
Abstract
Keywords
Introduction
Multidisciplinary approaches to cancer treatments have been reported to show improved clinical outcomes among cancer patients.1,2 The goal of the multidisciplinary team which comprises a group of experts and healthcare professionals 2 is to deliver personalized treatment, while also empowering patients in their cancer care. 2 The latter includes educating patients in essential lifestyle factors that has the potential to transform their health, and help maintain or improve their quality of life (QOL).
Lifestyle factors are increasingly accepted in the medical literature to have a positive impact on cancer prevention, prognosis, and survival. 3 Modifiable lifestyle factors including diet, physical activity, stress, social support, sleep, and mind-body connection, among others, have been shown to favorably impact health, including cancer, outcomes. 3 Findings from a study by Ornish et al, 4 suggest that intensive changes in diet and lifestyle could affect the progression of early prostate cancer. Researchers have also shown that a similar plant-based diet and Mindfulness-Based Stress Reduction (MBSR) program may help slow the progression of advanced prostate cancer over a period of 4 months. 5 Their findings suggest that the progression of the disease can be slowed or even reversed, without further surgery, radiation, or chemotherapy. 5 Additionally, a 6-month pilot clinical trial investigating the effect of adopting a plant-based diet, reinforced by stress management training, provided preliminary evidence that such lifestyle-factor changes may attenuate disease progression and have therapeutic potential for clinical management of recurrent prostate cancer. 6 These findings showed the potential for modifying cancer progression and outcome with changes in lifestyle factors.
Qualitative research by Turner on more than 1,500 cases of cancer survivors experiencing radical remission, also referred to as spontaneous remission or spontaneous regression,7 -9 has led to the identification of 9 key lifestyle factors which she refers to as “healing factors,” (outlined below) that were consistently reported by cancer survivors of all cancer types who experienced Radical Remission (RR).7,10 The occurrence of RR can be found in most types of cancer and has been defined in the literature as the partial or complete disappearance of a malignant tumor in the absence of treatment, or in the presence of therapy considered insufficient to exert a major influence on the disease progression.11,12
The Radical Remission Multimodal Intervention (RRMI), developed by Kelly A. Turner, Ph.D., comprises the key lifestyle factors she identified in her research on RR survivors.7 -9 According to Turner, thousands of RRMI participants reported in their evaluation forms, upon completion of the RRMI, that the intervention has helped improve the quality of their lives and their coping ability to live with cancer (K. Turner, personal communication, November 21, 2023). QOL is a major concern of cancer patients. People living with cancer experience a variety of challenges and symptoms due to the disease, as well as side effects to the treatments received.13 -16 Cancer pain is one of the greatest causes of reduced QOL in people with cancer. 17 Integrative management strategies, including acupuncture, massage, music therapies, and mind-body practices, have shown promise in reducing cancer pain.18 -20 Addressing QOL, including reducing cancer pain, is an important component of cancer care, as it contributes to enhanced health outcomes and overall well-being of the patient, including decreased treatment side effects and longer survival.16,21 -23 Improving QOL is an integral component of healing or disease recovery. 24
More recently, Turner has trained health coaches in the RRMI in order to educate more people with cancer about these lifestyle factors. We hypothesized that the RRMI will be associated with significant improvement in the QOL of adults with cancer, who participated in structured RRMI workshops, at 6 months after the intervention compared to before. Secondarily, we hypothesized that improvements will also be observed at month 1 post-intervention compared to baseline. Impact of the RRMI on QOL subscale measures such as emotional well-being and social and family well-being, at both month 1 and month 6, was also explored. Additionally, we explored the relationship between adherence to these factors and QOL.
Methods
Study Design
For this pilot study, to test our study hypotheses, and to explore the impact of the RRMI on the QOL subscale measures of our target population, we conducted a prospective pre-post outcome pilot study, between January 2019 and January 2022, on a convenience sample of adults with cancer who attended the RRMI workshops (on-line or in-person). Participants completed online questionnaires at baseline or pre-intervention (i.e., within a week prior to participation in the program), and at least 1 month and 6 months post-intervention. This simple and low-cost study design allows for measuring baseline levels of outcome measures of interest before the intervention and the assessment of how these measures change after the intervention at month 1 and month 6. The study design and participant enrollment flowchart is presented in Figure 1. Through our automated online tracking system and website, HARIS (Harvard Automated Research Information System), all potential participants were provided information about the purpose, any risks involved, and benefits of the study, study eligibility criteria, as well as the importance of their full cooperation if they chose to participate. These details were also included in the consent document, which each participant read and signed online before entering the study. The study protocol was reviewed and approved by the Institutional Review Board of the Harvard T.H. Chan School of Public Health (Protocol#: IRB18-1239) on December 10, 2018.
