
Abstract
Objective:
We examined the effects of Mindfulness-based interventions (MBIs) on depressive symptoms in women with breast cancer and examined the moderating effects of participant characteristics, research methodologies, and features of interventions.
Methods:
We systematically searched 12 databases through November 2022 without date restrictions using the following search terms: (mindful* or meditation) AND (cancer OR neoplasm) AND (depress*). Studies included were primary studies evaluating MBIs in women with breast cancer who also had depression. Studies were included if they used a control group and were written in English. We used a random-effects model to compute effect sizes (ESs) using Hedges’ g, forest plot, and Q and I2 statistics as measure of heterogeneity. We also requested moderator analyses.
Results:
We found 19 studies with 2139 participants (49.4 ± 8.3 years old) that met inclusion criteria for this meta-analysis and systematic review. Overall, women in MBI groups demonstrated significantly lower levels of depression (g = 0.48, 95% CI:0.159, 0.792, P < .001) compared to women in control groups. Regarding moderators, providing MBIs with a home assignment component showed a significantly greater effect on decreasing depressive symptoms (g = 1.75) compared to MBIs without a home assignment component (g = 0.20). When researchers used concealed allocation technique, the interventions demonstrated lower effects on depression than when concealed allocation (g = 0.11vs g = 1.33, P ≤ .001) was not reported. Additionally, when researchers reported high rates of sample attrition, they found a lower effect size on depression (β = −.019, Q = 3.97, P = .046) indicating that attrition moderates the effect.
Conclusion:
MBIs are moderately effective interventions to reduce depressive symptoms among women with breast cancer. Clinicians might consider encouraging MBIs as adjunct/alternative treatments for women with breast cancer to manage symptoms of depression. Interventions that incorporat home assignments for practicing mindfulness are likely to have a greater effect on reducing depressive symptoms. Additionally, methods including concealed allocation and attrition rate were moderators of the effects of MBIs on depression in women with breast cancer.
Introduction
In 2020, there were 2.3 million patients diagnosed with breast cancer and 685 000 deaths globally. As of the end of 2020, there were 7.8 million patients alive who were diagnosed with breast cancer in the past 5 years, making it the world’s most prevalent cancer. Globally, there are more disability-adjusted life years (DALYs) lost to breast cancer than any other type of cancer. 1 In 2022, approximately 287 850 new cases of invasive breast cancer and 51 400 cases of ductal carcinoma in situ (DCIS) were diagnosed among US population, and 43 250 patients died from breast cancer. 2
As treatments for breast cancer improve and access to mammography expands worldwide, more breast cancer diagnoses are being made earlier and patients are surviving for longer periods of time.3,4 While this is the goal of early detection and treatment for breast cancer, it has led to a concurrent increase in breast cancer survivors who experience significant sequelae and symptom burdens because of breast cancer treatment. Depression is one of the most common psychiatric symptoms in patients with breast cancer. For instance, a systematic review and meta-analysis reported that the global prevalence of depression among breast cancer patients is 32.3%. 5 Healthcare providers need to take early measures to treat depression in breast cancer patients and anticipate the need for depression management, to improve quality of life for breast cancer patients and survivors.
Mindfulness-based interventions (MBIs) have been growing in popularity as a complementary therapy for symptom management among cancer survivors.6 -9 As such, there have been increasing efforts to study the effects of interventions incorporating mindfulness. Originating in the Buddhist tradition, the practice of mindfulness has been adapted as a complementary therapy in several patient populations. 10 A core construct of mindfulness is the self-regulation of attention and achieving a state of consciousness of moment-to-moment awareness in which one attempts to avoid thoughts of the future or the past, and focus on patience, calmness, openness, trust, and living in the present. 11 MBIs have shown promise as a method to increase health-related-quality-of-life (HRQoL) in breast cancer survivors.12,13 Several meta-analyses and systematic reviews have been conducted to investigate the pooled effects of MBIs among patients with breast cancer.10,14 -16 For instance, a systematic review and meta-analysis by Castanhel and Liberali 14 found that MBIs improved psychological outcomes but the researchers did not specifically examine depression as an outcome. Other researchers have conducted systematic reviews and meta-analyses to explore the effects of MBIs on depression. They report that MBIs have moderate effects on reducing depressive symptoms in patients with breast cancer (Standardized mean difference [SMD] =−0.34, 95% CI: −0.46, −0.21 10 ; SMD = −0.61, 95% CI: −1.11, −0.11, P = .02 15 ; Hedges’ g = 0.43, 95% CI: 0.31, 0.54, P < .01. 16 ; However, the number of primary studies in each of these meta-analyses was small (s = 5-12) limiting their ability to conduct subgroup (moderator) analyses and explore the sources of heterogeneity among the studies.10,14 -16 Given the limitations of these previous meta-analyses, the purpose of this study was to investigate the effects of MBIs on depressive symptoms in patients with breast cancer and explore the moderating effects of participant characteristics, study methodologies, and features of the interventions.
