
Abstract
Objective:
To observe the clinical efficacy of Dendrobium officinale in the treatment of radiotherapy-induced oral mucositis in nasopharyngeal carcinoma patients, and to explore its regulating effect on immune function and oral microbiota by comparing immune-related factors and oral microbiota before and after the intervention.
Methods:
We conducted a randomized double-blinded controlled trial in Zhejiang Cancer Hospital. Sixty patients with nasopharyngeal cancer combined with radiotherapy-induced oral mucositis were randomly divided into a study group and control group, with 30 cases in each group The study group used compound vitamin B12 solution and Dendrobium tea drink, and the control group simply used compound vitamin B12 solution rinse. When the patients developed radiotherapy-induced oral mucositis (at the time of 10F radiotherapy), and after 1 month of Dendrobium treatment (at the end of radiotherapy), the salivary flow rate was measured without stimulation to evaluate the degree of oral mucositis and the clinical efficacy. We also detected the content of EGF in saliva and the content of IL-10 and IL-11 in serum, and analyzed the differences in microbial community structure. All patients consented before enrollment.
Results:
The salivary flow rate and oral mucosal fraction of the study group after treatment were significantly improved, which was better than that of the control group(P < .05). The content of IL-10 in the study group after treatment increased significantly compared with that before treatment(P < .05). There was a significant difference between the oral flora of the study group before and after treatment (Unique OTU counts: 5390 vs 3906), and there was also a difference between the oral flora of the study group and control group after treatment (Unique OTU counts: 5671 vs 5439). After treatment, Erysipelotrichales (Phylum Firmicutes, LDA score = 2.80, P = .034), Leptotrichiaceae (Fusobacteria,LDA score = 3.38, P = .030) and Campylobacteraceae (Proteobacteria, LDA score = 3.35, P = .026) were significantly enriched in the study group. The use of Dendrobium officinale in nasopharyngeal carcinoma patients with radiotherapy-induced oral mucositis showed little difference in microbial diversity and abundance, but there were significant differences among oral bacteria genera.
Conclusions:
Dendrobium officinale is effective in the treatment of radiotherapy-induced oral mucositis, which may be related to the improvement of salivary gland function and regulation of the oral microenvironment. Dendrobium officinale may reduce the symptoms of radiotherapy-induced oral mucositis by affecting the systemic cellular immune function. It may reduce the secretion of pro-inflammatory factors of the relevant flora by directly changing the oral flora and regulating the oral micro-ecology.
Keywords
Introduction
Nasopharyngeal Carcinoma (NPC) is a malignant tumor originating from squamous epithelial cells of the nasopharyngeal mucosa and occurring at the top and lateral wall of the nasopharyngeal cavity. Due to its special anatomical location and its sensitivity to radiotherapy, radiotherapy has been highly and widely used in the treatment of nasopharyngeal carcinoma. 1 However, due to the long period of radiotherapy for nasopharyngeal cancer, superimposed irradiation dose, and the lack of effective protection for the oral cavity and the maxillofacial area, it is inevitable that it will cause radioactive damage to the surrounding tissues, and the incidence of Radiotherapy-Induced Oral Mucositis (RIOM) is as high as 80%-100%, with the incidence of severe RIOM being 56%-60%.2,3 RIOM seriously affects the radiotherapy compliance and nasopharyngeal carcinoma patients’ life quality, therefore, how to prevent and control RIOM has become an urgent task.
Radiotherapy-induced oral mucositis is mainly caused by the dose of ionizing radiation to the oral mucosa exceeding its tolerance threshold, resulting in the destruction of normal cell DNA and serious damage to blood circulation and immune function, thus triggering an acute inflammatory reaction of the oral mucosa. Radiation stomatitis is often characterized by mucosal pain, dryness, erosion and bleeding, which may affect the patient’s daily eating habits and reduce the quality of life or even worse, finally lead to a reduction in the dose of radiotherapy or the complete termination of radiotherapy, thus affecting the overall therapeutic effect. Currently, no exact and effective treatment has been found in the field of Western medicine, and in most cases, symptomatic treatments such as lidocaine to relieve pain, dexamethasone to reduce inflammation, and Kangfuxin Liquid to promote mucosal regeneration are used, but the clinical efficacy of these methods is not satisfactory.4,5 For the treatment of radiotherapy-induced oral mucositis of nasopharyngeal carcinoma, we went to the ward for clinical investigation and found that vitamin B12 gargling is currently used as a limited treatment that has a certain curative effect. B12 is an important coenzyme in the process of cell synthesis of nucleic acid, which has a repair and regeneration effect on oral mucosal epithelial cells and vascular endothelial cells, and it is also an important part of many oral mucosal protective agents. Current research shows that TCM has demonstrated significant therapeutic effects in the prevention and control of RIOM. Specifically, TCM can effectively delay the onset of RIOM, reduce the incidence of mucosal damage, and to a certain extent, reduce the degree of damage and alleviate the pain. 6 This finding provides a new idea and direction for the treatment of RIOM and demonstrates the unique value and potential of TCM.
According to TCM, radiation is a “fire-heat” treatment, and it would reduce the fluid in human body, resulting in fluid deficiency, leading to thirst, dry throat, difficulty in swallowing and other symptoms. When the “fire-heat” goes deep into the blood, resulting congestion in the local, burning and corrosion of flesh and blood would occur, thus triggering sores and ulcers. The “fire-heat” often leads to symptoms such as dry mouth, thirst, and dryness of the nasopharynx and pharynx 7 . Therefore, in the treatment of RIOM, it is necessary to focus on clearing “fire-heat,” nourishing Yin and generating fluids in order to alleviate patients’ symptoms and improve their quality of life.
