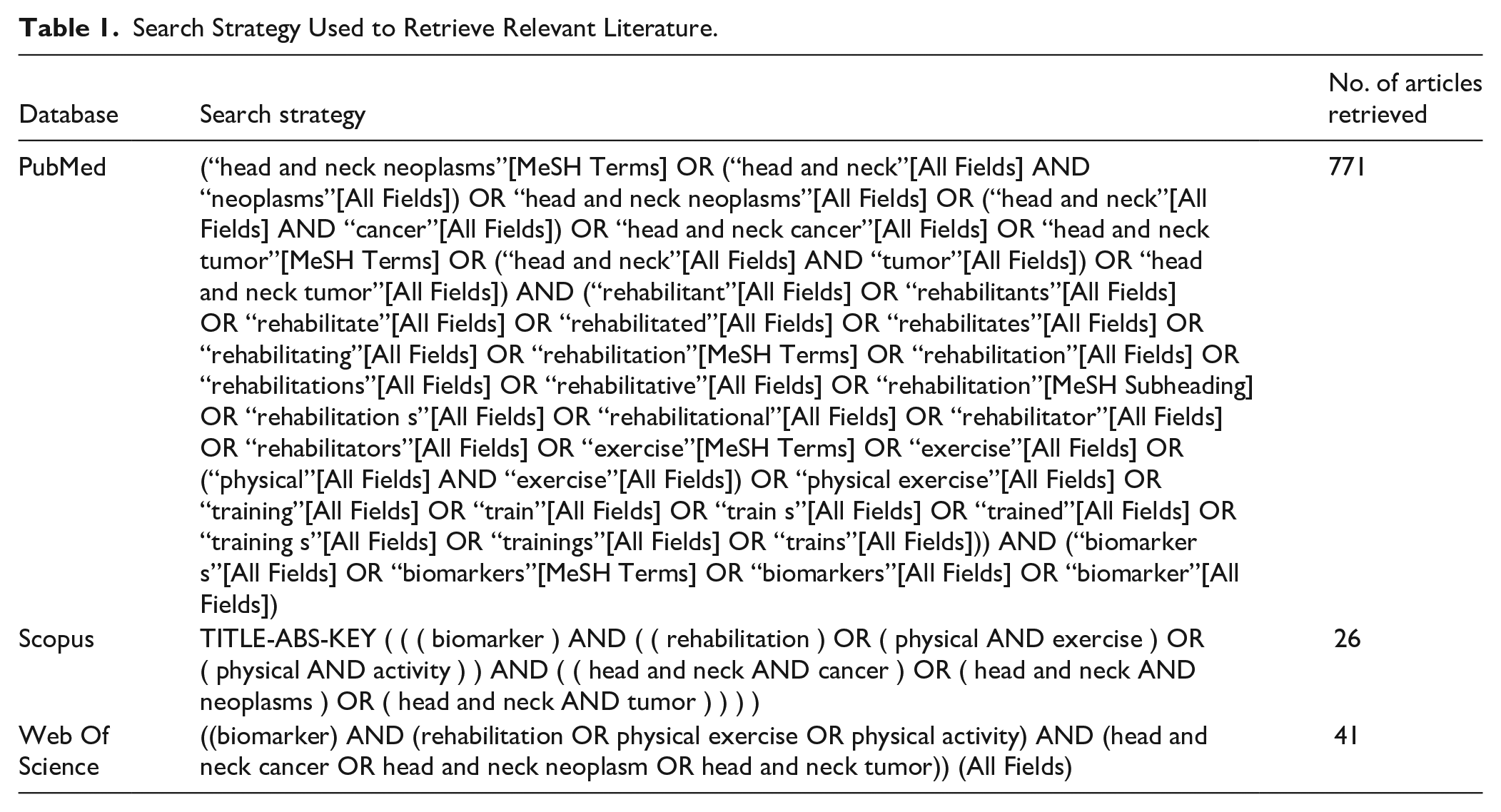
Two authors (HP and SD) performed a comprehensive search for relevant studies on 3 databases PubMed, Scopus, and Web of Science (WOS) to retrieve articles from inception to February 2024, by combining MeSH terms and keywords using the appropriate Boolean operators “AND” and “OR” to identify relevant literature. The keywords “exercise,” “biomarkers,” “head and neck cancer” were used to obtain the relevant literature. Logical operators “AND” and “OR” were combined with appropriate filters. Table 1. provides the complete search method as well as the number articles retrieved from the 3 databases.
