
Abstract
Objectives:
This study reports on the long-term effects of the Better Life After Cancer: Energy, Strength, and Support (BLESS) program, a 12-week social capital-based exercise adherence program for breast cancer survivors (BCS), implemented using a randomized controlled trial design. The study investigated outcomes related to cancer-related fatigue (CRF), quality of life (QOL), physical activity, depression, anxiety, sleep quality, and social capital.
Methods:
Participants who had moderate or greater CRF were randomly assigned to the intervention (n = 24), consisting of supervised and home-based exercise, or the control (n = 26), who received exercise leaflets. Generalized estimating equations models were fitted for the outcome variables. The assessment points were baseline (M1), immediately after completing the intervention at 12 weeks (M2), 1 month (M3), and 6 months post-intervention (M4).
Results:
A significant reduction in the total CRF score was found for both groups. We observed a significant time by group effect at M2, indicating a reduction of behavioral/severity CRF scores and a higher increase of physical activity. Also, there was an increase in the QOL score of both groups at M2, M3, and M4, compared to M1. Both groups had reduced anxiety at M3 and M4 compared to M1. The time by group effect for depression, sleep quality and social capital was not statistically significant.
Conclusion:
This 12-week exercise adherence program improved behavioral/severity CRF and physical activity post-intervention. Both the experimental group and control group showed significant improvements in CRF, QOL, and anxiety domains compared to the baseline, which extended to 6 months post-intervention.
Trial registration:
Korean Clinical Research Information Service (KCT0005763)
Introduction
The National Comprehensive Cancer Network defined cancer-related fatigue (CRF) as a “distressing persistent, subjective sense of physical, emotional, and/or cognitive tiredness or exhaustion related to cancer or cancer treatment that is not proportional to recent activity and interferes with usual functioning.” 1 A growing body of evidence indicated that exercise and exercise adherence reduces CRF. 2 The multifarious mechanisms of CRF include physiological, immunological, and behavioral factors. 3 However, exercise is known to positively influence these mechanisms, suggesting that its effects on CRF may also operate through these pathways.4,5
Nevertheless, findings on the effects of exercise on CRF for breast cancer survivors (BCS) have been inconsistent. Although there is strong evidence to support at least modest effects of exercise on CRF during and after breast cancer treatment,4,6 some studies have reported no significant differences in CRF between the exercise group and the control group, indicating the need for further research.7 -9 Furthermore, a few exercise studies have specifically focused on breast cancer survivors with moderate CRF. 10
Fatigue was associated with additional barriers such as social isolation and difficulty sustaining an exercise routine in cancer survivors. 11 Finding comfort and strength through exercise, as well as interacting with other breast cancer survivors, served as facilitative factors for physical activity. 12 Thus, peer support and fostering group cohesion as part of an exercise program may help support an exercise routine. 13 Engaging in physical activity with others can help establish positive social norms for physical activity among an individual’s social network. This, in turn, enables individuals to form a sense of attachment and connectedness with group members and provides access to resources that support physical activity. 14
With growing recognition of the social determinants of health, social capital is an increasingly important concept in health research. Social capital refers to the resources embedded in a social structure that is accessed and/or mobilized in purposive actions. 15 Further, one distinction that has gained currency dichotomizes social capital into “bonding” and “bridging” varieties. 16 Specifically, bonding social capital refers to trusting and cooperative relations within homogeneous groups, while bridging social capital describes relationships between individuals who are dissimilar with respect to social identity and power. 17 Therefore, we need to develop and verify the effectiveness of the exercise adherence program using social capital activation for breast cancer survivors.
The intervention “Better Life After Cancer: Energy, Strength, and Support (BLESS)” was developed to meet these needs. Using the intervention mapping protocol, it incorporates a theory and practice-based exercise adherence program rooted in behavioral change theories and practical knowledge, specifically tailored to the needs of BCS with CRF. 18 Moreover, the recently completed BLESS study examined the short-term effect in BCS with moderate or greater levels of CRF. 19
The present study aimed at confirming the long-term effectiveness of the BLESS program in maintaining exercise for BCS, and testing its effectiveness in CRF, depression, anxiety, sleep quality, social capital, and quality of life at the 6 months follow-up.
