
Abstract
Objective. The purpose of this randomized controlled trial (RCT) was to examine the feasibility and acceptability of a Tai Chi Chih (TCC) intervention in senior female cancer survivors with physical functioning limitations, and its effects on health-related quality of life (QOL). Design. This was a two-armed, parallel group, RCT with 12-weeks of Tai Chi Chih or Health Education Control. Methods. Sixty-three senior (M age = 67 years, SD = 7.15) female cancer survivors (83% breast cancer, stages I-III) with physical functioning limitations (SF-12 Health Survey role-physical & physical functioning subscales) were randomized to 12-weeks of TCC or Health Education control (HEC). Primary outcomes were feasibility and acceptability. Secondary outcomes included health-related QOL (SF-36 Health Survey), and participants’ qualitative feedback on the intervention. Results. Retention (TCC = 91%; HEC = 81%) and class attendance (TCC = 79%; HEC = 83%) rates, and satisfaction levels for both study arms were high, but did not significantly differ from one another. At one-week post-intervention, none of the SF-36 scores differed between the TCC and HEC groups. Within-group analyses revealed significant improvements in the mental component summary score in TCC (p = 0.01), but not in HEC. Qualitative analyses indicated that the TCC group felt they received mental and physical benefits, whereas HEC group reported on social support benefits and information received. Conclusion. The TCC intervention was found to be a feasible and acceptable modality for senior female cancer survivors. Future, larger definitive trials are needed to clarify TCC dosage effects on QOL in this vulnerable population.
Keywords
Introduction
Cancer survivors are living longer past their cancer diagnosis as a result of advances in early detection and treatment. In 2008, there were 11.9 million cancer survivors, a large proportion of whom were of an older age range (35% were 40-64 years of age, and 60% were ≥65 years of age), and 15% had been diagnosed ≥20 years earlier. 1 Although this is encouraging, it also means that more survivors may experience the late effects associated with cancer and/or its treatment, and for senior survivors, these effects can be compounded by age-related comorbidities. 2 Senior survivors report worse physical health status (eg, daily living activities and increased disability)3-5 and more difficulty with household activities that require strength and mobility than healthy controls. 6 They additionally report more fatigue, anxiety, and depression than the general population, all of which can adversely affect quality of life (QOL).7-10 Survivors are also at a greater risk than the general population for developing second primary cancers and other chronic diseases (eg, lung, cardiovascular, arthritis, diabetes mellitus, pain, and incontinence).3,4,7 For senior cancer survivors suffering from these late effects in addition to age-related comorbidities, QOL may be as important as overall survival time. 11 Clearly, there is a need for interventions that can help improve QOL for senior survivors.
Tai Chi (TC) is a mind-body exercise, also known as meditative movement, which incorporates both physical activity and stress-reducing aspects. It has been established as safe and effective in improving QOL for younger female cancer survivors and healthy elderly populations12-15; however, it has not been studied in older female cancer survivors. TC has ancient origins in China, where it was first used as a form of martial arts and later for health purposes. 16 It is a moderate-intensity exercise 17 that uses slow, deliberate movements coordinated with breath and imagery to strengthen and relax the body and mind, with the purpose of moving one’s life energy (qi).16,18 There is a growing body of evidence that TC confers both physical and mental health benefits, including improvements in physical functioning, balance, bone density, cardiovascular outcomes, immune function, sleep quality, QOL, depression, anxiety, and self-efficacy in older adults and breast cancer survivors.13,15,19-21 A condensed form of TC, known as Tai Chi Chih (TCC), has been designed for senior populations and may be particularly attractive for senior cancer survivors because it comprises gentle movements, is safe, easy to follow, and can be practiced in practically any setting. 22 Using this form of TCC, interventions in healthy elderly adults have reported improved QOL, sleep quality, and responses to pharmacological treatment of depression.13,23,24 Similarly, Tai Chi Chuan, another TC form, has been associated with health-related QOL, self-esteem, and improved functional capacity in breast cancer survivors.21,25 Presumably, these benefits would also extend to senior cancer survivor populations who are experiencing or are at risk for declines in QOL; however, a TCC intervention has not been scientifically evaluated in this population.
