
Abstract
Background. Lung cancer is the most frequently diagnosed cancer and one of the leading causes of cancer deaths. Surgery is the primary approach for curative treatment. Postoperative complications are common, and physiotherapy is often routinely provided for their prevention and treatment, even though the evidence is limited. The aim of this study was to examine the effect of in-hospital physiotherapy on postoperative physical capacity, physical activity, and lung function among patients undergoing lung cancer surgery. Methods. A total of 107 patients undergoing elective thoracic surgery were included in a single-blinded randomized controlled trial, and randomized to a study group, receiving in-hospital physiotherapy treatment, or a control group, not receiving in-hospital physiotherapy treatment. The patients were assessed preoperatively and 3 months after surgery. The in-hospital physiotherapy treatment consisted of early mobilization, ambulation, breathing exercises, and thoracic range of motion exercises. Physical capacity was assessed with the 6-minute walk test. Level of physical activity was objectively assessed with an accelerometer and subjectively assessed with the International Physical Activity Questionnaire Modified for the Elderly. Results. Physical capacity for the whole sample was significantly decreased 3 months postoperatively compared with preoperative values (P = .047). There were no statistically significant differences between the groups regarding physical capacity, physical activity, spirometric values, or dyspnea. However, patients in the study group increased their level of self-reported physical activity from preoperatively to 3 months postoperatively, while the patients in the control group did not. Conclusions. No difference in physical capacity, physical activity, or lung function was found 3 months postoperatively in lung cancer surgery patients receiving in-hospital physiotherapy compared with control patients.
Introduction
Lung cancer is the most frequently diagnosed cancer and one of the leading causes of cancer deaths worldwide. 1 Surgical resection is the primary approach for curative treatment of non–small cell lung cancer. 2 Postoperative complications are common after lung cancer surgery, 3 and patients may experience pain, 4 fatigue,5,6 dyspnea, 6 and impaired lung function. 7 Physical capacity 7 and level of physical activity8-10 are impaired postoperatively, and decreased health-related quality of life7,11 has been reported up to 5 years after surgery.
Patients undergoing lung cancer surgery may have an increased risk of sedentary behavior in the postoperative recovery phase. Physiotherapy is often routinely provided for patients undergoing thoracic surgery during the in-hospital phase with the aim of reducing postoperative complications and improving physical recovery.12-14 The treatment typically consists of early mobilization, shoulder exercises, and breathing exercises. In-hospital physiotherapy treatment after lung cancer surgery is often routinely provided, even though the evidence is limited.15-19 Positive effects have only been shown for a few outcomes such as decreased pain, 15 increased shoulder mobility, 15 and increased quadriceps strength. 17 No significant effects on pulmonary complications16,18 or physical capacity 17 have been reported.
To our knowledge, there are no studies evaluating the effect of in-hospital physiotherapy treatment on postoperative physical activity level after lung cancer surgery, compared with an untreated control group.
The aim of this study was to examine the effect of in-hospital physiotherapy on postoperative physical capacity, physical activity, and lung function 3 months after lung cancer surgery. Our hypothesis was that in-hospital physiotherapy in addition to standard care would have a positive effect on postoperative physical outcomes.
Material and Methods
Patients
All patients undergoing elective thoracic surgery due to suspected or confirmed lung cancer at the Department of Cardiothoracic and Vascular Surgery, Örebro University Hospital, Sweden, between December 2013 and January 2017 were eligible for the study. The patients had to be able to perform the lung function test and walking test, and read and understand Swedish. Patients who had undergone previous thoracic surgery were not included.
Informed written consent was obtained from each patient before inclusion, and the Regional Ethical Review Board in Uppsala, Sweden, approved the study (2013/199). The trial was registered at ClinicalTrials.gov (https://clinicaltrials.gov/show/NCT01961700).
