
Abstract
PROSPERO registration: CRD42023459
Introduction
Lung cancer is the second most common cancer worldwide 1 and has the highest mortality rate, accounting for 18 584 (22.3%) of the 83 378 deaths from cancer in Korea in 2022. 2 With recent advances in early detection and surgical treatment, the 5-year relative survival rate of patients with localized lung cancer has increased to 62.8%; however, in the case of regional and distant metastases, the survival rate has decreased to 34.8% and 8.2%, respectively. 3
The use of immune checkpoint inhibitors (ICIs) has significantly altered the therapeutic landscape for advanced non-small cell lung cancer (NSCLC) by targeting the immune system. However, most lung cancer patients experience either primary or acquired resistance, which can lead to reduced responsiveness to ICIs or tumor progression during immunotherapy.
Not only do tumor-intrinsic mechanisms play a major role in immunotherapy resistance, but the immunosuppressive tumor microenvironment (TME) is also a critical factor. 4
In cancer, the antitumor immune response, known as immunosurveillance, is interfered with by tumor cells themselves or by the immunosuppressive TME. Accumulation of proinflammatory cytokines and immunosuppressive cells, loss of tumor antigens, and complement sensitivity can impair immune function against cancer. 5 Immunoregulatory cells, such as tumor-associated macrophages and regulatory T cells (Tregs) suppress the function of T cells and are negatively correlated with clinical outcomes. 6 Furthermore, resistance to chemotherapy may be exacerbated by its immunosuppressive adverse effects, including the elevation of inflammatory mediators and tumor-promoting M2 macrophages, as well as the genetic diversity of cancer cells.7,8 Given the importance of preserving immune function and reducing the side effects of conventional cancer therapy, it is critical to explore the potential of herbal medicine (HM) as an adjunct immunotherapy. 9
HMs are widely used in East Asian countries and are known for their potential to enhance immune function, improve quality of life, and alleviate clinical symptoms in cancer patients. 10 Particularly for NSCLC, which accounts for more than three-quarters of all lung cancers. 2 Many systematic reviews and meta-analyses of clinical trials have been conducted on the effectiveness of combining HM with standard cancer therapies.11 -13 For instance, a meta-analysis showed that HM in combination with chemotherapy can increase the percentages of CD3+, CD4+, and NK cells and the CD4+/CD8+ ratio in patients with advanced NSCLC. 14 Ongoing clinical trials are being conducted on the efficacy of HM in enhancing the effect of ICIs and reducing ICI-related adverse effects. 15
However, there is a need to explore the immunological effects of HM alone, as most existing studies have focused on combined treatments. Therefore, our study aimed to investigate the immunological effects of HM alone, independent of conventional cancer therapies, in patients with NSCLC.
Methods
Study Registration
This review’s protocol was registered in PROSPERO (registration number CRD42023459904).
We conducted a systematic review according to this protocol, and the dates, changes, and rationale for each amendment were tracked using PROSPERO if no protocol amendments were made.
Search Method for Identifying the Studies
The following 8 electronic databases were searched in March 2023: MEDLINE via PubMed, EMBASE via Elsevier, Cochrane Central Register of Controlled Trials, China National Knowledge Infrastructure (CNKI), CINII, and Korean databases, including RISS, ScienceON, and Oriental Medicine Advanced Searching Integrated System (OASIS). The reference lists of the retrieved articles were manually searched and previous review articles were examined. No restrictions were imposed on the year or language of reviewed publications.
The search strategy for MEDLINE is shown in Supplemental File 1 and was modified in a manner similar to that for other databases. All lung cancers were evaluated for sensitivity and a final selection was performed.
Inclusion Criteria for This Review
Types of studies
This systematic review included RCTs that evaluated the effectiveness of HMs on immune function in patients with NSCLC. Studies with other designs, such as observational studies, cohort studies, case reports, case series, non-RCTs, and animal and experimental studies, were excluded.
Types of participants
Patients with NSCLC were included in this review regardless of sex, age, or cancer stage.