The purpose of this study was to examine the feasibility and acceptability of a 12-week TCC intervention, compared with a 12-week Health Education control (HEC), in senior female cancer survivors with some limitations in physical functioning (Short Form [SF]-12 Health Survey physical functioning or role physical subscales). Additionally, because many senior survivors experience declines in QOL as a result of late effects coupled with age-related declines, we also explored the effects of the TCC intervention on mental- and physical-health QOL. We focused on survivors with physical functioning limitations because a TCC intervention in older adults found that those with baseline impairments in physical functioning benefited the most from TCC, 14 and declines in physical functioning are very relevant in long-term older survivors. 2 Furthermore, we focused on female survivors in order to extend previous research on TC in breast cancer survivors that found QOL benefits.21,25 The results from this randomized controlled trial (RCT) provide important information regarding the design of a future, larger definitive RCT in this understudied, vulnerable population of senior female cancer survivors.
Methods
Study Design and Participants
This was a 2-armed, parallel-group, feasibility RCT guided by the Consolidated Standards of Reporting Trials (CONSORT) statement (Figure 1). 26 A single-blinded design was not followed because informed consent procedures required that participants be informed that they would be randomly assigned to either TCC or HEC; statisticians were blinded to study arm allocation. The study was approved by the University of Utah Institutional Review Board and registered at ClinicalTrials.gov (Identifier NCT01305044). Power calculations using a 2-sample t test indicated that a sample size of 21 in each arm would be sufficient to detect a change of 15 points on the SF-36 role-physical and physical functioning scores, assuming a standard deviation (SD) of 15, with 88% power at a 5% significance level. We increased the sample size to 63 to allow an approximate drop-out rate of 30%. However, this was a pilot trial with the purpose of establishing acceptability and feasibility in this population and to provide data to calculate the sample size required for a larger, more definitive trial.
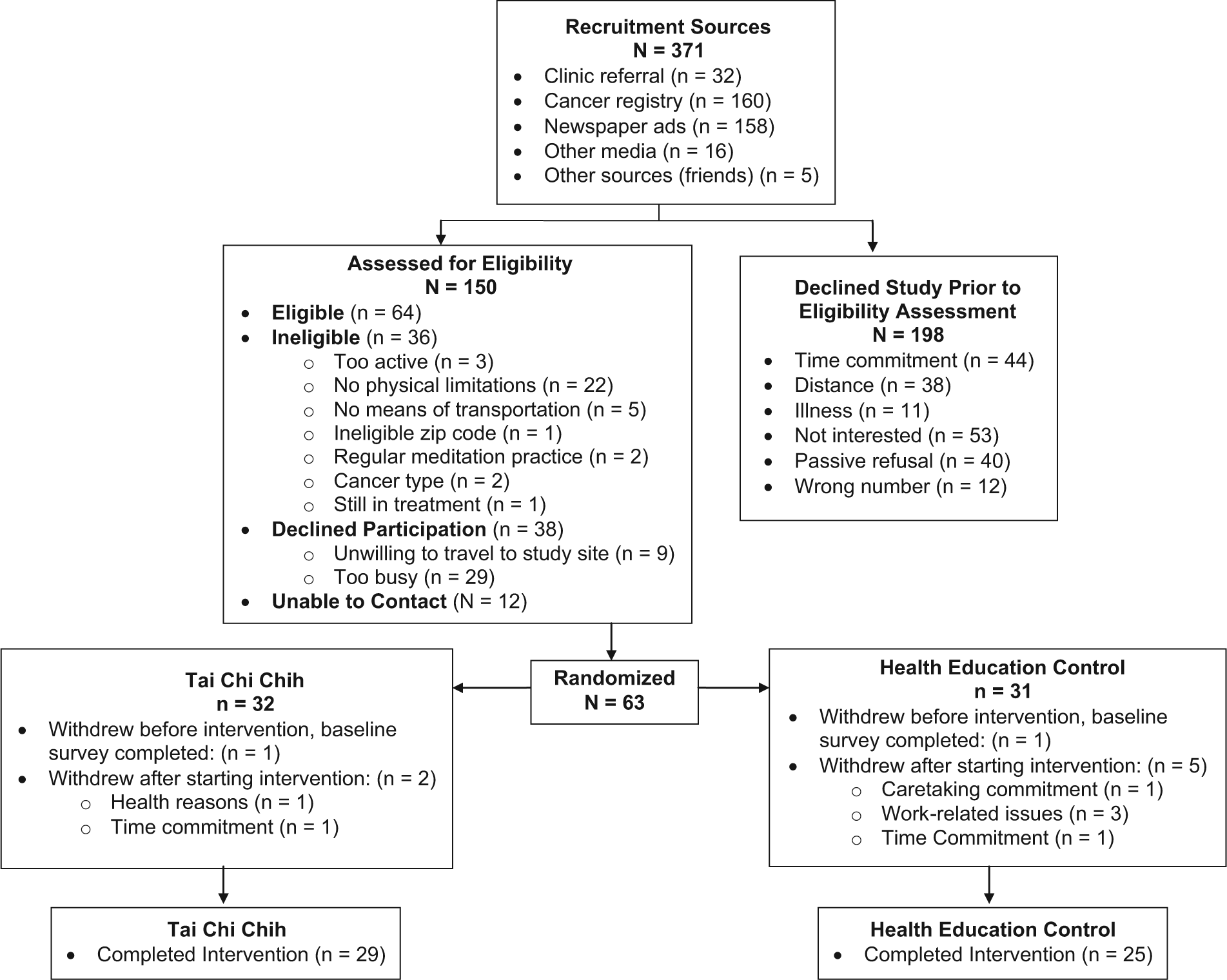
CONSORT diagram.