The study was a single-blinded, 1:1 parallel-group, randomized controlled trial. Information about the study was sent by mail to the patients before surgery. A computer-generated randomization list was created by a blinded statistician and administered by a blinded secretary using sequentially numbered, sealed, opaque envelopes. On the day of hospital admission, a study-responsible physiotherapist gave the patients written and oral information about the study and asked them about participation. Patients were randomized after baseline testing, which was performed on the day of admission. The allocation envelope was opened by a physiotherapist responsible for patient care at the ward.
Thoracic surgery was performed by either video-assisted thoracoscopic surgery or open anterolateral muscle-sparing thoracotomy, according to the surgeon’s preference. At the end of surgery, a single chest tube was placed in the pleural space and connected to a suction device (Thopaz Chest Drainage System, or Oasis dry suction water seal drain). A pressure of −15 cm H2O was applied. The chest drainage was removed when there was no air leak and the volume of pleural effusion per day was below 300 to 400 mL. Pain management was primarily delivered by continuous epidural infusion, with ropivacaine and sufentanil. Alternatively, locally placed catheters with ropivacaine were used. As a supplement, the patients received intravenous mor-phine, per-oral nonsteroidal anti-inflammatory drugs, and paracetamol for as long as needed.
Intervention
The study group received pre- and postoperative physiotherapy treatment in addition to standard care during hospital stay while the control group received standard care alone. The physiotherapy intervention was delivered once or twice per day (10-30 minutes per session) on all days except Sundays.
Study Group
Patients in the study group were treated by 1 of 3 physiotherapists at the ward, all of whom were clinically educated to follow the intervention protocol. The physiotherapy intervention was based on the routine treatment provided for patients undergoing cardiothoracic surgery, consisting of early mobilization, breathing exercises, and exercises for thoracic and shoulder range of motion.
Preoperative treatment
The study group received brief (5-10 minutes) individual preoperative physiotherapy information during admission day regarding the importance of postoperative mobilization, including instructions to perform deep breathing exercises every waking hour during the first few postoperative days and explanation of how to cough/huff using the ipsilateral arm and contralateral hand as support for pain relief (“Put your hand and arm over the wound as support when you cough, huff, or sneeze”).
Postoperative treatment
The study group received postoperative physiotherapy treatment once or twice daily during their hospital stay (typically 10-30 minutes per visit) consisting of the following:
Individually adapted early mobilization: sitting up in bed or in a chair on the day of surgery, and then progressive ambulation on the ward from the first postoperative day, with instructions to walk as much as possible during the day, with or without assistance, according to patient needs.
Deep breathing exercises with a positive expiratory pressure (PEP) of 10 cm H2O, performed with the Rium breathing exerciser. If heavy air leakage occurred in the drainage, a responsible surgeon was consulted, who decided if deep breathing exercises with or without PEP were to be applied. A typical instruction was 10 deep breaths with PEP, repeated 3 times with 1-minute rest between sets, performed every waking hour until discharge. The patients were instructed to cough, with support for pain relief, after finishing the breathing exercises.
Exercises for thoracic and shoulder range of motion: shoulder elevation, shoulder flexion while taking a deep breath, horizontal shoulder abduction with hands at the neck while taking a deep breath, and thoracic rotation. Patients were instructed to perform these exercises at least twice daily, with 5 repetitions per exercise each time, from the first postoperative day and during the first postoperative month.
Postoperative information
Prior to discharge, the patients in the study group received advice regarding physical activity. This advice was individually adapted, but was based on the World Health Organization recommendations, 20 which have been adopted in the Swedish national recommendations. 21 These recommendations state that all adults should engage in physical activity, on at least a moderate level, for at least a total of 150 minutes per week. The recommendations also include minimizing prolonged sedentary behavior; persons who spend a lot of time sitting should take short breaks regularly. Patients were instructed that even if they were unable to meet these recommendations, they should be as physically active as possible. They also received individually adapted advice regarding breathing exercises to be performed at home: 10 deep breaths with PEP, repeated 3 times with 1-minute rest between sets, performed 4 to 5 times per day, until they no longer experienced pain when taking deep breaths.