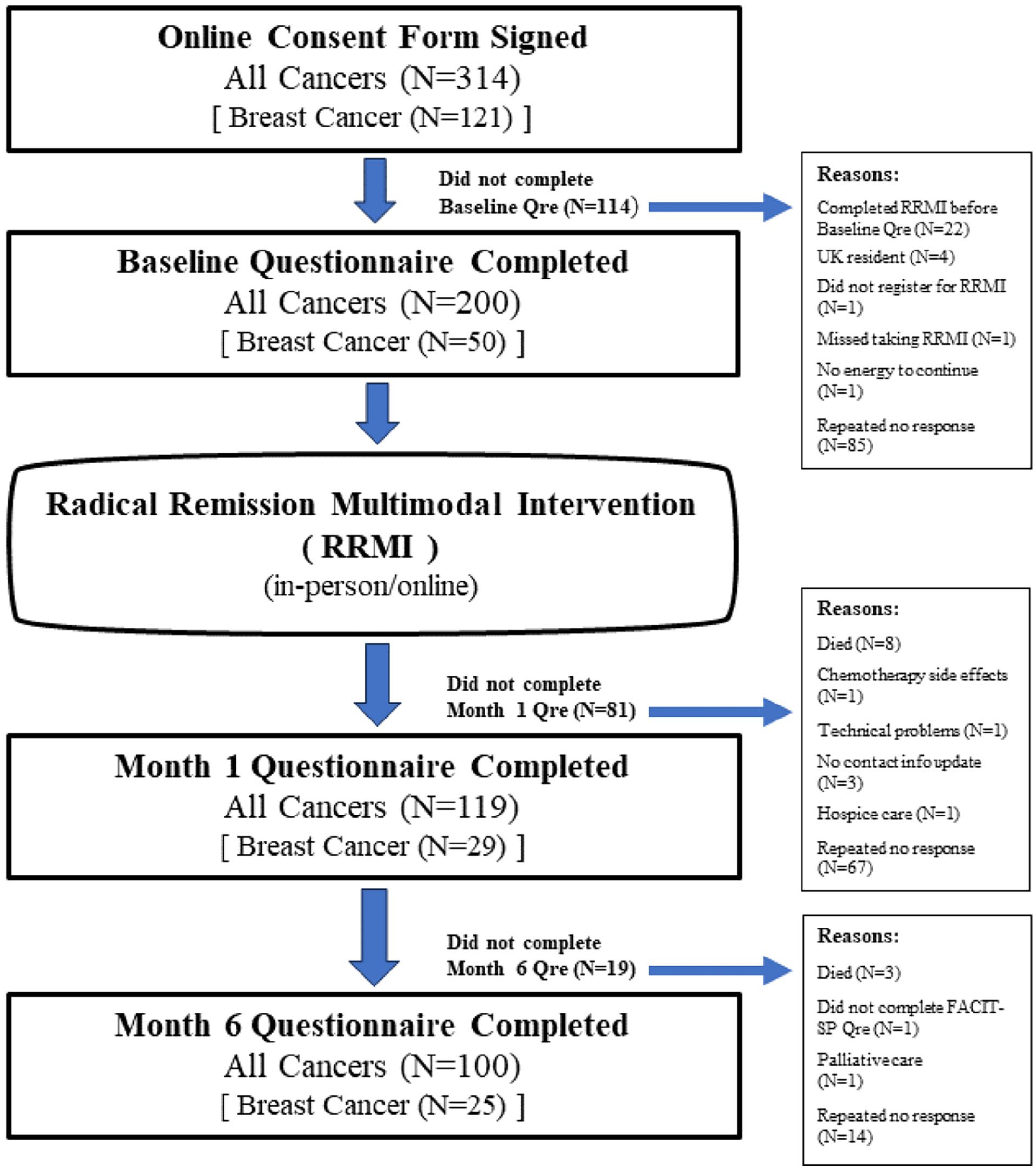
Study design and participant enrollment flowchart.
Eligibility Criteria and Recruitment
Participants were eligible for the study if they reported having been diagnosed with any cancer (other than non-melanoma skin cancer), aged 18 years or more, are citizens of the United States and non-European countries, had signed-up for the RRMI workshops either online or in-person, and had easy access to broadband internet. Citizens of countries in Europe were excluded due to higher costs needed to conform to the General Data Protection Regulation (GDPR). 25 Participants were not compensated for their participation.
Study recruitment was undertaken with the assistance of Turner and the Radical Remission Project staff, including through word of mouth, emailing, postering, social media, and advertising. The Radical Remission Project staff also contacted a network of oncology naturopaths, integrative medicine physicians and the Cancer Support Community, among others, to promote the workshops and to recruit participants. All participants who signed up for RRMI were informed about the study and offered an opportunity to participate. Those who expressed interest were provided more information, including eligibility criteria, as well as other pertinent information about the study, as mentioned above. Study staff were also available to answer questions via email or via telephone. Once all questions were answered to the full satisfaction of the potential participants, and if they still agreed to participate, they were asked to type their name and date of consent in the spaces provided, and check a box on the online consent form to indicate their consent.