Senior female cancer survivors were recruited via Huntsman Cancer Institute (HCI) Tissue Resource & Applications Core registry, Huntsman Cancer Hospital clinics, and community advertisements (media and newspapers). The study was advertised as aiming to help senior female survivors improve QOL. A research coordinator contacted potential participants to discuss study details and to assess their eligibility. Inclusion criteria were as follows: (1) age ≥55 years; (2) treatment of solid tumor cancers, stages I-III (excluding cancers that result in a limited life expectancy: lung, stomach, blood, pancreas, brain, or liver); (3) ≥3 months since completing treatment (exception of hormone therapy), with no detectable cancer; (4) residence within 30 miles of HCI and able to travel; (5) spoke and read English fluently; (6) physician’s medical release obtained; and (7) willing to be randomized to study arm. Exclusion criteria were the following: (1) engaged in focused, intense physical activity (ie, activity where heart beats rapidly 27 ) for 30 minutes or more a day, 3 days per week; (2) prior experience with TC, yoga, qigong, or meditation within the past 6 months; (3) inability to pass the Folstein Mini Mental Status Exam (score ≤23); (4) health conditions (ie, cardiovascular or neurological problems) that could interfere with intervention; and (5) SF-12 Health Survey physical functioning score >80 or role-physical score >72. Individuals with some physical functioning limitations (ie, SF-12 physical functioning, role-physical subscales) were enrolled because they may be most likely to benefit from a TCC intervention. Physical functioning limitations included limitations in performing physical activities such as carrying groceries, climbing stairs, and so on (ie, physical functioning subscale) and problems with work or other daily activities as a result of one’s physical health (ie, role-physical subscale). 28 The role-physical and physical functioning cutoff scores have been used in another TCC trial to identify low-functioning older adults, which also found that such impaired individuals benefited the most from TCC. 14 Note that the shorter SF-12 version, rather than the longer SF-36 version, was used to reduce respondent burden; these versions are highly correlated. 29
Measures
Retention, class attendance rates, and number of adverse events assessed the feasibility of the intervention. At baseline and 1 week postintervention, participants completed the SF-36v1 Health Survey, 30 which assesses QOL with 8 subscales and summary scores for mental health and physical health (Mental Component Summary [MCS] and Physical Component Summary [PCS]; internal consistency reliability = 0.65-0.94). 30 The SF-36v1 data were scored with the QualityMetric Health Outcomes Scoring Software 4.0. The score range is 0 to 100, with higher scores indicating better quality of life. At 1 week postintervention, single-item scales assessed study satisfaction and intention to continue TCC or the HEC group’s intention to exercise after completion of the study. Finally, 3 open-ended questions assessed what participants liked and disliked about the study arm and recommendations for future studies.
