
Abstract
Purpose:
Allogeneic hematopoietic stem cell transplantation (HSCT) can have a long-term impact on patients’ sexual functioning and consequently, their relationship satisfaction. This study aimed to examine the feasibility and acceptability of a 5-session psychosexual intervention for HSCT survivors and their partners.
Methods:
To be eligible patients were required to be more than 3 months post-allogeneic HSCT. The intervention comprised 2 components: (1) A psychosexual education session exploring medical/behavioral treatment options for sexual dysfunction, delivered by a specialist nurse; (2) A 4-session Emotionally-Focused Therapy-based relationship education program for couples delivered by a clinical psychologist. Measures assessing relationship quality, sexual functioning, anxiety, and depression were administered pre- and post-intervention. Feasibility was measured via participation rate, adherence and compliance with completing main measures. Acceptability of the intervention was assessed via patient/partner satisfaction surveys.
Results:
Eight of 85 (9.4%) eligible patients and their partners participated in the study. Reasons for declining participation included: feeling uncomfortable due to sensitive nature of intervention; did not have any relationship/sexual function issues; and experiencing ongoing medical issues. Six of 8 couples (75%) attended at least 4 intervention sessions and 5 of 8 (62.5%) completed the main study measures post-intervention. Four couples reported that sexual satisfaction and relationship satisfaction was somewhat or much better post-intervention; 1 reported no change.
Conclusion:
Feasibility criteria were not met, with low enrolment rate, however the intervention was deemed acceptable. Couples who participated adhered to the intervention and considered it beneficial. Further strategies to identify and manage sexual concerns are required.
Keywords
Introduction
Allogeneic hemopoietic stem cell transplantation (HSCT) is a treatment used for patients with hematological malignancies. In HSCT treatment, the patient undergoes high doses of chemotherapy or radiotherapy to eradicate disease, to create a space for donor cells and for immunosuppression. This is followed by infusion of HSCs from a donor.1,2 HSCT survivors may develop graft-versus-host disease (GVHD), an immune response in which the transplanted cells identify the recipient’s body as foreign and attack its tissues. 3 Chronic GVHD can affect any part of the body and is managed using immunosuppressants but this can also result in additional complications. 1
Patients who are eligible for HSCT are often below 50 years of age and are likely to be relatively healthy prior to their diagnosis. Thus, many women and men have active sexual lives prior to commencing treatment. 3 Sexual dysfunction is commonly reported as a side effect following allogeneic HSCT due to the effects of chemotherapy, total body irradiation, and medications for chronic GVHD.
In an Australian study of 421 allogeneic HSCT patients, a large percentage of men reported erectile dysfunction (79%) and decreased libido (61%), while women reported loss of libido (83%), painful intercourse (73%) and reduced enjoyment of sex (68%), as well as vaginal dryness (73%), vaginal narrowing (34%) and vaginal irritation (26%). 4 Women can experience genital tract GVHD as a complication post-HSCT. 5 Long term sexual problems are experienced by some survivors up to 5 to 10 years post-transplant. 6 Treatment agents impact on gonadal functions and can lead to genital tissue sensitivity, atrophy or scarring. 1
Given that an increased number of people are surviving longer post HSCT, 7 it is important to address the long-term of impact of treatment on patients’ sexual health. There are various medical interventions for sexual dysfunction in cancer patients, including hormone therapy options, PDE5 inhibitors, vaginal dilators and vacuum erection devices. In addition to these interventions, studies have shown the importance of addressing the cognitive, emotional, and relationship factors that impact on patients’ sexual health.3,8
There is a dearth of intervention studies that use a multidisciplinary approach (ie, medical management of symptoms and psychosocial counseling focusing on improving attachment security in couples) to improve sexual dysfunction in patients post-HSCT. Existing studies conducted in cancer populations post-treatment have demonstrated mixed findings and limited overall effectiveness, particularly for women. 9
In a pilot study, 47 patients who were at least 3 months post-transplant and indicated that their sexual dysfunction was causing distress were offered a multimodal intervention. The intervention comprised monthly sessions addressing causes of sexual dysfunction and aimed to empower patients to manage their sexual concerns and provided them with interventions targeted to their needs. This included psycho-education that addressed issues such as depression, anxiety, loss of intimacy and problems with interpersonal relationships and communication. 10 Participants reported improvements in satisfaction, interest in sex, orgasm, erectile function, and vaginal discomfort from pre-intervention to posti-ntervention. The intervention was targeted to the HSCT patients, rather than couples.