Methods
The present review was preregistered with PROSPERO (registration number: CRD42022373539). The Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA) reporting guidelines were used for reporting study inclusion.17,18
Search Strategy and Selection Criteria
We searched 12 electronic databases for relevant publications up to November 22, 2022. The content of the databases included Academic Search Completed (1887+), CINAHL (1937+), Clinical Trials (2000+), Cochrane (1995+), Mindfulness-Springer link (2010+), Ovid APA (1967+), Ovid Medline (1946+), ProQuest & Theses (1996+), PubMed (1809+), ScienceDirect (1880+), ERIC (1966+) and Scopus (1788+). The final search strategy was based on the PICO approach, 19 combining the following search terms: Population (cancer OR neoplasm) AND Intervention (mindful* OR meditation) AND Outcome (depress* OR major depressive disorder). (See Supplemental Table 1 for full search strategy). No search term for Comparison was included as this proved too restrictive. In addition, we reviewed reference lists of eligible studies (ancestry search).
Inclusion and Exclusion Criteria
We included primary studies that were conducted in adults (18 years and older) with breast cancer to examine the effects of MBIs on depression. MBIs included mindfulness-based stress reduction (MBSR), mindfulness based cognitive therapy (MBCT) or adapted mindfulness interventions which were based on the Buddhist philosophical perspectives and using formal mindfulness meditation as a main intervention component. Included articles were written in English. To determine the effects of MBIs, we retrieved studies in which an MBI intervention group was compared to a control group (e.g., usual care group, waitlist control group, control group without any treatment). To minimize selection bias, we included all MBI formats (e.g., individual, group, and mixed format), and experimental designs (e.g., RCT or quasi). We included articles in which participants had multiple cancer types as long as we were able to extract data pertaining to only the breast cancer patients.
We excluded primary studies if they were qualitative, systematic review and meta-analyses, or secondary data analyses. We also excluded articles in which the intervention group participants engaged in alternative interventions that potentially affected depression (such as yoga, tai chi, qigong, transcendental meditation [TM], acceptance and commitment therapy [ACT] or dialectical behavior therapy [DBT]. Additionally, we excluded active comparison groups in which participants were using antidepressant medication, psychotherapy, cognitive behavioral therapy [CBT], support group or relaxation/exercise as treatments for depression. Two researchers (CR & SP) independently screened the titles and abstracts of each primary study by using EndNote. If further discussion about including a study was required, we consulted the third researcher (KK) to reach a consensus.
Data Extraction and Coding
After removing duplicate publications using EndNote, 3 of the authors (CR, SP, KK) independently assessed the eligibility of all studies, based on the selection criteria. After reviewing the 19 primary studies, we developed a codebook. Two authors (CR & SP) revised the codebook after pilot testing with 5 studies. For each included study, the following data were independently extracted by the researchers: source of the information (i.e., setting of intervention, year of publication, and publication status); methods including quality indicators (e.g., concealed allocation, blinded data collector, intention-to-treat, a priori power analysis, participant characteristics at baseline, equality of baseline characteristics between groups, intervention fidelity); intervention (e.g., type of MBI, number of sessions per week, duration of each session, number of days across the intervention, intervention components, and length of follow up of depression measurements); participants’ characteristics (e.g., age, sample size of each group); and outcome (e.g., depression instrument, reliability of scale, depression score). Any inconsistencies in data extraction were resolved via discussions between the research team (See Supplemental Tables 2 & 3).