Methods
Study Design and Ethics
The 12-week randomized controlled trial (RCT) was conducted from June–to September 2017. Participants were randomly assigned to the intervention or control group using a 1:1 ratio applied through computer-generated random number sequencing. We used this randomizer tool to generate a random allocation number for each participant. The generated random numbers were kept hidden or protected. The random allocation sequence was not disclosed to the participants or the research team until the group assignments were made. An independent researcher performed the group assignments by verifying the random allocation numbers and assigning the participants to their respective groups. The researchers (and assessors) were not blinded to group allocation. Recruitment and enrollment occurred from March-May 2017 from the patient population of a cancer center at a tertiary hospital in Seoul, Korea and advertised via a breast cancer online community. Assessments points included baseline (M1), immediately after completing the intervention at 12 weeks (M2), 1 month (M3), 6 months (M4), and 12 months post-intervention (M5). The scope of this manuscript is focused on the time point data up to 6 months after the intervention (M4).
The study protocols received ethical approval from Severance Hospital, Korea (IRB 4–2017–0164). All procedures in this study were carried out in accordance with the Declaration of Helsinki. All patients signed informed consent forms
Participants
The inclusion criteria were: (1) women aged 20-69 years, (2) diagnosed with breast cancer, stage I–III, (3) completed surgery and chemotherapy, (4) experienced greater than moderate fatigue (≥4 out of 10),20,21 and (5) diagnosed at least 6 months prior to enrollment and within the last 5 years. The exclusion criteria were: (1) self-report of a diagnosed underlying disease that influences fatigue, (2) recurrent cancer, (3) other cancer(s) in addition to breast cancer, (4) mental health problems, (5) physically unable to engage in low-to-moderate intensity exercise, (6) pregnancy, and (7) current enrollment in regular exercise. The sample size was identified as 48 for statistical power of 80%.
Intervention
The BLESS program is a 12-week comprehensive exercise adherence program that comprises aerobic and strength training exercises with a social capital activation strategy. The exercise content was designed by a physical exercise expert. It incorporates core muscle exercises and enhancing physical balance through movements that alleviate strain on the shoulders and arms to reduce the likelihood of lymphedema and injuries in BSC. The BLESS program had 2 distinct phases. In the first phase, participants engaged in exercise sessions once a week for 6 weeks, totaling 6 sessions. During the exercise training sessions, an exercise expert demonstrated the movements at 3 levels of intensity (i.e., low, medium, and high intensity), and provided instructions and feedback. Information on exercise guidelines and the specific exercise components, fatigue management after cancer, and an exercise log was provided as a workbook and intervention participants were also given videos on how to exercise at the 3 levels of intensity. They also worked on building stronger connections with other participants through small group participation, with each group consisting of 3 to 6 people. During the second phase, the exercises were shifted to participants’ homes, and they performed them twice a week for another 6 weeks, resulting in a total of 12 home-based sessions. In this phase, the focus of the groups shifted toward developing bonding social capital and preparing for bridging social capital. The participants checked their individual exercise goals, took part in lectures and activities aimed at enhancing leadership skills, and engaged in expressive activities for self-reflection. In summary, the groups met 8 times, with each session lasting 2 hours. 18
The control group was provided with general written information on exercise movements, which was used at the hospital with all BCS, constituting usual care. After the 12 weeks, the control group was given the opportunity to participate in a one-time group exercise lesson. Both groups received text messages once a week to motivate them to monitor and reduce fatigue. The content of the messages encouraged them to engage in exercise as a means to alleviate cancer-related fatigue. This strategy was based on the theoretical foundation of social cognitive theory, which suggests that verbal persuasion is effective in enhancing motivation.