Given that sexual interactions between couples are complex and sexual dysfunction is associated with a number of couple-related factors, it is important to address patient sexual dysfunction within a couples’ framework. 11 It has been consistently demonstrated that Emotionally Focused Therapy (EFT) for couples can improve relationship satisfaction and these improvements are maintained over time. 12 EFT supports couples to develop a secure attachment bond so that sexual problems can be addressed within the dyad. 13 When a patient and partner perceive each other as a “safe haven,” this allows for the development of a healthy intimate relationship and improved sexual functioning. 14
There is research evidence indicating that EFT interventions for couples have resulted in positive outcomes, 15 particularly in aspects of relationship satisfaction, couple communication, and sexual difficulties. These results have been demonstrated in non-cancer populations, including culturally diverse groups 16 and same-sex couples. 17 There have been few studies of EFT-based research in cancer populations. In one study, 42 patients with metastatic cancer and their spousal caregivers were randomized to receive 8 sessions of EFT. It was found that the intervention group demonstrated an improvement in marital functioning and patients’ experience of caregiver empathic behavior. However, sexual problems were not assessed in this study. 18
The current study aimed to pilot a couples’ intervention that combines medical management of sexual dysfunction with a brief structured EFT-based relationships education program in an allogeneic HSCT population. The primary aim of this study was to examine the feasibility and acceptability of a 5-session psychosexual intervention for HSCT survivors and their partners who were more than 3 months post-transplantation.
Methods
Full details of the protocol have been published previously. 19 The methods of this study are outlined briefly below.
Study Design and Participants
This study was a prospective, single-arm descriptive study of a psychosexual intervention with patient and partner measures administered pre- post-intervention. The study was approved by the Human Research Ethics Committee (HREC) of the Peter MacCallum Cancer Centre (HREC reference number: HREC/53351/PMCC-2019; Project number: 19/54).
Couples were recruited through the Clinical Haematology service at Peter MacCallum Cancer Centre and Royal Melbourne Hospital Allogeneic Transplantation Service in Australia.
Participant inclusion criteria were: Aged ≥18 years old (both patient and partner); more than 3 months post-HSCT to treat a hematological malignancy; in a sexual relationship of ≥1 year but couples did not need to be currently sexually active; both patient and partner were willing to participate in the intervention to address sexual health problems. Participants were excluded from the study if they were suffering from significant or ongoing side effects that might impede their participation and/or had a relapse of disease since transplantation.
Intervention
The intervention comprised 2 components: (1) Psychosexual education about medical and behavioral treatment options for sexual dysfunction. (2) EFT-based relationship education program for couples. The sessions were delivered in-person or via Telehealth, depending on participants’ preferences.
Psychosexual education
A 60-min individual psychosexual education session was delivered to couple participants by a specialist nurse. This session included information about medical and behavioral management of sexual dysfunction (including the use of hormone treatment, topical treatments, lubricants and vaginal dilators for women, and phosphodiesterase type 5 inhibitor (PDE5) inhibitors). The session was delivered using the Permission, Limited information, Specific Suggestions and Intensive Therapy (PLISSIT) model of addressing sexual functioning. The specialist nurse would assess the patient’s needs, review the medical history and consult with the primary hematology treating team if a medical prescription was needed. Following the session, the specialist nurse provided a handover to the psychologist delivering the second component of the intervention (detailed below) so that the program could be tailored to the couples’ goals and the difficulties they may be experiencing.
EFT-based relationship education program for couples
The couples’ relationship education program comprised four 90-min sessions and was delivered to each couple by a clinical psychologist (BP). It used an EFT framework, aimed to assist couples in improving the attachment bond to improve the quality of their relationship and enhance sexual intimacy. 20 The intervention material was adapted from 3 EFT resources developed for couples21 -23 and modified to make it relevant to the HSCT population.
Goals for Session 1 included establishing an alliance with the couple, introducing the program, and giving them an opportunity to talk about how cancer and HSCT has affected their relationship. Session 2 focused on assisting the couple identify attachment fears and strategies that results in a negative interactional pattern and disconnection in the couple relationship. In Session 3 the couple were encouraged to share their fears and needs with each other with a focus on increasing partner responsiveness. Psychoeducation regarding the common impacts of cancer and HSCT on the sexual relationship was also provided. Session 4 explored the couple’s sexual relationship, including view of self, other and the relationship, and how this is related to sexual intimacy after cancer and treatment. Finally, an overview of sessions was provided along with practical ways to nurture the relationship moving forward.