Statistical Analysis
We used SPSS (version 28) to describe study characteristics. We then used Comprehensive Meta-Analysis (CMA) version 3.0 to compute primary study effect sizes (ESs). Because depression was measured by various outcomes across the primary studies, we used the standardized mean differences of depression scores between the post-intervention and control groups using Hedge’s g with 95% confidence intervals (CIs). A standardized mean difference allows comparison of ESs across studies with measures of different metrics.20,21 We used Hedges’ g because Cohen’s d has a slight bias, which tends to overestimate the ES with a small number of primary studies. We assumed that the ESs were normally distributed with variability due to differences in participants, methods, interventions, and outcomes. To estimate the mean of the effects, we utilized the random-effects model, in which CMA weights each study by the inverse of the within- and between-studies variance. Studies with higher precision were weighted more heavily than studies with lower precision.20,21
Heterogeneity Assessment
We assessed the heterogeneity across studies by using a visual inspection of the forest plot and the Q and I 2 statistics. 20 The Q statistic reflects total dispersion across ESs (i.e., weighted sum of squares). A significant Q statistic (P < .05) represents considerable heterogeneity. The I 2 statistic quantifies heterogeneity as the ratio of true heterogeneity to total variance across ESs. An I 2 statistic of 25%, 50%, and 75% reflects low, moderate, and high, respectively. A value of 0% indicates that there is no heterogeneity observed, whereas the values of I 2 higher than 50% indicate substantial heterogeneity.20,21 When heterogeneity was present, we used moderator analysis to investigate the source of the heterogeneity. We utilized an ANOVA analog for categorical moderators and meta-regression for continuous moderators. 20
Assessment of Methodological Quality
The quality of included primary studies is an important aspect of meta-analysis. The summary effect estimate can be distorted by poor study quality.20,21 Although there are many quality rating scales for assessing primary studies, they have questionable validity and do not adequately reflect study design quality. 22 Instead, we used quality indicators as moderators and examined the difference in effects for studies with and without the quality indicators. Quality indicators included assignment into groups (random vs. non-random), allocation concealment, masked data collector, a priori power analysis, fidelity of the intervention, comparison of participant characteristics at baseline, and intention-to-treat analysis. For instance, we compared ESs between studies that included a fidelity check and those studies that did not mention checking the fidelity of the intervention. Differences in ESs between the studies with regard to the presence or absence of a quality indicator provide an estimate of the effect of study quality. 20
Estimates of Bias
We used the funnel plot, Begg and Mazumdar rank correlation test, and Egger’s regression test to estimate publication bias. 20 A funnel plot is a basic scatterplot of individual study effect estimates against standard error. A visibly asymmetrical funnel diagram shows publishing bias. A significant (P > .05) result of the Begg and Mazumdar rank correlation test or the Egger regression test also indicates publication bias. 20
Ethical Approval
This meta-analysis does not require ethical approval or patient consent because the data used in the meta-analysis were extracted from primary studies that had declared ethical approval, and no original raw data was utilized.
Results
Demographic Characteristics of Included Studies
An initial pool of 3206 articles (from electronic database search and ancestry search) was identified for initial screening after duplicates were removed using EndNote. Of 1747 articles, 1662 were excluded based on title and abstract review, resulting in 85 articles for full-text review. The full-text evaluation further eliminated 66 primary studies, leading to an analytical sample of 19 primary studies (see Figure 1).

PRISMA flow of included primary studies.
Nineteen primary studies that met our inclusion criteria (s = 19) reported data on 19 between-group comparisons (k = 19) and 14 pre/post-test/control group comparisons. All primary studies were published between 2012 and 2022. A total of 2139 participants were included in this systematic review and meta-analysis; 1072 were exposed to mindfulness-based interventions and 1067 served as controls. Six primary studies were conducted in the U.S.23 -27, four in China28 -31, three in Iran,32 -34 and one in each Korea, 35 Denmark, 36 Sweden, 37 Taiwan, 38 Japan, 39 and England. 40 All trials were conducted in patients with breast cancer.
Mean age of participants’ ages ranged from 24.2 to 57.2 years (Mean 49.4± 8.3, s=15). See Table 1. Primary researchers used 7 different depressive instruments including: (1) Beck Depression Inventory (BDI; s = 2), (2) Psychology Health Questionnaire (PHQ, s=1), (3) Hospital Anxiety and Depression Scale (HADS; s =5) (4) Profile Mood States (POMS; s =1) (5) the Depression Anxiety and Stress Scales (DASS-21, s=3), (6) the Center for Epidemiological Studies Depression (CES-D, s=6), (7) Personality Assessment Inventory (PAI; s =1). Higher scores indicate higher levels of depression. The reliability of these scales ranged from 0.67 to 0.92 (s = 4). Thirteen primary studies were funded (s = 13). Twelve research teams employed MBSR, 4 employed adapted MBI, and 3 employed MBCT (see Supplemental Table 2).
Characteristics of Primary Studies (s = 19).