Control Group
The control group received no physiotherapy instructions or specific treatment during the in-hospital phase. Both the control group and the study group received standard care by the nursing staff regarding pain management and general nursing. Standard care for mobility included help with mobilization during activities of daily life, such as sitting out of bed when eating and, if needed, assistance during walking to facilities and dining room. The surgeon responsible for the patient was able to override the study protocol if deemed necessary, in which case a physiotherapist would treat the patient. This was not necessary in any of the cases.
Outcomes
The primary outcome was physical capacity 3 months postoperatively, measured with the 6-minute walk test (6MWT). Secondary outcomes were level of objectively and subjectively measured physical activity, lung function assessed by spirometry, dyspnea, and pain. All measurements were performed by 1 of 3 physiotherapists, blinded to group allocation. Measurements of physical capacity, subjectively measured physical activity, lung function, dyspnea, and pain were performed on day of admission and 3 months postoperatively. Objectively measured physical activity was assessed by accelerometry, during hospital stay and for 1 week at 3 months after surgery.
Physical Capacity
Physical capacity was assessed with the 6MWT. 22 The test was performed in a 25-m corridor, with patients instructed to walk as far as possible in 6 minutes. The output parameter was distance walked. The 6MWT has been shown to be valid and reliable in cancer patients. 23
Subjectively Reported Physical Activity
Self-reported sedentary time and physical activity covering the last week (7 days) were assessed preoperatively and 3 months postoperatively with the International Physical Activity Questionnaire Modified for the Elderly (IPAQ-E). 24 The self-reported data were transformed into metabolic equivalents and categorized into 3 groups of physical activity according to protocol. A description of the criteria for the categories 25 is given in Table 1. The IPAQ has shown reasonable reliability and validity. 26
Categories of Physical Activity According to the International Physical Activity Questionnaire a .

Abbreviation: MET, metabolic equivalent.
Level of self-reported physical activity transformed into categories. (International Physical Activity Questionnaire)
Objectively Measured Physical Activity
Objective measurement of physical activity was performed with the use of an accelerometer (ActiGraph, model GT3X+). The accelerometer measures change in acceleration with regard to time. The output variable is counts per time interval, processed by filtering, and summarizing procedures and presented as counts per time interval “epoch.” This study used a sample frequency of 30 Hz and an epoch of 10. The patients were instructed to wear the device at the waist during their hospital stay after surgery, starting on the morning of the first postoperative day, and during 1 week 3 months after surgery. For the in-hospital physical activity, total counts and steps were summarized for the first 3 postoperative days, and then divided by the hours the patients spent on the ward (some patients were discharged on the third day and did not wear the accelerometer the whole day), thus giving average counts and steps per hour. For the assessment 3 months after surgery, time spent in sedentary, light, or moderate and vigorous physical activity, counts, and steps per day were used to describe physical activity. Limits for minimum wear time were set to 600 minutes/day for at least 2 days. Measuring physical activity with an accelerometer has been reported to give a valid estimate of physical activity. 27
Lung Function
Lung function was assessed using a spirometer (MicroLab ML3500), according to the recommendations of the American Thoracic Society/European Respiratory Society. 28 The test was performed with the patient in a sitting position, wearing a nose clip. Variables assessed were forced vital capacity and forced expiratory volume in 1 second. The best out of 3 results was recorded.
Dyspnea
Perceived dyspnea was measured using the Modified Medical Research Council Dyspnea Scale, 29 on which patients rate dyspnea from 0 (no dyspnea) to 4 (breathless when washing/getting dressed).
Pain
Pain intensity from the thoracic cage and incision was assessed using a numeric rating scale at rest, while taking a deep breath, and when coughing. The scale ranged from 0 (no pain) to 10 (worst imaginable pain).