Participants who signed the online informed consent form, were asked to complete the CSA (Calender of Study Activities) questionnaire where, among others, they indicated when their workshop will start and when the workshop will end. Based on the information provided, HARIS generated a CSA for each participant. Participants were provided with a schedule of when they were due to complete their baseline, month 1 and month 6 questionnaires. They were also reminded at least 3 times to complete their baseline (pre-intervention), and month 1 and month 6 (post-intervention) questionnaires. Those failing to complete their questionnaires were contacted by the study Research Coordinator to inquire if they needed help completing the questionnaires so assistance could be provided if needed. Participants were free to indicate at any time if they preferred not to answer any questions on the study questionnaires, or not to proceed with the study. Participants needing medical support were referred to their treating physicians or primary care physicians. Those needing psychological support, were provided a toll-free psychological help number to call if they were in distress. Participants were informed to report to study personnel should there be any issues related to their participation in the study. Any issues presented were reported in the event evaluation form and submitted to the Institutional Review Board of the Harvard T.H. Chan School of Public Health. Among other information, this form included space for a description of the issue, a classification of seriousness, and assessment of potential relationship to the intervention. Summaries of non-serious adverse events were submitted to the Institutional Review Board of the Harvard T.H. Chan School of Public Health at least annually at continuing review.
Sample Size and Power Calculation
The primary outcome measure of interest was the Functional Assessment of Chronic Illness Therapy—Spiritual Well-Being Scale (FACIT-Sp) 26 score. Our initial sample size estimation showed that 43 people with cancer would provide 80% power at a two-sided 5% level of significance to detect an effect size of 0.44 point in the change of FACIT-Sp scores between baseline and 6 months after completing a 9-week intervention. 27 This change was observed in a study between groups of cancer patients receiving early palliative care and those not receiving the intervention over a period of 4 months. 27 We expected a dropout rate of 25%. Hence a minimum of 57 participants were needed to ensure that we meet our minimum sample size of 43 participants for this study. Due to high response rate to recruitment efforts, we received IRB approval to enroll more than 57 participants. Data collected from 200 people with various cancer types were used in the study analyses (Figure 1). To avoid multiple testing, analysis of available cases focused on changes observed at the primary timepoint of 6 months. Secondarily, we examined changes observed at 1 month following completion of the RRMI. We also examined the impact of the RRMI on a sub-group of 50 participants with breast cancer at 1 month and at 6 months post-intervention compared to baseline (Figure 1).
The Radical Remission Multimodal Intervention (RRMI)
The RRMI was developed to teach the 9 lifestyle factors from the book Radical Remission 10 to participants living with cancer and to guide them to implement healthful lifestyle changes in their cancer recovery journey. In 2020, as a result of Turner and White’s additional analysis of 500 new RR cases from 2014 to 2020, a 10th lifestyle factor–exercise/movement—was added to the RRMI. 28 However, the 10th lifestyle factor, which is also very important for cancer recovery29,30 was not included in this evaluation because this factor was added after study implementation was initiated. The 9 lifestyle factors evaluated in this study are:
Having strong reasons for living,
Embracing social support,
Using herbs and supplements,
Radically changing your diet,
Releasing suppressed emotions,
Following your intuition,
Increasing positive emotions,
Taking control of your health (a.k.a. empowerment), and
Deepening your spiritual connection.
A summary of the RRMI lifestyle factors, main points, aims, and activities provided by Turner and her coaches are presented in Table 1.
Radical Remission Multimodal Intervention: Lifestyle Factors, Main Points, Aims and Activities.

In general, the RR workshop is offered at a minimum of 10 instructional hours, and typically 1 hour is devoted per module (that is, 1 hour per healing factor, and there are 10 healing factors). Those 10 hours can be offered over the course of 2 weekend days (for example, Saturday and Sunday), often with additional hours of instruction offered before and after each days’ modules in order to allow for introduction time and conclusion/goal-setting time. A typical weekend RR workshop runs from 9 am to 5 pm on Saturday and Sunday. If the RR workshop is offered over 6 weeks, it is typically offered - for example - on Tuesday evenings from 6 to 8 pm over the course of 6 consecutive weeks (for a total of 12 hours of instruction).
RRS: Radical Remission Survivors
Although this factor is not part of the evaluation in this study, it is now an important part of the RRMI lifestyle factors identified by Turner, and thus is added to this table to present the current complete intervention.
The study intervention consisted of the RRMI workshops, offered in English, with a specific curriculum to teach the 9 lifestyle factors. The length of the workshops, conducted either in-person or online (live or pre-recorded), varies (~10-20 hours long) depending on whether they were offered over the weekend, or over a period of 6 or more weeks, with a range of 4 to 150 participants per workshop. The larger workshops were broken into smaller groups during specific sections of the workshop wherein group interaction was encouraged. The 9 lifestyle factors were presented in varying order in each RRMI workshop, as there is no order of importance known at this time to indicate 1 factor being more beneficial than another. The priority of the factors is specific to each individual and where they feel they most need to make changes.8,10,28
The workshops were led by certified RR health coaches. In order to be accepted into the RR Health Coach and Workshop Instructor Training, all applicants must already be licensed psychotherapists, psychologists, doctors, nurses, social workers, mental health counselors, or certified life or health coaches from a program accredited either by the National Board Certified Health & Wellness (NBHWC) or the International Coaching Foundation (ICF). Exceptions are made for individuals with substantial mental health counseling experience (e.g., a pastor with 20 years of experience).
The RR health coaches were trained to present the proprietary workshop slides by Turner and her senior coaches in a 40-hour training program. The program also involves 10 additional hours of practice coaching and studying for the final exam. Coaches were educated on the material as well as on how to facilitate each activity with the intent to help participants create a personal “game plan,” that is, a list of micro-goals in order to implement each factor into daily life after the conclusion of the workshop.