Types of interventions
Studies involving herbal injections and oral (eg, decoctions, tablets, pills, or powders) administration of HMs, such as single herbs, herbal extracts, and multi-herbal formulations, were included in this review. RCTs in which other interventions (eg, chemotherapy, radiotherapy, targeted therapy, and hormone therapy) were administered to all groups using the same protocol were excluded. Studies in which HMs were used in combination with other interventions were excluded.
There were no restrictions on the comparisons. Placebo, active control, no-treatment, and wait-list control groups were used as the control groups.
Type of outcome measures
The following outcomes related to immune functions were included in this review: CD3+, CD4+, CD8+, CD4+/CD8+ ratio, IL-1, IL-6, tumor necrosis factor (TNF)-a, Th17, and Treg. However, RCTs that did not report the measured values before and after treatment were excluded.
Data Collection, Extraction, and Assessment
Selection of studies
Two authors (YC and H-EJ) independently screened the titles and abstracts of the studies retrieved from the databases after excluding duplicate articles. The full texts of the selected articles were reviewed to ensure that each met the inclusion criteria. Finally, a third reviewer (SJ) provided a decisive factor if the 2 authors had differing opinions.
Data extraction
Two authors (YC and S-DK) extracted the data and a third author (M-KJ) reviewed the extracted data. The essential information for each article was summarized, including the title, first author, year of publication, journal, study period, participants, interventions, comparisons, outcomes, results, and adverse events.
Assessment of risk of bias
Two reviewers (YC and S-DK) assessed the quality of the included studies using the Cochrane library risk of bias (RoB) tool 1.0. RoB was assessed using the following 7 items: (1) random sequence generation, (2) allocation concealment, (3) blinding of participants and personnel, (4) blinding of outcome assessment, (5) completeness of outcome data, (6) completeness of reporting, and (7) other sources of bias. In each RCT, items were categorized as “high risk (H),” “unclear (U),” or “low risk (L).” In addition, an RoB graph was generated using Review Manager (Cochrane Collaboration Software, RevMan), version 5.4.1 for Windows (Copenhagen, The Nordic Cochrane Centre, the Cochrane Collaboration, 2012).
Data Synthesis and Statistical Analysis
Differences between the intervention and control groups were assessed using a meta-analysis. Mean differences (MDs) with 95% confidence intervals (CIs) were used to measure the treatment effects for continuous data. In addition, we converted the other forms of data into MDs. The heterogeneity of the effect measures between studies was assessed using the I-squared statistic (I2). All statistical analyses were conducted using RevMan version 5.4.1. We contacted the corresponding authors of studies with missing information to acquire and verify the data whenever possible. We pooled the data across the studies to conduct a meta-analysis using random effects. Publication bias was assessed using funnel plots when the number of included studies was greater than ten. When reporting bias was implied by funnel plot asymmetry, the authors attempted to explain possible reasons.
Ethical Statement and Competing Interests
All the data were collected from published trials; therefore, ethical approval was not required. The authors declare no conflicts of interest.
Results
Study Selection
We scanned 8 online databases, which initially identified 336 research papers published before April 2023. After excluding 45 duplicates, the abstracts of the remaining 291 studies were reviewed. This process led to a further reduction, excluding 274 articles and retaining 17 articles for a detailed reading. Using the established selection criteria in PROSPERO, 12 studies were excluded for the following reasons: 11 studies reported inappropriate outcomes and 1 study used a combined intervention. Ultimately, we included 5 RCTs (Figure 1). Newly published RCTs between April 2023 and December 2023 were also screened for additional research but were excluded from this review according to the inclusion criteria.

PRISMA 2020 flow diagram for new systematic reviews which included searches of databases and registers only.
Study Characteristics
This meta-analysis included 5 RCTs with 610 individuals diagnosed with NSCLC and TNM stages ranging from stage IIIa to IV. While the experimental groups received HM treatments, the control groups were treated with conventional chemotherapy, megestrol acetate, regular examinations, placebo, or symptomatic treatments. The treatment durations varied across these studies, as presented in Table 1. This study primarily assessed the immune marker expression.
