
Abstract
Background:
Adherence in rehabilitation services includes attending appointments, regularly performing prescribed exercises, and correct exercise execution. The Exercise Adherence Rating Scale (EARS) has been adapted into several languages, but there is lack of a standardized tool for various Indian languages and cultural contexts, particularly for use with cancer survivors. With the anticipated 57.7% rise in cancer cases by 2040, this study aims to address this gap.
Aims and objectives:
To cross-culturally adapt EARS to Kannada (EARS-Kn) and evaluate its validity and reliability amongst HNC survivors enrolled in the Multimodal Oncology Rehabilitation Exercise—MORE© Program.
Methodology:
Following Beaton guidelines, the EARS tool was adapted to Kannada. 34 HNC survivors engaged in the MORE© program. Internal consistency (Cronbach’s ⍺) and construct validity (Exploratory Factor Analysis, EFA) were assessed. The Receiver Operating Curve (ROC) determined cut-off scores, sensitivity and specificity of the EARS-Kn.
Results:
The EARS-Kn demonstrated a Cronbach’s-⍺ value of .93. The EFA revealed a one-factor solution with eigenvalues exceeding one and 70.1% loading. The area under the curve (AUC) was 0.908. A cut-off score of 17 was established, with 95.83% sensitivity and 80% specificity.
Conclusion:
The EARS-Kn version showed strong validity and reliability among Kannada-speaking HNC survivors, indicating its potential to enhance the understanding of exercise adherence among them. Future studies could explore the EARS-Kn version among diverse populations prescribed various rehabilitation regimes. Studies could also further investigate psychometric properties of the EARS in different Indian languages among cancer survivors, which would help improve survivorship outcomes.
Keywords
Introduction
The International Agency for Research on Cancer (IARC) latest update suggests that globally, 35 million new cancer cases are predicted by the year 2050, with a 77% rise from the estimated number of 20 million cases in 2022. 1 It is projected that 2.98 million Indians will be affected by cancer by 2025, up from 2.67 million in 2021. 2 The spectrum of the disease varies across regions owing to diverse lifestyles. 2 Head and neck cancers (HNC) encompass a wide range of malignancies for example, larynx, pharynx, oral cavity, paranasal and nasal cavity. 3 In India, the burden of HNC is estimated to rise by 57.7% by 2040, with over 2.1 million new cases as compared to 2020.4,5
Improvement in medical and surgical techniques has led to longer survival rates among cancer survivors.6,7 This in turn highlights the importance of improved quality of life and fewer side effects from the disease as well as its associated treatments. 8 Various studies in the past have regarded exercise as a promising intervention pre-, during, and after treatment of cancer to help decrease symptom burden and improve quality of life.9 -12 In addition to providing numerous benefits for cancer survivors in terms of supportive care, exercise has also been suggested as a potential cancer treatment in light of recent preclinical, observational and clinical research.13,14 A recent pilot RCT concluded that a combined aerobic, resistance and flexibility regimen improved physical fitness, quality of life and body composition in HNC survivors undergoing chemotherapy. 15
In the context of exercise-based rehabilitation, adherence is “the extent to which individuals undertake a prescribed adherence behavior accurately and at the agreed frequency, intensity and duration.”16,17 Adherence is a multifaceted and complex phenomenon that can be influenced by various factors namely, personal, therapy-related, provider-related, and healthsystem-related. 18 Studies in the past have explored various measures to assess exercise adherence among cancer survivors. Widely used methods include self-reported questionnaires, objective methods such as accelerometers or pedometers to measure physical activity levels and behavioral assessments focusing on psychological factors influencing exercise.19 -21 In addition, another widely used approach among cancer survivors was meeting the exercise and physical activity guidelines, attending exercise sessions, and adhering to prescribed exercise.22 -24
According to recent systematic reviews, developing strategies to promote exercise adherence is a key area for future research, emphasizing the need for established and reliable measures to assess adherence to exercise programs.25,26 Addressing this gap in the literature, Newman-Beinart et al 27 developed the Exercise Adherence Rating Scale (EARS) in 2017 as a patient-reported outcome measure (PROM) to evaluate the exercise adherence among patients with chronic low back pain in the UK. The original version of the EARS tool is a self-reported 16-item questionnaire, comprising 3 sections. The first section—section “A” is a five-item scale wherein participants qualitatively explain their adherence behavior. The second section, that is, section “B” consists of six items, is an actual measure of exercise adherence, and is used to measure adherence behavior. 27 Furthermore, the third section—section “C” is a 10-item scale describing the reasons for adherence/non-adherence to exercise. 27
The cross-cultural adaptation of the EARS tool has been conducted in several populations across the globe.28 -31 The cancer burden in India is substantial, ranking amongst the highest in Asia, and it is projected to continue increasing in the forthcoming years.32,33 The regional variation within India also highlights the need for targeted interventions including supportive care regimes across the country. It is of utmost importance to translate and cross-culturally adapt patient-reported outcome measures (PROM) to the country and language in which they are intended for use, 34 in order to help improve survivorship outcomes. To the best of our knowledge, there is a paucity of validated scales or gold standard tools for assessing exercise adherence in the Indian languages. Self-reported diaries or log books are commonly used to measure exercise adherence in India—methods that lack accuracy and standardization, hence limiting their validity and reliability in reporting the outcomes. 29 Therefore, the objectives of the present study were to cross-culturally adapt and translate the original English version of the EARS to Kannada, and to investigate its reliability and validity in patients with HNC in a tertiary care hospital in India.