Through repeated clinical practice and experience, we found that the efficacy of Dendrobium officinale in the form of a tea substitute for the treatment of RIOM is obvious, and it can reduce the gastrointestinal reaction of the patients. Dendrobium officinale is a new type of traditional Chinese medicine treatment developed by Zhejiang Cancer Hospital. Each pack of Dendrobium substitute tea drink contains 6 g of Dendrobium officinale, decocted into 100 ml liquid with purified water. All Dendrobium herbs was selected and cultivated according to strict standards. The use of Dendrobium in the form of a daily tea drink for the treatment of RIOM, on the one hand, increases the incidences and time of contact between the drug and the oral mucosa, which is conducive to the cleaning of the oral environment, and strengthens the local therapeutic effect; on the other hand, the Dendrobium officinale plays a systemic role after being absorbed through the digestive tract, so that it can play a comprehensive therapeutic effect.
Dendrobium is sweet in taste, slightly cold in TCM nature, with the efficacy of benefiting the stomach and generating fluids, nourishing yin and clearing heat. 8 The main chemical component of Dendrobium is Dendrobium polysaccharide, which contains water-soluble polysaccharides involved in various physiological activities in the cells of living organisms, which can regulate the level of certain cytokines, thus increasing the functions of cellular immunity and humoral immunity.9,10
RIOM is associated with the effects of a range of submucosal cells and tissue cytokines that accompany RIOM throughout its course. For example, IL-10 and IL-11 have a role in down-regulating the inflammatory response and mucosal protection. Studies have shown 11 that elevated levels of the anti-inflammatory cytokine IL-10 were found in the saliva and serum of patients with oral mucositis. In addition, epithelial cells in damaged tissues secrete IL-11, a cytokine that plays an important role in immunomodulation, inflammation suppression, promotion of basal cell proliferation, and inhibition of apoptosis, thereby protecting the integrity of the basal lamina and oral mucosa during radiotherapy. 12 Epithelial growth factor EGF is an important component of the oral mucosal barrier, which can promote the growth, differentiation and proliferation of mucosal epithelial cells and accelerate the repair of wounds. 13 There is a significant negative correlation between the EGF content and the severity of RIOM. 14 This study intends to observe the clinical efficacy of Dendrobium officinale tea drink for the treatment of RIOM in nasopharyngeal carcinoma patients, and to explore its effects on immune function and oral microecology by comparing immune-related factors and oral flora before and after the intervention, which will help to promote the application of TCM in patients with RIOM.
Methods
We conducted a randomized double-blinded controlled trial in Zhejiang Cancer Hospital between June 2022 and December 2023.The study had been approved by the Ethics Committee of Zhejiang Cancer Hospital (IRB-2022-709). All patients were consented by written documents before enrollment.
Population
The study subjects were 60 nasopharyngeal cancer patients who were admitted to outpatient clinics and wards of Head and Neck Radiotherapy Department of Zhejiang Cancer Hospital from January 1, 2023 to December 30, 2023 and met the inclusion criteria. The enrolled cases were subject to the following criteria. (1) Sample size: 60 nasopharyngeal cancer patients were enrolled, and all patients who met the inclusion criteria within 12 months from the start of the study were enrolled by December 30, 2023. (2) Western medical diagnostic criteria: Patients with primary nasopharyngeal carcinoma confirmed by puncture biopsy undergoing radiation therapy, and fulfill the diagnostic criteria for RIOM. The diagnostic criteria for RIOM were based on the Diagnostic Criteria for Radioactive Stomatitis in the National Occupational Health Standards of the People’s Republic of China (GBZ162-2004). (3) Inclusion criteria:① Age 18 to 80 years old; ② Nasopharyngeal cancer patients clearly diagnosed by biopsy pathology; ③ Those who meet the western medical diagnostic criteria of chronic RIOM; ④ Those who have no obvious symptoms of oral pharyngolaryngitis and damage to oral mucosa before radiotherapy; ⑤ Those who signed the informed consent form and agreed to join the cohort study. (4) Exclusion criteria: ① Combination of non-malignant serious diseases that will affect the patient’s compliance or put the patient at risk; ② Concomitant with other anti-tumor treatments or participating in other clinical trials; ③ Patients using antibiotics: including those who have received systemic high-dose antibiotic treatment in the 3 months prior to enrollment, those who have been using systemic antibiotics for a long period of time, or those who have been using antimicrobial mouthwash for a long period of time. (4) Subjects who are also using other medications for oral mucositis; (5) Subjects who have concomitant diseases such as leukemia. (5) Withdrawal criteria: ① Poor compliance; ② Patients do not comply with the study procedures; ③ Patients themselves request to terminate the trial. (6) Ethical principles: All investigations were approved by the Ethics Committee of the hospital (Ethics Approval: Zhejiang Cancer Hospital Ethical Review 2022-320, approved on 10/18/2022).
Randomization
Sixty patients who met the diagnostic criteria of nasopharyngeal cancer and the inclusion criteria were grouped according to the random ratio of 1:1, with 30 cases in each group. Patients were firstly numbered according to their entry order. We used the R3.6.1 software to generate random numbers, which were sealed in opaque envelopes. All participants were sequentially randomized into study group and control group after screening and consent. The sequential numbers were also printed on the external packing and bottles of all the medicine.
Dendrobium Officinale Preparation
Each pack of Dendrobium substitute tea drink contains 6 g of Dendrobium officinale, decocted into 100 ml liquid with purified water. All the liquid is decocted and packed by the Pharmaceutical Center of Zhejiang Cancer Hospital under the quality control of the institution (production date:; October 20, 2022, expiration date: December 31, 2023). All Dendrobium herb was purchased by the Hospital Pharmaceutical Center from Zhejiang Shouxian Valley Pharmaceutical Co., LTD. Dendrobium, as a genuine medicinal material in Zhejiang Province, China, was selected and cultivated according to strict standards. The Dendrobium officinale liquid was packaged immediately after decocting, and the decocting liquid is accurately measured before packaging. Each packet is evenly divided according to the actual amount of decocting liquid. Each single dose package of Dendrobium has a label attached to it. All packed Dendrobium liquid was stored in the cold room of the constant temperature and humidity refrigerator. The study group took 2 packs of Dendrobium officinale tea drink a day, reaching a daily dose of 200 ml.
