
Abstract
Background/Objective:
Promoting well-being is a key goal of cancer care, and it needs to be assessed using appropriate instruments. Flourishing is considered part of psychological well-being and it is commonly assessed with the Flourishing Scale (FS). To our knowledge, no studies have analyzed the psychometric properties of the FS in breast cancer patients. Our aim here was to provide validity evidence for use of the FS in this context.
Method:
Participants were 217 Spanish women with breast cancer who completed the FS and other scales assessing positive psychology constructs (life satisfaction, positive affect, resilience, self-esteem, optimism) and indicators of psychological maladjustment (negative affect, depression, anxiety, and stress). The internal structure of the FS was analyzed using confirmatory factor analysis (CFA). We calculated the average variance extracted (AVE) to evaluate convergent validity, and both McDonald’s omega and Cronbach’s alpha coefficients to estimate reliability. Item analysis was performed by computing corrected item-total correlations. Validity evidence based on relationships with other variables was obtained through Pearson correlation analysis, controlling for age and cancer stage.
Results:
The CFA supported a single-factor structure, with adequate goodness-of-fit indices (CFI = 0.997, NNFI = 0.996, RMSEA = 0.069, and SRMR = 0.047) and standardized factor loadings ranging from 0.70 to 0.87. The value of the AVE was 0.63, and the reliability coefficient obtained with both procedures was 0.91. Corrected item-total correlations ranged from .62 to .78. Correlation analysis showed direct and strong associations between the FS score and scores on positive psychology constructs (range from 0.43 to 0.74), the strongest correlations being with positive affect and life satisfaction. The FS score was inversely correlated with scores on depression, anxiety, stress, negative affect, and pessimism (range from −0.14 to −0.52), the strongest association being with stress.
Discussion:
The FS is a useful tool for exploring well-being in the breast cancer context, providing useful information for psychological assessment.
Introduction
Well-being has been a key topic of research in positive psychology. Two perspectives have been proposed: hedonic well-being and eudaimonic well-being. 1 The hedonic perspective considers both the cognitive component of well-being (i.e., life satisfaction) and its affective component (positive and negative affect). As regards eudaimonic well-being, this is defined by Ryff and Singer 2 as a form of psychological well-being involving full and positive social functioning, meaning in life, and purposefulness. In line with this perspective, the concept of flourishing refers to a sense of psychosocial prosperity and well-being, 3 as well as to perceived success in terms of positive relationships, self-esteem, optimism, self-acceptance, engagement, sense of purpose, achievements, and contribution to the well-being of others.4,5
One of the first attempts to assess flourishing was the European Social Survey.4,6 Although not a flourishing scale per se, the survey included items relating to this construct in its well-being module. Other scales designed specifically to measure flourishing were published subsequently, including the Human Flourishing Questionnaire (HFQ), 7 the Human Psychological Flourishing Scale (HPFS), 8 and the Flourishing Scale (FS). 3 The HFQ, based on Seligman’s 5 PERMA theory of well-being, is a 28-item questionnaire with a 4-factor internal structure referring to positive emotions, relationships, meaning, and achievement. It was developed with university students and designed for use in the Iranian population. As for the HPFS, which was developed with teachers, this was also designed to assess flourishing in the Iranian socio-cultural context, as its authors considered that existing scales did not provide sufficient information on flourishing in this population. The HPFS comprises 12 items grouped into 3 factors: satisfaction/happiness, individual competency, and social contribution. However, these 2 scales have received little attention outside the Iranian context. The FS, by contrast, is a shorter instrument with a unidimensional structure that has been widely used in different populations worldwide, and there is more empirical evidence regarding its psychometric properties.