Intervention
After completion of the baseline survey, HCI’s Research Informatics Core randomized participants to a study arm (TCC or HEC) using blocks of varying sizes (2-4) to minimize predictability of assignment. The TCC and HEC 60-minute sessions occurred 3 times a week, over a 12-week period, at the same time of day. The intervention period was set at 12 weeks to be an acceptable length in this senior sample for whom time commitment (ie, time required to attend classes and for traveling) is a barrier to engaging in physical activity. 31 Furthermore, most physical activity interventions for cancer survivors are held for 2 to 3 days a week for 10 to 24 weeks, 32 and TC studies of a 12-week period have found QOL effects.12,25,33,34 Make-up classes were not offered; however, the TCC participants were provided a DVD of the instructor performing the TCC movements (data were not collected on home practice). Because of space limitations, the HEC classes were held at HCI, whereas the TCC sessions were held at a senior center within 2 miles of HCI. Attendance to sessions was recorded by study staff. Participants were asked not to begin new physical activity during the study.
The TCC intervention was a Westernized form that is safe for senior populations 15 and was led by an experienced instructor certified in this form. It consisted of 19 simple, repetitive, nonstrenuous movements and 1 standing pose (Table 1; also see www.taichichih.org/movements). Participants were informed that all movements could be performed sitting if needed. Each session began with a 20-minute warm-up that consisted of a seated meditation, self-massage of acupressure points, and light stretching, followed by 30 minutes of TCC movements and 10 minutes of closing movements. Each week 1 to 2 new movements were added, until the entire form was practiced during the last 3 weeks. The HEC classes served as an attention control group and focused on topics relevant to aging (eg, successful aging, pain, nutrition, sleep changes, social roles, and relationships), with the majority of topics spanning 2 classes. These classes were led by a variety of health specialists, such as gerontology oncologists, nutritionists, physical therapists with specialization in aging issues, social workers, and health promotion specialists. The HEC classes were held in a small meeting room and were structured to be an interactive environment between the participants and the presenting health specialist. There were no at-home assignments associated with the HEC classes.
Tai Chi Chih Movements.

Data Analysis
Comparisons of the sociodemographics of the 2 study arms at baseline were assessed using Pearson χ2 tests for categorical data and Wilcoxon tests for continuous data. Wilcoxon nonparametric tests were used because the data were appreciably skewed. To assess the feasibility and acceptability of the intervention, retention (ie, proportion of participants who remained enrolled and completed postintervention measures) and attendance rates (ie, for those who did not withdraw, number of classes attended divided by total possible classes) were calculated, and study arms were compared with Fisher’s exact and Wilcoxon tests, respectively. Additionally, Wilcoxon tests assessed participants’ level of study satisfaction and intention for TCC participants to continue practicing TCC or HEC’s intention to start exercise after study completion. For the SF-36v1 subscales and the MCS and PCS scores, analysis of covariances (ANCOVAs) were used to test the differences of study arms at postintervention while controlling for baseline values. 35 Baseline values were used to control error and increase the precision to which the study arm effects could be measured by removing effects that may not have been effectively controlled by randomization.