Intervention
The control group received the following treatment: Compound vitamin B12 solution gargle, 3 times/day, no gargling within 30 minutes after the drug, eating and drinking were also not allowed. Study group received the following treatment: compound vitamin B12 solution + Dendrobium substitute tea drink (2 packs per day, 100 ml per pack, reaching a total dose of 200 ml per day). Both groups were treated for 1 month as the course of treatment (since the emergence of RIOM related symptoms), and the patients were advised to abstain from eating cold, greasy, spicy, fishy and other stimulating foods during the period of medication.
Patients’ Information and Sample Collection
We collected patients’ basic information including gender, age, as well as patients’ disease information. We collected the saliva of patients who have undergone before and after the treatment by using the static total salivary flow rate and cotton swab method, and we collected the saliva once at the time when the patients developed RIOM, at 10 fractions of radiotherapy (10F; the number of times the total dose of the radiotherapy prescription was divided) and once after 1 month of the treatment (at the end of radiotherapy), respectively. The specific steps of saliva collection were as follows: First, the patients were asked to rinse their mouths with purified water to clean their mouths, and cotton swabs were used to absorb the residual saliva in the patients’ mouths to ensure that the mouths were kept dry. Secondly, another 3 dry cotton swabs, which were weighed accurately, were gently placed under the patient’s tongue and on both sides of the parotid gland to collect saliva. There was no stimulation throughout the saliva collection, to ensure that the patient’s saliva is secreted naturally. During this process, the patient was instructed not to swallow their saliva. After a 2-minute wait, the swabs were removed and the residual saliva on the tongue and tongue fossa was aspirated with the swabs. Finally, the swabs were weighed after aspiration of saliva and the data were recorded.
Efficacy Evaluation
Before and after the treatment, we would evaluate the efficacy according to the oral mucositis grading. Chronic radiotherapy-induced oral mucositis grading criteria: The grading criteria for chronic radiotherapy-induced oral mucositis are formulated with reference to the Diagnostic Criteria for Radioactive Oral Stomatitis (GBZ162-2004) in the National Occupational Health Standards, as shown in Table 1.
Grading Criteria for Chronic Radiotherapy-Induced Oral Mucositis.

Detection of Immune-Related Factors
Regarding the detection of immune-related factors before and after the Dendrobium intervention, we collected saliva and serum specimens according to the method as described above at the time of the patients’ development of RIOM (at 10F of radiotherapy) and 1 month after the treatment (at the end of radiotherapy), respectively, and left them to stand for half an hour. We then used centrifugation of 3000 r/min, rewarming and equilibrating them at room temperature for 20 minutes. Detecting the saliva’s EGF content, and IL-10 and IL-11 content in serum was peformed by enzyme-linked immunosorbent assay. Control group I: (Saliva) A: At the appearance of RIOM; B: After 1 month of treatment with Dendrobium substitute tea drink; control group II: (serum) A: At the appearance of RIOM in the control group; B: after 1 month of treatment in the control group; C: at the appearance of RIOM in the study group; D: after 1 month of treatment in the study group.
For saliva specimens, we performed centrifugation at 1000 g for 20 minutes to remove impurities and cellular debris. The supernatant was taken for testing and the amount of EGF was measured using an Elisa assay kit. For serum specimens, we used tubes free of pyrogen and endotoxin, avoiding any cellular stimulation during the procedure and centrifuge the serum at 4000 rpm for 20 minutes, carefully isolated the serum and store it below −20°C, avoiding reverse freezing and thawing. Then, the supernatant was taken for the assay and the levels of IL-10 and IL-11 were measured using the Elisa assay kit.
Oral Flora Detection
We examined the oral flora of nasopharyngeal cancer patients at different time points and pre-treated the collected saliva. We sampled saliva from 2 groups of nasopharyngeal cancer patients at the time of the appearance of RIOM (at the time of 10F of radiotherapy) and 1 month after the treatment with Dendrobium (at the time of the end of radiotherapy), respectively. Half an hour before sampling, the patients were prohibited from eating, brushing teeth, gargling, etc. During saliva collection, the patients were prohibited from expectorating. We adopted the non-stimulating saliva collection method, instructing the patients to let the saliva flow into the 10 ml EP tubes on its own, and repeating the sampling for several times until the amount of saliva samples reached 2 ml, and then the samples were placed into the refrigerator at −80°C for the subsequent testing.
We performed high-throughput 16S rDNA sequencing and analysis of saliva specimens. The main instruments and reagents we used are shown in Tables 2 and 3. Firstly, we extracted DNA from the pre-treated saliva samples; we collected the precipitate by centrifugation and extracted the DNA using a kit, and then performed electrophoresis for detection. Next, PCR amplification and high-throughput sequencing were performed. Highly variable regions were amplified using specific enzymes, PCR products were normalized and Illumina sequencing libraries were constructed. After repairing ends, adding bases and sequencing junctions, performing size selection and purification, on-board sequencing was performed. Finally, 16S rDNA bioinformatics analysis was performed. We used BLAST to differentiate the samples, removed Barcode + primer, removed low-quality sequences by Lucy software, compared and classified them with NCBI database. Operational taxonomic units were determined based on sequence similarity, library diversity was assessed, and microbial community structural differences were analyzed using the UnifracPCoA method.
Main Reagent Consumables.

Instrument.

Sample Size Estimation
Early clinical observation showed that Dendrobium officinale showed good potential in improving the symptoms of radiotherapy-induced oral mucositis of nasopharyngeal carcinoma and promoting the balance of oral flora. The incidence of adverse events was estimated to be less than 30% in the study group and 100% in the control group. The significance level α was set to 0.05, and the test efficiency was set to 80%. SAS software was used to calculate that the sample size of the study group was 27 cases (N1), the control group was 27 cases (N2). A total of at least 54 cases should be included in the 2 groups. Considering the loss of follow-up rate of 10%, 30 patients were included in each group in this study. The results of each index were consistent and significant between the 2 groups, so the influence of chance could be excluded, indicating that there was indeed a difference between the 2 groups.