Search Strategy Used to Retrieve Relevant Literature.
Study Selection
Post removal of duplicates, all articles were retrieved and screened for eligibility by the authors independently. Study selection was performed by 2 authors (HP and SD) based on the inclusion and exclusion criteria, screening of title and abstracts (linear evaluation) followed by full-text screening. The studies were eligible for inclusion if they met the preset PICOS criteria. Discrepancies were sorted following a discussion with SRS, KVK, and PMP following which a decision of either inclusion or exclusion of articles for the current systematic review was agreed upon.
Data Extraction
The data extraction was done using a prior designed data extraction sheet comprising of the following: first authors name, year of publication, country, study design, study population (EG or CG), stage of tumor, type of treatment (RT/CT/Surgery), exercise intervention (FITT), outcomes (biomarkers), and secondary outcomes assessed. Results were described as mean and standard deviation where possible.
Assessment of Study Quality
The Joanna Briggs Institute (JBI) critical assessment checklist was used to appraise the quality of the studies. 21 The quality of the studies was assessed by 3 authors HP, SD and SRS. The studies were analyzed using JBI checklist for quasi experimental studies 2023 and JBI critical appraisal tool for assessment of risk of bias for RCT 2023.
Data Synthesis
Data extracted from the included studies were synthesized qualitatively to report the findings. Meta analysis was attempted if there were more than 2 studies reporting the same outcome using the same parameters. However, in this review we did not find studies for pooled quantitative analyses.
Results
Study Selection
A total 838 studies were retrieved from 3 databases (PubMed, Scopus, and Web of Science), using relevant keywords and MeSH terms from “identification of studies via databases and registers”. Post removal of duplicates (25), a total of 813 studies were identified and screened. After the exclusion of 807 studies, 6 full text studies were sought for retrieval. However 5 studies were assessed for eligibility as the full text of 1 study could not be retrieved. 22 Of these 5 studies, 1 record did not include a specific exercise regimen, 23 and 1 study included another intervention (neuromuscular electrical stimulation). 24 Furthermore, 3 studies were identified via other sources (backward citation) of which all 3 were excluded as they did not include relevant molecular biomarkers. The studies shortlisted for full text screening and reasons for exclusion are detailed in Figure 1. 3 studies were included in the current review.25–27 Efforts were made to obtain additional details from the study authors for clarification purposes; however, responses were not received, or the requested information was unavailable.

PRISMA 2020 flow diagram for new systematic reviews which included searches of databases, registers and other sources.
Characteristic of the Studies
The studies included in the current systematic review were published between 2015 25 and 2020.26,27 One RCT was conducted among the Dutch (Denmark) HNC survivors 25 in 2015, another pilot study was conducted in the United States in 2020, 26 and the third study, a single arm pre-post design was conducted among Taiwanese HNC survivors in 2020. 27 A summary of the participant and exercise program characteristics is provided in Table 2.
Description of Exercise-Based Interventions in the Included Studies.

Note: I, intensity; D, Duration; wk, week; min, minutes; IG, intervention group; CG, control group; RM, repetition maximum.
Study Participants
One-hundred and eighteen (118) subjects were assessed in the present review of which 97 were HNC survivors. In the RCT, the authors recruited 62 subjects with corresponding 21 healthy participants as age and gender matched controls. 25 The pilot study included 26 HNC survivors, with 14 enrolled in the control group. 26 Furthermore, the study conducted among Taiwanese HNC survivors recruited 30 survivors (Control group = 14 and Intervention group = 12) in an 8-week exercise program. 27 The mean age of the HNC survivors included in the studies was 56-57 years, of which 97 were males and 24 were females. Majority of the survivors (84%) in the study by Xiao et al, were in advanced stages of HNC that is, stages III and IV. 26 The average BMI of the participants in 2 studies ranged from 23.4 ± 3.6 25 to 26.89 ± 4.2. 26 The study conducted by Yen et al, failed to specify the stage of carcinoma the survivors presented with, 27 however the survivors in the remaining 2 studies presented with stages I to IV.25,26 The survivors recruited in the studies received varying from of anti-cancer treatments such as radiotherapy, 25 chemotherapy, 27 and a few survivors underwent neoadjuvant therapies with Intensity—Modulated Radiation Therapy (IMRT). 26
Exercise-Based Intervention
The participants in the three studies were enrolled in progressive resistance training (PRT) programs. Two studies included both resistance and aerobic training in their regimes.26,27 The exercise interventions ranged from 8 to 12 weeks, with an average of 2 to 5 sessions performed per week. The studies involved varying levels of supervision with Yen et al, providing fully supervised sessions in the university gym by a physiotherapist, Nedergaard et al, providing semi-supervised sessions that is, 7-8 supervised sessions of 30 sessions in a commercial gym and Xiao et al, providing a home-based rehabilitation program with no direct supervision. 26
The Danish survivors were enrolled in a strength training program involving the upper and lower extremities using machine or body weight exercises, 25 while the participants in the other studies utilized resistance bands targeting both their upper and lower extremities.26,27 The participants performed progressive resistance exercises (incremental volume and load) with each exercise involving 3 sets of 10-15 repetitions.