Basic Information of the Included Trials.

Abbreviations: NSCLC, non-small cell lung cancer; I, intervention group; C, control group; NR, not recorded.
Risk of Bias in Included Trials
Using the Cochrane risk of bias assessment, the studies in this review demonstrated a high risk of bias owing to inadequate methodological descriptions (Figure 2). All studies employed appropriate random sequence generation.16 -20 However, 3 trials did not provide details on allocation concealment, resulting in an uncertain risk of bias evaluation.16,17,20 With the exception of 1 study that used a placebo, 19 performance bias was considered high in 4 studies16 -18,20 and detection bias was viewed as high in all studies because HM was administered exclusively to the experimental group. Due to the absence of accessible registered protocols, all studies had an unclear risk of reporting bias. All studies had a low risk of attrition and other potential biases considering funding sources, conflicts of interest, and ethical issues (Figure 3).

Risk of bias graph.
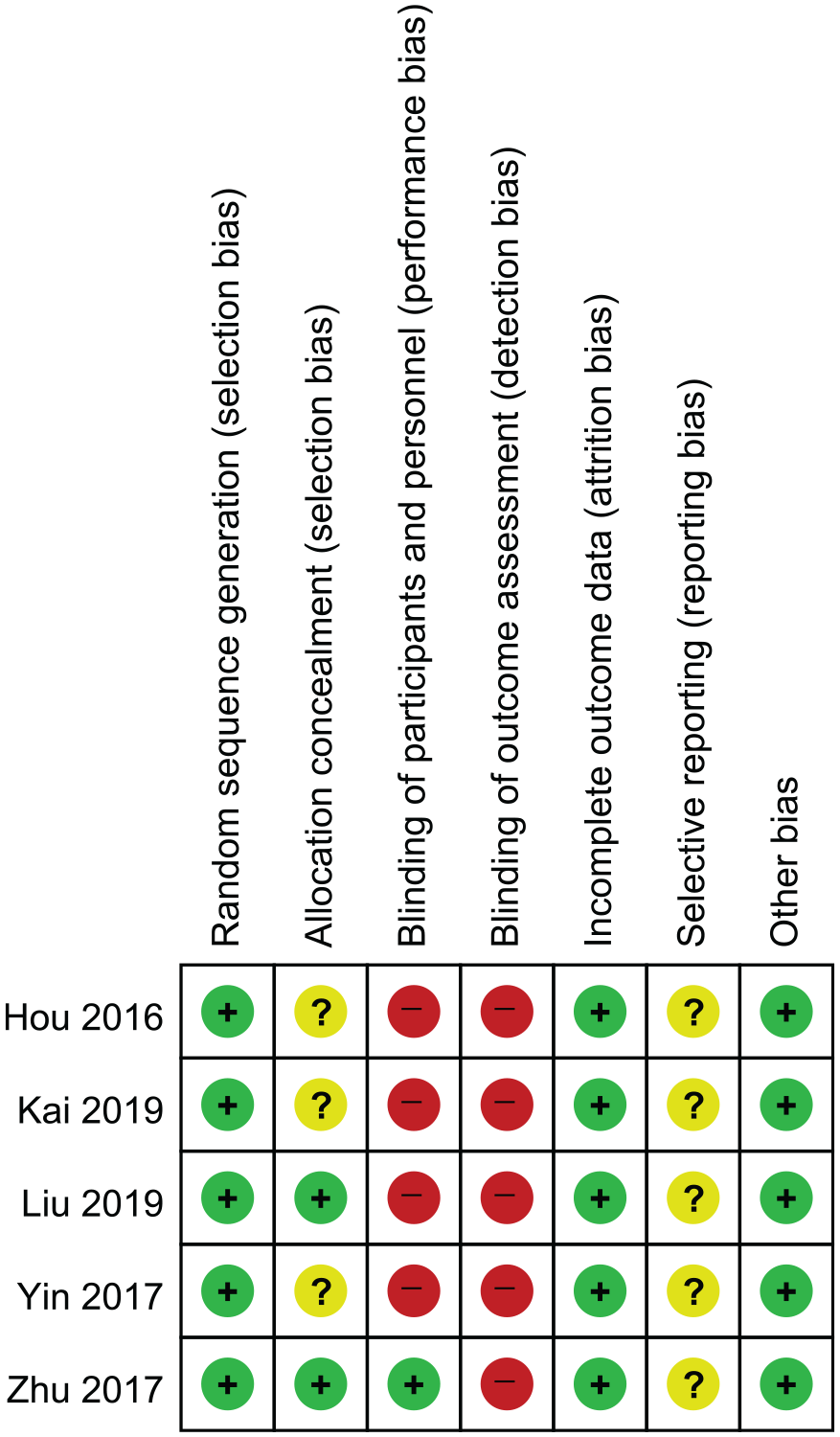
Risk of bias summary.