Materials and Methods
The permission for cross-culturally adapting the EARS tool was obtained from the developer. Written informed consent was obtained from all the Head and Neck cancer survivors prior to data collection. Ethical approval was obtained from the Institution Ethics Committee, Kasturba Medical College, Mangalore to conduct the study on 17/05/2023, Protocol No: IEC KMC MLR 05/2023/205.
Cross-Cultural Adaptation
The present study employed the Beaton Guidelines, a widely-used guideline for cross-cultural adaptation of measurement tools, based on the recommendation of Dr. Emma Godfrey, the original developer of the tool. 35 In addition, we adhered to the “evidence for cross cultural adaptation” followed by Takasaki et al, 36 to cross culturally adapt the original EARS tool to Kannada language. According to the Beaton guidelines, there are five steps to effectively cross culturally adapt a tool; (a) forward translation, (b) synthesis, (c) backward translation, (d) expert committee review, and (e) pre-testing of the tool. The five steps followed in the present study are described in Figure 1.35,37
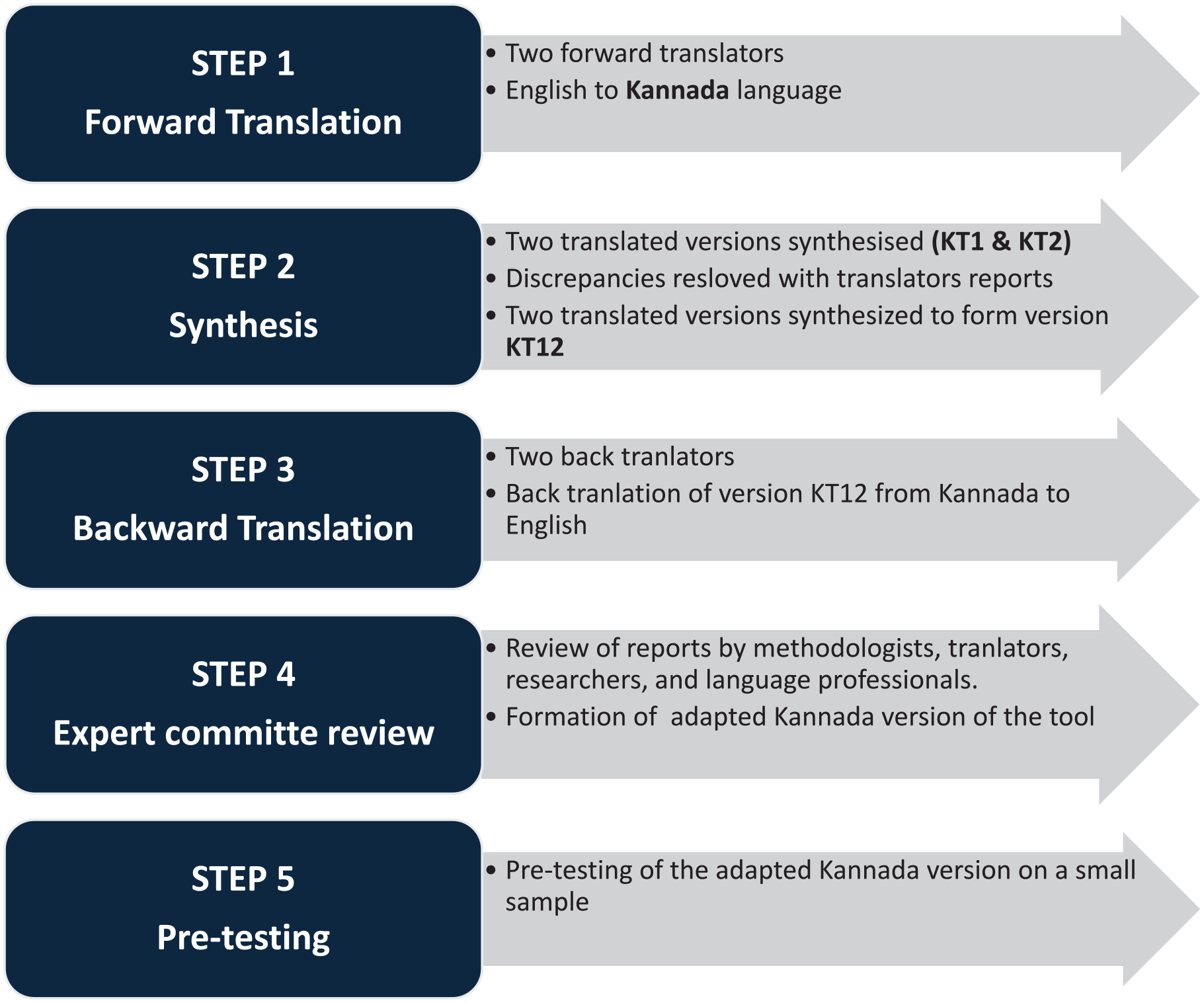
The process of cross-cultural adaptation based on the Beaton guidelines.
The original version of the EARS tool was translated into Kannada version by two separate non-medical translators who were proficient in both languages, and two forward translated versions were created (KT1 and KT2). A formal meeting was conducted by the authors of the present study with the two translators to resolve minor discrepancies in the translated versions. After an agreement within the team, the final version of the forward translation (KT12) was developed. Furthermore, it was requested of two bilingual physical therapists (English and Kannada) to back translate version KT12 to English. This process ensured that components of the adapted version were similar to the original English version. Thus, the back translated version was reviewed and developed.35,36 (The synthesized versions, KT12, and its back—translation to English are available in the Supplementary files section.)