Statistical Analysis
In this study, SPSS 25.0 software was used to statistically analyze the data. The measurement information in the data was uniformly expressed as mean ± standard deviation (x ± s ) and t-test was used; the count data and rank data were expressed as absolute numbers or rates. The selection of statistical methods was based on the type of data: t-test was used for normally distributed data in the measurement data, and non-parametric testing was used for the opposite. χ2 test and rank-sum test were used for the count data and rank data respectively. P < .05 indicated that the difference was statistically significant. The oral flora part was compared with the differences in oral flora at different time points by Anosim similarity respectively. The data were downscaled with Principal coordinates analysis (PCoA). The species abundance of oral flora at different time points was analyzed using the rank-sum test Kruskal-Wallis test, and the genera with significant differences were screened out. In order to ensure the reliability of the results, we also introduced the Dunn test as a post-hoc test, which was further validated against the results of the Kruskal-Wallis test. All the above data were considered statistically significant at P < .05.
Results
General Characteristics
In this study, a total of 60 patients who met the criteria for enrollment entered the trial. The patients who met the diagnostic criteria of nasopharyngeal cancer and the inclusion criteria were grouped according to the random ratio of 1:1, with 30 cases in each group. Of 60 patients who were randomly assigned, there were no drop-offs or withdrawals. Thirty patients in the study group and 30 patients in the control group completed all treatments and were finally analyzed. The Figure 1 shows the consort flow diagram, which describes the situation of the enrollment.

Consort flow diagram.
Comparison of gender, age, and clinical characteristics between the 2 groups: 60 of patients with nasopharyngeal carcinoma RIOM were included in this study. Thirty cases were in the study group, 19 males and 11 females, aged 57.16 ± 9.87 years. In the control group, there were 30 cases, 22 males and 8 females, aged 60.13 ± 9.76 years. As analyzed by χ2 test and t-test, there was no statistical difference in gender and age between the 2 groups (P > .05), and they were comparable, as the following tables show (Tables 4 and 5):
Comparison of Gender Between the Two Groups of Patients.

The two groups were not statistically significant in terms of gender (P .405 > .05) and were comparable.
Comparison of the Age of Patients in the Two Groups (¯x ± s, years).

The difference in age between the 2 groups of patients was not significant (P = .240 > .05) and is comparable.
On the determination of salivary flow rate before and after the intervention of Dendrobium officinale, according to Table 6, it can be seen that there is no statistically significant difference in the comparison of salivary flow rate between the 2 groups of patients before treatment (P > .05), and the data of the 2 groups are comparable. The difference in the comparison of salivary flow rate between the 2 groups of patients after treatment was statistically significant (P < .05), and there was also a statistically significant difference between the study group before and after treatment (P < .01).
Changes in Salivary Flow Rate Before and After Dendrobium Treatment (¯χ ± s, n = 30).

On the determination of RIOM scores before and after treatment, The oral mucositis scores of the experimental and control groups before and after treatment are shown in the Table 7 below. According to the Table, it can be seen that before treatment the difference between the oral mucositis scores of the control group and the study group before treatment was not significant (P > .05) and was comparable. After treatment, the RIOM scores of the study group were statistically different from those of the control group (P < .05), and there was a significant decrease in the number of patients with severe degrees (III and IV) compared with those of the control group (P < .01).
Radiation Oral Mucositis Classification Before and After Treatment (n = 30).

On the content of EGF in saliva and changes in serum levels of IL-10 and IL-11, as can be seen in Table 8, there was no significant change (P > .05) in the EGF content in the saliva after treatment with Dendrobium officinale compared to the pre-treatment period.
EGF Content in Saliva (¯χ ± s, n=11).

As can be seen from Figure 2,there is no significant difference between the IL-10 content in serum of the study group and the control group before treatment (P > .05), at the same baseline level. After treatment, the IL-10 content of the control group had a tendency to increase compared with the former, but there was no statistical significance (P > .05); the IL-10 content of the study group increased significantly compared with the former, with statistical significance (P < .05), and compared with the control group there was a tendency to increase but there was no statistical significance (P > .05). Figure 2 also shows that there was no significant difference in IL-11 content in serum between the study group and the control group before and after treatment (P > .05), but IL-11 had a tendency to increase after treatment in both groups.