Outcomes
CRF was measured using the 19-item Korean Revised Piper Fatigue Scale (R-PFS-K). 22 CRF was measured using 4 subscales: (1) behavioral/severity, (2)affective meaning, (3) sensory, and (4) cognitive/mood. The behavioral/severity subscale measures the extent to which fatigue affects individuals’ ability to engage in work, social, or interpersonal activities. The affective meaning subscale assesses feelings of frustration, helplessness, and vulnerability associated with fatigue. The sensory subscale evaluates the physical intensity or severity of fatigue, while the cognitive/mood subscale captures emotions related to tension, depression, and clarity of thought. Quality of life (QOL) was measured using the Korean version of the 37-item Functional Assessment of Cancer Therapy Scale-B (FACT-B), 23 which measures subjective QOL in 5 wellbeing subscales. Physical activity was measured using the Korean version of the Global Physical Activity Questionnaire (GPAQ). 24 Depression and anxiety were measured using the Korean version of the 14-item Hospital Anxiety and Depression Scale (K-HADS), 25 through payment to GL Assessment. Sleep quality was measured using the Korean version of the 19-item Pittsburgh Sleep Quality Index (PSQI) 26 adapted for use in Korea by Sohn et al . 27 Social capital was measured using the 8-item Personal Social Capital Scale (PSCS-8). 28 Details on measurements are described elsewhere. 18
Statistical Analysis
The statistical analyses were performed using SPSS Statistics 25.0. We conducted descriptive analysis for demographic and clinical characteristics. Baseline differences between the BLESS and the control group were tested using independent t-tests and Chi-square for contingency tests. Generalized estimating equations (GEE) provide an excellent method to capture the correlation of repeated measures of variables and offer more efficient estimates in longitudinal studies. 29 In contrast to traditional repeated measures ANOVA, the GEE approach permits analysis using all available outcome data. 30 In this study, GEE models were fitted for the outcome variables. And the analysis was conducted using the log link function for the gamma distribution. In the GEE analysis, each outcome was regressed on the randomization group (BLESS group), time point, and group by time point interaction. The effect of time was partitioned into planned contrasts of baseline assessment against each follow-up.
Results
Participants
Twenty-four participants were assigned to the intervention (BLESS) group, and 26 to the control group. Forty BCS (intervention group, n = 20/control group, n = 20) patients completed the study at 6 months and reasons for dropping out are listed in the CONSORT flow diagram (Figure 1).

Consort diagram.
General Characteristics of the Participants
The majority of participants consisted of stage 1 or 2 cancer, diagnosed within the last 2 years, and had undergone both chemotherapy and radiation therapy (Table 1). The 2 groups were not significantly different in terms of personal BCS health characteristics. Moreover, homogeneity tests reported no significant differences in participants’ baseline CRF, QOL, physical activity, depression, anxiety, sleep quality, and social capital scores between the 2 groups. Regarding part-time or regular work within the last 6 months, there were 5 participants (21.7%) in the BLESS group and 8 participants (42.1%) in the control group. However, no statistically significant difference was found according to an additional assessment at M3.
Sociodemographics of the Study Sample (N = 46).

Abbreviations: Int, intervention group; Cont, control group.
Effect of the BLESS Intervention on CRF and QOL
The means and standard deviations (SD) of scores on all measurements at baseline (M1), post-intervention (M2), and at 1 and 6 months are presented in Table 2. Mean scores across all measurement points are illustrated separately for the intervention and control groups in Figure 2.
Effects of the Intervention on Fatigue, Social Capital, Physical Activity, Sleep Quality, Depression, Anxiety, and Quality of Life.