The FS was designed to measure psychosocial prosperity, and it is based on humanistic theories and other approaches to well-being.9 -11 It consists of 8 items, each rated on a 7-point Likert-type scale, that explore positive relationships, feelings of competence, and a sense of meaning and purpose in life. Diener et al 3 analyzed the internal structure of the FS and found support for a single-factor model. Regarding the reliability of scale scores, they reported Cronbach’s alpha and test-retest coefficients of .87 and .71, respectively. Validity evidence based on relationships with other variables was obtained by examining the correlation between scores on the FS and those on other measures of psychological well-being, specifically the Satisfaction with Life Scale (SWLS), 12 the Psychological Well-being Scales, 13 which assess autonomy, growth, mastery, relationships, self-esteem, and purpose and meaning, and the General Basic Needs Satisfaction Scale, 14 which evaluates competence, relatedness, and autonomy. The results showed strong positive correlations between scores on the FS and those on these other measures. It was also found that individuals who scored higher on the FS tended to have a higher level of optimism.
As mentioned above, the FS has been widely used around the world, and psychometric studies of the scale have been conducted in numerous languages and geographic regions: Europe,15 -22 Africa, 23 Asia,24 -31 North America,32 -34 Latin America, 35 and New Zealand. 36 These studies have been performed with different populations, including adolescents,26,30 young people,15,17,19,23,28,29,32 adults,16,20 -22,24,31,35,36 and older adults.25,27
In general, the aforementioned studies have replicated the single-factor structure proposed by Diener et al, 3 and most of them report a reliability coefficient above .80,16,17,19 -27,29 -34,36 which is considered a good indicator of score reliability. 37 In terms of validity evidence based on relationships with other variables, scores on the FS have been found to correlate positively with scores on satisfaction with life,15,16,18,20 -23,25,26,29,31 -36 positive affect,16,19,32,35 optimism,16,19,22,34,35 self-esteem, 20 and resilience.22,34 Conversely, a negative correlation has been observed between scores on the FS and those on measures of negative affect,16,19,32,35 depression,15,17,20,22,25,26,34 anxiety,15,17,19,22,26,34 and stress.17,34
Psychometric studies of the FS in clinical populations are, however, scarce. They have so far been conducted with individuals with chronic pain, 19 parents of children with cancer, 18 and adults with spinal cord injury 33 or physical disability, 34 but to our knowledge there are no studies that analyze the psychometric properties of the FS in the oncology population, either in general or in specific sub-populations such as women with breast cancer. Research in our country, Spain, has provided evidence of the psychometric properties of the FS in the general population, 16 university students,17,19 and some clinical samples,18,19 but not among cancer patients. It should be noted that cancer differs from other types of physical illness in that treatments and surgical interventions are often highly invasive, resulting in ongoing emotional distress. Breast cancer also differs from other types of cancer, insofar as it primarily affects women and a part of their body that can lead to altered body image. Given that the inferences drawn from scores on an instrument are for a specific use, context, and population, 38 further studies are warranted to provide empirical evidence for use of the FS in the breast cancer population.
Accordingly, the aim of the present study was to analyze the psychometric properties of the FS in a sample of women with breast cancer. First, validity evidence based on the internal structure is provided through confirmatory factor analysis (CFA). We then calculate the average variance extracted (AVE) to evaluate convergent validity, compute corrected item-total correlations for item analysis, and calculate both McDonald’s omega and Cronbach’s alpha coefficients to estimate the reliability of scale scores. Finally, we also provide validity evidence based on relationships with other variables. The variables considered include both positive psychology constructs (i.e., life satisfaction, positive affect, resilience, self-esteem, and optimism) and indicators of psychological maladjustment (negative affect, depression, anxiety, and stress). We expected to find that the FS score is positively related to scores on life satisfaction, positive affect, resilience, self-esteem, and optimism, and negatively associated with scores on negative affect, pessimism, depression, anxiety, and stress.