Statistical Methods
A between-group difference of 60 m in the 6MWT at 3 months after surgery compared with baseline was considered possible and clinically relevant. In a previous study, the standard deviation of the 6MWT 12 weeks after thoracic surgery was 103 m. 17 Applying a .05 level of significance and 80% power yielded a group size of 47 patients per group. To compensate for loss to follow-up, 53 patients per group were recruited.
For patients’ characteristics, continuous data are summarized as mean ± standard deviation or median with the corresponding first quartile (Q1) and third quartile (Q3), and categorical data are presented as numbers and percentages. Between-groups differences were tested with Student’s t test for normally distributed variables, and the Mann-Whitney U test was used for continuous variables with skewed distribution. Between-groups differences in categorical variables were tested using the χ2 test or McNemar’s test. Within-group differences between preoperative and postoperative values were tested with the Wilcoxon signed-rank test.
Missing data were imputed using the multiple imputation method for postoperative 6MWT, pre- and postoperative IPAQ-E, and postoperative accelerometer data. Age, sex, body mass index, length of surgery, duration of drainage, length of stay, and preoperative 6MWT were used as predictors during multiple imputations. Five imputed datasets were used when comparing the variables with missing values, and the average of the statistics or P values was used for statistical inference.
For all analyses, a 2-sided P < .05 was considered statistically significant. All the analyses were performed using IBM SPSS Statistics 25 and Stata 14.2.
Results