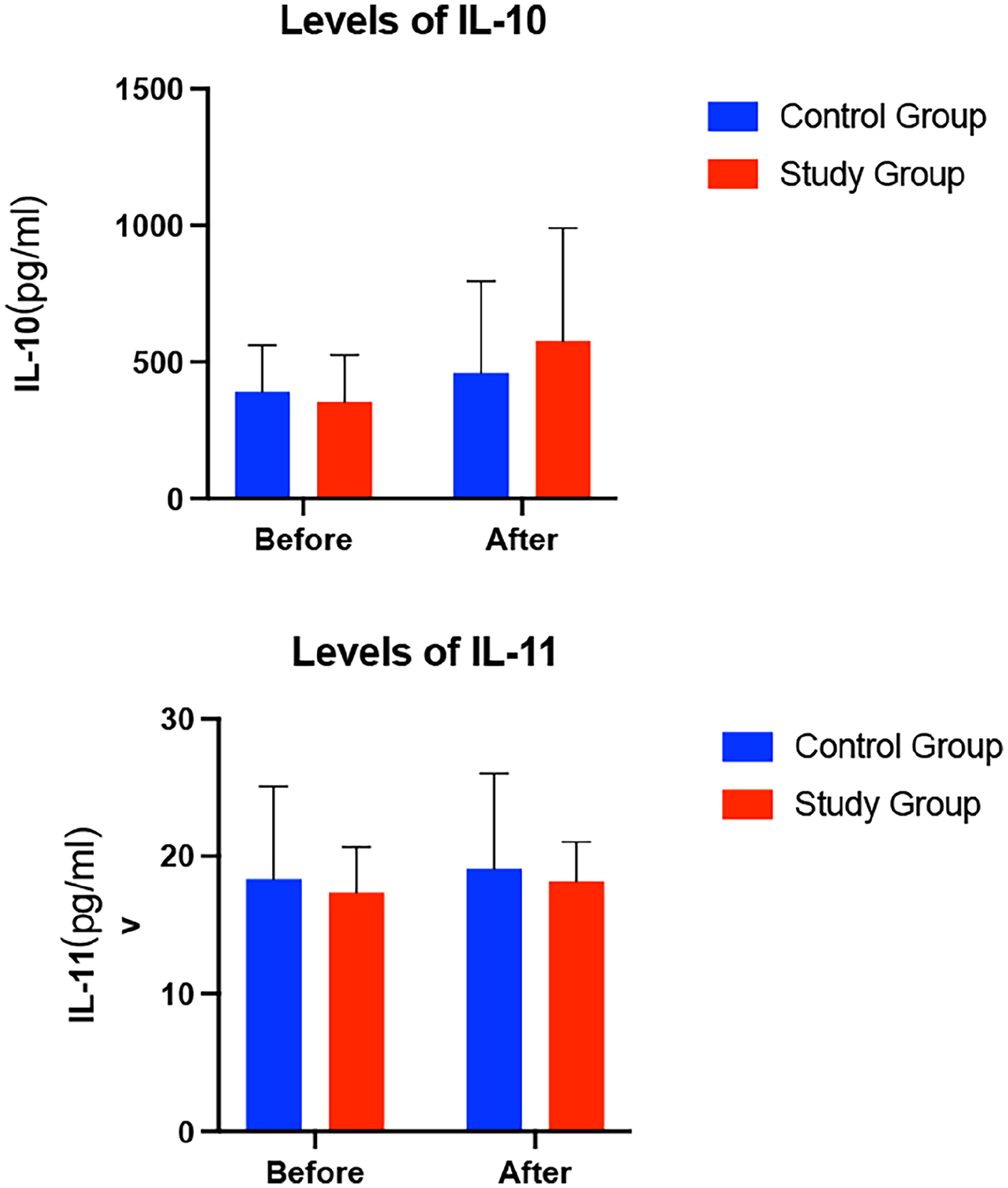
IL-10,IL-11 content in serum of the study group and the control group before treatment.
OTUs and Alpha of Oral Flora
Regarding the changes in oral flora of nasopharyngeal cancer patients at different time points, we performed categorical annotated statistics on OTUs before and after treatment in the study group and between the study group and the control group and comprehensively assessed the Alpha diversity of the microbial community, as shown in Figure 3.

OTUs and alpha of oral flora (A−D).
The results of 16SrDNA sequencing analysis showed that 5390 OTUs were unique before treatment and 3906 OTUs were unique after Dendrobium treatment in this study, as shown in Figure 3A. As a preliminary indication of sample species abundance, the study group of patients before and after treatment OTUs have some differences. As shown in Figure 3B in this study, the study group had 5671 OTUs uniquely after treatment, and the control group had 5439 OTUs uniquely after treatment. This indicates that the application of Dendrobium officinale has a certain effect on the oral flora OTUs. As shown in Figure 3C and D. We used Chao1 and Observed species indices to reflect the abundance of microbial communities, and microbial community diversity was captured through Shannon and Simpson indices. We used Faith’s PD index to characterize evolution-based diversity and Pielou’s evenness index to assess the evenness of species distribution in microbial communities. To ensure the reliability of the analyses, we introduced Good’s coverage index to assess the coverage of the samples. By analyzing this series of indices, we were able to assess the Alpha diversity of the microbial community more accurately. It was found that all the above indices before and after treatment were roughly similar and none of the differences were statistically significant (P > .05), indicating that the differences in the diversity and abundance of the flora before and after Dendrobium officinale treatment in patients with nasopharyngeal carcinoma with RIOM were relatively small. On the diversity index of oral flora in the study and control group after treatment, none of the differences in the indices of the 2 groups were statistically significant (P > .05), and the data suggests that the application of Dendrobium is less different in terms of bacterial diversity and abundance for patients with nasopharyngeal carcinoma with RIOM.
Heat Map and LEfse of Distribution and Variation of Oral Flora
We analyzed the distribution and abundance variability of the composition of oral flora, used the abundance data of the top 50 genera in terms of mean abundance to create a heat map, and also performed LEfSe analyses of the differences between pre- and post-treatment. The results are shown in Figure 4.
