
Abstract
Introduction
Cancer patients often report significant symptoms such as fatigue, insomnia, pain, and gastrointestinal symptoms, which can have a major impact on their quality of life (QOL). 1 A systematic review suggested that almost half of cancer patients suffered from pain; the risk of pain was higher in women and African Americans, and pain was associated with depression and disability. 2 Similarly, other studies have examined relationships among common cancer-related symptoms such as fatigue, insomnia, anxiety, and depression.3,4 A recent review of 59 studies suggested that almost all showed a significant correlation of fatigue with depression and anxiety. 4 This prompted a statement by the National Institutes of Health (NIH) calling for more research on symptom management for fatigue, pain, and depression. 5
Integrative medicine (IM) provides patient-centered care and addresses the full range of physical, emotional, mental, social, spiritual, and environmental influences that affect a person’s health. 6 Using a personalized strategy that considers the patient’s unique conditions, needs, and circumstances, IM uses the most appropriate interventions from an array of scientific disciplines to heal illness and help people regain and maintain optimum health. 6
Although the comprehensive and individualized philosophy and approach of IM seems ideal for cancer care, there is little published clinical research that has documented improved outcomes. Two central pillars of IM care—stress management and spirituality—have been associated with greater well-being and coping in cancer patients 7 as well as improved physical function, management of cancer-related symptoms, and QOL.7-13 Spirituality may be most simply defined as a sense of meaning and purpose that usually includes a universal power as a guide and is associated with feelings of comfort, peace, hope, and faith. 8
This analysis describes the characteristics and QOL of 353 cancer patients who sought care at 1 of 8 IM clinical practices that comprise the Bravewell practice-based research network (PBRN), BraveNet. 14 We present lifestyle habits and reasons for seeking integrative cancer care for this cohort (as well as their physical and psychosocial characteristics) and associations. Finally, features of the patients particularly hoping to address spirituality at their IM center are assessed.
Research Design and Methods
Patient Recruitment and Inclusion
The 8 centers that comprised the BraveNet PBRN in 2011 contributed to this analysis. 14 The Duke Clinical Research Institute provided network and study coordination, data management, and statistical support. Each center contributed approximately 500 participants. 14 Clinical research staff approached participants at their visits by phone or mail and invited them to participate. Because not all patients who were approached decided to participate, this was a self-selected cross-sectional sample, and we did not quantify how many patients declined to participate. All participants provided informed consent. Eligible participants were at least 18 years old, English or Spanish literate, and received treatment from or consulted with an IM clinician. Patients enrolled in the study between January 5, 2008, and August 16, 2010.
At their IM visit or within 2 weeks, participants spent 15 to 30 minutes completing the QOL questionnaires described below. A corresponding form, completed by the provider or research staff, indicated the practitioner’s (physicians, nurses, psychologists, acupuncturists, massage therapists, and nutritionists/dieticians) assessment of current medical conditions that were addressed at the IM visit. Study procedures for each clinical center and the Duke Clinical Research Institute received full institutional review board or ethics committee approval.
The cancer cohort described here is comprised of 353 participants who were diagnosed with cancer by self-report, the clinician, or a medical record. They were compared to the larger noncancer cohort (n = 3587) in the BraveNet registry study.
Measures
Participants provided demographic information, including information on gender, ethnicity, race, education, socioeconomic status, lifestyle (exercise, tobacco, and alcohol use), and current symptoms. Individuals with cancer who had 4 or more visits to IM centers were classified as “returning” patients, whereas patients with cancer who had up to 3 visits were deemed to be “new” patients. Participants also reported their current weight and height.
QOL was assessed using the 12-Item Short Form Health Survey (SF12v2) to obtain an estimate of both physical and mental functioning. 15 Mood was assessed with the Center for Epidemiologic Studies Depression Scale (CES-D), and patients’ perception of stress was reported on the 4-item Perceived Stress Scale.16,17 Three self-report Numerical Rating Scales (NRSs) were used to measure pain, fatigue, and restfulness of sleep. On the NRS, participants circled a number between 0 (meaning none—no pain, no fatigue, or not at all rested) and 10 (meaning highest degree) to indicate their experience over the past month.