Procedure
Eligible patients were identified by the post-transplant nurse consultant on the research team and sent an invitation letter about the study with a brief description of the psychosexual intervention. Patients were given the option to decline further contact or to ask for further information by returning a reply slip via mail. The patient was followed up via phone after 2 weeks if no response was received. Participants were provided an Information Form if interested and signed informed consent was obtained prior to commencing the study.
Measures
In addition to collecting a range of clinical and demographic data such as cancer type, time since transplant, age, gender, country of birth, ethnicity, marital status, education level and length of relationship, participants were administered measures pre- and post-intervention.
The Patient Health Questionnaire (PHQ-9), 24 General Anxiety Disorder-7 (GAD-7), 25 Perceived Relationship Quality Components Inventory, 26 International Index of Erectile Functioning (IIEF), 27 and Female Sexual Function Index (FSFI) 28 were administered to patients pre-and post-intervention. The Experiences in Close Relationship Scale—Short Form (ECR short-form) 29 was only administered pre-intervention to help to inform the clinician’s delivery of the intervention. Please refer to previously published protocol paper 19 for details about each of the measures listed.
Feasibility of intervention
To measure feasibility, the uptake and completion of the intervention was assessed, including reasons for declining participation or withdrawing from the study. Fidelity of the intervention was assessed through: (1) a review of each session by the clinician administering the intervention using session checklists and (2) objective raters (JG and CS) reviewed 10% of sessions (via audio recordings) to check compliance with session checklists. We anticipated that 90% of the psychology interventions sessions delivered will cover all required material based on the session checklist.
Acceptability of intervention
Patient and partner satisfaction survey