Abbreviations: s, number of studies providing data; Min, minimum; Q1, first quartile; Mdn, median; Q3, third quartile; Max, maximum; MBI, mindfulness-based intervention.
Effects of MBIs
Meta-analysis revealed that MBIs significantly improved depressive symptoms (g = 0.475, 95% CI:0.159, 0.792, P < .001, I 2 =92%; See Figure 2). Each square reflects the direction and magnitude of the effect; the size of the square reflects the weight assigned to the primary study (based on precision) and its influence on the summary ES. The width of the line shows the CIs of the ES of each primary study. The diamond below the studies shows the mean ES and the width of the diamond indicates its CIs. 20
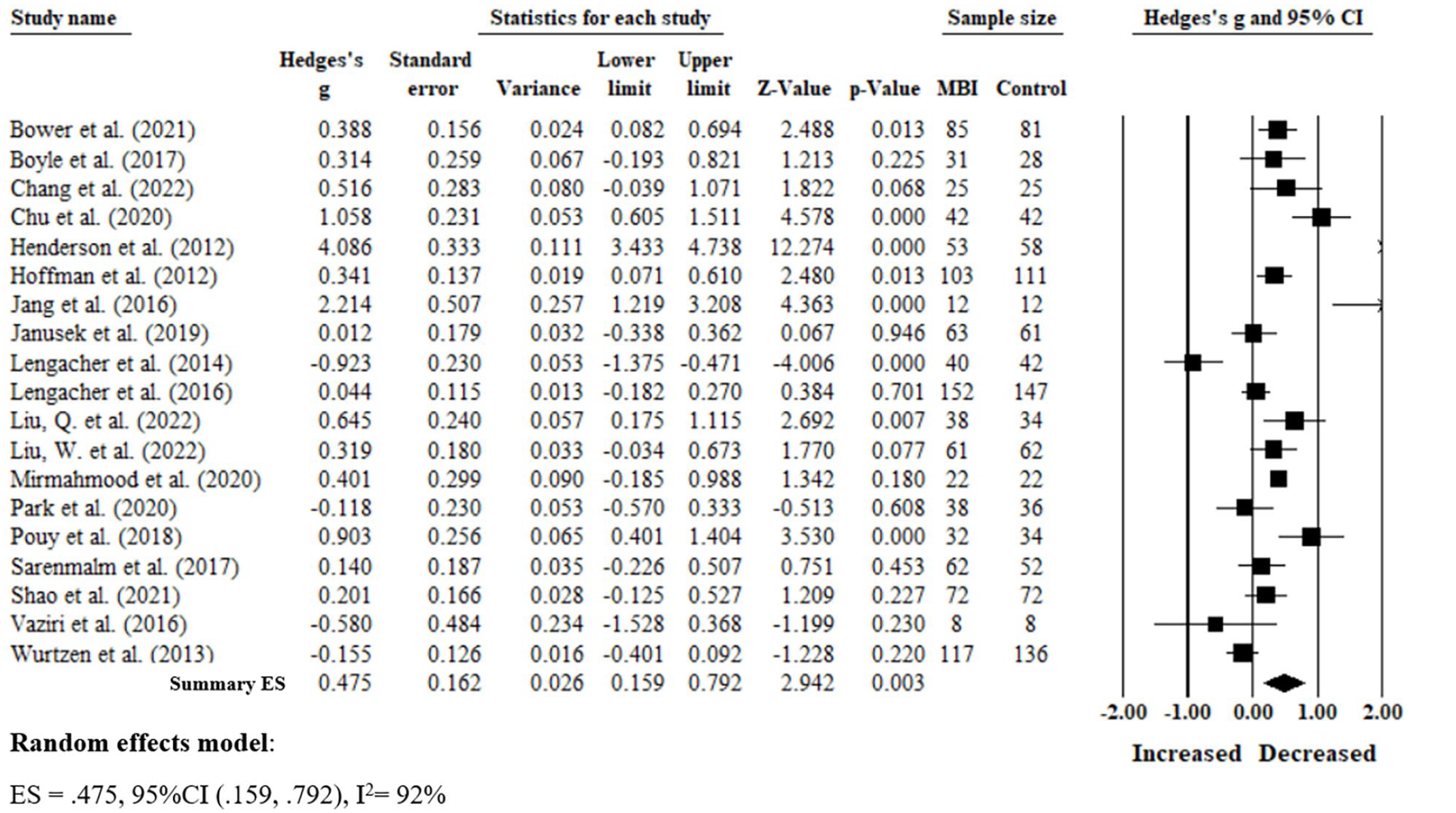
Forest’s plot of the effect of MBIs versus control group on depression in women with breast cancer.