A total of 107 patients were included in the study (Figure 1). There were no statistically significant baseline differences between the groups except that the study group had a higher proportion of men (Table 2) and longer time in surgery (Table 3). There were no statistically significant differences between the groups during hospital stay, except for the study group being more physically active (49 [47] vs 37 [34] steps per hour, mean difference [95% confidence interval (CI) = 3 to 30]).

Flow chart of the patients in the study.
Patient Characteristics a .
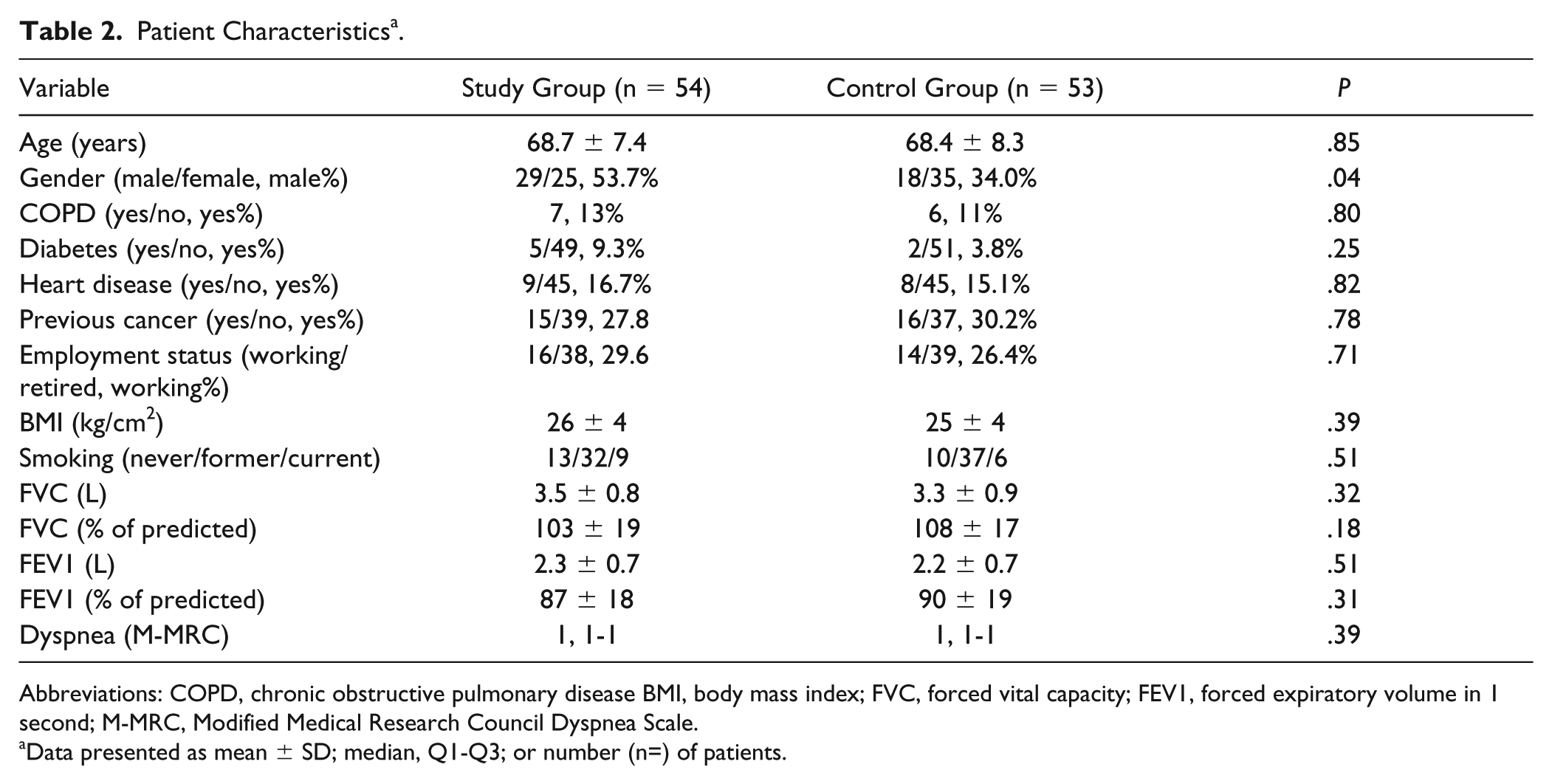
Abbreviations: COPD, chronic obstructive pulmonary disease BMI, body mass index; FVC, forced vital capacity; FEV1, forced expiratory volume in 1 second; M-MRC, Modified Medical Research Council Dyspnea Scale.
Data presented as mean ± SD; median, Q1-Q3; or number (n=) of patients.
Surgical Data a .

Abbreviation: VATS, video-assisted thoracic surgery.
Data presented as mean ± standard deviation; median, Q1-Q3; or number (n) of patients.
Physical capacity for the whole sample, measured with the 6MWT, was normal at baseline: 92% of predicted values according to Enright et al. 30 When comparing the pre- and postoperative 6MWT, there was a statistically significant decrease of 12 m (95% CI = 0.3-23.5, P = .045) for the whole sample 3 months postoperatively. There were no differences in 6MWT between the groups (Table 4). Self-reported physical activity, assessed with IPAQ-E category, did not differ between the groups pre- or postoperatively, but increased in the study group from preoperatively to 3 months after surgery (P = .047), while no difference could be found in the control group (P = .87; Table 5).
Physical Capacity Assessed With the 6MWT Preoperatively and 3 Months Postoperatively a .

Abbreviation: 6MWT, 6-minute walk test.
Data presented as means with corresponding 95% confidence intervals.
Subjectively Reported Physical Activity Assessed With the IPAQ-E Preoperatively and 3 Months Postoperatively a .
