
Abstract
Purpose:
Preoperative chemotherapy in borderline resectable pancreatic cancer (BRPC) reduces tumor size to enable surgery but may cause physical function decline. This study aimed to examine changes in physical function before and after preoperative chemotherapy in patients with BRPC, and explored factors associated with the change.
Methods:
This retrospective study included 17 patients with BRPC who underwent preoperative chemotherapy and surgery between January 2020 and December 2021. Physical function was assessed using grip strength and the 6-minute walking test (6MWT). Patients were divided into 2 groups based on changes in physical function: (1) those with maintained physical function and (2) those with reduced physical function. Physical function, treatment duration, and the number of chemotherapy sessions were compared between the groups.
Results:
Grip strength (24.7 ± 6.8 vs 25.1 ± 6.8 kg, P = .462) and 6MWT (451.8 ± 95.7 vs 470.0 ± 82.5 m, P = .119) showed no significant decline after chemotherapy. On subgroup analysis, the reduced physical function group (6 patients) had significantly more chemotherapy sessions than the maintained group (5.0 ± 2.0 vs 2.0 ± 0.6, P = .042), suggesting that prolonged chemotherapy regimens may increase physical function decline risk due to cumulative toxicity.
Conclusion:
These findings underscore the need for individualized treatment planning, balancing tumor reduction benefits with physical decline risk, especially in frail patients.
Introduction
Pancreatic cancer is a disease with a markedly poor prognosis, and has been reported as a leading cause of cancer-related mortality in Western countries. 1 The 5-year survival rate for pancreatic cancer patients is approximately 12%, the lowest among gastrointestinal cancers. 2 One of the primary reasons for this poor prognosis is the lack of distinct early symptoms, often leading to advanced metastasis by the time of diagnosis. Consequently, only a limited number of cases are eligible for surgical resection. Resectability is frequently determined based on imaging findings, and cases are classified into resectable pancreatic cancer, borderline resectable pancreatic cancer (BRPC), and unresectable pancreatic cancer. BRPC is characterized by tumors adjacent to major blood vessels, encasing portions of the superior mesenteric or portal vein. This increases the risk of positive surgical margins if surgery is attempted without additional intervention.
Chemotherapy is essential for the treatment of BRPC, as it shrinks tumors and makes them operable. Therefore, neoadjuvant therapy is often performed to mitigate the risk of positive surgical margins. 3 Recently, preoperative chemotherapy has demonstrated promising results in BRPC cases by achieving tumor reduction, suppressing disease progression, enhancing surgical rates, and improving patient outcomes.4,5 Thus, this approach has garnered attention as a valuable treatment strategy to increase resectability and prolong survival in patients with BRPC.
Neoadjuvant chemotherapy for patients with BRPC is associated with concerns regarding the significant physical burden imposed by the side effects of chemotherapeutic agents. In particular, agents such as FOLFIRINOX, gemcitabine, and nab-PTX are known to cause frequent adverse events, 6 including organ toxicity, such as hepatotoxicity, as well as cytotoxic effects, such as thrombocytopenia and neutropenia, affecting both cellular and organ function.7,8 Consequently, these events might lead to reduced physical function and the emergence of various physical symptoms. A study on patients with esophageal cancer reported that preoperative chemotherapy led to a deterioration in general condition and immunity, resulting in decreased postoperative survival rates. 9 Furthermore, side effects of preoperative chemotherapy, such as vomiting and weight loss, were identified in patients with pharyngeal cancer. 10 The decline in physical function significantly impairs quality of life (QOL) after treatment and may also negatively affect surgical outcomes and postoperative recovery. 11 Additionally, older adults or physically weakened patients with reduced preoperative physical function are reported to have an increased risk of postoperative complications. 12 Therefore, support or interventions aimed at maintaining or improving physical function may be beneficial for patients with cancer undergoing preoperative chemotherapy. Previous studies have shown that exercise interventions during chemotherapy in cancer patients can improve exercise tolerance and muscle strength. 13 This highlights the necessity of monitoring these physical functions during chemotherapy. However, the factors associated with a decline in physical function after chemotherapy for BRPC remain unclear.