Finally, participants were asked questions about their reasons for seeking care at an IM practice, including whether they were looking for a setting that “addresses spirituality as an aspect of care.”
Data Analysis
Data were entered/collated via a central database using a secure Web site and confidential identifiers for each participant. Descriptive summaries were presented as means and standard deviations for continuous variables and as frequencies and percentages for categorical variables. Comparisons between groups were assessed utilizing T tests and χ2 tests, respectively. α Was set at .01 to control for type I error, given multiple comparisons. Analyses were performed in SAS (version 9.3, SAS Inc, Cary, NC).
Results
Demographics and Cancer Types
The 8 participating IM centers enrolled 353 cancer patients into the study between January 5, 2008, and August 16, 2010. The majority of participants were white (85.9%) and female (76.4%), with a mean age of 55.0 (11.8) years (see Table 1). The participant group was highly educated (80.4% completed college), and the majority of participants were married (55.6%). The most common cancer diagnoses were breast cancer (45.3%), hematological malignancies (9.9%), and colorectal cancer (7.1%). Less-frequent malignancies included prostate (5.7%), ovarian (4.8%), lung (4.0%), pancreatic (3.9%), head and neck (3.9%), and other cancers (15.6%).
Characteristics for Participants With Cancer, Compared With Noncancer Cohort.

Versus >5/wk.
Lifestyle Indicators
Current tobacco use in the cancer cohort, as in the noncancer cohort, was virtually absent, although significant numbers of these patients had prior smoking histories. The average number of days per week that alcoholic beverages were reportedly consumed was 1.5 (2.1). The percentage of the cancer group indicating no current alcohol use was 49.0% and was significantly higher than that in the noncancer cohort (40.8%; P < .01). Average BMI for the cohort was 24.7 (5.2) kg/m2, with 38.4% in the overweight or obese range.
Patient Symptom Profiles
The mean number of years that participants lived as a cancer survivor was reported to be 4.4 (5.5) years. More cancer patients were seen as “new” patients compared with noncancer patients: 58.4% versus 38.8%, respectively (P < .01). There was a trend toward a higher percentage of cancer patients being referred to the IM center by a physician than noncancer patients (31.8% vs 27.3%; P = .07). Current medical conditions and symptoms were collected for a subset of 236 participants for whom the data were available. The most common comorbidities included: chronic pain (39.8%), fatigue (33.5%), insomnia (23.3%), and anxiety (20.3%). Practitioners were able to indicate multiple conditions for a given patient.
QOL, Perceived Stress, Depression, and Sleep Quality
QOL scores on the SF12v1—87.8 (15.36)—were below the national norm of 50.0 (10.00) on both the physical component score—43.3 (11.41)—and mental component score—44.6 (10.75; see Table 2). Perceived stress (5.6 vs 5.8; P = .31) and depression scores (8.7 vs 8.5; P = .60) were equivalent among cancer patients and those without cancer. The proportion of participants classified as depressed, indicated by a CES-D score > 16 (13), was not significantly different between cohorts (15.2% vs 14.6%; P = .76). The cancer patients’ scores on the NRS for fatigue (5.1 vs 4.9; P = .04) and sleep quality (6.0 vs 5.9; P = .43) were comparable with that of the noncancer cohort. There was also a difference in average pain between cancer and noncancer patients—2.6 versus 3.3, respectively—favoring the cancer patients (P < .01). This is likely explained by the fact that 42.8% of the IM noncancer cohort were seen for acute (9.7%) or chronic (33.1%) pain. 14
Scores for Quality of Life and Symptoms: Cancer Versus Noncancer Cohort.

Abbreviations: SF, short form; CES-D, Center for Epidemiological Studies Depression Scale (Seeking Spirituality).
Indicates better health.
Indicates likelihood of clinical depression.