Eleven head and neck (HNC) survivors from a tertiary care hospital in Mangalore, (Dakshina Kanada district) Karnataka participated in the tool’s pre-testing. These survivors were not part of the validity and reliability testing. On a visual analog scale (VAS) of 1 to 10, the survivors were asked to rate their responses; a score of more than 8 indicated that the KT12 version was understandable and easily comprehended. 29 Hence the KT12 version was considered as the final version of the EARS—Kannada version with no modifications to the original English version. The EARS-Kn version was mailed to the original developer and a positive response was received for the same.
Validation of EARS-Kn
Head and neck cancer survivors Stages III and IV (not recruited for pre-testing), who were fluent in Kannada were screened for inclusion. Survivors were considered eligible if they satisfied the following inclusion criteria: (1) Histologically proven diagnosis of HNC Stages III and IV (IVa and IVb), (b) an Eastern Co-operative Oncology Group (ECOG) score ranging from 0 to 2, (c) Patients aged above 18 years, (c) clearance from the attending medical or radiation oncologists to participate in the exercise program, (d) completed the course of definitive CRT without severe adverse events, (e) completed the in-patient hospital stay and participated in the Multimodal Oncology Rehabilitation Exercise (MORE©) Program during the same, (f) patients who were called for follow-up post 3 months of discharge.
Procedure
HNC survivors were screened at KMC Hospital, Attavara, Mangalore, India from June 2023 to May 2024. Written informed consents were obtained during the in-patient stay as well as during the follow-up visits. Demographic and clinical characteristics of the participants were collected, and they were asked to fill out the EARS-Kn tool during the follow-up visit. The patients were instructed by the attending physical therapist to remember their exercise performance from the day of discharge to the day of follow-up (3rd month) and the reasons for adherence or non-adherence. The tailored MORE© program consisted of exercises addressing the physical (upper extremity, lower extremity, mouth opening exercises), cognitive motor activities (printed puzzles, mazes etc.) and relaxation exercises (breathing and progressive relaxation activities). The survivors were instructed to perform the exercises three times/week for 45 to 60 min/day. The participants with native tongue other than Kannada language were purposely excluded from the study to increase the reliability of the findings in the Kannada—speaking populations.