Material and Methods
Participants
The sample comprised 217 women diagnosed with breast cancer. They were aged between 23 and 76 years (M = 52.20, SD = 9.59) and were recruited through 14 clinical centers and associations providing breast cancer care. The mean time since diagnosis was 5.70 years (SD = 6.58), while age at the time of diagnosis ranged between 18 and 72 years (M = 46.42, SD = 9.20). At the time of the study, 45.6% of the sample had attended university, 71.4% were married or living with their partner, 65.9% were unemployed, and almost half (44.2%) were stage II according to the TNM tumor classification system. The inclusion criteria were as follows: Signing informed consent, having a diagnosis of breast cancer, and not having a diagnosis of any other type of cancer or psychological disorder. This information was obtained based on self-report. Table 1 provides more information about the characteristics of participants. In order to obtain validity evidence based on relationships with other variables, the sample was split into 2 sub-samples of similar size. Each sub-sample completed, in addition to the FS, different questionnaires so as to avoid participant fatigue. Subsample 1 (N = 107) completed the Satisfaction with Life Scale (SWLS), Negative and Positive Affect Scale (NAPAS), and the 21-item version of the Depression, Anxiety, and Stress Scales (DASS-21), whereas subsample 2 (N = 110) completed the 10-item version of the Connor-Davidson Resilience Scale (CD-RISC-10), the Self-Esteem Scale (SES), and the Life Orientation Test-Revised (LOT-R).
Sample Characteristics (N = 217).

Instruments
Flourishing Scale (FS), 3 in its Spanish version. 16 The FS assesses flourishing as a sense of competence, self-acceptance, optimism, and contribution to the well-being of others. It comprises 8 items that are rated on a 7-point Likert-type scale (1 = strongly disagree; 7 = strongly agree), and hence the total score ranges from 8 to 56 points, with high scores indicating high levels of flourishing. Reliability of scale scores (McDonald’s omega) in the present sample was 0.91.
Satisfaction with Life Scale (SWLS), 12 in its Spanish version 39 that has been validated in breast cancer patients. 40 The SWLS has 5 items, each rated on a 7-point Likert-type scale (1 = strongly disagree; 7 = strongly agree). The total score therefore ranges between 5 and 35, and high scores indicate a high level of satisfaction with life as a whole. McDonald’s omega in the present sample was 0.88.
Negative and Positive Affect Scale (NAPAS), 41 in its Spanish version. 42 The NAPAS is composed of 12 items that evaluate both negative affect (6 items) and positive affect (6 items). All items are rated on a 5-point Likert-type scale (1 = none of the time; 5 = all of the time), and hence the total score for each type of affect ranges from 6 to 30. High scores indicate a high level of the respective affect. McDonald’s omega coefficients in the present sample were 0.87 and 0.91 for the negative and positive affect scales, respectively.
21-item version of the Depression, Anxiety, and Stress Scales (DASS-21), 43 in its Spanish version. 44 The DASS-21 comprises 21 items that assess depression, anxiety, and stress (7 items each), and it yields a total score representing general psychological distress. Each item is rated on a 4-point Likert-type scale (0 = does not apply to me at all; 3 = applies to me a lot or most of the time), and hence the total score ranges between 0 and 63 points. High scores indicate high levels of the respective construct. McDonald’s omega coefficients in the present sample were 0.82, 0.88, 0.87, and 0.94 for depression, anxiety, stress, and the total scale, respectively.
10-item version of the Connor-Davidson Resilience Scale (CD-RISC-10), 45 in its Spanish version 46 that has been validated in the breast cancer population. 47 The 10 items of this scale are each rated using a 5-point Likert-type scale (0 = not true at all; 4 = true nearly all the time), such that the total score ranges between 0 and 40. High scores indicate high resilience. McDonald’s omega was 0.89 in the present sample.
Self-Esteem Scale (SES), 48 in its Spanish version. 49 The SES comprises 10 items, each rated on a 4-point Likert-type scale (1 = strongly disagree; 4 = strongly agree), and thus the total score ranges between 10 and 40 points. High scores are indicative of a high level of self-esteem. In the present sample, McDonald’s omega was 0.85.
Life Orientation Test-Revised (LOT-R), 50 in its Spanish version. 51 The LOT-R has 10 items, three of which are positively worded and measure optimism, three are negatively worded and measure pessimism (these items are reverse coded before scoring), and four are fillers. Respondents rate each item using a 5-point Likert-type scale (0 = strongly disagree; 4 = strongly agree). The total score ranges between 0 and 24 points, because the filler items are not counted. A high total score indicates a high level of overall optimism. McDonald’s omega coefficients in the present sample were 0.69, 0.62, and 0.69 for optimism, pessimism, and overall optimism (total score), respectively.