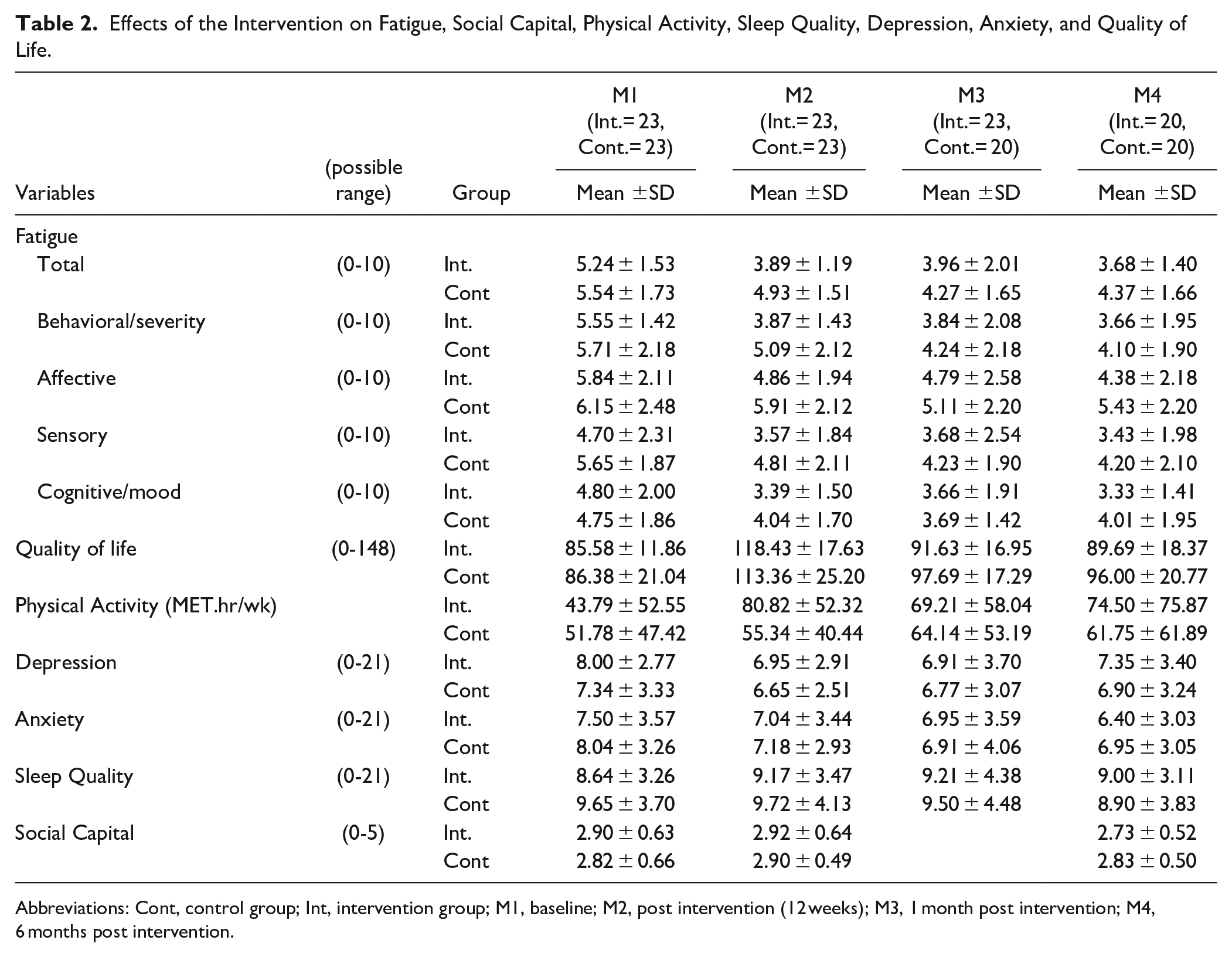
Abbreviations: Cont, control group; Int, intervention group; M1, baseline; M2, post intervention (12 weeks); M3, 1 month post intervention; M4, 6 months post intervention.

Effects of the intervention on fatigue, social capital, physical activity, sleep quality, depression, anxiety and quality of life at different measurement points in the intervention and control group.