This survey was designed by the research team to determine the patient’s and partner’s experience of the intervention, including aspects they found helpful/ unhelpful and whether there were self-perceived changes in their relationship functioning following the intervention. This survey consists of 11 questions (multiple choice and open-ended items). Patients and partners were asked to complete the survey within 2 weeks of completing the intervention.
Satisfaction survey after each session
Patients and partners were given a satisfaction survey after each of the 4 sessions within the relationship education component of the intervention. The survey comprised 4 questions briefly asking participants what was beneficial from sessions and what could have been done differently.
Data Analysis
Demographic, clinical and feasibility data (including time measures) and survey responses were analyzed descriptively. Patient-reported and partner-reported outcomes were scored according to their manuals and presented descriptively. Feasibility was assessed using previously established criteria (see Table 4) based on other feasibility studies in cancer populations. 30 The Patient/Partner Satisfaction Survey responses were collated and frequency data for each item were reported to determine acceptability of the intervention and its feasibility. Data were managed through REDCap. Free-text items from the patient satisfaction surveys were analyzed through identifying themes in the data using Braun and Clarke’s thematic analysis approach. 31
Results
Participants
Two hundred twelve patients who were at least 3 months post-HSCT were screened for eligibility and 40% (n = 85) met eligibility criteria to be contacted. One hundred twenty-seven patients did not meet eligibility criteria for reasons such as: did not have a partner; experiencing complications or side effects that could impact participation and/or had a relapse of disease since HSCT. Out of the 85 patients contacted, 28 were not interested and 43 declined but did not provide a reason. Fourteen patients expressed interest and 8 consented to participating. Figure 1 demonstrates the recruitment numbers, reasons for declining participation, and intervention delivery process.
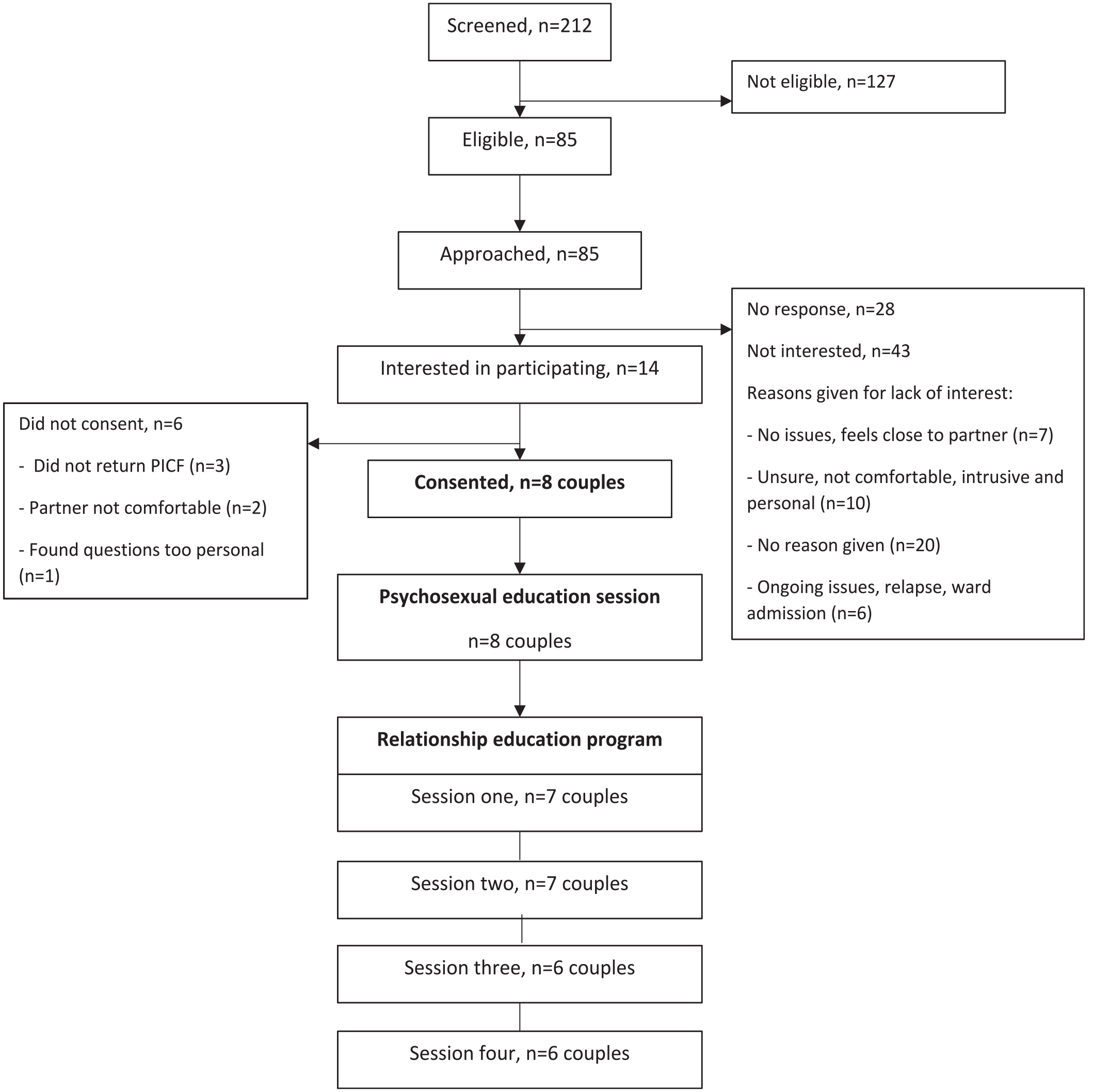
Flow chart of recruitment and intervention delivery.
Demographic and Clinical Data