Two studies incorporated moderate intensity aerobic exercises in their intervention protocol lasting 30 min per day.25,27 One was a structured program including warm-up and cool-down sessions, 25 and the study by Yen et al, involved an incremental walking program which was objectively monitored with a multisensory wrist band used to monitor the progression as a measure of adherence. 27
The Biomarkers
A variety of biomarkers were analyzed in the current review; additional analyses were also performed in some studies to explore the relationship between the biomarkers and cancer related outcomes. Oxidative stress markers among HNC survivors were assessed by Yen et al, including total antioxidant capacity, malondialdehyde (MDA), carbonyl content and 8-hydroxy-2’-deoxyguaosine (8-OHdG). 27 Nedergaard et al, explored the changes in collagen fragment biomarkers like Pro C3, IC6, C6M and the ratio between levels of IC6 and C6M different time points during the exercise intervention. 25 The study also aimed to investigate the correlation between the collagen fragment biomarkers as markers of lean body mass (LBM) not only among HNC survivors but also the age matched controls. 25
Inflammatory markers such as C-reactive protein (CRP), interleukin 1 receptor antagonist (IL1ra), interleukin 6 (IL6), monocyte chemoattractant protein (MCP1), soluble tumor necrosis factor receptor 2 (sTNFR2) and tumor necrosis factor α (TNFα) were assessed by Xaio et al. 26 In addition, the authors also investigated the epigenetic changes by analysing the DNA methylation patterns among HNC survivors. 26
Assessment of Outcome
A summary of the results is provided in Table 3. Two of the three studies reported some significant differences in the biomarkers examined. Specifically, Nedergaard et al 25 compared biomarker levels at baseline and across time between the intervention groups (IG) and control groups (CG). At baseline, no significant differences were found between the IG and CG for IC6 and ProC3 or for the IC6/C6M ratio. However, significant effects for time (P = .016) and borderline significant effects for group (P = .057) were noted for IC6 across time. In addition, the IC6/C6M ratio also showed significant effects for time (P = .028) and borderline group effects (P = .05) for changes across time. However, post-hoc results indicated no significant differences at any time points.