Table 2 depicts changes in the total CRF and all subscale scores over time. We observed slightly lower levels of CRF in the BLESS group patients at 1 month (M3), and 6 months post-intervention (M4) compared to baseline, although this result was not statistically significant. Table 3 presents results from fitting the GEE models. There was a significant reduction in total CRF score in both groups at M2 (coefficient = −1.60, CI [−1.10, −0.11]), M3 (coefficient = −1.36, CI [−1.92, −0.79]), M4 (coefficient = −1.03, CI [−1.66, −0.40]) compared to the M1 average. For the intervention group participants, the additional reduction in total CRF score at M2, M3, and M4 was not significantly greater than that of the control group. However, at M2 the additional reduction in behavioral/severity subscale was statistically significantly greater than that of the control group (coefficient = −1.06, CI [−1.94, −0.19]).
GEE model Results of Intervention and Time Effect.
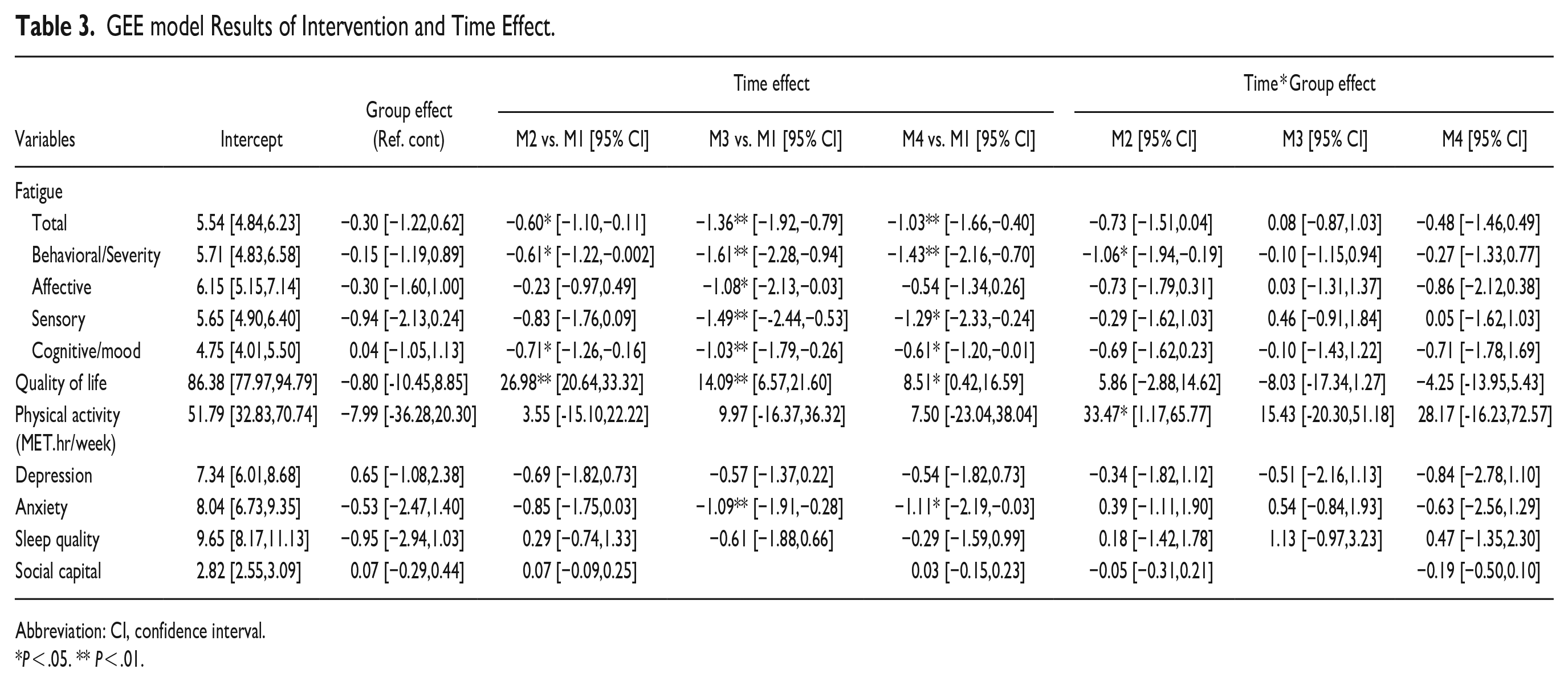
Abbreviation: CI, confidence interval.