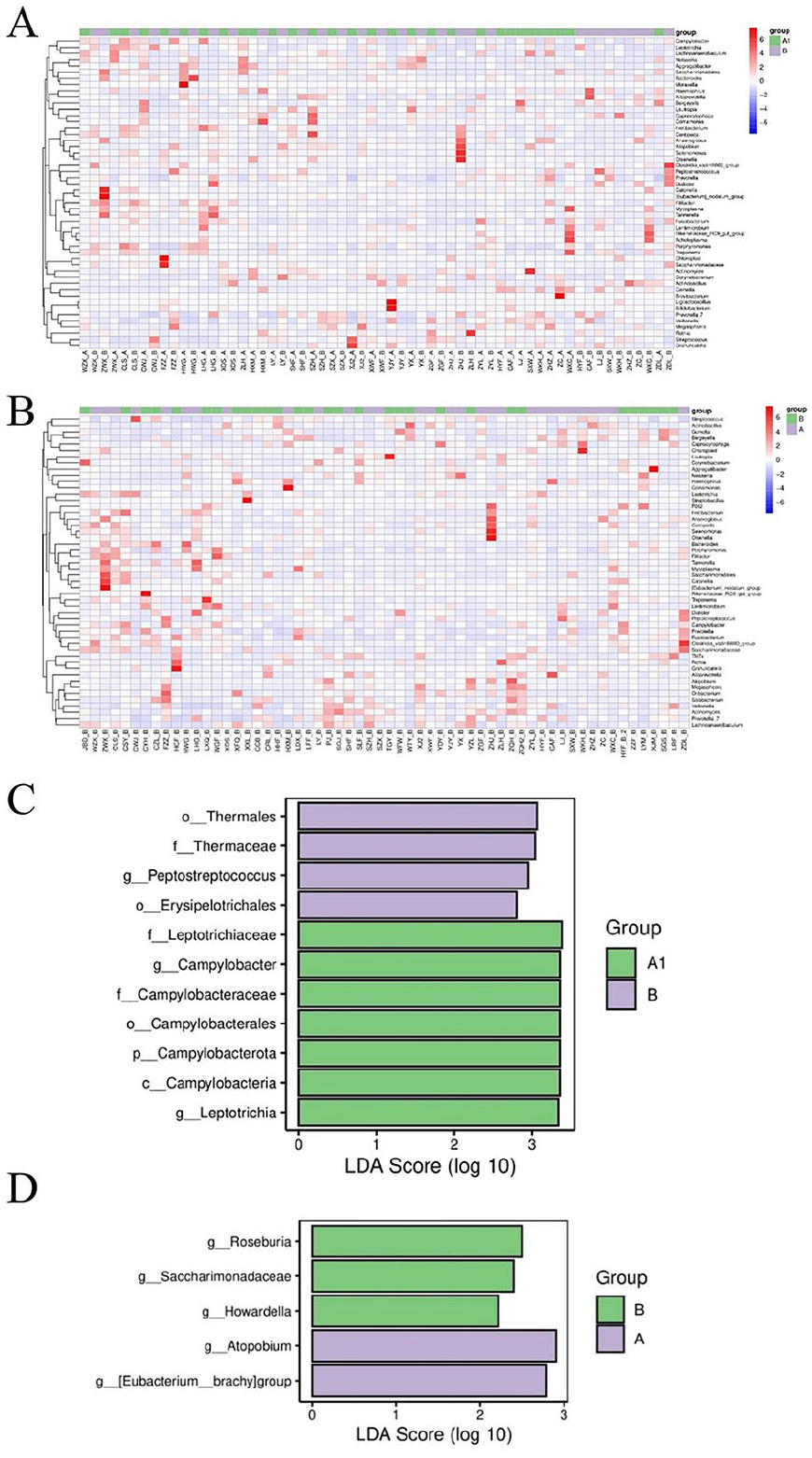
Heat map and LEfse of distribution and variation of oral flora (A−D).
As can be seen in Figure 4A, there was a significant difference between the genera of oral bacteria in the study group before and after treatment with Dendrobium officinale. As can be seen from the heat map of genus differences between the study and control groups in Figure 4B, the use of Dendrobium officinale or not made a significant difference in the oral flora. In Figure 4C, where LDA was performed on samples from both groups, retaining by default the results of LDA score >2 as well as P < .05. The significantly different genera in the pre-treatment group included Peptostreptococcus (Phylum Firmicutes, LDA score = 2.95, P = .006), Thermaceae (Thermales, LDA score =3.03, P = .045); while the species significantly enriched in the post-treatment group compared to the pre-treatment group included Erysipelotrichales (Phylum Firmicutes, LDA score = 2.80, P= .034, Leptotrichiaceae (Fusobacteria, LDA score = 3.38, P = .030), Campylobacteraceae (Proteobacteria, LDA score = 3.35, P = .026).
We also analyzed species for differences between the study and control groups after treatment. As shown in Figure 4D, the significantly different genera in the control group included Howardella (Hahella, LDA score = 2.21, P = .038), Roseburia (Actinobacteria, LDA score = 2.50, P = .005), and Saccharimonadaceae (Saccharimonas, LDA score = 2.39, P = .040), while the species significantly enriched in the study group compared to the control group included Atopobium (Proteobacteria, LDA score = 2.90, P = .032) and Eubacterium Brachy (Actinomycetes, LDA score = 2.78, P = .016).
Discussion
Nasopharyngeal carcinoma, as a common type of head and neck tumor, is particularly prevalent in the southern region of China, with the incidence rate of men significantly exceeding that of women. The peak age group of incidence is concentrated at 40 to 59 years old, and in terms of pathological types, squamous carcinoma occupies the majority, with a proportion as high as more than 95%. Given the high sensitivity of nasopharyngeal cancer to ionizing radiation, radiotherapy has become the main treatment for non-metastatic nasopharyngeal cancer. However, toxic side effects of radiotherapy have been an important issue for patients. Specifically, radiation destroys the division compensation mechanism of the oral mucosa through direct or indirect mechanisms of action, which in turn triggers damage to the epithelium of the oral mucosa, ultimately leading to the occurrence of radiotherapy-induced oral mucositis. 15 Effective inhibition of the inflammatory response and maintenance of the dynamic balance of the oral flora are important strategies for the relief of radiation oral mucositis. Therefore, the authors speculate that inhibiting the inflammatory response and balancing the oral flora is an effective way to relieve radiation oral mucositis.