Next, we found a significant one-group pre-posttest effect of MBIs when samples were both correlated 0.8 (g = 0.443, 95% CI: 0.289, 0.596, P < .001) and not correlated 0.0 (g = 0.418, 95% CI: 0.240, 0.595, P < .001). The one-group pre-posttest comparison of control groups showed no significance when samples were correlated 0.8 (g = −0.034, 95% CI: −0.216, 0.148, P = .713) and not correlated 0.0 (g = 0.011, 95% CI: −0.211, 0.233, P = .921) suggesting no evidence of spontaneous recovery (See Table 2).
Effect Size of MBI Versus Control Groups.

Subgroup Analyses
We explored the sources of the heterogeneity between participant characteristics, methodological quality indicators, and features of the interventions to understand our findings as well as generate hypotheses for future research. Three moderators influenced effect size. Providing MBIs with a home assignment component had a greater effect on depressive symptoms (g = 1.75) compared to providing MBIs without home assignments (g = 0.20, P < .001). Regarding research methodologies, when the researchers reported using concealed allocation to assign participants into groups, the interventions demonstrated lower effects on depression than when concealed allocation was not used (g = 0.11vs g = 1.33, P =< .001). Additionally, increasing rates of attrition decreased the effect size of MBIs on depression in patients with breast cancer (β = −.019, Q = 3.97, P = .046). Please see Tables 3 and 4.
Categorical Moderator Results for Depression Comparing MBI Versus Control Groups.
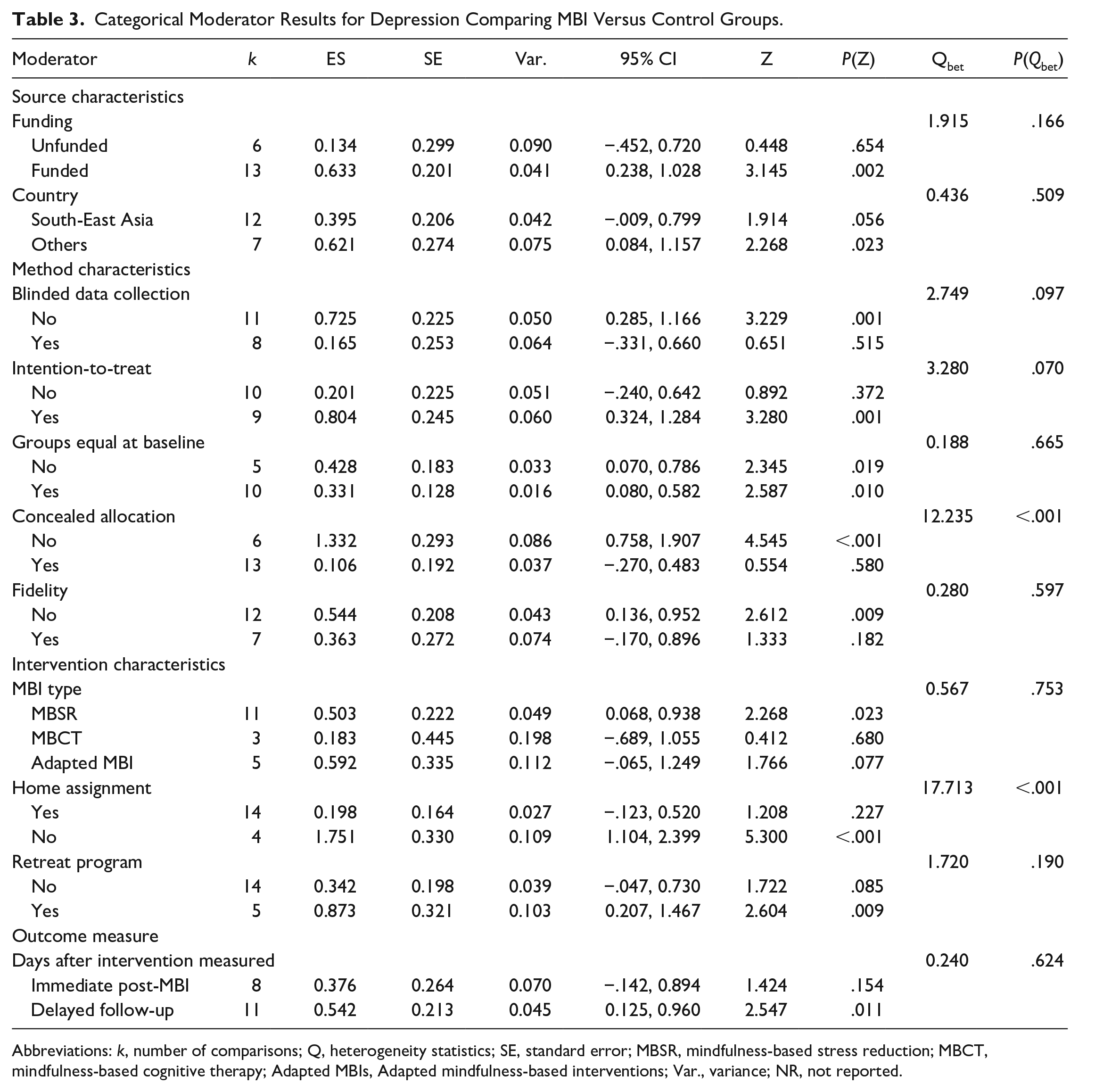
Abbreviations: k, number of comparisons; Q, heterogeneity statistics; SE, standard error; MBSR, mindfulness-based stress reduction; MBCT, mindfulness-based cognitive therapy; Adapted MBIs, Adapted mindfulness-based interventions; Var., variance; NR, not reported.