Through social support and group interaction, the coaches led group discussions to encourage the sharing of personal experiences, resources, success stories, and obstacles. Important workshop components included activity worksheets for each lifestyle factor to guide each participant to brainstorm actions for how that particular factor could be implemented. Additionally, a summary “game plan” worksheet was provided and completed during the workshop, where each participant set 1-week, 1-month, 6-month, and 12-month personalized goals to outline action steps to be followed at the end of the workshop. Typically, the trainers do not receive many follow-up questions post-intervention, other than some brief follow-up questions via email.
Training duration, as reported by participants, varied and details are presented in Supplemental Table 1. Overall, 68% of participants completed the intervention (in-person or online) in less than 2 weeks. Given training duration was not normally distributed, and most participants completed the 10-hour intervention in less than 2 weeks, this cut off point (i.e., <2 weeks or ≥2 weeks) was used to include training duration as a bivariate variable in the mixed-effects regression analyses models described below.
Data Collection
Data were collected online and tracked using the Harvard Automated Research Information System (HARIS) administered and managed by Aumtech. 31 HARIS is an automated research tracking system used to track about 1400 participants of the Lifestyle Validation Study at Harvard over a period of 4 years. 32 HARIS and its related website were adapted for use with the current study. It reminded participants to complete all study questionnaires at designated pre-agreed timepoints. At baseline, month 1 and month 6, HARIS automatically emailed reminders as well as provided a link to the questionnaires that were due to be completed at that time point.
Data were collected using the following questionnaires at baseline, and at a minimum of 1 month post-intervention (mean = 62 days; range = 30-165 days) and 6 months post-intervention (mean = 250 days; range = 180-516 days).
Statistical Analysis
Summary statistics including percentages, means, and standard deviations were used to describe the RRMI as reported by study participants (Supplemental Table 1), and to describe participant characteristics, including BMI, cancer diagnosis, and treatments used at baseline, month 1, and month 6 (Table 2). Supplemental Table 2 presents the characteristics of participants with breast cancer using similar summary statistics.
Characteristics of All Cancer Participants in the RRMI Study at Baseline (Pre-Intervention), and at Month 1 and Month 6 (Post-Intervention).

Characteristics of all cancer participants who provided data at month 1 and those who did not were compared using t-tests for continuous and normally distributed variables and Fisher’s exact tests or Chi-square tests for categorical variables (Supplemental Table 3). This analysis was also conducted for participants who provided data at month 6 and those who did not (Supplemental Table 3). As mentioned, the primary QOL outcome measure was the FACIT-Sp scores, while other outcome measures (i.e., FACIT-G, PWB, EWB, SWB, FWB, and FACIT-Sp-12) were secondary. The distributions of the differences and percentage differences in FACIT-Sp and other scores, between month 1 and baseline, as well as between month 6 and baseline, were examined. Wilcoxon signed-rank tests were applied as some of these measures did not follow a normal distribution.
Longitudinal patterns were studied using mixed-effects models. The outcome measures in these models were differences in scores between month 1 and baseline, and between month 6 and baseline. All models included timepoints (month 1 or month 6), training type (online or in-person), adherence score, and interaction between timepoints and adherence score, along with the corresponding baseline scores as fixed effects and participants as random effects. Potential covariates considered were age, BMI, gender (male or female), ethnic group (Non-Hispanic White or Other), education (college and below or above college), living situation (living alone or not living alone), training duration (<2 weeks or ≥2 weeks), country of residence (US or Non-US), use of conventional medicine (yes or no), and use of alternative medicine (yes or no). Those who received both treatments were coded as “yes” within each treatment category, and those did not receive any treatment were coded as “no” within each treatment category. Only covariates that were significantly associated with each outcome measure were included in the final models (Tables 3 and 4). Supplementary models also considered age, BMI and ethnic group, as the published literature suggested their potential association with the QOL scores 38 (Supplementary Table 4). To ensure the validity of the models, residual plot analyses were performed, revealing no major violations of model assumptions. Effect sizes were calculated for the differences and percent differences in the primary QOL outcome measure, FACIT-Sp scores. Similar analyses were conducted on our sub-sample of women with breast cancer (all breast cancer participants were females, as such gender was not included in the model as a covariate) (Table 3).
Facit-Sp Total Score of All Cancer and Breast Cancer Participants at Baseline (Pre-Intervention), and at Month 1 and Month 6 (Post-Intervention).

Unadjusted P-values were from Wilcoxon signed rank test.
Adjusted P-values were from the mixed-effects regression analyses. All mixed-effects models included timepoint (month 1 or month 6 post-intervention), training type (in-person or online), adherence score, adherence score by timepoint interaction, and corresponding baseline measure as fixed effects. Model for emotional well-being also included an additional covariate, living situation (living alone or not living alone), as a fixed effect.
Other Quality of Life Measures of All Cancer Participants at Baseline (Pre-Intervention), and at Month 1 and Month 6 (Post-Intervention).