Because the purpose of this pilot trial was to determine its feasibility in senior female cancer survivors, success criteria for feasibility were considered to be 70% completion of postintervention measures (retention) and 80% mean adherence to TCC and HEC sessions (attendance) over the 12-week study period. Per protocol analyses were conducted on participants with complete data at baseline and postintervention, with statistical programs SAS (version 9.2) and R (version 2.12.2). Intent-to-treat analyses were not used because we did not have postintervention data on participants who withdrew from the study to conduct complete case analyses, and our sample size was too small to conduct multiple imputation techniques. Below, we report results comparing SF-36 MCS and PCS baseline scores of withdrawn participants with those of participants who remained enrolled. Statistical significance was based on an α of .05; however, generally, the emphasis in pilot studies should be on feasibility and less on statistical significance. 36
Finally, participants’ comments for the open-ended questions of what they liked and disliked about the assigned study arm and study recommendations were analyzed using a qualitative content analysis approach.37-39 This is an inductive approach that derives coding categories from the data, rather than applying preconceived categories. The process consisted of 2 independent coders (RAC, KO’C) first reviewing all comments to get a sense of the data; codes were developed that best categorized the comments, and then, the reviewers independently coded each question’s comments while blinded to study arm. High interrater agreement between the 2 reviewers was met for each of the 3 questions (Cohen’s κ >0.85, percentage agreement >89%).
Results
Feasibility and Acceptability
As shown in the CONSORT diagram (Figure 1), 371 female cancer patients were contacted for recruitment or called the study line in response to advertisements; 40% (n = 150) expressed an interest in participating, and of these, 42% (n = 63) were randomized. The study arms did not differ significantly with respect to baseline sociodemographic data (Table 2). Among the participants, 83% had a history of breast cancer (TCC = 78%; HEC = 87%); other types included colorectal, ovarian, cervical/uterine, thyroid, bladder, and nasopharyngeal. The mean time since cancer diagnosis was 9.96 years (SD = 9.2 years) and 12.94 years (SD = 9.7 years) for the HEC and TCC arms (P = .11), respectively. The retention rate for the 12-week intervention was good (overall retention = 86%; TCC = 91% [3 out of 32 withdrew]; HEC = 81% [6 out of 31 withdrew]; P = .44). Furthermore, participants’ attendance to the 12-week period of 3 classes per week was good (overall attendance = 81%; TCC = 79%; HEC = 83%; P = .36; also see Figure 2). The percentage of participants who attended ≥80% of possible classes was as follows: HEC, 76% (19 out of 25 participants who remained enrolled); TCC, 55% (16 out of 29 participants who remained enrolled); P = .18. At postintervention, both study arms expressed high satisfaction with the assigned study arm, but did not differ significantly (TCC: median = 1.00, interquartile range (IQR) = 0.45; HEC: median = 1.11, IQR = 0.55; P = .08; 0 = strongly agree to 4 = strongly disagree). Similarly, at postintervention, both study arms expressed high levels of intention to continue TCC or, in the case of HEC, start exercising after study completion, but did not significantly differ from one another (TCC: median = 0, IQR = 1.0; HEC: median = 0, IQR = 1.0; P = .66; 0 = strongly agree to 4 = strongly disagree). Participants were asked to record their physical activity over the course of the intervention to ascertain whether TC may have been practiced in the HEC arm. A review of these records confirmed that none of the participants in the HEC arm had practiced TC during the study. Finally, there were no adverse events to report. At the start of the TCC classes, 4 participants sat during a majority of the movements. However, after 3 weeks, 3 of these participants were standing for a majority of the movements, and the fourth participant increased standing time after 6 weeks of TCC classes.
Baseline Characteristics of Participants by Study Arm. a

Abbreviations: TCC, Tai Chi Chih; HEC, Health Education Class.
Unless specified, values represent percentage (n). Wilcoxon tests were used for continuous data, and Pearson χ2 tests were used for categorical data. Mantel-Haenszel χ2 was used if cell <5.
Values reflect median (range).
Value is other racial category not specified.