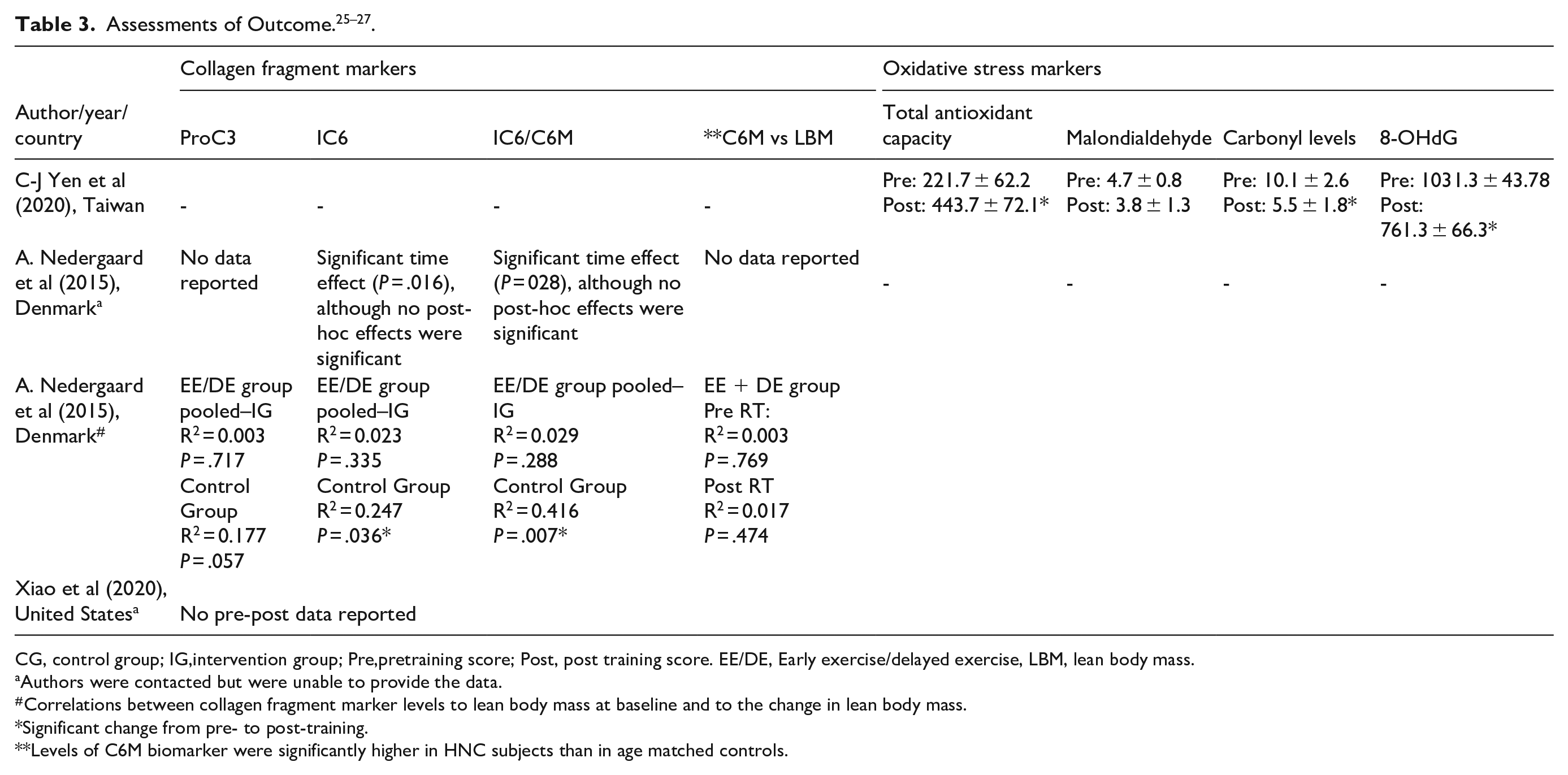
CG, control group; IG,intervention group; Pre,pretraining score; Post, post training score. EE/DE, Early exercise/delayed exercise, LBM, lean body mass.
Authors were contacted but were unable to provide the data.
Correlations between collagen fragment marker levels to lean body mass at baseline and to the change in lean body mass.
Significant change from pre- to post-training.
Levels of C6M biomarker were significantly higher in HNC subjects than in age matched controls.
The exercise intervention (aerobic + resistance) catered to the survivors by Yen et al led to significant rise in total antioxidant capacity levels post training (P < .05). Additionally, plasma levels of 8-OHdG (marker of oxidative DNA damage) and carbonyl content were significantly reduced post-intervention. However, malondialdehyde (MDA) levels did not show significant changes post-intervention. 27 In contrast, no significant differences in any inflammatory markers including CRP, IL1ra, IL6, MCP1, sTNFR2 or TNFα were reported by Xiao et al. 26
Correlations between several inflammatory and immune function markers and outcomes relevant to overall health and physical function were reported in two studies. As seen in Table 3, Nedergaard et al. 25 found no significant correlations between lean body mass (LBM) and IC6 (R2 = 0.024, P = .335), ProC3 (R2 = 0.003, P = .717) and the ratio between IC6 and C6M (R2 = 0.003, P = .288) at baseline in 41 HNC survivors. Although two of these correlations were significant (IC6 and IC6/C6M) among healthy individuals. In addition, no significant correlations between the rate of LBM regain and C6M levels were observed pre (R2 = 0.003, P = .769) and post (R2 = 0.017, P = .474) resistance training.
Xiao et al 26 also examined correlations between several inflammatory markers to fatigue and physical function. While no significant group differences were observed in inflammatory markers post-intervention, significant correlations were observed between inflammatory markers, fatigue, and physical function. Fatigued patients had significantly higher levels of CRP (P = .021). Lower levels of CRP, IL-6, IL-1ra, TNFα and sTNFR2 were significantly associated with better physical function test performance, including six – minute walk distance, chair stand, and bicep curl tests (P < .05). A summary of the results is provided in Table 4.