Mean age of patients who participated was 55.9 years (SD = 8.7 years). 75% of patient participants were born in Australia. Mean length of relationship was 26.1 years (SD = 10.4 years). All patient reported being in a heterosexual relationship. Participants’ demographic and clinical data are displayed in Tables 1 and 2 respectively.
Participant Demographics.

Participants’ Clinical Data.
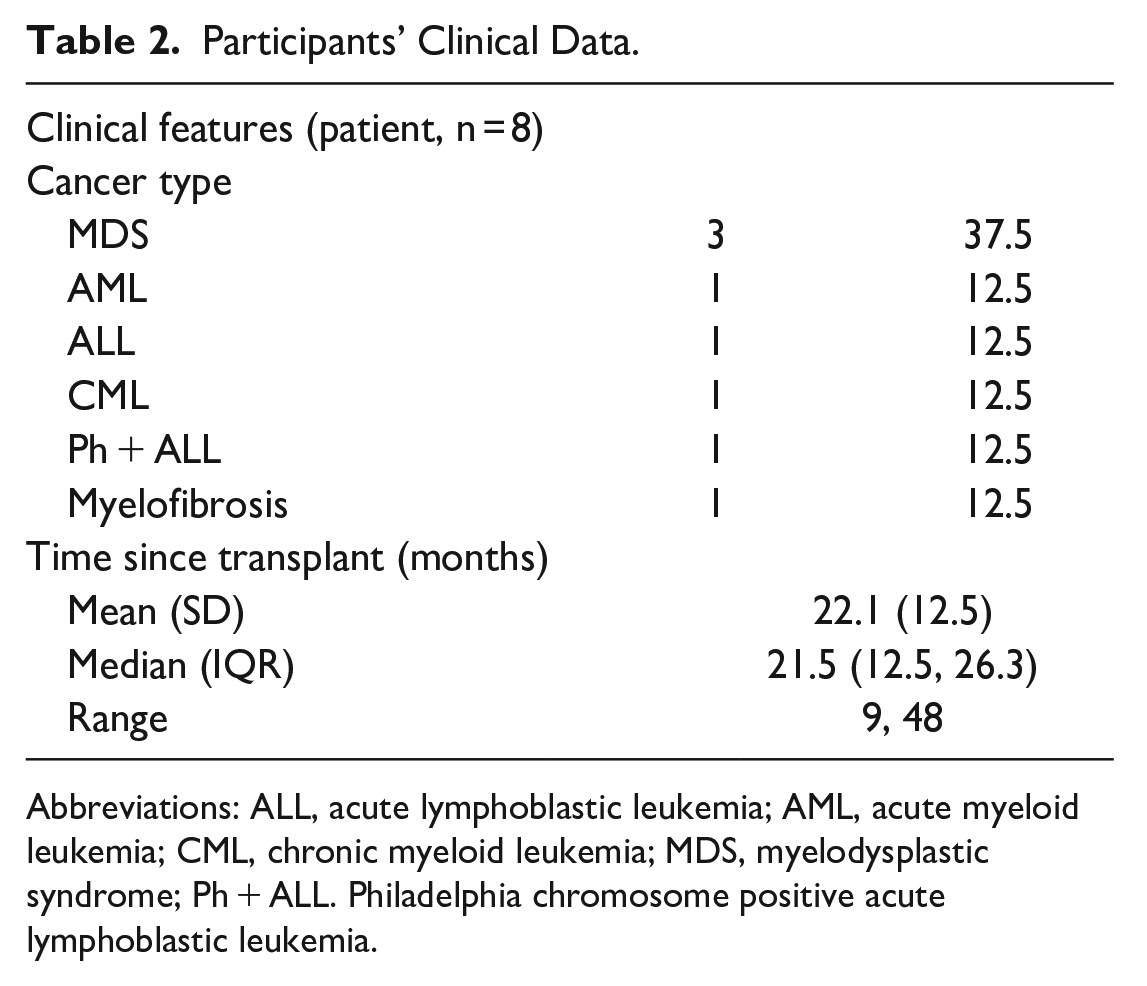
Abbreviations: ALL, acute lymphoblastic leukemia; AML, acute myeloid leukemia; CML, chronic myeloid leukemia; MDS, myelodysplastic syndrome; Ph + ALL. Philadelphia chromosome positive acute lymphoblastic leukemia.
Measures
Table 3 displays the means and standard deviations of scores on measures administered pre- and post-intervention. The scores for the male and female sexual function measures post-intervention were not reported due to only having data for 2 couples for each measure.
Means and Standard Deviations of Scores on Measures Administered Pre- and Post-intervention.
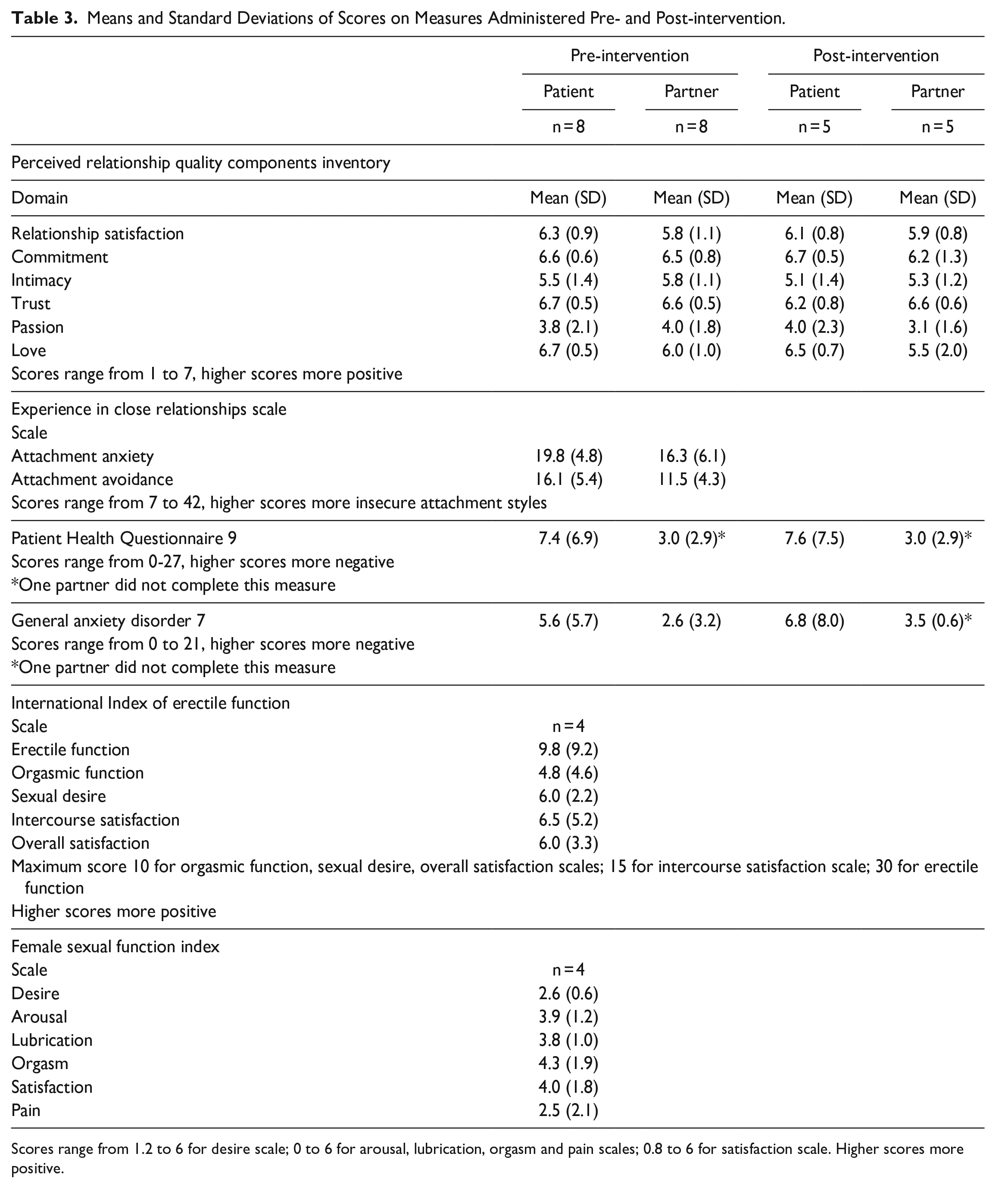
Scores range from 1.2 to 6 for desire scale; 0 to 6 for arousal, lubrication, orgasm and pain scales; 0.8 to 6 for satisfaction scale. Higher scores more positive.
Feasibility
Table 4 displays feasibility data for the study. 9.4% of eligible patients who were approached enrolled in the study. Seventy-five percent of patients enrolled attended at least 4 intervention sessions and 62.5% completed the main study measures post-intervention.
Feasibility.

Fidelity
Independent raters (CS and JG) who rated 4 sessions based on the session checklists indicated that on average 60% of content in the intervention were covered according to the level of detail and order set out in the manual.
Acceptability of Intervention
The intervention was deemed to be largely acceptable by patients and their partners. All patients and partners rated sessions as scoring either 4 or 5 (1 is Poor and 5 is Excellent).
Five of the 8 couples completed questions about their perception of change in sexual and relationship satisfaction. Four patients reported that sexual satisfaction and relationship satisfaction was much better or somewhat better post-intervention while one reported no change. In contrast, 5 partners deemed there was no change to sexual satisfaction from pre- to post-intervention but 4 endorsed changes to relationship satisfaction (“somewhat better”) while one reported no change in relationship satisfaction.