Includes divorced, separated, never married, and widowed.
One person’s data missing from HEC.
Income not reported for 2 TCC and 4 HEC participants.
Data missing for 2 TCC and 3 HEC participants.

Participants’ percentage of class attendance by study arms.
MOS (Medical Outcomes Study) SF-36 Quality of Life
Comparisons of the baseline SF-36v1 subscales and summary scores for participants who withdrew and those who completed the study revealed significantly lower MCS (P = .04) and a trend for lower vitality (P = .06) in those who withdrew from the study. We also assessed whether the length of time since participants’ completion of their cancer treatment may have affected QOL, such that participants closer to their cancer treatment would report worse QOL than those further from their cancer treatment. To examine this, we dichotomized the baseline sample into participants who had completed their cancer treatment between the years 2005 and 2010 and participants who had completed their cancer treatment earlier than 2005. Comparisons of the baseline SF-36v1 subscales and summary scores on these 2 treatment-time groups did not reveal any significant differences (all P >.05). Notably, our entire sample’s baseline SF-36 subscale scores were lower than those for the general US female population of similar ages (see supplementary table); however, this may be reflective of our eligibility criteria (physical functioning limitations).
For participants who completed the study (n= 54), the study arms were not significantly different on the baseline MOS SF-36 subscales or the MCS and PCS scores (see Table 3 for medians). ANCOVA results did not reveal significant differences or trends between study arms for the SF-36 subscales or the MCS and PCS scores at postintervention (all P >.05; Table 4), although a large proportion of participants in both study arms had more improvement than decline (see supplementary figure). Wilcoxon signed-rank tests were used to examine whether significant changes in MCS and PCS occurred within each study arm. These tests were used instead of t tests because the data did not meet assumptions of normality. These results indicated that the TCC group had improved MCS scores at postintervention (P = .01), but not PCS scores (P = .71). Similar analyses for the HEC group suggested trends for improved PCS (P = .06) and MCS (P = .07) at postintervention.
Health-Related Quality of Life SF-36v1 Median Values for Baseline, Postintervention, and Change. a

Abbreviations: TCC, Tai Chi Chih; HEC, Health Education; LL, lower limit; UL, upper limit; MCS, Mental Component Summary; PCS, Physical Component Summary (higher scores indicate better functioning).
Values are given only for those participants who completed the postintervention survey. Change reflects the median change within participants from baseline to postintervention.
Health-Related Quality of Life SF-36v1 Postintervention Adjusted Means for Subscales and Summary Scores. a

Abbreviations: TCC, Tai Chi Chih; HEC, Health Education; Madj, adjusted mean; SE, standard error; MCS, Mental Component Summary; PCS, Physical Component Summary.
The data (adjusted means) in Table 4 are presented as tied to the ANCOVA analysis on postintervention scores; thus, change scores are not included in this table because these were not used in the analysis. Higher scores indicate better functioning.
Qualitative Analysis
In all, 54 participants had the opportunity to comment on what they liked and disliked about the assigned study arm and recommendations for future trials; 2 (3.7%), 5 (9.2%), and 6 (11.1%) participants chose not to comment on these questions, respectively. Participants wrote as many comments as desired for each question; thus, each question may have been coded for multiple categories. Here, we report on the highest occurring categories.
In regard to what they liked about the study arm, the TCC participants commented on the mental (25%) and physical benefits (19%) gained from TCC. Participants reported that TCC helped them feel more relaxed, less stressed, and better emotionally. Physically, they reported that TCC helped with balance, increased energy, and improved sleep. Additionally, TCC participants enjoyed the opportunity to interact and practice TCC with other female survivors (19%) and also the general aspects of TCC (15%; eg, the instructor and having music). In comparison, HEC participants commented on the social support received from fellow participants, particularly being able to share and validate their cancer survivorship experience and learn from one another (33%). They also commented (31%) that the information received from the class topics was beneficial for their health (eg, nutrition) and appreciated learning new relevant information (eg, causes of fatigue). Finally, HEC participants enjoyed the variety of health specialists who led the classes (11%) and general aspects of HEC (11%; eg, handouts).