In this study, we retrospectively investigated changes in physical function before and after preoperative chemotherapy in patients with BRPC using data from a clinical database. Furthermore, we aimed to identify differences in clinical variables between 2 groups: (1) patients with decreased physical function and (2) those with maintained physical function after preoperative chemotherapy.
Methods
This study used a retrospective cohort design. The participants were 17 patients diagnosed with borderline resectable pancreatic cancer (BRPC) between January 1, 2020, and December 31, 2021, who underwent preoperative chemotherapy in conjunction with surgical resection. All data were retrospectively extracted from the hospital’s electronic database.
Resectability was determined based on the “7th Edition of the General Rules for the Study of Pancreatic Cancer” in Japan. Cases meeting any of the following criteria on CT imaging were classified as BRPC 14 :
Tumors showing no contact or invasion of the superior mesenteric artery, celiac artery, or common hepatic artery but with ≥180° contact or invasion, or obstruction, of the superior mesenteric vein or portal vein, confined within the lower border of the duodenum.
Tumors with ≥180° contact or invasion of the superior mesenteric or celiac artery, without stenosis or deformation.
Tumors with contact or invasion of the common hepatic artery without involving the proper hepatic artery or celiac artery.
All participants received one of the following regimens as preoperative chemotherapy before surgical resection: gemcitabine (GEM) therapy, modified FOLFIRINOX (mFOLFIRINOX) therapy, GS therapy (GEM combined with S-1), or GAS therapy (GEM combined with nab-paclitaxel and S-1). Basic demographic and clinical information, including gender, age, height, weight, body mass index (BMI), treatment duration, number of chemotherapy sessions, and postoperative hospital stay duration, were collected for each participant.
This study was approved by the Ethics Committee for Epidemiological Research at Hiroshima University (Approval No: E2017-0808) and was conducted according to established ethical standards consistent with the current Declaration of Helsinki. Informed consent was obtained from all participants before their inclusion in the study. During the course of chemotherapy, no specific nutritional or exercise interventions were implemented. Instead, appropriate nutritional management and regular monitoring were conducted by the attending physicians as part of routine clinical care. Additionally, physical therapists provided basic exercise guidance, including daily walking and lower limb muscle-strengthening exercises.
Physical Function Assessment
Physical function was assessed using grip strength and the 6-minute walking test (6 MWT). The 6-minute walk test is used to evaluate aerobic capacity, endurance, and functional mobility. 15 Grip strength, which directly assesses muscle strength, is an indicator reflecting overall muscle strength. 16 Clinical implementation of these tests for cancer patients has demonstrated sufficient validity and reliability.17,18 These measures are commonly used in clinical settings and are key indicators closely associated with the comprehensive geriatric assessment. This assessment evaluates activities of daily living, mental and psychological function, socio-economic function, and overall QOL. 19 The data were collected by 2 experienced physical therapists who routinely conduct strength assessments in clinical practice. Both physical therapists had over 5 years of clinical experience and were proficient in strength measurement techniques, with specific training on the use of handgrip dynamometers for reliable data collection. To minimize error, a standardized protocol was followed, including calibration of the dynamometer before each session and consistent measurement instructions provided to participants.
Grip strength was measured using a digital handgrip dynamometer in a standing position, with the arm at the side and the elbow slightly flexed, following the protocol used in the Japanese “New Physical Fitness Test.” 20 Although international guidelines recommend measurement in a seated position with the elbow flexed at 90°, forearm in mid-prone, and wrist in neutral, 21 the standing posture was adopted in this study to reflect common practice in Japan, and to elicit maximum muscle exertion in the target population. The 6MWT was conducted following the American Thoracic Society statement, with the distance covered during 6 minutes recorded (walking aids were permitted). Measurements were conducted both before and after preoperative chemotherapy.