There is a direct correlation between the occurrence of radiation oral mucositis and radiation dose. When the irradiation dose received in the target area reaches 10 to 20 Gy, the appearance of RIOM can be observed. 16 Therefore, in this study, the patients with nasopharyngeal carcinoma treated with radiotherapy of 10F were selected to be enrolled. After the end of radiotherapy, when the direct effect of radiation disappeared, was selected as the point in time to assess the therapeutic efficacy. This point embodies the characteristics of TCM of stopping the therapies when the disease condition is alleviated or eliminated, and also examining its role in the acute phase to inhibit the inflammatory response. 17
The results showed that after treatment with Dendrobium officinale, the serum level of IL-10 increased significantly compared with that before treatment, which was different from that of the control group. The role of IL-10 in the immune system can be divided into 2 aspects: intrinsic immunity and adaptive immunity. In intrinsic immunity, IL-10 mainly acts on antigen-presenting cells, and it suppresses the inflammatory response by inducing an immunosuppressive response. 18 Since its discovery, IL-10 has been shown to inhibit the production of inflammatory cytokines by Th1 cells 19 and to inhibit the antigen-presenting capacity of monocytes by down-regulating major histocompatibility complex II (MHC-II), thereby preventing the specific proliferation of T cells. 14 IL-10 plays a complicated role in the modulation of T-cell function in different inflammatory stages. Specifically, it can directly inhibit the pro-inflammatory effects of CD4+ T cell subsets, which slows down the progression of inflammation to some extent. 20 As an important pro-inflammatory cell, Foxp3-overexpressing CD4+ T cells, with their surface-expressed CD40L protein, activate B cells, which in turn exacerbate inflammation. 21 However, IL-10 can inhibit inflammation by affecting the stability of Foxp3+ regulatory T cells. At the same time, IL-10 inhibits the differentiation of Th17 cells, further regulating the inflammatory response. In summary, the effects of IL-10 in regulating T cell function are diverse and complex, and more in-depth studies are needed to fully understand its mechanism of action in different inflammatory stages.
IL-10, as an anti-inflammatory factor, was elevated more in the study group than in the control group, and the grades of radiographic oral mucositis in the study group were statistically different from those in the control group after treatment: there was a significant reduction in the number of patients with severe degrees (III and IV) compared with those in the control group, which suggests that Dendrobium officinale may ameliorate radiographic oral mucositis by influencing the level of IL-10 in vivo and exerting an anti-inflammatory effect.
Combined with the analysis of related literature, Dendrobium officinale has been shown in clinical trials in dentistry to promote healing of oral ulcers.22,23 The most active polysaccharide component in Dendrobium officinale, neutral polysaccharide (DOP-1), can promote human oral mucosal epithelial keratin formation, improve anti-inflammatory ability and show a positive correlation with its drug concentration. 24 Studies have shown 25 that Dendrobium polysaccharides in Dendrobium can significantly promote cell proliferation, reduce the incidence of apoptosis, promote the S-phase process of the cell cycle in RAW264.7 macrophages, and promote the secretion of TNF-α, IL-1β, iNOS, and IL-6 cytokines by RAW264.7 macrophages to play anti-inflammatory roles.
While radiation treats malignant tumors by killing and inhibiting malignant cells, it also has adverse effects on normal cells, such as producing direct damage to the epithelial cells of the oral mucosa and replacing the plasma vesicular cells with fibrous tissues, leading to dysfunction of the secretory glands of the oral cavity.26,27 In present research, we observed that the salivary flow rate of the study group was decreased to a lesser extent than that of the control group, which suggests that Dendrobium officinale tea drink can reduce the damage of radiation on salivary gland function and relieve the symptom of dry mouth and thirst. Xiang et al. 28 found that Dendrobium improves the function of the salivary glands by inhibiting the apoptosis of human salivary gland cell lines induced by TNF-α. Lin Xiao et al. 29 found that Dendrobium officinale extract could regulate the expression of AQP-5 in the lacrimal glands of patients with desiccation syndrome, thereby promoting salivary secretion and relieve the symptoms of mouth dryness.
The damage to the glandular tissue from radiation results in a significant decrease in salivary secretion and a slowing down of the salivary flow rate, which in turn leads to an increase in the viscosity of the oral secretions. These changes not only weaken the moisturizing and cleansing functions of the oral cavity, but also reduce its purifying capacity. 30 The knock-on effect of this series of physiological responses provides favorable environmental conditions for the growth and synergy of microorganisms such as fungi and bacteria. In this environment, the structure and equilibrium of the oral microbial community undergoes significant changes, and the original colony balance is disrupted. This change further induces or exacerbates the symptoms of oral mucosal inflammation, posing a serious threat to oral health.31,32 The data from the current study showed that the significantly different bacterial genera before treatment included Peptostreptococcus, Thermaceae and others. Peptostreptococcus is a Gram-positive coccobacillus, dominant in the oral flora, and a common pathogenic bacterium, 33 which could create an inflammatory environment, favoring bacterial survival, proliferation, recurrent infections, and release of virulence, leading to digestive malfunction.
Meanwhile, the results of the present study showed that there were significant differences between the oral bacterial genera before and after the treatment of Dendrobium officinale in the study group. Among the species that were significantly enriched after treatment included Erysipelotrichales, Leptotrichiaceae, Campylobacteraceae, and others. The Erysipelotrichales is a branch under the Phylum Firmicutes, in which it belongs to the Erysipelotrichia. When the organism is infected with these pathogenic bacteria, in histopathological observation, we can find that the endothelial cells of capillaries and microvessels in many tissues and organs show significant swelling and degeneration. At the same time, neutrophils and mononuclear macrophages were markedly infiltrated at the lesion site, and the formation of microthrombi was common. 34 These pathological changes coincided with the signs demonstrated in radiolucent oral mucositis, further revealing the serious consequence of infection by Erysipelotrichales in the development of oral mucosal inflammation. Leptotrichiaceae belong to the Fusobacteria, which are Gram-negative bacteria that are conditionally pathogenic. These bacteria break down carbohydrate to produce acid, the main products of which are DL-lactic acid and acetic acid, which lower the environmental pH and can produce endotoxin, leading to the development of inflammation. It has been demonstrated that the relative abundance of Fusobacteria and Leptotrichia increases with increasing radiation dose, promoting inflammation and helping to create a long-term inflammatory environment.
