
Abstract
Objectives:
Chinese herbal medicine (CHM) is widely used in breast cancer, but there is no consensus on the Chinese medicine (CM) syndromes in the different conventional treatment stages (preoperative, postoperative, chemotherapy, radiation therapy and endocrine therapy) of early breast cancer. This Delphi study aimed to achieve expert consensus on the CM syndromes, signs and symptoms, and the Chinese herbal formulae for early breast cancer.
Methods:
Thirty senior CM clinicians with expertise in managing breast cancer were enrolled. The syndromes selected by ≥50% of experts and the corresponding most common Chinese herbal formulae were considered a consensus. Consensus on signs and symptoms was defined as a median score ≥4 (the item was important or very important) and ≥70% of experts rating the sign or symptom as 4 (important) or 5 (very important) on a 5-point Likert scale.
Results:
Three survey rounds were conducted from 15 October 2021 to 10 March 2022. Consensus was reached with 3 syndromes confirmed for each treatment stage. Several syndromes, such as dual deficiency of qi and Blood, were considered common to multiple treatment stages. Some important signs and symptoms were presented in multiple treatment stages (eg, shortage of qi in the radiation therapy and endocrine therapy stages).
Conclusions:
This Delphi study achieved consensus on the most common CM syndromes, corresponding signs and symptoms, and the most common formulae in each treatment stage of early breast cancer, providing an evidence-based approach for future clinical practice.
Background
Breast cancer is common and is the leading cause of cancer-related death among females. 1 Conventional treatments include surgery and adjuvant treatments (eg, chemotherapy) based on the pathological results. 2 Such treatments have unavoidable side effects, and many patients seek adjunctive treatment, such as Chinese medicine (CM), to relieve adverse symptoms and improve their quality of life. 3
Chinese herbal medicine (CHM) is prescribed according to CM syndrome differentiation. 4 Syndrome differentiation is the cornerstone of disease recognition and treatment in CM and describes the dysfunction of the interrelationship between the body and the surrounding environment under the action of pathogenic factors. 5 Guo et al conducted a systematic review identifying diversity in the CM syndromes for early breast cancer described in contemporary literature. 6 In the case of early breast cancer (without metastases), syndrome differentiation may vary due to a range of factors, such as signs and symptoms associated with various conventional interventions (eg, chemotherapy and radiotherapy) during the long period of cancer treatment. Further, CM practitioners exercise their clinical judgement in syndrome differentiation based on personal clinical experience; hence, they may select different Chinese herbal formulae for different patients.
To date, only one guideline, published in 2008, the Guideline for Diagnosis and Treatment of Tumour in Traditional Chinese Medicine, included guidance on syndrome distribution for breast cancer. 7 However, the syndromes in this guideline were not presented according to the different treatment stages and were not aligned with current clinical practice. Therefore, anecdotally, few experts have incorporated this guideline into clinical practice. The guideline should be updated accordingly. In the context of evidence-based medicine development and health care, the lack of consensus on CM clinical decision-making for breast cancer challenges clinical research, translation and evidence-based practice. Therefore, this study sought to standardise the CM syndromes observed during the different cancer treatment stages to provide precise and better treatment in clinical practice, further informing clinicians’ use of Chinese herbal formulae for early breast cancer.
As proposed by Zhu, 8 the 3 essential studies to inform CM syndrome differentiation are the literature review, clinical study and expert survey. The former 2 study types have been conducted for early breast cancer.6,9 This study reports the conduct and findings of the expert survey. The Delphi method has been widely used to gain consensus in health research,10 -13 including for CM syndromes in breast cancer. Delphi studies by Guan 14 and Guo 15 focussed on the different treatment stages in early breast cancer, and the latter involved the same experts in each of the different rounds. However, neither study systematically reviewed the literature before developing the surveys, which may bias the survey results. Further, the lack of clinical data to inform the survey limits the study’s conclusions.
Methods
To address the gaps in previous research, this study sought experts’ opinions on the CM syndromes for each conventional treatment stage of early breast cancer. The Delphi study was informed by previous systematic review 6 and clinical study. 9 This Delphi study was designed with 3 survey rounds to gain experts’ opinions on CM syndromes, Chinese herbal formulae and the corresponding signs and symptoms in each of the 5 breast cancer treatment stages (adapted from Guo and Chen) 16 : preoperative, postoperative, chemotherapy, radiation therapy and endocrine therapy.