Statistical Analysis
All statistical analyses were conducted using SPSS software for Mac ver 29.0 (IBM Corp., Armonk, NY, USA). Patients were divided into 2 groups: a “maintained physical function group” and a “reduced physical function group,” based on changes in grip strength and 6 MWT after preoperative chemotherapy. Groups were characterized as follows: a “reduced physical function group” (patients with declines in both measures) and a “maintained physical function group” (patients who showed either no decline in both measures or improvement in at least 1 measure). Mann–Whitney U tests were used to compare the maintained and reduced physical function groups. Comparisons before and after chemotherapy were performed using paired Wilcoxon signed-rank tests. A significance level of 5% was set for all analyses.
Results
Basic Information of Participants
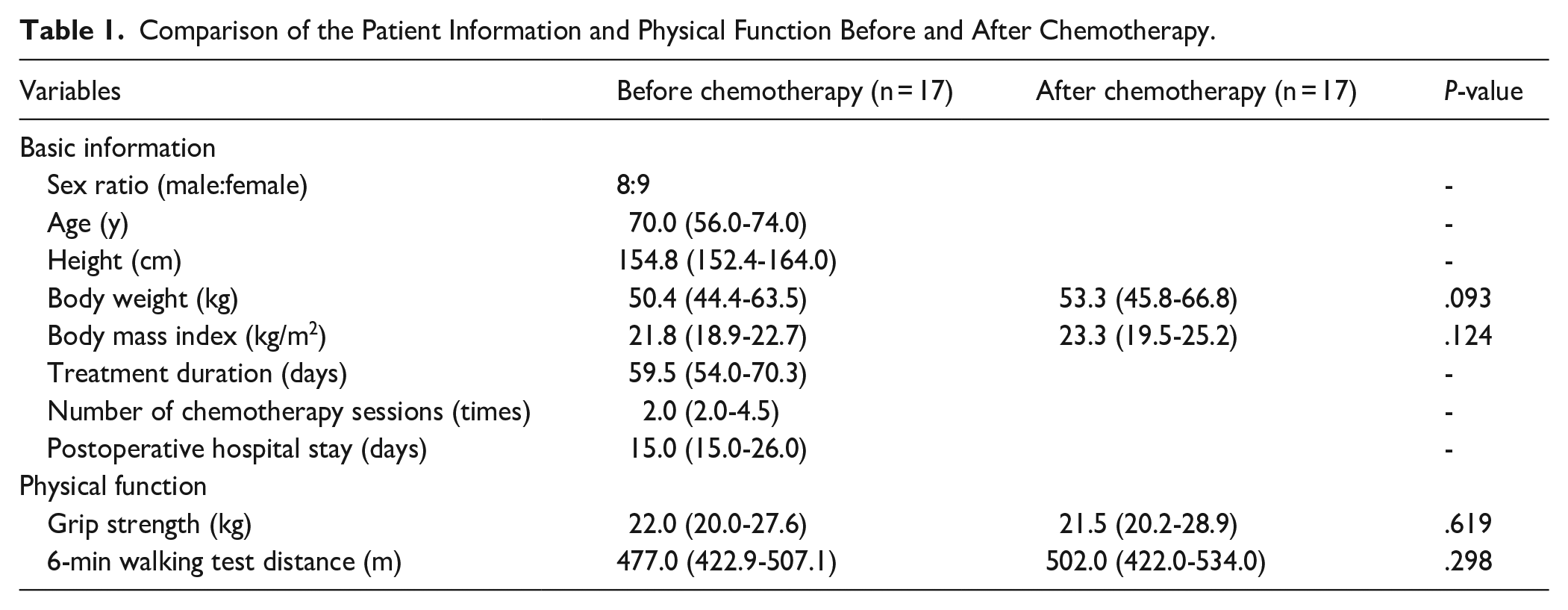
Table 1 presents the patients’ basic information. Data were obtained from 17 patients (8 males and 9 females). The basic demographic information for this group (median [interquartile range]) included age (70.0 [56.0-74.0] years), height (154.8 [152.4-164.0] cm), weight (pre-chemotherapy: 50.4 [44.4-63.5] kg, post-chemotherapy: 53.3 [45.8-66.8] kg), and BMI (pre-chemotherapy: 21.8 [18.9-22.7] kg/m², post-chemotherapy: 22.3 [19.5-25.2] kg/m²). The median treatment duration was 59.5 (54.0-70.3) days; the median number of chemotherapy sessions was 2.0 (2.0-4.5); and the median postoperative hospital stay was 15.0 (15.0-26.0) days. No significant differences in weight or BMI were observed before and after chemotherapy (P = .093; P = .124).