Statistical Analysis
Mean and standard deviations; counts and percentages were calculated for continuous and categorical variables respectively, to describe the demographic and clinical characteristics of the HNC survivors. Reliability of the tool was calculated using Cronbach’s alpha (α) to establish internal consistency. The receiver operating curve was plotted to illustrate the sensitivity and specificity, and to determine the cut-off score of the EARS-Kn version. To determine the validity (construct) of the study findings we performed exploratory factor analysis (EFA) using varimax rotation. In addition, to determine the number of factors to be retained and assess the relative importance of each and determine factor loadings, eigenvalues were calculated. The Bartlett’s test was used to determine sampling sphericity and the Kaiser-Meyer-Olkin’s (KMO) test was performed to determine sampling adequacy. A minimum KMO value of 0.60 indicates sampling adequacy. 38 The Jamovi version 2.3.28 was used to perform the data analysis. 39 A P-value of <.05 was indicative of statistical significance.
Results
Thirty-four HNC survivors were recruited for the current study. The mean age of the survivors was 53.3 years ± 10.7 years. A majority of the survivors were males (n = 25, 73.5%). In addition, the survivors presented with Stages III and IV of HNC, with 61.8% (n = 21) of survivors, presenting with Stage IV of the disease. In regards to the diagnosis, the survivors presented with varied tumor sites namely; (a) carcinoma oral cavity (tongue = 23.5%, buccal mucosa = 35.3%, and retromolar trigone = 6%), (b) carcinoma pharynx (oropharynx = 8.8%, nasopharynx = 2.9% and hypopharynx = 11.8%), (c) carcinoma larynx (supraglottic = 5.9%), carcinoma nasal cavity and paranasal sinuses (maxillary sinus = 2.9%), (d) carcinoma of salivary glands (submandibular gland = 2.9%).40 -42
As illustrated in Table 1, mean scores for the six-item Exercise Adherence Rating Scale (EARS) ranged from 2.67 to 2.97. The score for item—8 was the least (2.00 ± 1.61). All the survivors were prescribed a tailored MORE© program and were provided with instructions prior to discharge at the 8th week.
Demographic, Clinical Characteristics and Exercise Profile of HNC Survivors (N = 34).

Test of Reliability
As depicted in Table 2, the Cronbach’s α value was .93 for adherence behavior. The Cronbach’s α value for item rest correlation ranged from .72 to .86. In case of item deletion, the Cronbach’s α ranged from .90 to .92. To prevent lower Cronbach’s α values, it is essential to retain all items.
Determination of Internal Consistency of EARS-Kn (N = 34).

Test of Validity
The exploratory factor analysis (EFA) was used to explore the construct validity of the six-item EARS-Kn version. The Bartlett’s test for sphericity had values as follows: Chi square: 163, P < .001. The KMO value for the six-item adherence behavior was 0.85, this value exceeded the required value of 0.60, which ensures excellent sampling adequacy. Thus, the criteria necessary for sampling adequacy and sphericity were achieved for the EARS-Kn version. The EFA for the six-item EARS-Kn version, revealed one factor solution, with eigenvalues exceeding one (Table 3). The scree-plot revealed an extraction of only one factor, with a loading of 70.1%.
The Exploratory Factor Analysis of the 6-Item EARS-Kn (N = 34).

The area under the curve (AUC)—ROC, for the six-item adherence scale as depicted in Figure 2, was 0.908 with 95% CI 0.79 to 1.00 at P < .001. A cut-point of 17 was achieved with 95.83% sensitivity, 80% specificity and a Youden’s index of 0.75, which is consistent with previous studies.29,30

Receiver operating characteristic (ROC) curve of six-items—adherence behavior scale (EARS-Kn version).
Correlation
The Pearsons correlation was conducted between the six-item adherence behavior scale and the 10-item reasons for adherence/non-adherence scale of the EARS-Kn version. This method was performed as a means of further validating the EARS-Kn version. As shown in Table 4. The six-item scale demonstrated significant correlations with the following items of the 10-item scale namely, item 1 (PC: .5, P < .001), item 2 (PC: .5, P < .001), item 3 (PC: .3, P = .02), item 4 (PC: .4, P = .004), item 6 (PC: .3, P = .02), item 9 (PC: .3, P = .03), item 10 (PC: .5, P = .001). However, no significant correlations were found between items 5, item 7 and item 8 of the 10 item reasons for adherence/non-adherence scale.