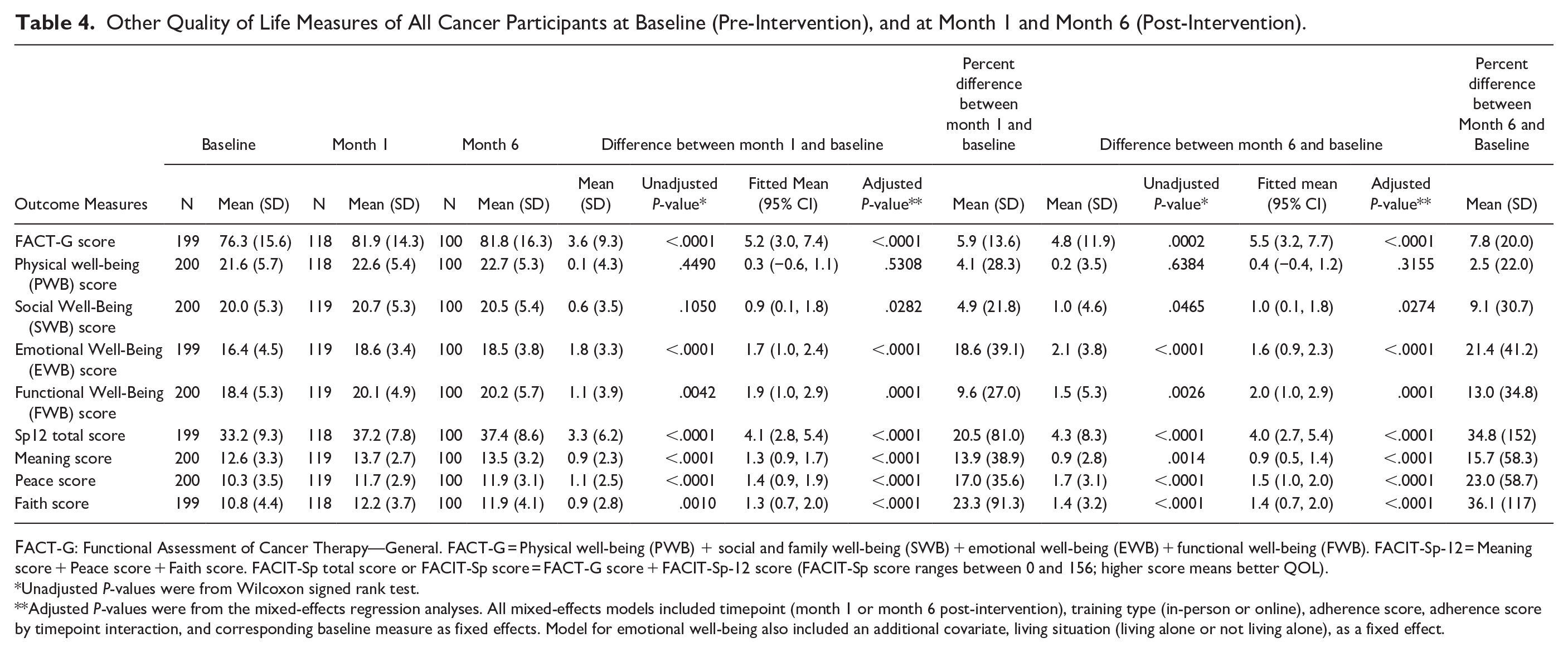
FACT-G: Functional Assessment of Cancer Therapy—General. FACT-G = Physical well-being (PWB) + social and family well-being (SWB) + emotional well-being (EWB) + functional well-being (FWB). FACIT-Sp-12 = Meaning score + Peace score + Faith score. FACIT-Sp total score or FACIT-Sp score = FACT-G score + FACIT-Sp-12 score (FACIT-Sp score ranges between 0 and 156; higher score means better QOL).
Unadjusted P-values were from Wilcoxon signed rank test.
Adjusted P-values were from the mixed-effects regression analyses. All mixed-effects models included timepoint (month 1 or month 6 post-intervention), training type (in-person or online), adherence score, adherence score by timepoint interaction, and corresponding baseline measure as fixed effects. Model for emotional well-being also included an additional covariate, living situation (living alone or not living alone), as a fixed effect.
Two-sided tests with a type I error of 0.05 were used. Since FACIT-Sp scores were the only primary outcome, no multiple comparison adjustment was made. All analyses were conducted using SAS Version 9.4.
Results
Table 2 displays the characteristics of all cancer participants recruited at baseline (pre-intervention), and month 1 and month 6 post-intervention. At baseline, the majority of participants were women (92%), Non-Hispanic White (77%), living in the US (88%), and not living alone (66.5%). The percentage of income < or ≥100 000 USD were similar (37.5% and 37.5%). The mean age ± SD was 55.3 ± 11.5 years, and the mean BMI ± SD was 24.2 ± 4.7. About 50% of the participants had above-college education. A diagnosis of breast cancer was reported by 25% of participants (characteristics of breast cancer participants are presented in Supplemental Table 2). Twenty participants (10.0%) received conventional treatments alone, while 18 (9.0%) received alternative treatment methods alone; 53 (26.5%) participants utilized both treatment methods. The number of participants who completed study questionnaires at month 1 and month 6 were 119 and 100, respectively (Table 2), although not all participants answered every question on the FACIT questionnaires. Characteristics of participants who did not complete month 1 and month 6 questionnaires are shown in Supplemental Table 3. The only significant difference in the distribution of participants across baseline characteristics, between the groups of participants who did and did not provide data (at month 1 and at month 6), was in the type of treatments received, and only between the groups of participants who did and did not complete data at month 1 (Fisher’s exact test; P = .047). Out of a maximum adherence score of 90, the average score ± SD at month 1 was 68.4 ± 20.7 and at month 6 was 72.5 ± 20.0.