Five patients reported that the changes to relationship and/or sexual function was partly related to the intervention while 3 partners deemed the changes to be partly related, and 1 partner believed it was completely related to the intervention.
All 5 couples (both patients and partners) strongly agreed or agreed that the intervention has helped them better understand issues in their relationship that influenced their sexual wellbeing as a couple.
Qualitative feedback regarding intervention
Thematic analysis revealed 2 major themes: learning new skills and information and having a comfortable space to speak about sensitive issues.
Learning New Skills and Information
Patients and partners highlighted that the intervention facilitated the learning of new skills and provided psychoeducation regarding intimacy and relationships post-transplant. In particular, participants stated that the intervention helped them to identify issues in the relationship they would like to address and the use of practical strategies to increase comfort with intimacy. Participants also expressed that they appreciated learning about relationship patterns, how their behaviors affected each other, and became more aware of their own reactions and that of their partners’. As one patient highlighted, she and her partner found “new ways to talk about feelings.”
Comfortable Space to Speak About Sensitive Issues
Participants expressed that they appreciated having a “safe place” to have an open discussion about their relationship and intimacy issues post-transplantation. They reported that they enjoyed the relaxed nature of sessions and felt relieved that sessions were not “one-sided or critical.” Another participant similarly expressed that they “felt heard.” In addition to having a comfortable therapeutic space, one participant highlighted that he appreciated the balance between following a session plan and having the opportunity to deviate from the set plan to address other topics that arose during the session. Most participants expressed that they enjoyed speaking in more depth about their feelings and experiences as it allowed them to understand each other’s perspectives better, and for some, appreciate the strengths in their relationships.