P < .05. ** P < .01.
There was a significant increase in QOL score of both groups at M2 (coefficient = 26.98, CI [20.64,33.32]), M3 (coefficient = 14.09, CI [6.57, 21.60]), and M4 (coefficient = 8.51, CI [0.42, 16.59]) compared with the M1 average (Table 3). The additional increase in QOL at M2, M3, and M4 was not significantly greater than that of the control group, thus indicating a similar development of QOL trajectories in both groups.
Effect of the BLESS Intervention on Physical Activity
Table 2 presents the changes in physical activity and psychosocial factors. Results from the GEE model indicate that the overall model without time interaction term did not show a significant effect for the BLESS program on the physical activity (Table 3: coefficient = 1.69, CI [−1.09, 4.47]). There was no significant time effect to demonstrate that both groups had increased physical activity at M2, M3, and M4 compared to M1. We observed a significant time by group effect at M2 indicating a higher increase of physical activity among the BLESS group compared to the control group (coefficient = 33.47, CI [1.17, 65.77]).
Effect of the BLESS Intervention on Psychosocial Factors
Psychosocial factors such as depression, anxiety, sleep quality, and social capital followed similar patterns as the main outcomes. (see Table 2 for means and SD at the 4-time points and Figure 2 for mean scare trajectories.) There was a statistically significant time effect (Table 3) showing reduced anxiety in both groups at M3 (coefficient = −1.09, CI [−1.91, −0.28]) and M4 (coefficient = −1.11, CI [−2.19, −0.03]) compared to M1. The additional decrease in anxiety at M2, M3, and M4 was not significantly greater than that of the control group, indicating a similar improvement of anxiety trajectories in both groups. Moreover, statistically significant results were not found in the GEE model of the group × time interaction for depression, sleep quality, and social capital.
Discussion
The present study evaluated the long-term effects of the BLESS intervention on various factors including CRF, QOL, physical activity, depression, anxiety, sleep quality, and social capital, demonstrating sustained improvements in CRF, QOL, physical activity, and anxiety levels. However, no statistically significant difference was found between the experimental group and control group at 6 months post-intervention.
We demonstrated that the decrease in behavioral/severity CRF was significantly greater in the BLESS group compared to the control group during the 12-week intervention. There was no significant difference between the groups over time in other domains, thus indicating that this intervention contributed to reducing CRF in this sample of BCS with moderate or greater fatigue levels at baseline.
We observed slightly lower levels of CRF in the BLESS participants at 6 months post-intervention (M4), although the result was not statistically significant. In both groups, the CRF score decreased over time, which may not have resulted in a statistically significant difference. This can be confirmed through the finding that the CRF scores were found to have a significant time effect at M2, M3, and M4 compared to the baseline. Considering that the majority of participants in this study had 1 to 2 years since diagnosis, these results are similar to prior study findings that confirm the effect of exercise on CRF at the long-term follow-up of up to 4 years.31,32 A possible explanation for this might be the natural occurring reduction in CRF over time. 33 Moreover, since this study targeted BCS with moderate or greater CRF, the difference in average CRF score may have been small. In other words, because patients with moderate to severe fatigue already experience high levels of fatigue, it implies that implementing additional interventions may not result in a substantial change in their average fatigue. In line with the present study results, a previous study reported no significant difference between the exercise group and the control group in fatigue perception among BCS with moderate CRF. 10 Nevertheless, a study that applied nurse-led home-based exercise and cognitive behavioral therapy in ovarian cancer survivors with moderate CRF reported lower CRF in the experimental group compared to the control group until 6 months post-intervention. 34 Therefore, we propose in-depth and diverse exercise studies including psychosocial intervention for BCS with CRF. Furthermore, in this study’s intervention, both groups received text messages once a week to self-assess their level of CRF and encourage participation in exercise. Considering the previous findings of reduced CRF through remote contact such as text messages and mobile apps,35,36 it should be noted that both groups may have experienced similar effects. In this study, providing text messages to the control group was intended to increase participation rates; however, it is possible that it had an impact on the results. Therefore, for future studies, it is recommended to carefully consider the selection of intervention methods for the control group, taking into account the potential influence on outcomes.