On average, all cancer participants had a 7.0 ± 13.1 point improvement (7.7% increase, effect size = 0.53) on FACIT-Sp scores at month 1 and a 9.0 ± 18.6 point improvement (10.8% increase, effect size = 0.48) at month 6, compared with baseline, when unadjusted for other covariates (P < .0001 in both cases) (Table 3). The mixed-effects model regression analyses controlling for baseline FACIT-Sp score, timepoints, training type, adherence score, and timepoints and adherence score interaction, showed similar findings as the unadjusted analyses (Table 3). Although the distribution of participants across treatments received differed between those who did and did not provide data at month 1 (Supplemental Table 3), the use of conventional medicine (yes or no) and use of alternative medicine (yes or no) were not found to be significantly associated with outcome measures of interest. Thus, as mentioned above, these variables, and others found not to be significantly associated with outcomes measures of interest, were excluded from the final models. The improvement in FACIT-Sp scores remained consistent (estimated difference in score between month 1 and baseline = 9.5 (95% confidence interval [CI]: 6.2-12.8; P < .0001) and between month 6 and baseline = 9.7 (95% CI: 6.4-13.0; P < .0001). The improvement did not differ significantly between training types (P = .13; Figure 2). Gender was also found not to have a significant effect (P = .2364).

Boxplot and trajectory of FACIT-Sp* total scores over time by training type.
Breast cancer participants had a 9.2 ± 14.3 point improvement (11.1% increase, effect size = 0.64) on FACIT-Sp scores at month 1 and a 6.7 ± 21.3 point improvement (13.2% increase, effect size = 0.30) at month 6, compared with baseline, when unadjusted for other covariates (P = .0015 and P = .2727, respectively; Table 3). Our final mixed regression models for breast cancer participants showed significant improvements [estimated difference in score between month 1 and baseline = 14.2 (95% confidence interval [CI]: 6.9-21.5; P = .0008) and between month 6 and baseline = 8.4 (95% CI: 1.0-15.9; P = .0287; Table 3].
Furthermore, results from the mixed-effects model regression analyses showed that all QOL measures for all cancer participants were significantly higher at month 1 compared with baseline, except for physical well-being score (P = .53 for physical well-being score, and P < .05 for all other measures; Table 4). Similar findings were observed at month 6 (P = .32 for physical well-being score, and P < .05 for all other measures). The percentage increase in QOL scores ranged from 2.5% (for physical well-being) to 36% (for Faith score) at month 6 compared with baseline. Additionally, emotional well-being score increased by 21.4% (<0.0001) at month 6 compared with baseline.
The living situation was significantly associated with the emotional well-being score: participants living with a partner, family member, or pet had an average change in FACIT-Sp score of 1.5 points higher than those living alone (P = .0087).
Figure 3 illustrates the relationship between the change in FACIT-Sp scores from baseline and adherence scores at both month 1 and month 6.

The relationship between adherence scores and changes from baseline (pre-intervention) in FACIT-Sp* scores, at month 1 and month 6 (post-intervention), by training type.
At month 1, adherence score did not appear to be associated with the change in FACIT-Sp scores for both training types (i.e., in-person and online). However, by month 6, participants with higher adherence scores had a greater change in FACIT-Sp scores (P = .0002 for the main effect of adherence score; and P = .0003 for the interaction term between adherence score and timepoint). These effects were consistent across training types.
Supplemental Table 4 shows the results from models that also included age, ethnic group and BMI as covariates. These 3 covariates were not associated with changes of any QOL scores.
Discussion
This study found that the RRMI workshops were successful in improving the QOL of adult participants with cancer. The primary QOL outcome scores increased significantly from baseline by 7.7% at month 1 and remained significant at month 6 with an increase from baseline of 10.8%. The QOL sub-domain measures of social and family well-being, emotional well-being, and functional well-being all showed significant improvements, while the physical well-being measure did not. Additionally, the sub-measures of meaning, peace, and faith were all significantly higher at month1 and month 6, compared with baseline. Changes in QOL over time were independent of gender, ethnicity, BMI, and age
At month 1, the effect size of the difference is medium for all cancer participants (0.53) and for breast cancer participants (0.64). Our initial sample size estimation was to detect an effect size of 0.44 points in the change of FACIT-Sp scores between baseline and 6 months. The observed effect size for all cancer participants at month 6 is 0.48, slightly larger than 0.44. However, for breast cancer participants, we did not have a large enough sample size, and the effect size is small (0.31), which can be noted as a limitation.