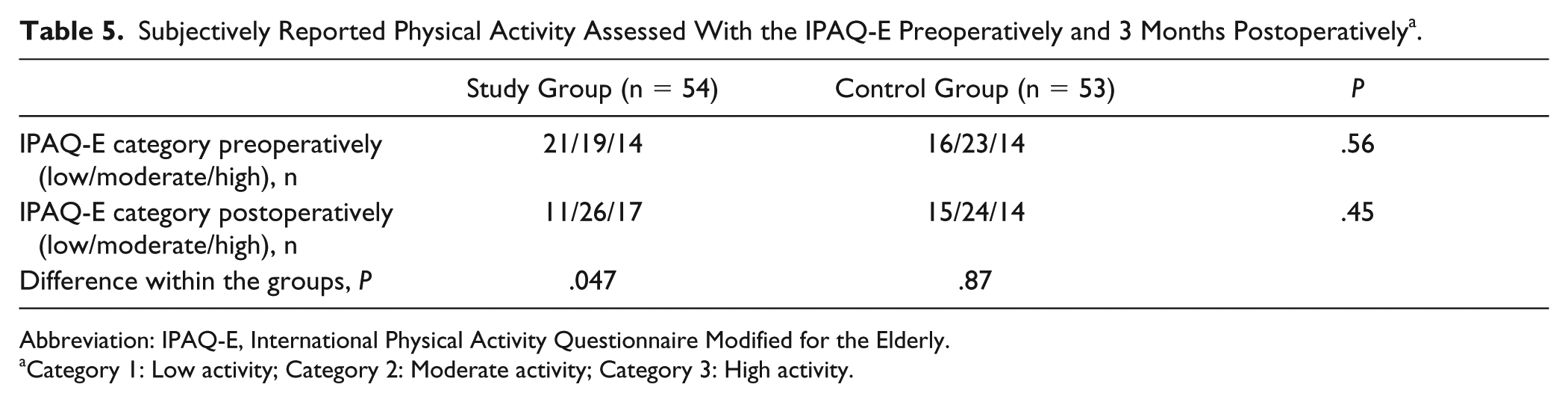
Abbreviation: IPAQ-E, International Physical Activity Questionnaire Modified for the Elderly.
Category 1: Low activity; Category 2: Moderate activity; Category 3: High activity.
Regarding physical activity measured objectively with an accelerometer 3 months after surgery, there were no statistically significant differences between the groups (Table 6).
Physical Activity Measured With Accelerometer 3 Months Postoperatively a .

Abbreviation: MVPA, moderate and vigorous physical activity.
Data presented as means with corresponding 95% confidence intervals.
There were no significant differences between the groups 3 months after surgery in lung function (forced expiratory volume in 1 second = 1.98 ± 0.65 vs 1.97 ± 0.59, P = .92) or dyspnea (Modified Medical Research Council Dyspnea Scale 1 = 1-2 vs 1, 1-2, P = .56).
Pain was low both preoperatively and 3 months postoperatively, with 50% of the patients reporting no pain at rest 3 months after surgery, and there were no statistically significant differences between the groups (pain at rest: 0, 0-2 vs 0, 0-2, P = .49).
In the whole sample, distance walked during the 6MWT was significantly correlated with physical activity measured with an accelerometer 3 months after surgery (steps/day: r = 0.507, P < .001).
No statistically significant correlation was found between objectively measured physical activity during hospital stay and physical activity 3 months after surgery (r = 0.1, P = .42).
Discussion
In this randomized controlled trial, we found no differences in physical capacity, measured with the 6MWT, 3 months after lung cancer surgery between patients receiving physiotherapy during their hospital stay and patients not receiving physiotherapy.
We also found no differences between the groups in objectively measured physical activity, lung function, pain, or dyspnea. However, the patients in the study group reported a significantly increased level of self-reported physical activity 3 months after surgery compared with preoperatively, whereas the patients in the control group reported no change in level of physical activity.
As far as we know, this is the first study evaluating the effect of in-hospital physiotherapy on level of physical activity, using a protocol similar to routine care, and making comparisons between patients treated by physiotherapists and patients not treated by physiotherapists.
In the present study, in-hospital physiotherapy had no statistically significant effect on the 6MWT 3 months after surgery. The lack of difference between the groups is supported by Arbane et al, 17 who reported no effect of strength and mobility training on postoperative 6MWT. The treatment that was delivered during the hospital stay in our study was focused on preventing postoperative pulmonary complications and enhancing level of physical activity; and although it included walking and ambulation, the emphasis was not on exercise. It is possible that the intensity of the walking was too low to have an impact on the 6MWT. In addition, the duration of the treatment might have been too short, as it was delivered during a rather short time (4-5 days). Finally, the 6MWT for the whole sample was normal preoperatively, which makes a large postoperative increase unlikely; the study might therefore have been underpowered to detect significant differences between the groups.