Procedure
The study followed the ethical standards of the Declaration of Helsinki and was approved by the Experimental Ethics Committee of the University of Malaga (Spain). Participants were recruited following a convenience sampling strategy. They were all volunteers and did not receive any incentives. In a first step, we contacted by e-mail and subsequently conducted a telephone interview with the staff of various centers and associations that provide care to women with breast cancer. Staff at each center contacted potential participants and invited them to participate in the study. Those who accepted were randomly split into 2 groups using the random function of the Excel program and sent an e-mail with the link to the respective questionnaires. The first group received the link to the survey containing the FS, SWLS, NAPAS, and DASS-21, whereas the second group received the link to the FS, CD-RISC-10, SES, and LOT-R. Before completing the questionnaires, participants were informed about the study objectives and procedures and signed an online informed consent form indicating that the information collected would be treated anonymously and confidentially and would only be used for research purposes. There were no missing data because participants could not submit the questionnaires unless all items had been answered.
Data Analysis
We began by performing a descriptive analysis of FS items and the other study variables. Then, in order to obtain validity evidence based on internal structure, CFA was carried out to test the single-factor structure found in previous studies. This analysis used the diagonally weighted least squares (DWLS) estimator based on the polychoric correlation matrix, which has been shown to provide accurate parameter estimates when dealing with categorical items. 52 Model fit was assessed by computing the chi-square statistic (χ2) and the following indices: Comparative fit index (CFI), non-normalized fit index (NNFI), root mean square error of approximation (RMSEA) and its 90% confidence interval, and the standardized root mean square residual (SRMR). The criteria for the interpretation of these indices were as follows: CFI and NNFI values of 0.95 or higher indicate a satisfactory fit 53 ; RMSEA values between 0.06 and 0.08 indicate a reasonable fit 54 and those below 0.06 a satisfactory fit 53 ; and a SRMR value close to 0.08 is considered a good fit. 53
Next, and to evaluate convergent validity, we computed the AVE, considering values greater than .50 as acceptable. Item analysis was then performed, calculating homogeneity indices in the form of corrected item-total correlation coefficients, with values above .30 being considered as satisfactory. The reliability of FS scores was assessed by calculating McDonald’s omega and Cronbach’s alpha coefficients, considering a value of .70 or higher as satisfactory.