In regard to what the participants disliked about the assigned study arm, notably, a large proportion of TCC participants stated that there were no dislikes to report (40%). Other TCC comments were that the warm-up period was too long; there was too much repetition of poses (24%); and they disliked having classes in the middle of the day (16%). In comparison, fewer HEC participants indicated that there were no dislikes to report (19%). Additional HEC group comments were that having sessions 3 times a week was too frequent (19%), and they did not like traveling to the sessions (16%). Finally, some comments were made with regard to the class topics (19%), stating that the information would have been more useful closer to treatment or desired topics could be personalized to their informational needs.
Finally, 56% of TCC group recommendations for future trials were to not change anything. The few remaining recommendations (less than 8% of comments) were to have more class time and location options, provide more variety of TCC postures, and provide options for individual attention from the instructor. In contrast, the majority of HEC group recommendations were to have fewer classes per week (21%) and even more group discussions (12%); some recommended not making any changes (12%).
Discussion
This feasibility RCT is the first to demonstrate that a TCC intervention is feasible and acceptable in a sample of senior female cancer survivors. We achieved high retention and attendance rates, which were comparable with those in other TC intervention studies.13,40 Additionally, our participants reported high levels of satisfaction with the assigned study arm and intention to continue TCC or start exercising (ie, HEC arm) after completion of the study. Contrary to predictions, there were no significant differences among the study arms for QOL (SF-36v1 Health Survey). Within-group analyses revealed that the TCC group made significant improvements in MCS at postintervention, indicating overall improvements in mental health, but with no significant improvements in PCS. Whereas we demonstrated the intervention’s feasibility in senior female cancer survivors, future directions should consider protocol modifications (eg, longer duration to allow for progressive intensity) to result in larger QOL outcomes.
One of this study’s strengths was the participants’ qualitative assessment of their experiences with the study, which will be informative for designing future trials. Clearly, the TCC participants felt that they derived mental and physical benefits from practicing TCC, despite null group comparisons on validated quantitative measures of mental and physical health-related QOL, and a majority of their recommendations were to not change anything. On the other hand, a large proportion of the HEC group’s comments were related to the socially supportive aspect of their experience, and they even made recommendations to increase group discussion. However, the TCC group also reported on social supportive aspects, such as enjoying TCC practice with other survivors. We had anticipated that the TCC and HEC groups would be similarly socially supportive because both settings brought senior survivors together for 12 weeks. However, it is possible that the HEC setting was a more socially supportive context because the participants often shared their cancer experiences during classes, whereas in the TCC group, fewer opportunities existed to share their cancer experiences (ie, right before or after each class). We can only speculate that this study did not observe strong QOL effects of the TCC intervention because the HEC group benefited from sharing their cancer experiences and receiving information on healthy aging. A more appropriate control for the TCC intervention could have been a music relaxation group that consisted of participants quietly listening to music, without group discussions of participants’ cancer experiences. However, other TC intervention studies on healthy senior adults have demonstrated significant improvements in SF-36 physical functioning, bodily pain, vitality, and mental health subscales in a TC group, compared with a HEC group, 13 even for the most functionally impaired participants (ie, physical functioning and role-physical improvements). 41 Similarly, a TC intervention in younger breast cancer survivors found improvements in health-related QOL among the TC group compared with psychosocial therapy control. 25 It is important to note that the participants in these studies were either healthy older adults or breast cancer survivors of a younger age range (age = 33-78 years; mean age = 52 years). A strength of our study is that we have applied a TCC intervention to a population of senior female cancer survivors who had some physical functioning limitations on entry into the study (ie, SF-12 <80 for physical functioning and <72 for role-physical), and the baseline SF-36 subscale scores in our participants were lower than those in the general US population within similar age ranges (see supplementary table). Prior TC studies did not include such limitations in their eligibility criteria.