Level of self-reported physical activity has been shown to deteriorate from preoperative to 2 months postoperatively for patients undergoing lung cancer surgery. 31 The fact that the patients in the study group in our study reported an increase in level of physical activity is interesting and calls for further research in larger trials. The lack of significant between-group difference could have been due to the relatively small number of patients in the study.
Patients receiving a (possibly new) diagnosis of cancer might be unable to comprehend information about lifestyle choices during cancer recovery. The timing of an intervention is crucial for adherence, 32 and it has been suggested that interventions should only be offered to patients after they have completed first-line treatment. 32 Some patients see the cancer as an opportunity for behavior change and a trigger to start exercising. 33 Even short information on physical activity can help increase the level of physical activity in older adults. 34 It has been reported that patients would like to receive information about how to cope with recovery in general 35 as well as specifically about physical activity. 10 Patients who have undergone lung cancer surgery report that they are both able and willing to participate in physical activity, but still do not engage in a sufficient amount of physical activity. 10 The length of stay after surgery in our study was only 4 to 5 days, and it might be difficult for patients to comprehend the information regarding the importance of physical activity when given so close to the surgery, especially since the majority was diagnosed with cancer. Future studies with the aim of increasing level of physical activity should preferably place the intervention some time after diagnosis and first-line treatment.
We found a statistically significant correlation between the 6MWT and objectively measured physical activity 3 months after surgery, supporting the results of Granger et al, 36 who found a strong correlation between the 6MWT and steps per day. The 6MWT has been shown to be a predictor of survival in lung cancer patients 37 and deteriorates after lung cancer surgery. 31 In our study, there was a statistically significant but small (12 m) deterioration in the 6MWT 3 months postoperatively compared with preoperatively for the whole sample. Although this change was statistically significant, it fails to reach the point of a clinically important difference, which has been suggested to be between 22 and 42 m. 38
In our study, the study group had more men than the control group. Female gender has been linked to shorter length of stay and fewer postoperative complications.39,40
We found no difference in pain between the groups 3 months after surgery. This is in contrast to the results presented by Reeve et al. 15 This could be due to the fact that the patients in our study reported low levels of pain, with 50% of the patients reporting no pain at rest.
There are some limitations in our study. First, there were significant baseline differences in surgery time and gender between the groups. These differences are unfortunate, and it is hard to tell in what way they could have possibly interfered with the results. Another limitation is the lack of objective assessment of preoperative level of physical activity. The optimal design would be to have the patients wear an accelerometer preoperatively. Unfortunately, this was not possible, because the patients presented at the thoracic surgery department at short notice, making it hard to reach them in time for objective preoperative assessment of physical activity. The number of registered days could also be regarded as a limitation, although there is no well-established recommendation on how many days are required to represent habitual physical activity. Another limitation is the single-blind design, although an in-hospital physiotherapy treatment study in the lung cancer surgery population would be impossible to perform double-blinded. To minimize the risk of bias, the pre- and postoperative tests were performed by a physiotherapist unaware of the group allocation. As mentioned above, a recent study suggests that the minimal clinically important difference in the 6MWT is between 22 and 42 m, 38 and so our study could have been underpowered to detect differences in the 6MWT.
In conclusion, no significant effect of routine in-hospital physiotherapy during the immediate postoperative period was found on physical capacity, physical activity, or lung function 3 months after surgery.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Grants from the Research Committee of Örebro County Council (OLL-363321, OLL-686781), the Swedish Heart and Lung Patients National Association (E o86/13), and the Swedish Cancer Society (CAN 2015/721).
Trial Registration
The trial was registered at ClinicalTrials.gov (NCT01961700; ![]() ).
).