Correlation Between 6-Item and 10-Item EARS-Kn.

The Pearsons correlation (PC) analysis was performed to between individual items of the 10-item and 6-item scale Pearsons coefficient.
P < .05, **P < .01, and ***P < .001 are indicative of levels of significance.
Discussion
Evidence has shown the importance of exercise as an adjunctive treatment across the spectrum of the disease (cancer) which helps improve various physical and psychological outcomes, in turn improving quality of life (QOL). 43 Exercise has been proven to alleviate various side effects associated with anti-cancer therapies; fatigue, lymphedema, and sleep disturbances, while also promoting psychological well-being and improved QOL. Exercise interventions among HNC survivors have emerged as a promising and well-supported approach to support the holistic recovery of cancer survivors.14,43,44 The findings from literature in the past decade underscore the importance of incorporating exercise as an integral part of comprehensive cancer care and survivorship programs. The MORE© program, which was undertaken by participants as a home-based exercise intervention in the present study, included exercise with potential benefits spanning across the cognitive, physical, and psychosocial domains.
To the best of our knowledge, this is the first study undertaken among HNC survivors exploring exercise adherence using the EARS tool to assess a tailored home-based exercise program. In the present study, the original version of the EARS was cross culturally adapted to the Kannada language (spoken widely in the South Indian state of Karnataka). The EARS-Kn version demonstrated excellent internal consistency and good construct validity. The survivors in the study were a diverse group of HNC survivors, with various subsites and stages of the disease. Since all the participants in the study were fluent in Kannada, the process of cross-cultural adaptation proved to be both robust and effective.
The process of cross-cultural adaptation in the current study was based on the Beaton guidelines. 35 The translation process, which constituted forward and backward translation, did not reveal concerns related to content or language. During the pre-testing phase, which was conducted among 11 HNC survivors, the participants stated that the questions were clear and easily understood, requiring no modifications to its items. Most of the survivors had no difficulty in comprehending the questions in all three sections. As opposed to the findings by Meade et al, 45 wherein challenges were encountered while answering questions related to dosage of the prescribed exercise, the survivors did not report any concerns related to dosage and type of exercise to be performed. This can be attributed to the tailored MORE© program catered to the HNC survivors wherein, specifications regarding the frequency, time and type of exercises to be performed were clearly explained by the concerned physical therapist at the time of discharge. In addition, weekly telephone calls were made to the survivors regarding the progress of the program and rectifications related for the difficulties faced.
Assessment of Reliability and Validity
The reliability and validity analysis of the EARS-Kn demonstrated acceptable scores. We calculated the Cronbach’s α for assessment of internal consistency of the six-item adherence behavior scale. This method helps measure the degree of inter-relatedness among the items of the scale. 46 Higher α values are indicative of higher internal consistency.46,47 The internal consistency of the EARS-Kn version was found to be excellent, with an α value of .93 for the six-item adherence behavior scale. These scores are comparable with the internal consistency of the original English version (.8), Brazilian version (.88), and the Nepalese version (.94). Furthermore, the authors of the Japanese version conducted the Rasch analysis of the EARS tool, wherein the internal consistency, that is, Cronbach’s α value was estimated to be .81.27 -30
The EARS-Kn version had a higher alpha value of .93, which suggests that the items are highly inter-related and measurement of exercise adherence is effective, which is consistent with the findings of the Nepalese version of the tool. 29 With respect to the measurement of the internal consistency of the 10-item (reasons for adherence/non-adherence), the internal consistency was not determined in the original English version, the Brazilian-Portuguese version, and the Nepalese version either.27,29,30 In summary the internal consistency of 10-item scale was not assessed due to the inability to sum up the total score, based on the recommendations by the authors of the original EARS tool for reasons for adherence/non-adherence.
The findings of the current study support the structural validity of the six-item adherence scale, with a one factor solution, underlining a total of 70.1% of the variance using the Exploratory Factor Analysis (EFA), which is quite similar to the original English version (71% factor loading). 27 The AUC of the six-item scale was 0.98, demonstrating statistical significance as suggested by previous evidence.29,48 A cut-off score of 17 was obtained, with 95.83% sensitivity and 80% specificity, for the six-item scale, indicating patients with scores >17 of 24 were adherent to the exercises prescribed through the MORE© program. The Brazilian and Nepalese version demonstrated cutoff scores of 17 and 17.5 respectively, which is consistent with our study findings.29,30 The cutoff scores were not established by the authors of the original version, however, as they suggested it is crucial to carefully determine the cut-off scores of the scale by understanding the level of exercise required for a particular exercise regimen to be effective for the intended population. 27 The authors of the original version reported a sensitivity of 87.2% and specificity of 76.3% among patients with chronic low back pain, which is comparable with the findings of the present study.