Continuous Moderators of the Effects of Mindfulness Based Intervention on Depression.
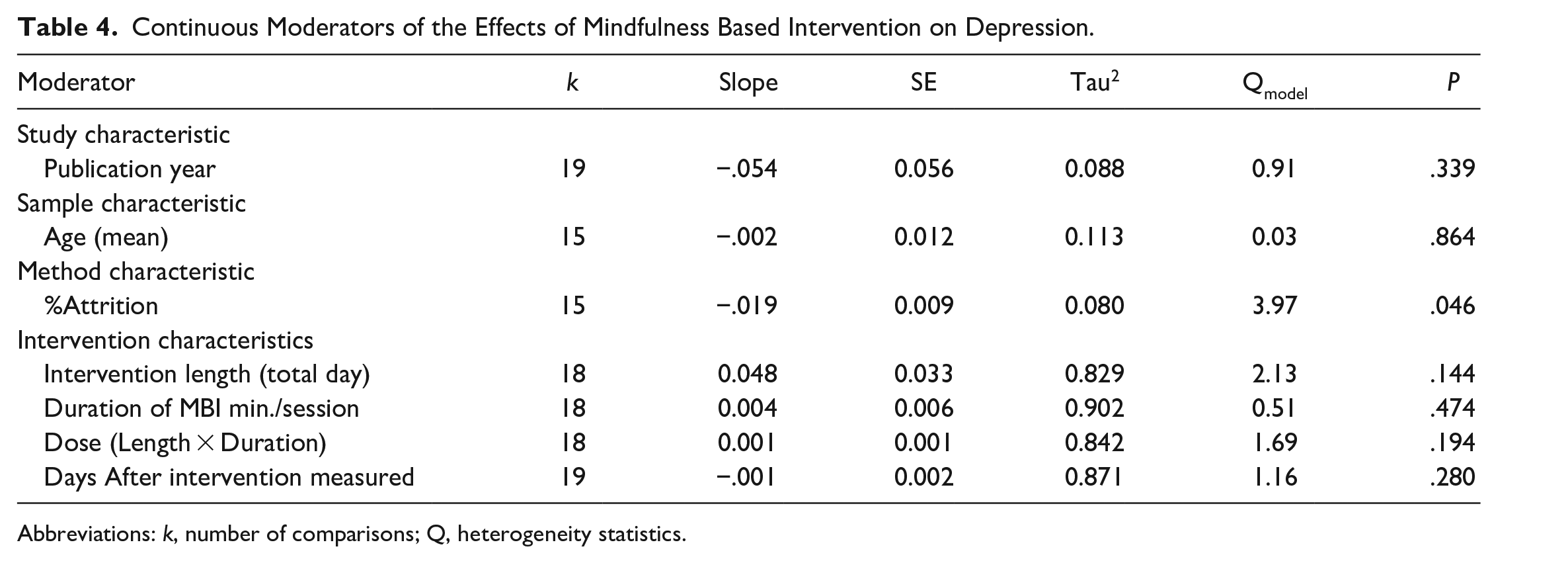
Abbreviations: k, number of comparisons; Q, heterogeneity statistics.