Correlations Between Inflammatory Marker Levels to Fatigue and Physical Function Post-Training from Xiao et al. 26 .

6MWD, 6-minute walk distance; CRP, C-reactive protein, IL1ra, interleukin 1 receptor antagonist; IL6, interleukin 6; MCP1, monocyte chemoattractant protein 1; sTNFR2, soluble tumor necrosis factor receptor 2; TNFα, tumour necrosis factor α; MCP1, monocyte chemoattractant protein 1.
Significant correlation coefficients among fatigue, physical function and inflammation at 3 months, Fatigue measured using Multidimensional Fatigue Inventory-20.
Quality Assessment
The present systematic review used the Joanna Briggs Institute (JBI) critical tool of appraisal as a quality assessment tool to assess the quality of the study methodology. 21 Scores were assigned based on the questions as “Yes,” “No,” “Unclear,” and “Not Applicable” The detailed result of the critical appraisal is mentioned in Table 5. Given the varying study designs, the risk of bias assessment was applied to each individual study using the JBI tool
Assessment of Study Quality.

Note: The results of the risk of bias have been presented based on sum of the scores of the individual the domains of critical appraisal, with “1” indicating Yes, “2” indicating No, “UC” indicating unclear and “N/A” indicating Not applicable. The studies were critically appraised using the Joanna Briggs Institute quality assessment tool.
For the randomized controlled trail (RCT) conducted by Nedergaard et al, the study provided some clear and precise information related to internal validity and statistical conclusion validity, however it ranked poorly for the risk of bias related to selection and allocation as well as administration of the intervention. 25 However, additional details were sought from the authors for greater clarity on the analysis. For studies by Yen et al, and Xiao et al, the JBI checklist for quasi-experimental studies was applied, with the authors providing thorough information concerning both internal validity and statistical conclusion validity.26,27
Discussion
The present review aimed to assess the effects of exercise-based interventions on molecular biomarkers, specifically those associated with inflammation, collagen fragment and oxidative stress in HNC survivors. The Joanna Briggs Institute (JBI) critical appraisal tool was used to evaluate the methodological quality of the included studies. 21 This systematic review included 3 studies25–27 that met the inclusion criteria. Although the studies were somewhat heterogenous with respect to aspects of their methodology, designs, and biomarkers assessed, this review highlights the significant research gap in evaluating the effects of exercise-based interventions on molecular biomarkers among HNC survivors. The identified studies collectively underscore the potential of exercise-based interventions to modulate molecular pathways. Moreover, the various biomarkers assessed in these studies reflect the potential benefits of exercise on various physiological systems, thus demonstrating its potential influence on inflammation, oxidative stress and extra cellular matrix (ECM) remodelling. Thus, the findings of this review provide preliminary insights which can help guide future standardized investigations in cancer research.
The average age of the HNC survivors was 56 to 57 years, with most of them being males and in advanced stages (III-IV) of cancer. The studies included in the review comprised of resistance and aerobic exercise regimes that ranged for a duration of 8 to 12 weeks, with varying levels of supervision of the survivors enrolled in the studies ranging from supervised exercise programs25,26 to home-based exercise protocols. 27 The studies included in current review analysed biomarkers such as oxidative stress, 27 collagen fragments, 25 and inflammation. 26 After exercise intervention significant changes were observed in oxidative stress markers, particularly 8-hydroxy-2'-deoxyguanosine (8-OHdG) and protein carbonyl content. 27 These findings are consistent with current literature underlining the positive effects of exercise (both aerobic and resistance training) on the aforementioned outcomes. In particularly, reductions in oxidative stress resulting from exercise-based interventions have the ability to trigger specific cellular pathways that could potentially improve acute oxidative stress tolerance which may decrease the adverse effects of anticancer treatments like chemotherapy on healthy tissue.11,27,28
Although literature suggests that there have been notable reductions in inflammatory markers such as CRP, IL-6, and TNF-α post aerobic and resistance training among colorectal and prostate cancer survivors, 29 our review did not observe significant reductions in inflammatory markers amongst HNC survivors. 26 These discrepancies may be due to the shorter duration of the exercise intervention that is, 8 weeks, or the distinct inflammatory profiles of HNC survivors, who due to their advanced stages may show resistant or complex responses to exercise. Furthermore, the absence of appreciable changes in levels of inflammatory markers could indicate that the dose or type of exercise prescribed to the survivors may not have been sufficient to cause the inflammatory profiles of the survivors to elicit a detectable anti-inflammatory response.