Suggestions for Improvement to Intervention
One couple suggested having an individual session with the patient and partner by themselves prior to the joint sessions. It was hoped that this would have allowed for more open discussion with the therapist about issues experienced by each person. It was also suggested that 4 sessions were not sufficient, and it would be beneficial to have a follow-up session 6 months following conclusion of the main intervention.
Couples had mixed opinions about content of the intervention. Some couples felt that there should have been more focus on intimacy issues while others felt that communication in the dyad should have been the focus rather than sexual intimacy. One patient highlighted that she would have liked her partner to participate more in the sessions, but it was also confronting to hear what her partner had to say. This resulted in anticipatory anxiety for this patient prior to each session. One couple suggested having more structure in the intervention and being made aware of the content of all 4 sessions at the start of the program.
Discussion
This pilot study aimed to examine the feasibility and acceptability of a 5-session psychosexual intervention for HSCT patients and their partners. Few studies have used an approach that combines medical management of sexual dysfunction and psychoeducation focusing on improving attachment security in couples. Research has increasingly suggested that couples interventions in cancer are an effective means of reducing distress and improving the dyad’s coping and adjustment to cancer. 32 This is particularly important when couples are experiencing stressors associated with undergoing HSCT which has longer-term emotional and physical impacts on the dyad.
In this study, an eligibility time frame of “at least 3 months post-HSCT” was chosen as patients are likely to be experiencing fewer physical side effects of transplantation by that time. Furthermore, an intervention offered to patients at an early stage may be more effectively received compared with providing it at a much later stage post-transplant when relationship patterns may be more ingrained. Given that some patients may need a longer period to recognize sexual concerns post-HSCT, no upper time limit post-transplantation was placed on inclusion of patients into the study. However, it is important to note that in screening participants for eligibility, a sizable proportion of patients reported that they were dealing with various medical issues and ongoing side effects. Hence only 40% of patients screened were deemed as eligible to participate. This is a similar result to a couples-based mindfulness intervention study for breast cancer survivors that identified 42% of patients screened as eligible. 33
Interestingly, only 9.4% of eligible patients decided to participate in the current study. In previous studies assessing couples-based interventions for sexual and relationship concerns in cancer, participation rates of eligible couples have ranged from 26.7% to 53%.33 -35 Notably, one of these studies used a telephone-based intervention and the other was an online intervention, potentially indicating that the intervention placed minimal burden on participants. Reasons for declining in the current study included patients expressing that they or their partners were not comfortable with participation given the personal and sensitive nature of content in intervention. Other patients stated that they had no issues and did not feel they needed the intervention. Several patients declined participation due to experiencing ongoing health issues that required active medical management. In a literature review analyzing the uptake and attrition of couples-based interventions for cancer survivors, it was found that communication-focused interventions and those that required both patient and partner to participate together had low uptake rates. 36 The barriers to participation highlighted in this review included difficulties with accessibility, having competing priorities and severity of illness.
The current study’s intervention was deemed to be acceptable to patients, based on responses in their feedback questionnaire. Patients generally reported that their relationship satisfaction was impacted positively by the intervention. Based on the qualitative feedback, it was apparent that patients and their partners benefited from having a safe space to learn new skills and discuss intimacy and relationship changes post-HSCT. This is in line with the EFT framework which indicates that relationship distress is a result of engaging in negative interaction patterns and change is achieved by helping couples develop new positive interaction patterns that includes mutual sharing of primary emotions and attachment needs, as well as responding to each with attuned support. 13
Couples’ opinions regarding content of the intervention varied, with some preferring a focus on sexual issues while others preferring greater attention to be placed on relationship issues. It was also suggested that both the patient and partner have an individual session with the therapist at the start of the intervention. Having individual sessions with each member of the couple after 1 or 2 joint sessions is commonly practiced in EFT couples’ work. This may be primarily done to foster therapeutic alliance, assess experiences of close relationships (including trauma) throughout the individual’s development to identify and understand attachment strategies in context of developmental experiences. 37
Fidelity testing indicated than an average of 60% of content in the intervention were covered according to the level of detail and order set out in the manual. The authors note that the current intervention was developed as a brief psychosexual and relationship education program. However, in delivering the intervention, the relationship education component was found to comprise a large amount of psychoeducational content, resulting in challenges covering the content as set out in the manual. In addition, couples spontaneously raised issues relating to their relationship and sexual health at different points during the intervention. The clinician delivering the intervention attempted to balance the need to address material couples brought to the session while also delivering the relevant content for each session. Future EFT-based interventions in this setting may benefit from increasing the experiential component of the intervention using EFT skills (eg, evocative questioning to allow couples to access deeper emotions, tracking process, and interactional patterns within session) and reducing the amount of psychoeducational content in each session.