In a low-functioning population such as ours, it may take a longer and more intense TCC intervention to help improve QOL. Likewise, a review of TC interventions 19 noted that the majority of the nonsignficant findings were found in studies with participants with some form of chronic illness or who were recovering from cancer at study entry. Similarly, null effects of TC have been reported in other vulnerable populations, such as sedentary senior adults with type 2 diabetes. 42 Senior cancer survivors, with physical functioning limitations, may require an intervention that is longer than 12 weeks to allow for more TC patterns to be performed while standing and to progressively introduce greater intensity in movements. For instance, movements that promote greater muscle force production in the legs and are eccentrically biased could have enhanced the physical function outcomes. 43 However, we should also note that 55% of the TCC group attended 80% or more of the classes. Although this is a good percentage, perhaps a higher attendance to 80% or more of the classes would have resulted in stronger QOL effects for the TCC group. The challenge in designing interventions for senior survivors is finding the balance between maintaining a safe level for physically vulnerable seniors with an intensity level that will achieve results, and exercising for a sufficient duration of time (ie, >12 weeks) that will be acceptable to seniors. 31
There are a few limitations of this study to take note of. First, the SF-36 was only measured at 2 time points, and research has indicated that the test-retest reliability of the SF-36 in senior, frail populations may not meet standards for clinical application. 44 Considering the extensive day-to-day variability in these measures, future trials with a larger sample and more frequent assessments (eg, biweekly, rather than at 2 time points) may help capture a more stable representation of QOL effects in this population. Another limitation is the reliance on self-report data. Objective physical functioning measures (eg, flexibility, strength, and balance) would have provided additional information on the effectiveness of the TCC in improving physical functioning rather than relying on self-reported QOL. Additionally, although we aimed to extend past TC studies in breast cancer survivors that found QOL benefits,21,25 the effectiveness of a TCC intervention should also be examined in senior male survivors. For instance, TCC may be beneficial for older prostate cancer survivors who are experiencing androgen-deprivation side effects of fatigue, hot flashes, osteoporosis, and muscle wasting. 45 Finally, because our study sample consisted primarily of white, non-Latino senior survivors, additional research is needed to examine the effectiveness of this intervention for senior survivors of ethnic/racial minority backgrounds. According to the double jeopardy hypothesis, being both an older and an ethnic minority cancer survivor may be associated with compounded detrimental effects on health outcomes. 46 This would be another vulnerable senior survivor population in which one can implement TCC interventions for improving QOL.
Despite these limitations, this feasibility RCT is one of the first to demonstrate that a TCC intervention is feasible and acceptable among senior female cancer survivors. Overall, the participants were very satisfied with the trial, commented on the physical and mental benefits gained from practicing TCC, and provided valuable recommendations for designing future trials. Larger, definitive trials are recommended to assess a modified protocol with a longer duration that will allow for a progression of intensity in the TC movements to help increase physical functioning. Additionally, larger trials will allow for more frequent QOL assessments to reduce the day-to-day variability in these measures. Mind-body interventions provide value beyond strictly physical activity interventions because they offer a meditative component in addition to physical activity. The meditative aspects of TCC may be particularly beneficial for older cancer survivors in light of research findings that practice of meditation can reduce loneliness and downregulate gene expression associated with inflammation in older adults 47 and caregivers of individuals with dementia. 48 This points to the importance of continuing to examine the value of mind-body interventions, such as TCC, in senior cancer survivors.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The HEALS Project was funded by the National Cancer Institute (R21 CA135250-02; Kinney, PI) and the Huntsman Cancer Foundation. Additional support was provided by the Shared Resources (P30 CA042014) and the Linda B. and Robert B. Wiggins Wellness-Survivorship Center at Huntsman Cancer Institute. This content is solely the responsibility of the authors and does not necessarily represent the official views of the funding and supporting agencies.
Authors’ Note
This article was prepared using the Health Education & Active Living in Surviving Seniors (HEALS) Project data obtained from the Kinney Research Group.