However, the findings from our review suggest that participants who engaged in exercise experienced reductions in fatigue and improvements in physical function, such benefits were significantly correlated with inflammatory markers, including IL-6, IL-1 receptor antagonist, TNF-receptor II, and CRP. 26 These results are consistent with previous studies highlighting elderly subjects who participated in aerobic exercise had significantly lower levels of IL-6 and TNF α. 30 These results indicate that among HNC survivors receiving active anti-cancer treatments, the modulations in inflammatory and epigenetic pathways may be linked to exercise-based treatments catered during the anticancer treatments, leading to enhanced physical functions and decreases in fatigue scores.11,31,32 It is however unclear if the exercise-related improvements in physical performance and fatigue improvements are caused by or contribute to the maintenance of inflammatory improvements consistent with levels for individuals without cancer.
Collagen fragment markers provide unique insights into extra-cellular matrix (ECM) remodelling, a process essential to understanding tumour progression and metastasis. 33 Unlike oxidative stress and inflammatory markers, which reflect systemic physiological responses, collagen fragment markers indicate tissue-specific changes within the tumour microenvironment, including changes in ECM composition and structure. 33 This review found that biomarkers such as IC6, ProC3, and the IC6/C6M ratio were found to be linked with lean body mass (LBM) in healthy individuals (age matched controls), thus suggesting that collagen fragment biomarkers may be useful as biomarkers of LBM among cancer survivors. 25
However, the published work in this area did not note any appreciable changes in the levels of these biomarkers or anabolic responses to exercise measured by variation in LBM among HNC survivors undergoing resistance training. The authors reported that modest changes were seen in biomarkers over time, with IC6 and IC6/C6M showing substantial time effects, but no significant post hoc differences were noted between specific time points. This could imply that there was no significant impact of resistance training in a short time interval on collagen fragment biomarkers.
Based on the findings presented in our review, there seems to be variable and limited evidence regarding the effect of exercise on collagen fragment biomarkers among HNC survivors. These biomarkers have potential as measures of LBM among healthy subjects, however their role among cancer survivors may be diminished due to the complexity of physiological pathways between the anti-cancer treatment and muscle metabolism.
Thus, the available evidence indicates that exercise-based interventions particularly in HNC survivors may have the potential to positively influence molecular biomarkers via processes involving the immune function, body composition, extracellular matrix remodelling and oxidative stress mechanisms. However, further research is necessary to thoroughly comprehend these relationships and optimize exercise based interventions among HNC survivors.
Conclusion
The results of our review emphasize that exercise can lead to several physiological benefits for HNC survivors, including enhanced antioxidant capacity, regulation of collagen specific as well as inflammatory biomarkers which can consequently lead to improved physical performance. The effects on specific biomarkers, particularly collagen-related and inflammatory markers, is variable and not conclusive, hence requiring further exploration. However, our review could provide valuable insights for future large-scale trials on biomarker—specific responses to exercise among HNC and other cancer populations.
We do acknowledge a number of limitations within our review that may limit the generalisability of these results. These include the inclusion of only 3 studies with relatively small sample sizes (n = 26–62 participants per study) and some inter-study variation in study designs, exercise programs, and outcome measures. At the relatively short follow-up periods and confounding factors, like variability in baseline health status and concurrent treatments, also restrict the generalizability of our findings.
To thoroughly understand the long-term effect of exercise on biomarkers, future large-scale trials must be conducted with standardized exercise-based regimes and longer follow-up periods. Detailed studies elucidating the exact mechanisms by which exercise impacts cancer as well as the overall systemic health might help advance the scope of exercise as an adjuvant therapy particularly during the advanced stages of the disease.
Footnotes
Acknowledgements
Manipal Academy of Higher Education.
Ethical Considerations
This is study is a systematic review, ethics approval and consent to participate are not applicable
Consent for Publication
Stephen Rajan Samuel is an Associate Editor for Integrative Cancer Therapies, but did not take part in the review or decision process for this manuscript.
Author Contributions
Concept, idea and research design were conducted by HP, SD, KVK and SRS. Writing by HP, SRS, SD and JK. HP, KVK, SRS, PMP, PM, and JK edited the draft of the manuscript and prepared figures and tables. All authors contributed to the critical review of the manuscript before submission.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.