Finally, validity evidence based on relationships with other variables was obtained by calculating Pearson correlation coefficients between scores on the FS and those on both positive psychology constructs and indicators of psychological maladjustment, controlling for age and cancer stage. Coefficients were interpreted according to Cohen’s 55 criteria: around |0.10|, low correlation; close to |0.30|, moderate; near |0.50| or higher, strong correlation. All analyses were performed with the R package lavaan. 56
Results
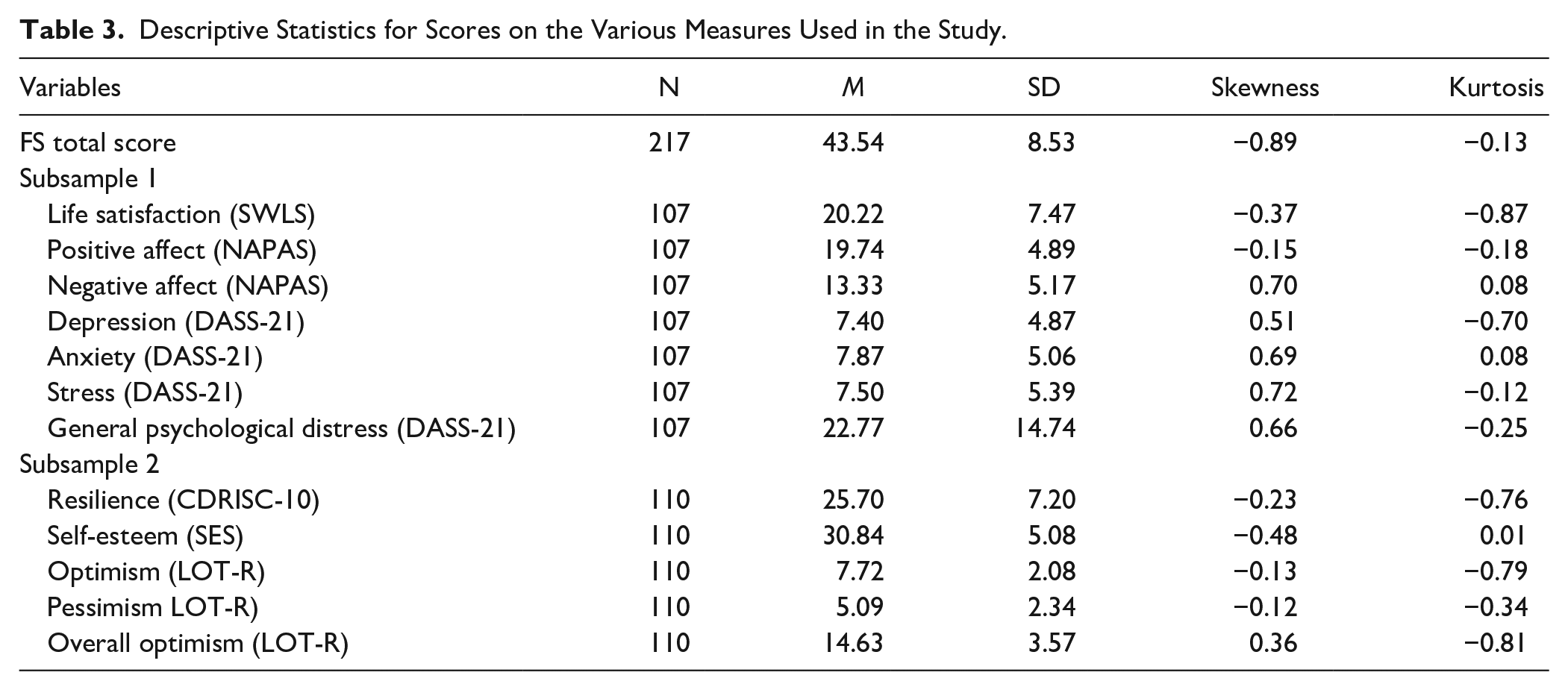
Table 2 shows descriptive statistics for FS items and Table 3 for scores on all the measures considered in the study. The mean total FS score was 43.54, with a standard deviation of 8.53.
Descriptive Statistics for FS Items, and Corrected Item-Total Correlations.

Descriptive Statistics for Scores on the Various Measures Used in the Study.
In the CFA, the χ2(20) statistic was equal to 40.66, P = .004. All goodness-of-fit indices were adequate according to the criteria established for the single-factor model: CFI = 0.997, NNFI = 0.996, RMSEA = 0.069, 90% CI [0.038, 0.10], and SRMR = 0.047. The standardized parameters were all significant and are shown in Figure 1. The value of the AVE was 0.63, above the 0.50 threshold.

Standardized factor loadings for the 1-factor model of the FS.
Table 2 also shows the corrected item-total correlations for each item of the FS. Values ranged between 0.62 and 0.78, all above the cut-off of 0.30. Both McDonald’s omega and Cronbach’s alpha yielded a coefficient of .91, above .70 and thus indicating satisfactory reliability of FS scores.
Regarding validity evidence based on relationships with other variables, the results (controlling for age and cancer stage) showed strong positive correlations between FS scores and scores on life satisfaction, positive affect, resilience, self-esteem, and optimism. Strong negative correlations were obtained with depression, anxiety, stress, and general psychological distress, and a moderate negative correlation was observed between FS scores and negative affect. No statistically significant correlation was obtained with pessimism. Among positive psychology constructs, the strongest correlations were those between FS scores and scores on positive affect and life satisfaction (coefficients of 0.74 and 0.70, respectively). With respect to indicators of psychological maladjustment, the strongest correlation was that between FS scores and stress (coefficient of −0.50). These results are shown in Table 4.