Immunological Effects of Herbal Medicine in the Peripheral Blood of Patients With NSCLC
CD4+ levels
Three RCTs examined the effect of HM on CD4+ cell counts in patients with NSCLC.16,18,20 Combined data from these studies revealed a marked increase in CD4+ cell counts in patients receiving HM. This difference was significant, as indicated by an MD of 5.27 (95% CI [3.26, 7.27], I 2 = 61%, P < .001, n = 428; Figure 4A).

Comparative analysis. (A) Effects of HM on CD4+ levels in patients with NSCLC. (B) Effects of HM on CD8+ levels in patients with NSCLC and (C) Effects of HM on CD4+/CD8+ ratio in patients with NSCLC.
CD8+ levels
Three RCTs have examined the influence of HM on CD8+ counts in patients with NSCLC.16,18,20 A combined analysis from these studies showed that HM treatment did not significantly increase CD8+ counts, with an MD of −3.04 (95% CI [−5.80, −0.29], I 2 = 74%, P = .03, n = 428, Figure 4B).
CD4+/CD8+ ratio
Only two RCTs examined the impact of HM on the CD4+/CD8+ ratio in patients with NSCLC.16,18 Combined data from these studies showed a statistically significant improvement in the CD4+/CD8+ ratio in patients receiving HM with an MD of 0.22 (95% CI [0.18, 0.26]; I 2 = 0%; P < .001; n = 278; Figure 4C).
CD3+ levels
A single RCT investigated the effects of HM on CD3+ levels in patients with NSCLC. 16 The study demonstrated a statistically significant improvement in CD3+ levels in patients treated with HM, as evidenced by an MD of 10.60 (95% CI [7.22, 13.98], P < .001) (Table 2).
Effects of Herbal Medicines on Immune Markers Except for CD4+ and CD8+ in Included Trials.

Cytokines: IL-1, IL-6, and TNF-a
A solitary RCT delved into the impact of HM on the cytokine levels of interleukin (IL)-1, IL-6, and TNF-a in patients with NSCLC. 17 The results revealed that HM significantly reduced the levels of these cytokines. Specifically, IL-1 levels decreased with an MD of −9.15 (95% CI [−9.80, −8.50], P < .001). Similarly, IL-6 levels showed a decrease with an MD of −7.37 (95% CI [−8.07, −6.67], P < .001). TNF-a levels also exhibited a notable reduction with an MD of −3.71 (95% CI [−4.14, −3.28], P < .001) (Table 2).
Treg, Th17 levels, and Th17/Treg ratios
In a single RCT, 19 the effects of HM on Treg and Th17 levels as well as Th17/Treg ratios in patients with NSCLC were examined. The study revealed a significant decrease in Treg levels with an MD of −1.59 (95% CI: [−2.56, −0.62], P = .001). Conversely, Th17 levels increased (MD, 0.29 (95% CI, [0.21, 0.37]; P < .001). Additionally, there was a noticeable rise in the Th17/Treg ratios, demonstrated by an MD of 0.07 (95% CI: [0.04, 0.10], P < .001) (Table 2).