Comparison of the Patient Information and Physical Function Before and After Chemotherapy.
Comparison of Physical Function Before and After Chemotherapy
No significant changes in grip strength were observed before and after chemotherapy (22.0 [20.0-27.6] vs 21.5 [20.2-28.9] kg, P = .619, Table 1). Similarly, no significant differences were observed in the 6MWT before and after chemotherapy (477.0 [422.9-507.1] vs 502.0 [422.0-534.0] m, P = .298; Table 1).
Comparison Between Maintained Physical Function Group and Reduced Physical Function Group
The grouping results indicated that 11 patients were in the maintained physical function group, while 6 were in the reduced physical function group (Table 2). The maintained physical function group attended fewer chemotherapy sessions (2.0 [2.0-2.0], P = .042; Figure 1). No significant changes in grip strength were observed between the 2 groups after chemotherapy (21.5 [20.4-28.5] vs 24.0 [19.9-34.6] kg, P = 1.000; Table 2). Additionally, no significant differences were observed in the 6MWT between the 2 groups after chemotherapy (507.8 [419.1-525.0] vs 458.4 [430.3-530.9] m, P = .884; Table 2).
Comparison of the Physical Function Between the “Maintained Physical Function Group” and the “Reduced Physical Function Group” After Chemotherapy.


Comparison of the number of chemotherapy sessions between the maintained physical function group and reduced physical function group.
Similarly, no significant differences were observed between the groups regarding treatment duration (58.0 [52.0-63.0] vs 81.5 (61.3-96.5) days, P = .073; Table 2) or length of hospital stay (15.0 [15.0-23.5] vs 18.5 [15.0-25.8] days, P = .733; Table 2).
Discussion
In this study, we examined the impact of preoperative chemotherapy on physical function and identified factors associated with changes in physical function in patients with BRPC. The main finding was the significant difference in the number of chemotherapy sessions between the maintained physical function group and the reduced physical function group.
Physical function was lower in participants who underwent a greater number of chemotherapy sessions, based on median comparisons. This finding emphasizes that, although increasing the number of preoperative chemotherapy sessions can enhance treatment efficacy by reducing tumor size and prolonging treatment, it also increases the risk of cumulative adverse effects. Chemotherapy is known to cause systemic side effects such as fatigue, loss of appetite, muscle weakness, and weight loss due to the cumulative toxicity of anticancer drugs.22,23 These side effects are exacerbated over multiple cycles, increasing the risk of declining physical function.