In terms of correlation, various studies in the past have described the validity of the patient related outcome measures (PROMs) by emphasizing on the strength of correlation between the said items of the scale.45,49 The six-item scale demonstrated strong correlations items 1, 2, 3, 4, 6, 9, and 10 of the 10-item scale (reasons for adherence/non-adherence). The original English version demonstrated correlation between items 1, 2, 3, 4, 7, and 9. 27 These results provide substantial reasons for adherence and non-adherence to the exercise regimen; however, this may vary among patients based on the diagnosis, stage of the disease and other clinical as well demographic characteristics.
Strength and Limitations
The cross-cultural adaptation was carried out based on an established guidelines that enhances its methodological quality. The study is the first to explore exercise adherence using the EARS tool in a tailored home based-exercise program (MORE© program) among HNC survivors using an adapted version. The program demonstrated excellent internal consistency and good construct validity along with strong correlations among a heterogenous group of HNC survivors with varied diagnosis (site and stage). However, this study is not without its limitations, the survivors in the study were asked to recall their previous exercise performance during the follow-up period which could have led to a potential recall bias in the final scores. Additionally, study was conducted among HNC survivors in a specific region of India, which may limit its generalizability to other populations or regions. Furthermore, a majority of the participants in the study were literate, however most of the survivors admitted in our tertiary care set-up were illiterate, hence as suggested by Adhikari et al, 29 an oral version of the EARS-Kn version could be beneficial.
Conclusion
The EARS-Kn version demonstrated replicable psychometric properties, which can be compared to the original (English) version of the tool. A cut-off score of 17 was achieved with excellent sensitivity and specificity. Future studies could conduct longitudinal evaluations to assess long term adherence of tailored home-based exercise interventions among various histological forms of cancer. In addition, studies can focus on the cross culturally adapting the EARS tool among various languages spoken by diverse populations in India to enhance inclusivity and accessibility, and in turn help improve patient outcomes.
Supplemental Material
sj-docx-1-ict-10.1177_15347354251313534 – Supplemental material for Translation, Cross-Cultural Adaptation, and Validation of the Kannada Version of the Exercise Adherence Rating Scale (EARS-Kn) Among Head and Neck Cancer (HNC) Survivors in a Tertiary Care Setup in India
Supplemental material, sj-docx-1-ict-10.1177_15347354251313534 for Translation, Cross-Cultural Adaptation, and Validation of the Kannada Version of the Exercise Adherence Rating Scale (EARS-Kn) Among Head and Neck Cancer (HNC) Survivors in a Tertiary Care Setup in India by Hritika D. Pai, K Vijaya Kumar, Prasanna Mithra, Stephen Rajan Samuel, Mariappan Senthiappan Athiyamaan and Emma Louise Godfrey in Integrative Cancer Therapies
Footnotes
Acknowledgements
(1) Kasturba Medical College Mangalore, Manipal Academy of Higher Education. (2) The Multimodal Oncology Rehabilitation Exercise (MORE©) Program has been granted the Copyright by the Copyright Office Government of India on 08/01/2024.
Author Contributions
Hritika D. Pai, K Vijaya Kumar, Prasanna Mithra, and Emma Louise Godfrey conceived the idea, analyzed the data, prepared figures and/or tables, authored or reviewed drafts of the article, and approved the final draft. Stephen Rajan Samuel and Mariappan Senthiappan Athiyamaan authored or reviewed drafts of the article, and approved the final draft.
Data Availability Statement
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Considerations
This study was approved by the Institutional Ethics Committee, Kasturba Medical College, Mangalore (Protocol IEC KMC MLR 05/2023/205). This research was conducted ethically in accordance with the World Medical Association Declaration of Helsinki.
Consent to Participate
This study was approved by the Institutional Ethics Committee, Kasturba Medical College, Mangalore (Protocol IEC KMC MLR 05/2023/205). All participants provided written informed consent prior to participating.
Consent to Publisher
Stephen Rajan Samuel is an Associate Editor for Integrative Cancer Therapies, but did not take part in the review or decision processes for this manuscript.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.