Correlations Between the FS Total Score and Scores on the Other Study Variables, Controlling for Age and Cancer Stage.

P < .001.
Discussion
The aim of this study was to analyze and report the psychometric properties of the FS so as to provide evidence supporting its use with breast cancer patients. To this end, we analyzed the internal structure of the scale, evaluated convergent validity, conducted item analysis, examined the reliability of test scores, and obtained validity evidence based on relationships with other variables.
Regarding validity evidence based on the internal structure of the FS, the CFA showed satisfactory fit indices for the single-factor structure. This model is consistent with the original validation study, 3 as well as with that reported in other studies involving adults from both the general16,20,21,24,31,35,36 and clinical populations.18,19,33,34 The value of the AVE was 0.62, above the 0.50 threshold, indicating that the amount of variance explained by the construct is greater than the variance due to measurement error. The homogeneity indices for all items of the FS were also satisfactory (range from 0.62 to 0.78). Regarding the reliability of FS scores, values of McDonald’s omega and Cronbach’s alpha (both .91) indicated that this was adequate, in line with previous research.23,24,29,33,34,36 In general, the results show that the FS is a unidimensional measure of flourishing with satisfactory reliability in which high scores reflect a greater sense of competence, self-acceptance, optimism, and a greater contribution to the well-being of others.
In terms of validity evidence based on relationships with other variables, the results were consistent with what we expected. Specifically, scores on the FS were strongly and positively correlated with life satisfaction, positive affect, resilience, self-esteem, and optimism, with all coefficients being close to or above 0.50. Conversely, FS scores showed a moderate negative correlation with negative affect, and strong and negative associations with depression, anxiety, stress, and general psychological distress. These results are likewise consistent with previous studies15 -23,25,26,29,31 -36 and suggest that breast cancer patients with a higher level of flourishing tend to feel more satisfied with their lives in general, experience a greater sense of happiness and pleasure in life, cope better with adversity, value themselves more, and see the future with more hope. In addition, these women also show better psychological adjustment, expressing less general discomfort and generally feeling less irritable, anxious, sad or despondent. Given the cross-sectional nature of this study, causality cannot be established for these relationships.
The strongest correlations for FS scores were with life satisfaction and positive affect, both of which are components of hedonic well-being. This supports the strong relationship between hedonic and eudaimonic well-being, whereby the former is defined within a framework of pleasure, happiness, and enjoyment, while the latter focuses more on well-being as a consequence of personal growth and self-fulfillment, and is based fundamentally on how individuals deal with life’s challenges.2 -4,9
Taken together, the results suggest that flourishing is a key variable to consider when conducting psychological assessment in the breast cancer context. Women who feel they do not have positive relationships, who do not feel competent, and who struggle to find meaning and a sense of purpose in life are likely also to show low levels of well-being and a high level of anxiety, depression, and stress. They should therefore be considered a target population for psychological support in coping with their cancer process, as they are at risk of psychological maladjustment. By contrast, those women who are found to have adequate levels of flourishing are less likely to be in a vulnerable psychological state.
This study has a number of limitations that should be acknowledged. First, our reliance on a convenience sample of volunteer participants may limit the generalizability of results. Second, as a self-report scale the FS may be affected by response bias (e.g., social desirability, order effect bias). Third, validity evidence based on relationships with other variables was provided with respect to a limited number of variables, and further research is needed to explore the relationship between flourishing and factors such as personality, coping strategies, or social support. Finally, the cross-sectional study design means that causal attributions cannot be established. Future research should include longitudinal studies to clarify causal relationships.
Notwithstanding these limitations, the present study provides empirical support for use of the FS in the field of psycho-oncology. Overall, the results suggest that it is a suitable instrument for measuring perceived psychological prosperity in this context and that it may contribute useful information to the psychological assessment of women with breast cancer.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by funding from the Regional Government of Andalusia to Consolidated Research Group CTS110.
Ethical Approval Statement
This study followed the ethical standards of the Declaration of Helsinki and was approved by the Experimentation Ethics Committee of the University of Malaga (55-2017 H).
Informed Consent
All participants in this study signed informed consent prior to data collection.