Significantly different genera in the control group after radiotherapy included Roseburia, Saccharimonadaceae, and Howardella. Roseburia act as symbiotic bacteria that produce high levels of butyrate and digest multiple species of prebiotic polysaccharide structures to promote host intestinal health. 35 As shown by Nooshin et al, 36 Roseburia may control the inflammatory process by influencing the expression of pro- and anti-inflammatory cytokines through the modulation of Treg/Th17 balance. Meanwhile, butyrate produced by Roseburia may enhance anti-PD-1 efficacy in colorectal cancer by activating cytotoxic CD8+ T cells. 37 However, the functions of Roseburia are not entirely singular. Flagellin preparations obtained from bulk cultures of Roseburia. were able to stimulate IL-8 secretion from human intestinal epithelial cell lines, suggesting a pro-inflammatory role for flagellin. 38
Species that were significantly enriched in the study group compared to the control group included Atopobium and Eubacterium Brachy. The Atopobium is a Gram-stain-positive anaerobic bacillus, and Yuchao Li et al. 39 found that the relative abundance of Atopobium in patients with squamous cell carcinoma of the gingiva showed a trend of significant increase. Moreover, this genus was closely associated with the formation of periodontal abscesses and subgingival plaque, suggesting its important role in oral health problems. Eubacterium shortum is a Gram-positive bacterium belonging to the family Eubacteriaceae, phylum Thick-walled Bacteria. It is one of the core genera of the human intestinal microbiota and shows extensive colonization of the intestinal tract, oral cavity and other parts of the intestines in most populations, and has an important role in the body’s nutrient metabolism and the maintenance of intestinal homeostasis, including the production of short-chain fatty acids, modulation of prevention of intestinal inflammation 40 and prevention of colorectal cancer. 41 These fatty acids not only provide an exceptional source of nutrients and energy to the intestinal epithelium, but also help to protect the integrity of the intestinal mucosal barrier. In addition, short-chain fatty acids play an important role in reducing the level of inflammation in the body and help enhance the motility of the gastrointestinal tract. Taken together, the enrichment of inflammation-associated flora is also consistent with the manifestations of RIOM.
The present study suggests that RIOM may affect the oral flora by influencing the systemic cellular immune function. Based on the above research results we hypothesize that Dendrobium may be involved in adjusting the oral microbial community by directly or indirectly altering the relative abundance of communities such as Atopobium, Eubacterium Brachy and Roseburia, thus altering the oral micro-ecology, and at the same time, inflammatory factors produced by the associated pathogens may also affect the healing of the oral mucosa, which would further influence the disease progression of oral mucositis.
Currently, the principles of management for RIOM include relieving oral pain, protecting the ulcerated surface and keeping the mouth clean, with relatively few improvement measures targeting the oral flora. 42 Therefore, it is particularly crucial to deeply investigate the association between Dendrobium officinale tea drink and RIOM. On the one hand, RIOM is often associated with complications such as mouth dryness, eating disorders, loss of taste, and sore throat, which not only significantly affects the quality of life of patients, but also may lead to nutritional deficiencies, which may further exacerbate the condition. On the other hand, severe RIOM may force patients to interrupt or even abandon treatment, which not only prolongs the course of the disease, but also reduces the overall effect of radiotherapy due to the accelerated repopulation of tumor stem cells. The results of this study showed that Dendrobium officinale tea drink can effectively improve the salivary flow rate, regulate the oral flora and immune factors, thus reduce the symptoms of RIOM, so we may regard this study as a basis to further explore the molecular mechanism of Dendrobium officinale in the treatment of RIOM, and to extract the key components of the drug, so as to provide a clear theoretical basis for the treatment of the disease and the subsequent use of the drug. By systematically investigating the potential of Dendrobium officinale tea drink in the prevention and treatment of RIOM, it is expected to provide a safer and more effective therapeutic strategy for patients with nasopharyngeal carcinoma.
Limitations
Due to time and condition limitations, there are still some shortcomings in our study. The number of patients enrolled in this study was too small to provide more precise supportive data; and detailed data tracking tests about the relationship between specific oral microecological changes and the progression of radiotherapy-induced oral mucositis are still lacking.
In view of the above shortcomings, in future studies, we plan to further improve the relevant experiments, consider increasing the sample size, and monitor from the beginning of radiotherapy prophylactic medication until after the end of radiotherapy, with continued medication until the cure of radiation oral mucositis. Inflammatory factors and oral microecology will be in multiple time periods, and further studies carried out based on continuous supplementation. As the composition of the medicine is complex, we can further explore the molecular mechanism of Dendrobium officinale in the treatment of radiotherapy-induced oral mucositis and extract the key components of the drug, so as to provide a clear theoretical basis for the clinical treatment of radiotherapy-induced oral mucositis as well as for the subsequent use and development of the drug.
Conclusions
Dendrobium officinale is effective in the treatment of RIOM, which may be related to its ability to improve the function of salivary glands and regulate the oral microenvironment. Dendrobium officinale may reduce the symptoms of RIOM and improve it by affecting the systemic cellular immune function and regulating related immune factors. What is more, Dendrobium officinale may reduce the secretion of pro-inflammatory factors of the relevant flora by directly altering the oral flora, regulating the oral microecology, and thus alleviating the disease. This study suggests that Dendrobium officinale is effective in the treatment of RIOM and provides a certain research basis for exploring the alleviation of the side effects of Dendrobium officinale against tumor. We believe that this study will be a good starting point, from which patients with nasopharyngeal cancer can benefit.
Footnotes
Author Contributions
Jiaying Yang: Writing—original draft, Visualization, Investigation, Data curation. Yuancai Liu: Writing—review & editing, Investigation. He Yao: Writing—review & editing, Investigation. Mengying Sun: Writing—review & editing, Methodology, Conceptualization. Yangbo Tong: Writing—review & editing, Investigation. Guanjun Ma: Writing—review & editing, Investigation. Zhuo Chen: Writing—review & editing, Investigation. Xiang Qian: Writing—review & editing, Investigation. Aiqin Zhang: Writing—review & editing, Supervision, Funding acquisition, Conceptualization.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This event was funded by the Basic Public Welfare Research Program of Zhejiang Province (grant number LGF22H270004).
Informed Consent Statement
All investigations were approved by the Hospital Ethics Committee (Ethics File No.: Zhejiang Cancer Hospital 2022-320 (Section)). All participants volunteered to participate in this study and signed the informed consent forms.