In the cancer cohort, perceived stress, a surrogate for anxiety, was significantly correlated with depression (P = .01). Perceived stress was also correlated with fatigue (P < .01), sleep (P < .01), and average pain (P < .01). Finally, perceived stress was inversely correlated with the overall SF12 QOL score (P < .01) as well as the SF12 physical score (P < .01) and the SF12 mental score (P < .01).
Seeking Spirituality as a Component of Care
Overall, 52.4% of the cancer cohort reported seeking a clinical care setting that addressed spirituality as part of their care, comparable with that in the noncancer cohort (58.7%). Cancer patients seeking spirituality had significantly more depression (10.1 vs 7.1; P < .01), perceived stress (6.2 vs 4.9; P < .01), and average pain (3.0 vs 2.1; P < .01) than those not looking for this aspect of care. Although this was also observed in the noncancer cohort, noncancer patients seeking spirituality as an aspect of their care also indicated poorer health status according to the physical component of the SF12v1 (44.1 vs 45.9; P < .01) and on the sleep (5.7 vs 6.3; P < .01) and fatigue (5.2 vs 4.4; P < .01) scales.
Discussion
Our data suggest that cancer patients seeking treatment at IM clinical practices are similar to those who seek IM care for other conditions. Thus, they are more likely to be female, married, well educated, and of a higher socioeconomic status. At the same time, they are typical of other cancer cohorts in terms of comorbid symptoms such as pain, fatigue, and insomnia and psychological characteristics such as depression and perceived stress.1-5
These data are consistent with those from other studies that have shown a highly significant correlation between depression and anxiety (perceived stress was used as a surrogate) and between anxiety/depression and fatigue. 4 Our data only partially supported this relationship because we did find a correlation between perceived stress and depression, and between perceived stress and fatigue, but there was only a trend in the relationship between depression and fatigue (P < .07). Cancer-related fatigue is one of the most common and distressing symptoms faced by survivors and is present in up to 40% at diagnosis, 90% undergoing radiation therapy, and 80% receiving chemotherapy. 18 Because of the multifactorial influences and characteristics of fatigue, researchers and clinicians alike are increasingly interested in how fatigue might be improved through an integrative approach to care. One challenging question in cancer patients is how much of the fatigue may be related to coexisting depression.
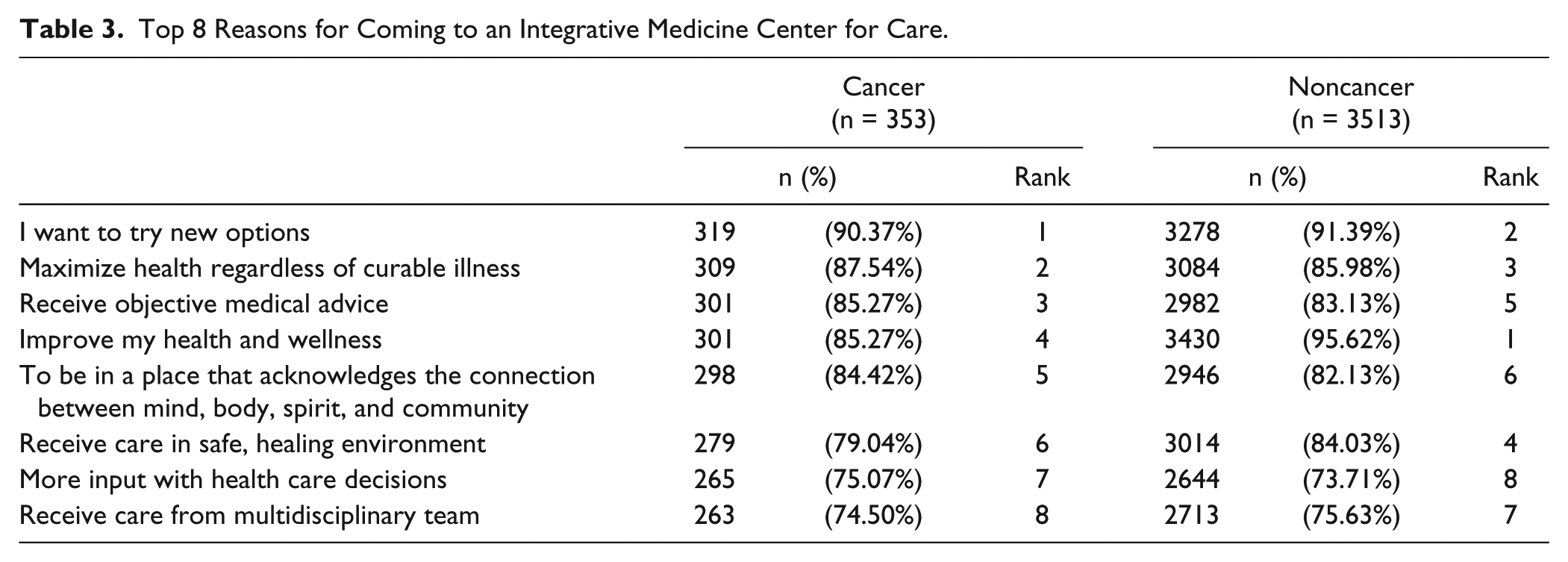
As shown in Table 3, there are only minor differences in the ranking of reasons that cancer patients and noncancer patients gave for attending IM clinical practices. The only reason for pursuing IM care that we examined in more depth was “seeking a health care setting that addresses spirituality as an aspect of care” because this is one of the hallmarks of integrative care, and we wondered if this might influence their characteristics.
Top 8 Reasons for Coming to an Integrative Medicine Center for Care.