Publication Bias
The funnel plot was visually asymmetrical suggesting that publication bias was likely; primary studies with large sample sizes with negative effects were missing. See Figure 3. The Egger’s test was significant with an intercept of 4.23 (95% CI: −0.230, 8.701, P = .030). Begg and Mazumdar’s test was also significant (P = .031). These results indicate the potential presence of publication bias.

Funnel plot.
Discussion
We found that MBIs significantly decrease depressive symptoms in patients with breast cancer. Additionally, we found that providing MBIs with a home assignment component increased the effect of the interventions. One explanation might be that home assignment aims to help participants engage in regular mindfulness practices so that they become integrated into their daily schedules. 41 Home assignments provide more opportunities to strengthen the mind and decrease the ruminative/repetitive thoughts and stress levels that often accompany depression. Like us, Lloyd et al 42 found that home practice predicted improvements in clinical outcomes such as depression and anxiety. Similarly, in their meta-analysis, Parsons et al 43 found that self-reported home practice was significantly associated with psychological outcomes. Thus, evidence supports the use of MBIs with a home assignment component to help patients with breast cancer develop the habitual practice of mindfulness.
We included quality indicators in our moderator analysis to determine if study quality moderated the effects of the interventions. We found that when researchers reported using concealed allocation, the MBIs demonstrated lower effects on depression than when concealed allocation was not used. Similarly, a meta-analysis by Armijo-Olivo et al 44 found that studies demonstrating inappropriate allocation concealment tended to overestimate treatment effects when compared with trials in which adequate concealment of allocation was used (ES = 0.12, 95% CI:−0.06, 0.30). Thus, allocation concealment is a technique used to prevent selection bias in randomized controlled trials by concealing the allocation sequence from those assigning participants to the intervention or control groups.45 -47
Moreover, we found that attrition rates moderated the effect of the intervention on depressive symptoms. Studies in which researchers reported higher rates of attrition demonstrated a lower reduction in depressive symptoms among patients with breast cancer. We found that a 1% increase in attrition rate, resulted in a 0.2 unit increase in depressive symptom scores. Patients who drop out of studies are likely to be nonadherent to practicing mindfulness or do not perceive a derived benefit from the practice. This indicates that methods to promote adherence to mindfulness practices in patients who elect to try them are likely to contribute to observed improvements in depressive symptoms.
Based on our findings, we can recommend that future researchers consider incorporating home assignments into their MBI curricula to promote adherence to the practice of mindfulness in daily life. This is likely to lead to more long-term, habitual practice of mindfulness which is highly anticipated to have greater effects on reducing depressive symptoms in patients with breast cancer.
Moreover, MBIs represent a cost effective, minimally invasive, non-pharmacologic method to manage depressive symptoms in a patient population that has many risk factors for developing depression during their treatment. Healthcare providers might consider that the benefits of practicing mindfulness likely outweigh any risks making it a valuable adjunct treatment for depression in patients with breast cancer. MBIs should certainly be offered to patients with breast cancer to provide some resilience against depression and potentially improve their quality of life while on treatment and throughout survivorship.
Strengths and Limitations
This systematic review and meta-analysis provided a comprehensive summary of the currently available trials that have explored the effects when MBIs are used to reduce depressive symptoms in patients with breast cancer. We included 19 trials conducted up to 2022 that specifically examined the effects of MBIs on depression in patients with breast cancer. Our systematic review and meta-analysis is novel in that it provides a comprehensive examination of the effect of MBIs on depressive symptoms in patients with breast cancer with a greater number of primary studies (s = 19) than prior meta-analyses (s = 4-9), thus, allowing us to conduct moderator analyses to explore the sources of heterogeneity among the studies. To our knowledge, ours is the first meta-analysis and systematic review that includes subgroup analyses.
However, there were limitations in our study. First, this meta-analysis was limited to reports written in English, excluding several potentially pertinent studies. Excluding non-English reports may induce language bias and reduce the precision of summary treatment effect estimates. 48 Second, there were small numbers of primary studies in some subgroup analyses to explore moderators (s = 3-4). Thus, parameter estimation is likely poor, rendering conclusions that are uncertain. Additionally, our analysis indicates that publication bias is likely. Our findings must be considered considering these relevant limitations. Yet, assessing these limitations allows us to make recommendations for future research.