Findings from this study suggest that a safe, low-cost, and relatively easy to implement intervention such as the RRMI has the potential to significantly improve the QOL of individuals with cancer. Higher QOL is associated with improved well-being and cancer prognoses, including decreased side effects,21,22 decreased morbidity, 23 and increased lifespan. 23 Cancer survivors generally report having more comorbid conditions, higher physical symptom burden, especially fatigue, insomnia and pain, compared with the general population. 39
In addition, individuals with cancer often experience higher levels of psychological distress.11,40,41 Negative emotions experienced by them include fear (e.g., of dying and recurrence), trauma, anxiety, grief, worry, hopelessness/helplessness, and a loss of peace.24,40,42 -45 Such conditions of stress have been shown to weaken the immune system’s response to cancer in various studies. 41 In general, these conditions of stress are detrimental to the conditions that need to prevail for cancer patients to heal. Stressful life events, including increased financial burdens, 15 and their related emotional responses, are most likely to result in detrimental long-term or permanent changes in several factors, including emotional well-being (e.g., increased anxiety and depression symptoms)44,46; physiological well-being (e.g., hormonal imbalances, digestive issues, and continued immune suppression; decreased apoptosis, decreased enzymes that degrade chemical carcinogens, and reduced ability to repair cellular DNA).45,47,48 Changes in behavior (e.g., greater alcohol and tobacco consumption, lower physical activity levels as well as poorer dietary and sleep quality) are also observed in cancer patients.46,49,50 The RRMI raises participants’ awareness to the role of stress in impeding disease recovery. It provides ways in which cancer patients can recognize, accept and manage their stress, so healing or disease recovery can occur.10,28
The RRMI significantly increased cancer participants’ emotional well-being at month 6 compared with baseline. This finding suggests that the information and tools provided by the RRMI and introduced to cancer participants with the aim of helping to improve emotional well-being (Table 1) are likely to have a positive impact. In addition to increased emotional well-being associated with the RRMI, our current findings indicate that not living alone (including living with pets), is associated with higher emotional well-being as compared with living alone. Furthermore, the significant increase in social and family well-being at month 6 compared with baseline also appears to reflect a positive influence of the RRMI’s approach in helping all cancer participants recognize the importance of social support (Table 1). Companionship and social support are critical contributors to higher emotional and social well-being. After cancer diagnosis, larger social networks and greater social support/integration have been related to higher QOL, 51 while socially isolated individuals experience increased risk of all-cause and cancer mortality. 52
Meaning, peace, and faith scores were also significantly increased at month 6 compared with baseline. The tools provided by the RRMI in these areas (Table 1) also appear to improve the meaning, peace and faith scores. This is of particular importance, given that a cancer diagnosis may threaten people’s sense of meaning in life and affect their life purpose and priorities. 53 Regaining or discovering their meaning in life, and accepting their disease, have been shown to improve individuals’ cancer coping strategies and psychological well-being. 54 Sense of peace is also strongly associated with mental health. 55 Increased sense of peace, that is, reduced stress, also triggers healing. 56
There is substantial evidence that links greater spiritual well-being with better health outcomes, and ability to cope with illness, including terminal illness.23,37 Low spiritual well-being in people with cancer has been associated with worse physical and mental health, among other dysfunctions.37,57 High spiritual well-being is positively correlated with fighting spirit and negatively correlated with feelings of helplessness/hopelessness. 37 Given that the RRMI showed significant increases in FACIT-Sp and FACIT-Sp-12 scores at month 6 compared with baseline, it is likely that RRMI participants find hope, along with a reawakening of their fighting spirit, to commit to living. These attributes have been reported to improve QOL, and extend the lifespan of cancer patients.58 -60
A cancer diagnosis can make it difficult for individuals to feel that they have control over their lives.61,62 The RRMI empowers people to be active in taking responsibility for all aspects of their lives, and to include their intuition in their decision-making processes (Table 1). These are key RRMI lifestyle factors, and are likely contributing factors toward the increased QOL observed in this study.
The use of herbs and nutritional supplements is also a RRMI lifestyle factor. Turner and White identified 3 main categories of supplements that RR survivors reported they took: immune-boosting, detoxifying, and those improving digestion and absorption of nutrients. 28 Herbal and nutritional supplements are widely used among cancer patients.62,63 RRMI participants are advised to take supplements only under the guidance of trained licensed health professionals. Additionally, RR survivors consistently reported increased intake of organic vegetables and fruits, and reduced intake of processed meats, red meat, and added sugars. 28 Making such dietary changes is also an important RRMI lifestyle factor. These dietary patterns are recommended by the American Cancer Society, the World Cancer Research Fund/American Institute for Cancer Research, and the American College of Lifestyle Medicine.64,65 A predominantly plant-based dietary pattern is high in fiber, dense in essential nutrients, rich in bioactive compounds66,67 with various anti-cancer properties, 68 and has been shown to improve QOL. 69 Further, organically grown foods have also been reported to have higher concentrations of antioxidants and lower incidence of pesticide residues than conventionally grown foods. 70 The RRMI also emphasized the importance of working with licensed practitioners to identify foods that may trigger adverse reactions due to food sensitivities or intolerances.28,71
A significant greater change in FACT-Sp scores was observed with increased adherence scores at month 6, compared with month 1 (Figure 3). This suggests that a greater improvement on participants’ QOL is observed when the information and tools provided in all the RRMI modules (Table 1) were more actively practiced for at least 6 months. Disease recovery takes time. The consistent implementation of the RRMI key lifestyle factors (daily, and/or on a regular basis) over time is likely to start transforming a person’s mindset to promote mental, spiritual and overall health. These outcomes have been reported by RR survivors 72 who were highly committed to making these lifestyle changes.10,28,72
Current findings suggest that the RRMI may play an important role in improving QOL. Its incorporation as part of routine cancer care has the potential to safely complement standard oncological treatment, supporting improved health outcomes, increasing survival time, and reducing health care costs. 73 Contrary to expectations, our findings show no significant difference in outcomes when the RRMI workshops were attended online or in-person. Therefore, individuals with a broadband internet connection can potentially reap benefits even if their health or social circumstances limit their ability to attend in-person sessions. This means that the RRMI has the potential to influence cancer care across distances, at relatively low cost, giving hope and support to people newly diagnosed with cancer, as well as those living with cancer chronically and cancer survivors.