CD28, CD152, CD80, and CD86
In an RCT, 20 researchers investigated the effects of HM on the expression levels of the immune markers CD28, CD152, CD80, and CD86 in patients with NSCLC. The results showed a statistically significant increase in CD28 levels (MD 1.50, 95% CI [0.09, 2.91], P = .04) and a significant decrease in CD152 levels (MD −1.50, 95% CI [−2.44, −0.56], P = .002). However, changes in CD80 (MD −0.70, 95% CI [−1.65, 0.25], P = .15) and CD86 (MD 0.20, 95% CI [−0.57, 0.97], P = .61) levels were not statistically significant (Table 2). These findings suggest that HM may modulate specific immune markers in patients with NSCLC; however, further research is needed to determine their clinical implications.
HM Components
All 5RCTs included in this review used different HMs. 21 The commonly used herbs were Atractylodes macrocephala Koidzumi (4 of 5), Astragalus membranaceus Bunge, Poria cocos (3 of 5), and Codonopsis pilosulae (Franch.) Nannf., Citrus unshiu Markovich, Coix lacryma-jobi Linné var Pinellia ternata Breitenbach, Cornus officinalis Siebold et Zuccarini, and Glycyrrhiza uralensis Fischer (2 of 5) (Table 3).
Compositions of Herbal Medicine Used in Included Trials.

Herbal medicines commonly used in RCTs.
The amount of each component is not recorded in the article.
Publication Bias
Publication bias was not assessed because the number of included studies was 5, which is less than 10.
Discussion
The symptoms of lung cancer are similar to those of the common cold, such as cough and phlegm; therefore, patients with lung cancer are often found in an advanced state. 3 Targeting the immune system has become a crucial approach in cancer treatment. Tumors can escape the immune response by changing tumor antigens, inhibiting T cell expansion, and taking advantage of immunosuppression. 5
As ICIs have become a major standard therapy for advanced NSCLC, numerous studies have been undertaken to predict ICI response and assess patients’ immune function. 4 Especially, immune profiling in peripheral blood is a minimally invasive method with significant potential to predict treatment outcomes after immune-based therapies. Increasing evidence suggests that circulating immune cells and soluble factors in the peripheral blood of patients may reflect some parts of the immune landscape in the tumor environment as well as the dynamic changes in systemic immunity.22 -24 T lymphocytes and their related cytokines play a pivotal role in controlling tumor growth and immune response.10,25,26 Although tumor-specific cytotoxic T cells act as direct attackers against the tumor, CD4 T cells function as coordinators, differentiating into various subsets that can either promote tumor regression through mechanisms such as secreting proinflammatory cytokines like IL-2 and IFN-γ and enhancing tumor-specific CD8+ T cell function or promote tumor growth by secreting immunosuppressive cytokines such as TGF-β and IL-10.27 -29
The principle of enhancing immune function in patients with cancer has long been prioritized in traditional Eastern medicine. 14 Recent preclinical studies have extensively investigated the immunological properties of HMs, focusing on their effects on immunosuppressive TME.30,31 Therefore, we systematically reviewed clinical trials to assess the immunological effects of HM on immune function in patients with NSCLC.