Furthermore, frail older patients with cancer undergoing preoperative chemotherapy have been reported to experience worsened immunity and general health, along with symptoms such as vomiting and weight loss.6,7 This study highlights the potential risks of prolonged chemotherapy in this population. Repeated chemotherapy cycles can lead to decreased physical activity, muscle mass, and muscle quality, resulting in a decline in physical function.24,25
Despite these findings, this study did not observe a significant overall decline in physical function before and after chemotherapy. Several factors could explain this outcome. First, the average age of participants was relatively young (66 years) compared to previous studies that reported worse outcomes in older patients aged 75 years or older.9,26 Younger patients may be more resilient to the side effects of chemotherapy, maintaining their physical function. Second, participants in this study tended to gain weight before and after chemotherapy, which may have contributed to their ability to tolerate treatment. Weight loss, often associated with poor nutritional status, has been identified as a factor reducing tolerance to chemotherapy and survival rates in patients with pancreatic cancer.27,28 The findings of this study underscore the importance of personalized treatment planning for patients with BRPC. Not all patients can tolerate the same number of chemotherapy sessions due to differences in age, nutritional status, underlying diseases, and baseline physical function. Careful consideration of these factors is essential when designing treatment plans to maximize the efficacy of chemotherapy while minimizing adverse effects.22,29 One promising approach is the integration of prehabilitation during preoperative chemotherapy. Prehabilitation includes optimizing exercise, nutrition, and psychological factors before surgery to maintain or improve physical function. This comprehensive strategy can help patients better tolerate chemotherapy and potentially improve surgical outcomes.23,30 Early introduction of prehabilitation may increase the likelihood of completing preoperative chemotherapy and prevent declines in physical function.
Although chemotherapy significantly limits physical activity due to side effects like fatigue and thrombocytopenia-induced bleeding tendencies, it remains essential for BRPC treatment. Preoperative chemotherapy can facilitate successful surgical resection, a critical step in cancer management, by reducing tumor size. Rehabilitation programs aimed at maintaining patients’ physical function and activity levels can enhance their readiness for surgery and optimize treatment outcomes. Furthermore, this study revealed a dose-dependent relationship in which patients with BRPC who underwent a higher number of preoperative chemotherapy sessions experienced a decline in physical function. This emphasizes the need for early prehabilitation interventions to prevent physical function deterioration. Future studies should investigate the optimal timing and intensity of prehabilitation interventions for patients with BRPC to effectively assess their impact on maintaining preoperative physical function.
This study has several limitations. First, although there were no significant differences between the groups in terms of characteristics such as age or the presence of underlying diseases, owing to the small sample size, it cannot be definitively stated that these factors did not affect the results of this study. Additionally, the small sample size limits the generalizability of the study findings. Moreover, only preliminary insights into the effect of preoperative chemotherapy on physical function in patients with BRPC have been provided. Second, there was a lack of data on participants’ daily activities, such as physical activity levels, exercise habits, or prehabilitation engagement. Baseline exercise habits and physical activity levels could influence susceptibility to chemotherapy-related side effects. 31 Last, this study did not analyze the impact of chemotherapy type, treatment duration, individual baseline comorbidities, or nutritional status on physical function decline. Future research should include these factors and recruit larger, more diverse cohorts for validation.
Conclusion
This study aimed to investigate the impact of preoperative chemotherapy on physical function and its associated factors in patients with BRPC. The findings revealed that while overall physical function did not significantly decline during treatment, individual variability existed. Notably, patients in the reduced physical function group underwent significantly more chemotherapy sessions than those in the maintained group. These results suggest the importance of individualized chemotherapy planning that considers both oncologic effectiveness and physical resilience. Incorporating prehabilitation strategies may help maintain physical function and improve treatment outcomes in this population.
Footnotes
Ethical Considerations
This study was approved by the Ethics Committee for Epidemiological Research at Hiroshima University (Approval No: E2017-0808).
Consent to Participate
Informed consent to participate was obtained from all individual participants included in the study.
Consent for Publication
Informed consent for publication was obtained from the participants.
Author Contributions
KK designed the study and wrote the manuscript. YN and SK collected and analyzed the data. AI and TN contributed to the interpretation of the results and revised the manuscript. MA supervised the manuscript preparation. YM supervised the overall study. NM, TA, and YU provided critical supervision of data interpretation. All authors reviewed and approved the final version of the manuscript.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by JSPS KAKENHI Grant Number JP (20K11188).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.