This study has limitations due to the use of a convenience sample that was not randomized into intervention and control groups, combining cancer types, lack of control for disease stage and progression, and does not provide long-term evaluation of the effects. Participants who chose not to participate for any reason, such as the cost of the intervention, lack of time or support from family members, and poor health, are not represented in this study. Hence, findings on the impact of the intervention on our outcome measures of interest cannot be attributed solely to the intervention, and thus cannot be considered conclusive. Additionally, they cannot be generalized to all cancer populations. However, the lifestyle factors identified are known to prevent, slow, halt, and reverse multiple chronic diseases such as diabetes, and cardiovascular disease,65,74 -80 including cancer,4,78,81,82 promoting disease recovery. Hence, they are likely to be generally beneficial in most disease states. Despite these limitations, this study provides valuable preliminary information on the impact of the RRMI on participants’ QOL, and data obtained serves as an important foundation for further research. This study’s findings are critical for the development of an intervention that can be tested in a fully powered randomized clinical trial that is able to control for cancer type and stage.
Conclusion
The pre-post RRMI study was found to improve the overall QOL of cancer participants at month 1 post-intervention. This improvement in QOL was maintained at month 6 post-intervention. Given improved QOL contributes to enhanced health outcomes and overall well-being, including decreased treatment side effects and increased survival time, our findings suggest that individuals with cancer can benefit from the RRMI.
Supplemental Material
sj-docx-1-ict-10.1177_15347354241293197 – Supplemental material for Effect of the Radical Remission Multimodal Intervention on Quality of Life of People with Cancer
Supplemental material, sj-docx-1-ict-10.1177_15347354241293197 for Effect of the Radical Remission Multimodal Intervention on Quality of Life of People with Cancer by Junaidah B. Barnett, George C. Wang, Wu Zeng, Ruth W. Kimokoti, Teresa T. Fung, Yuan H. Chen, Jerry Kantor, Wei Wang and Michelle D. Holmes in Integrative Cancer Therapies
Footnotes
Acknowledgements
The authors wish to recognize the following for their significant contributions to this important work:
All participants, who volunteered to participate in this study, in hope of helping others with cancer to better navigate their cancer recovery journey
Dr. Kelly Turner and her staff, (the late) Ms. Tara Flanagan Koening, Ms. Sarah Weldy, and Ms. Jess Hershey, Radical Remission Foundation, for assistance with study recruitment and follow-up of participants
Radical Remission health coaches for their role in conducting the RRMI, and recruiting study participants
Dr. Kelly Turner for providing ![]() , and review of manuscript to ensure all information provided regarding the RRMI are correct
, and review of manuscript to ensure all information provided regarding the RRMI are correct
Mr. Madhav Bidhe, Aumtech, Inc, for providing use of HARIS for the study, and it’s management by his staff without charge. Mr. Murali Sounderarjan, Aumtech, Inc, for adapting HARIS for this study, and helping manage online study data collection
Ms. Yueming Liu, Department of Statistics, Northwestern University, for her data analysis of the QOL data under the supervision of Dr. Wu Zeng
Dr. Maryam S. Farvid, Nutrition and Food Studies, George Mason University, for her review of the manuscript and critical input
All study team members who volunteered their time and expertise to ensure the high quality of this work
Author Contributions
JBB, GCW, MDH, WW, and WZ were responsible for conceptualizing and designing the evaluation component of the study. JBB oversaw and guided data collection, with inputs from other authors. RWK assisted with participant follow-up and data collection. WW, WZ and YHC conducted data cleaning, preliminary and final analyses, with input from all authors. JBB drafted the manuscript. All authors (JBB, GCW, WZ, RWK, TTF, JK, YHC, WW, and MDH) were responsible for the interpretation of data, critical review of the manuscript, and approval of the final manuscript for submission.
Data Availability Statement
The raw data supporting the conclusion of this article will be made available by the authors, without undue reservation.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was conducted through the voluntary contribution of all authors. Funding for data cleaning, preliminary and final data analyses was provided to WW and YC by the Radical Remission Foundation. Funding for publication of this article was also provided by the Radical Remission Foundation. Other contributions by the Radical Remission Foundation to this work are described in the ACKNOWLEDGMENTS section.
Ethics Statement
The study protocol was reviewed and approved by the Institutional Review Board of the Harvard T.H. Chan School of Public Health. The participants provided their written informed consent to participate in this study.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.