In this study, 3 RCTs showed a marked elevation in CD4+ counts but a decrease in CD8+ counts in patients with NSCLC receiving HM. A comparative analysis of these studies revealed a statistically significant increase in the CD4+/CD8+ ratio in the HM treatment groups. Besides the stimulus signals from dendritic cells, help signals from CD4+ T cells are essential for cytotoxic T lymphocyte (CTL) priming. 10
In cell-mediated immunity, dendritic cells present tumor antigens to naïve helper T cells via major histocompatibility complex class (MHC) II molecules and activate type 1 T helper cells (Th1) to secrete IL-2, which activates CD8+ T cells and their proliferation. In addition, Th1 cells upregulate NK and B cell activation to further strengthen antitumor immune responses. 29
Although CD8+ counts decreased in the HM treatment groups, help from CD4+ T cells and the CD4+/CD8+ ratio are critical for optimal CTL function in patients with cancer. 26 In addition, peripheral-activated CD4+ T cells play a major role in systemic immunity that drives tumor rejection. 22 Tumor-specific CD4 T cells collaborate with macrophages and play a major role in cancer immunosurveillance via the release of IFN-γ. 28 Hakim et al reported that CD4+ T cells are especially slow to recover to normal levels following chemotherapeutic treatments. 32 In a cohort study, a high CD4+/CD8+ ratio showed positive relevance in predicting tumor response and overall survival in patients undergoing ICI therapy. 33 The relatively low number of Th1-type CD4+ T cells with reversed CD4/CD8 ratios showed significantly low clinical outcomes in patients with cervical carcinoma. 34 Hence, there is increasing evidence that circulating T cell subsets are correlated with tumor response and survival in cancer patients. 35
In Yin et al, 19 Tregs significantly decreased, while the Th17 and the Th17/Treg ratio increased in the HM treatment group. Th17 cells are a subset of CD4+ T lymphocytes that induce neutropenic reactions to kill extracellular pathogens by secreting IL-17. 36 Although there is a contradictory role of Th17 cells secreting IL-17 and IL-22 in cancer, 37 Th17 cells are vital for promoting inflammatory response and mediating tumor regression in immunotherapy. 38 Tregs are a subset of CD4+ T cells that are required for self-tolerance and defense against autoimmunity but are often correlated with cancer development and metastasis. 39 Tregs located in the TME mediate immunosuppression by releasing cytokines such as TGF-β and IL-10. 28 Higher levels of Tregs are suggested to decrease the survival of patients with cancer. 30 The functional balance between those T helper subsets is crucial in treating cancer. 38 Tregs and Th17 cells modulate the inflammatory immune response in lung cancer, and restoring an adequate cytokine balance and Th17/Treg ratio may help to achieve a better clinical response in lung cancer. 40
Wang et al 17 measured cytokine levels of patients with stage IV NSCLC complicated with cachexia and showed decreased levels of IL-1, IL-6, and TNF-a in the HM group. Upon exposure to inflammatory stimuli, TNF-a as well as IL-1 are produced mainly by activated macrophages which attract and activate neutrophils and monocytes to the tumor site. 41 However, beyond the antitumor effect of cytokines, there is a dark side that TNF-α is involved in pathological processes such as chronic inflammation in adipose tissue and cancer cachexia. 42 Tumors overexpressing TNF-a, IL-1, and IL-6 exhibit severe weight loss and muscle atrophy, ultimately leading to aggressive tumor progression. 43 In addition, IL-6 came out to be an independent predictive factor for survival in patients with cancer. 27 Moreover, a strong association between inflammation and cancer is reflected by high levels of IL-6 in TME via regulating multiple signaling pathways including anti-apoptotic, pro-survival, and metabolism in cancer. 24
T-cell activity relies on their signaling interactions with antigen-presenting cells (APCs), involving molecules such as CD28 and CD152. 9 Zhu et al 20 showed that HM has a certain immunological effect in Qi- and Yin-deficient patients with NSCLC. HM significantly increased CD28 levels and reduced CD152 levels. In addition to MHC and T cell receptor interactions, a co-stimulatory signal is required to activate T lymphocytes. When CD80 or CD86 from APCs bind to CD28 on T cells, T cells become activated and are capable of killing infected and tumor cells. In contrast, binding to CD152 expressed on activated T cells transmits an inhibitory signal, which downregulates T cell activation. 44 When activated B cells or dendritic cells express high levels of CD80 and CD86, these molecules provide co-stimulatory signals to T cells through their interaction with CD28, enhancing T cell activation. 20