Research Implications
In recent years, there has been a noticeable increase in the amount of research pertaining to MBIs and the health benefits that they confer. The evidence is strong that MBIs have many advantages including reducing depressive symptoms among patients with breast cancer. However, we found that depression was often measured as an outcome among patients with Stage 0-III breast cancer. Only 3 researchers included patients with Stage IV breast cancer in their study samples29,31,38 and most noted metastatic disease among their exclusion criteria. We view this as a problem as it is producing a gap in the knowledge base regarding the effectiveness of MBIs. Patients with metastatic breast cancer are more vulnerable to depressive symptoms. 49 Thus, future studies of MBIs in patients with breast cancer should be conducted among or at least include patients with Stage IV breast cancer. As patients with Stage IV breast cancer have higher symptom burdens and limited life expectancy, they stand the greatest chance to benefit from the anti-depressive effects of MBIs. Future researchers might consider investigating MBIs among samples of patients with more advanced breast cancer so that the effects are more well-understood among patients with significant burdens of disease.
Another limitation of our research is that patients reported mild depressive symptoms, but did not meet the criteria for a diagnosis of clinical depression. Future researchers might consider starting with a sample of people who are clinically depressed to provide more clinically useful data regarding the effectiveness of MBIs as an adjunct treatment for clinical depression among patients with breast cancer.
Lastly, we recommend that future researchers consider the implications of methodologic choices in their research designs. Based on our findings we can recommend using allocation concealment to reduce bias among the participants. We can also recommend that researchers note the effect that attrition may have on the effects of their interventions.
Clinical Implications
Participants across primary studies were patients with breast cancer who self-reported depressive symptoms, but did not meet the criteria for a diagnosis of clinical depression. We recommend promoting the use of MBIs with home assignment for patients with breast cancer who also display mild-to-moderate depression. to provide an alternative to traditional psychosocial treatment. There is evidence that MBIs reduce depressive symptoms among patients with breast cancer and they provide an alternative to traditional psychosocial treatment and its related cost, lack of availability of mental health professionals, and stigma. Moreover, MBIs might help prevent major depressive disorders in patients with breast cancer as they undergo treatment and management of their illness.
Conclusion
Overall, MBIs are effective interventions to reduce depressive symptoms in patients with breast cancer. Providing MBIs with a home assignment component, using allocation concealment, and high rates of attrition moderated the effects of interventions. Healthcare providers might consider using MBIs as alternative treatment to decrease depressive symptoms in patients with breast cancer.
Supplemental Material
sj-docx-1-ict-10.1177_15347354231220617 – Supplemental material for Effects of Mindfulness-Based Interventions on Depression in Patients With Breast Cancer: A Systematic Review and Meta-Analysis
Supplemental material, sj-docx-1-ict-10.1177_15347354231220617 for Effects of Mindfulness-Based Interventions on Depression in Patients With Breast Cancer: A Systematic Review and Meta-Analysis by Chuntana Reangsing, Sasinun Punsuwun and Kristine Keller in Integrative Cancer Therapies
Supplemental Material
sj-docx-2-ict-10.1177_15347354231220617 – Supplemental material for Effects of Mindfulness-Based Interventions on Depression in Patients With Breast Cancer: A Systematic Review and Meta-Analysis
Supplemental material, sj-docx-2-ict-10.1177_15347354231220617 for Effects of Mindfulness-Based Interventions on Depression in Patients With Breast Cancer: A Systematic Review and Meta-Analysis by Chuntana Reangsing, Sasinun Punsuwun and Kristine Keller in Integrative Cancer Therapies
Supplemental Material
sj-docx-3-ict-10.1177_15347354231220617 – Supplemental material for Effects of Mindfulness-Based Interventions on Depression in Patients With Breast Cancer: A Systematic Review and Meta-Analysis
Supplemental material, sj-docx-3-ict-10.1177_15347354231220617 for Effects of Mindfulness-Based Interventions on Depression in Patients With Breast Cancer: A Systematic Review and Meta-Analysis by Chuntana Reangsing, Sasinun Punsuwun and Kristine Keller in Integrative Cancer Therapies
Footnotes
Author Contributions
All three authors (CR, SP & KK) were responsible for acquisition, interpretation, and drafting the article. Two authors (CR & SP) substantially contributed to the data extraction, and critically revised the work for important intellectual content. The first (CR) and last authors (KK) were included in the identification, selection, article drafting, and critically revised the work. All authors (CR, SP & KK) provided final approval of the version to be published and agree to be accountable for all aspect of the work.
Data Available Statement
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This article processing charges of this work was financially supported by Mae Fah Luang University, Thailand.
Ethical Approval
A systematic review and meta-analysis was not subject to ethical review.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.