The QOL scores were also found to change in a similar pattern to that of CRF. Both groups had significant within-group improvement in QOL scores from baseline to every follow-up point. However, there was no significant difference between groups in QOL at any assessment point. Similarly, this result might be due to the natural change in QOL over time, as QOL has been reported to improve over time for most BCS as they transition from treatment to survivorship during the 2 year post-diagnosis. 37 In line with this finding, a prior study found lower QOL among BCS immediately after diagnosis compared with individuals without cancer; however, the QOL became similar to that of cancer-free counterparts after 2 years. 38 Most of our participants were less than 2 years post-diagnosis; therefore, it is possible that their QOL naturally stabilized, regardless of the intervention. Another possible explanation for this is the non-specific effect that is similar to the placebo effect 39 on the control group. While the control group only received written material and identical motivational text messages were sent to both groups, it is possible that the control group may have perceived this as an additional sense of connection and support that added to improved QOL. Given that studies have reported the role of the placebo effect in occasioning the psychological benefits associated with exercise, 40 future studies including placebo groups in randomized controlled trials are recommended to further elucidate exercise impact on QOL. This finding also suggests that any additional motivational support in the early survivorship stage may help improve QOL in BCS
The physical activity scores of the BLESS group participants showed the greater increase post-intervention; however, both groups reported similar scores at 1 month and 6 months post-intervention. Although the BLESS participants showed a rapid increase in physical activity the control group caught up with the increased amount of physical activity over the longer period of time. While it is difficult to provide a reason for this, the participants’ working status could have had an effect on the physical activity scores. The control group participant was found to be more likely to work than the experimental at one-month post-intervention. However, no statistically significant difference was found between the 2 groups regarding this result.
Anxiety was significantly decreased compared to the baseline at 1 month and 6 months post-intervention in both groups. Those results are by previous studies indicating that an exercise intervention resulted in decreased anxiety at 12 weeks follow-up. 41 Our study supports the effectiveness of an exercise intervention in reducing state anxiety in BCS.
This study was limited by the small size and mostly included BCS in early survivorship stages. Future studies that expand the sample size and extend to BCS at longer survival periods may be helpful in better determining the effects of exercise adherence programs and their translatability to clinical practice. However, this study reported on long-term effects, up to 6 months post-intervention, offering insight and implications for cancer survivorship.
Conclusions
Our results demonstrate that the 12-week BLESS program showed improvements in behavioral/severity CRF and physical activity post-intervention. However, the effect was not maintained at 1 month and 6 months post-intervention. Both the experimental group and the control group showed significant improvement in CRF, QOL, and anxiety domains compared with the baseline. Future studies that expand the sample size and extend to BCS at longer survival periods may be helpful in better determining the effects of exercise adherence programs and their translatability to clinical practice.
Footnotes
Acknowledgements
We wish to acknowledge the breast cancer survivors who participated in our study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Basic Science Research Program through the National Research Foundation for Korea (NRF) and funded by the Ministry of Education (grant number: 2015R1D1A1A01059846). This trial is registered with Korean Clinical Research Information Service (KCT0005763).
Ethical Statements
The study protocols received ethical approval from Severance Hospital, Korea (IRB 4–2017–0164).
A Data Availability Statement
The data that support the findings of this study are available upon request to the corresponding author.