One of the most commonly used herbs in our study was Astragalus membranaceus, which contains more than 100 compounds, including flavonoids, saponins, polysaccharides, and amino acids. It is used as an immune stimulant, tonic, antioxidant, hepatoprotectant, diuretic, antidiabetic, and anticancer medication. 45 Astragalus membranaceus is one of the most commonly used herbs for NSCLC according to several systematic reviews and meta-analyses. A meta-analysis of 19 clinical trials showed the effectiveness of Astragalus-containing HM in improving tumor response and Karnofsky performance scores.46,47 Its main component, Astragalus, has been shown in ex vivo experiments to enhance T cell-mediated immune responses for anticancer therapy in NSCLC via M1 polarization of macrophages and the functional maturation of dendritic cells. 48 Additionally, Astragalus polysaccharides promotes the differentiation and maturation of peripheral dendritic cells (DCs) and enhances their function, as well as the functions of NK cells and lymphokine-activated killer cells. 49
Codonopsis pilosula enhances immunity, microcirculation, and hematopoietic functions. Additionally, a randomized, double-blind, placebo-controlled study showed that a herbal complex with Codonopsis pilosula and Angelica sinensis alleviated immune impairment in patients with breast cancer who had undergone leukopenia and decreased T cell levels during chemotherapy or radiotherapy. 50 Mixed polysaccharide fractions from the root of Astragalus membranaceus and Codonopsis pilosula ex vivo enhanced the efficiency of a DC-based vaccine against metastasis of mammary carcinoma in mice, following enhanced CD4+ and CD8+ T cell proliferation and augmented expression of CD40, CD80, and CD86 markers in DCs. 51
Another commonly used herb, Atractylodes macrocephala, stimulates antibody production, lymphocyte proliferation, and cytokine secretion in mouse splenocytes. Particularly, it induced better stimulation of Th1 type than Th2 type T lymphocytes. 52 Atractylodes polysaccharide, a major component of Atractylodes macrocephala, may increase immune response by stimulating toll-like receptor 4 pathway and enhancing cytokine secretion such as IL-2, IL-4, and IFN-γ. 53
Poria cocos extract plays beneficial roles in NK cell activity and stimulates IFN-γ secretion without immunotoxic effects. Purified lanostane triterpenoids suppress the Th2 immune response by IL-4 and IL-5 inhibition. 54 Ginseng saponins used by Wu et al 55 elevated the differentiation of naive T cells into Th1 cells by activating DCs.
In addition, a well-known herbal formula, Bojungikki-Tang, which includes Astragalus membranaceus and Atractylodes macrocephala, synergistically enhances the antitumor effects of an anti-PD-1 antibody by regulating various immune factors in the immunosuppressive microenvironment.56,57 HM consisting of Atractylodes macrocephala and Poria cocos reduces cancer-related cachexia symptoms by reducing serum IL-6 levels and inhibiting MAPK/NF-kB activation. 58 Feiyanning formula, which has been used to treat NSCLC for decades in China and studied by Zheng et al, 59 includes Astragalus membranaceus and Atractylodes macrocephala. In an experiment Feiyanning downregulated the transcription of migration-associated genes in NSCLC cells. 60 Feiyanning also inhibited the protective autophagy induced by cisplatin in NSCLC cells. 59 Shenmai injection, which contains Panax ginseng C. A. Meyer, promoted apoptosis in NK cells when combined with a PD-1 inhibitor, compared to PD-1 inhibitor monotherapy in NSCLC. 61
Many preclinical studies have reported that tumor-repressing HMs exert their effects by upregulating immune responses. HM can regulate both innate immunity, including macrophages, DCs, and NK cells, and adaptive immunity, including CD4+/CD8+ T lymphocytes and Tregs.31,49
However, limited clinical studies have evaluated the immunological effects of HM on these immune markers.