The present pilot feasibility study is limited by small numbers of participants in the intervention and its delivery within a single cancer institution in Melbourne, Australia. Given the small sample size, the findings of the study may not be representative of the experiences of all allogeneic HSCT patients and their partners. For example, all our study participants identified as heterosexual, so we were unable to determine if the intervention would be deemed acceptable to participants of different sexual orientations. In the psychosexual education component of the intervention, couples’ preferred type of sexual experience (eg, penetrative, non-penetrative, oral, anal) was not assessed; hence we were unable to determine the impact of this factor on participants’ experience of the intervention.
In addition, HSCT patients in the present study were in long-term relationships with their partners, so the findings may not be generalizable to couples in new relationships. Also, participants in our study had a median age of 54 years. Given that younger age in women and being pre-menopausal prior to transplant, as well as, older age in men are risk factors for sexual dysfunction post-HSCT, 3 it is possible that younger adult patients may have a different experience of the intervention offered.
Given the small rate of uptake of the intervention, the intervention in its current form may not be feasibly delivered in a sustainable way within this setting. Furthermore, patients who are experiencing significant adverse effects post-HSCT that require ongoing management may be less likely to consent to such an intervention.
Couples who took part in the intervention found it valuable to openly discuss intimacy and relationship issues post-HSCT. However, given that a proportion of patients declined participation due to the sensitive/personal nature of intervention content, it is important to tailor interventions to suit the needs and comfort levels of various HSCT patients and their partners. Participants may be more open to a staged care approach. This could include providing patients with self-help psychosexual and relationship education material regarding potential changes in sexual and/or relationship functioning post-transplantation, and basic strategies and resources they could access to manage these issues. If patients require more intensive support following the self-help intervention, they could then be given the option to access more specialized nursing intervention or EFT-based couple support. This approach may be helpful for couples who find the prospect of opting for a couples intervention daunting and requiring too much investment. Further research is required to determine the feasibility and effectiveness of this approach.
Conclusions
The present study piloted a psychosexual intervention for couples post-HSCT, comprising a single session psychosexual educational component and a 4-session EFT-based relationship education program. Feasibility criteria were not met, particularly in terms of enrolment rate. Couples who did participate adhered to the intervention and found it to be beneficial as they learnt skills to manage relationship and intimacy issues post-HSCT. Future research projects may focus on the utility of offering written self-help material to couples post-HSCT, while also offering them the option to have more specialized couples’ psychosexual intervention and/or relationship education sessions if they wished.
Footnotes
Author Contributions
The authors confirm contribution to the paper as follows:
Conception and design of the work: Pillay, Brindha; Ritchie, David; Panek-Hudson, Yvonne; Jefford, Michael; Garcia, Teresa; Shields, Cassandra; Gniel, Jo; Phipps-Nelson, Jo; Drosdowsky, Allison; Ellen, Steve; Ftanou, Maria.
Data collection: Pillay, Brindha; Garcia, Teresa.
Data analysis and interpretation: Pillay, Brindha, Panek-Hudson, Yvonne, Garcia, Teresa, Gniel, Jo; Shields, Cassandra; Drosdowsky, Allison; Ftanou, Maria.
Drafting the article or critical revision of the article: Pillay, Brindha; Ritchie, David; Panek-Hudson, Yvonne; Jefford, Michael; Garcia, Teresa; Shields, Cassandra; Gniel, Jo; Phipps-Nelson, Jo; Drosdowsky, Allison; Ellen, Steve; Ftanou, Maria.
Approved the version to be published: Pillay, Brindha; Ritchie, David; Panek-Hudson, Yvonne; Jefford, Michael; Garcia, Teresa; Shields, Cassandra; Gniel, Jo; Phipps-Nelson, Jo; Drosdowsky, Allison; Ellen, Steve; Ftanou, Maria.
Agreed to be accountable for all aspects of the work in ensuring the questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved:
Pillay, Brindha; Ritchie, David; Panek-Hudson, Yvonne; Jefford, Michael; Garcia, Teresa; Shields, Cassandra; Gniel, Jo; Phipps-Nelson, Jo; Drosdowsky, Allison; Ellen, Steve; Ftanou, Maria.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a grant from the Peter MacCallum Cancer Foundation, grant number (1839).