Compared with other IM cancer patients, those seeking IM to address spirituality had significantly worse psychosocial characteristics (perceived stress, depression, and pain). This suggests that their interest in spirituality and possible desire or need to engage in one or more spiritual practices may be to help improve these measures because research has found that spirituality is associated with less anxiety and depression and with greater resilience. 19 Clinicians should be aware of this relationship and make appropriate referrals to pastoral and other counseling services.
Most research in spirituality and health is cross-sectional, making it more difficult to examine how it might change over time. 20 A recent study, however, did show a longitudinal effect of relaxation and meditative practices that produced both psychological benefits and biological improvements, 21 and this may be an example of involvement with a spiritual practice or spirituality over time that produced important health-related effects. Additionally, most of this research is descriptive in nature, and definitions of spirituality and spiritual well-being are quite heterogeneous. A recent study examining the multidimensionality of spirituality found that the 3-factor model (peace, meaning, and faith) of the Functional Assessment of Chronic Illness Therapy–Spiritual Well-being was superior to previous models because of its greater discrimination between key spirituality factors (peace, meaning, and faith) and others that may be less important. 22
The other important finding in this research is that perceived stress was significantly positively associated with depression, fatigue, insomnia, and pain, and significantly inversely associated with overall QOL and the physical and mental subscales. Future research should evaluate these relationships, try to confirm these findings, and determine what integrative medical modalities could improve perceived stress and potentially affect these other physical and emotional symptoms.
An important limitation of this study is that the data are a cross-sectional view of cancer patients with various types of and in various stages of disease, in different phases of treatment or posttreatment follow-up, and seeking a range of services from IM clinical practices. Nonetheless, there are no other comprehensive descriptive reports of cancer patients seeking IM care, and it is helpful to identify relationships among psychosocial characteristics, symptoms, and QOL to inform treatment.
Future research should examine the potential benefits of integrative interventions for leading comorbid symptoms and QOL. In addition, providers can consider whether it would be beneficial to routinely assess perceived stress and spirituality or spiritual well-being, appreciating its potentially significant relationship to depression, fatigue, insomnia, pain, and QOL. An increasing and targeted evidence base for integrative cancer care may positively affect patient QOL and outcomes regardless of where patients are in their cancer journey.
Footnotes
Acknowledgements
The Bravewell Collaborative funded the creation of BraveNet and this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research and the BraveNet practice-based research network was funded by the Bravewell Collaborative, a nonprofit organization.