In addition, most clinical trials in this review did not report major clinical outcomes such as quality of life (QOL), safety, and survival benefits. However, several systematic reviews have not evaluated the immunological effect of HM but have shown the benefits of HM in improving QOL and its clinical effectiveness, including the survival time of patients with advanced NSCLC.11,12,62 In a single RCT of 106 patients with advanced NSCLC, HM therapy improved 3-month progression-free survival (PFS) and QOL, including physical well-being, emotional well-being, and functional well-being. No severe adverse effects were observed. 63
In addition to NSCLC, a single RCT was conducted on 68 patients with hepatocellular carcinoma. The results showed that the levels of CD3+ and CD4+ and the CD4+/CD8+ ratio in the peripheral blood of the HM with supportive care group were higher than those in the supportive care group. Moreover, the HM group showed immediate improvement in Karnofsky performance status scores, CD3+ and CD4+ T cell levels, and prolonged PFS. 64
This study provides insights into the application of HM as an adjunct immunotherapy. Substantial evidence, including our results, indicates that HM positively influences immune function in patients with advanced NSCLC.
However, this study has several limitations. First, we limited the types of cancer while searching the database to ensure that the HM applied to certain types of cancer (NSCLC) had immunological effects. Secondly, we examined the HM treatment group without any other conventional chemotherapy, radiation therapy, or other treatments. Therefore, the effects of herb-drug interactions were excluded. Third, this study did not conduct subgroup analyses based on the type of comparison because of the small number of studies included. Heterogeneity is rather high and must be considered when interpreting the results. High heterogeneity of CD4+ counts and CD4+/CD8+ ratios occurred in Hou and Meng, 16 who compared HM treatment with chemotherapy, in contrast to other RCTs that compared HM with symptomatic usual care. Several common herbs were used in the treatments; however, all the RCTs used heterogeneous HM prescriptions. Four RCTs used orally administered herbal decoctions, and 1 RCT used intravenous injections. 20 In addition, among 5 RCTs only Hou and Meng reported adverse events and only Zhu et al 20 reported the results of liver and kidney function tests. The blinding of participants and outcome assessments had a high risk of bias. The excluded RCTs may have existed beyond the 8 databases, although we searched for primary databases in the fields of traditional medicine and medical science.
Although there has been some improvement in the immune markers in the peripheral blood of patients, the detailed mechanism by which HMs exert their immunological effects at the molecular level requires further study. To date, most systematic reviews have addressed HM as a complementary medicine when combined with standard treatments to improve the survival rate and QOL of patients with cancer. 65 This study demonstrates that using HM alone can improve immune function in patients with NSCLC and provides comprehensive and systematic evidence for the immunological effects of herbal medicine. Future studies should explore how the immunological effects of HM correlate with clinical outcomes, such as tumor response and survival rates, to provide evidence of the role of HMs in improving immune function in patients with cancer. In addition, considering the genetic, environmental, and lifestyle diversity among patients with NSCLC, studies based on genetic markers or immunological characteristics are needed to make HM more precise and personalized.
Supplemental Material
sj-docx-1-ict-10.1177_15347354241287775 – Supplemental material for Herbal Medicines for the Improvement of Immune Function in Patients With Non-Small Cell Lung Cancer: A Systematic Review and Meta-Analysis
Supplemental material, sj-docx-1-ict-10.1177_15347354241287775 for Herbal Medicines for the Improvement of Immune Function in Patients With Non-Small Cell Lung Cancer: A Systematic Review and Meta-Analysis by Youngmin Cho, Hwa-Seung Yoo, Soo-Dam Kim, Mimi Ko, Han-eum Joo, Soobin Jang and Mi-Kyung Jeong in Integrative Cancer Therapies
Footnotes
Author Contributions
Conceptualization: M-KJ, SJ. Methodology: SJ, MMK, M-KJ, S-DK. Supervision: M-KJ, SJ. Writing – original draft: YC, M-KJ, S-DK, HEJ. Data curation: S-DK. Writing – review & editing: M-KJ, SJ, HSY.
Data Availability
Data supporting the findings of this study are available from the corresponding author upon reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Korea Institute of Oriental Medicine, Republic of Korea (KSN2321240), and the Korea Health Industry Development Institute (KHIDI), Republic of Korea (HI19C1046). The funding source did not influence the interpretation or publication of the study results.
Ethical Considerations
No ethical approval was required as this study did not involve human participants or laboratory animals.
Consent to Participate
Not applicable.
Consent for Publication
Not applicable.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.