Inclusion Criteria of Experts
Eligible experts were qualified as an associate chief physician or chief physician, had ≥10 years of clinical experience of Chinese herbal formula use for breast cancer and were currently employed in clinical practice. Thirty CM experts were selected to participate in each of the 3 survey rounds.
Survey Design
The online survey was hosted on the Wenjuanxing platform and took approximately 20 to 30 minutes to complete. The first-round survey collected demographic information and experts’ opinions on the most common CM syndromes and corresponding Chinese herbal formulae used among the different breast cancer treatment stages. The syndrome and Chinese herbal formula results from a previously published systematic review 6 and a clinical study on CM syndrome differentiation in 620 people with breast cancer 9 were summarised in the survey. The research team thoroughly reviewed and checked the survey before sending it to the experts.
The second-round survey determined experts’ opinions about the signs and symptoms for the most common syndromes (ie, those rated as important or very important by ≥50% of experts) from the first-round survey. The signs and symptoms for each syndrome from the published systematic review 6 were listed. As mentioned, the research team carefully reviewed the signs and symptoms results extracted from the systematic review to ensure they were accurately incorporated into the survey design. The systematic review found that the signs and symptoms for a given syndrome differed according to the treatment stage. Therefore, 2 versions of the surveys were designed to allow experts to complete the survey according to whether they considered the signs and symptoms of a given syndrome would be the same for all treatment stages (survey A) or different among the different treatment stages (survey B). The results from both surveys were merged for analysis. The signs and symptoms were ranked on a 5-point Likert scale from 1 point (very unimportant) to 5 points (very important). Experts could nominate additional signs and symptoms for each syndrome.
The third-round survey clarified the results from the second round and gained further opinions. In the third round, the descriptive statistics (mean, median and number of Likert scale responses) from the second-round survey were presented for each sign and symptom. The third-round survey was customised for each participant to include their rating of each item from the second-round survey; participants could choose to retain their original rating or, if they had changed their opinion, revise their rating. Participants who revised their ratings for each sign and symptom did so on the same 5-point Likert scale.
Study Procedure
Experts were recruited from the Breast Disease Branch of the China Association of Chinese Medicine. Members received an invitation letter that explained the project and asked about the number of years of experience and the number of patients the expert had admitted to the outpatient department in the previous week. These 2 questions were considered, to a certain extent, to reflect the clinical skills of the experts. Once the interested experts with the most experience had been identified, a link to the online first-round survey was sent.
Experts were given a 2-week deadline to complete each of the 3 online surveys and were sent a reminder 1 week before the deadline. After receiving responses, the researchers analysed opinions from the first-round survey and designed the second-round survey, which determined the corresponding signs and symptoms for the most common syndromes. Some experts nominated some new signs and symptoms items, and some items were not assessed by all experts because of the 2 survey designs in the second round. Therefore, a third-round survey was needed.
Data Analysis
Data were analysed using SPSS software (version 26.0). Descriptive statistics were applied to analyse the expert demographic information, CM syndrome frequency and Chinese herbal formula frequency. The response rate was calculated based on the number of responses in each round.
The mean and median of each sign and symptom were calculated.17 -19 Higher values indicated greater importance of the item in diagnosing CM syndromes. Currently, there is no agreement on how to define important items and the threshold for consensus, and the various definitions provided in the literature have been contentious. 20 Loughlin and Moore suggested 51% as an acceptable level. 21 Vogel considered that items with a median score ≥6.0 (on a 7-point Likert scale) were relevant or feasible. 22 Rayens indicated that if a factor has an interquartile range ≤1.00 and ≥70% of the respondents provided a positive response (scores of 4 and 5 on a 5-point Likert scale) for this factor, then consensus has been achieved. 23 Based on the previous literature, the syndromes selected by ≥50% of experts and the corresponding most common formulae were considered to have reached a consensus in this study. Two criteria were used for selecting the important signs and symptoms that achieved consensus: (a) the items had a median score of 4 or higher, and (b) ≥ 70% of experts rated the importance as 4 (important) or 5 (very important).
Results
The Delphi study was conducted from 15 October 2021 to 10 March 2022. Forty-five experts received the invitation letter and 43 experts responded (see Figure 1). Three experts did not meet the inclusion criteria. Thirty-eight eligible experts agreed to participate in this study. Experts were selected according to (in order) (a) the average number of patients admitted per week (ie, those who admitted more patients were prioritised), (b) the length of clinical experience and (c) their geographical location (to ensure representativeness). Thirty experts were enrolled in the Delphi study after the selection process.

Flow chart of eligibility assessment.
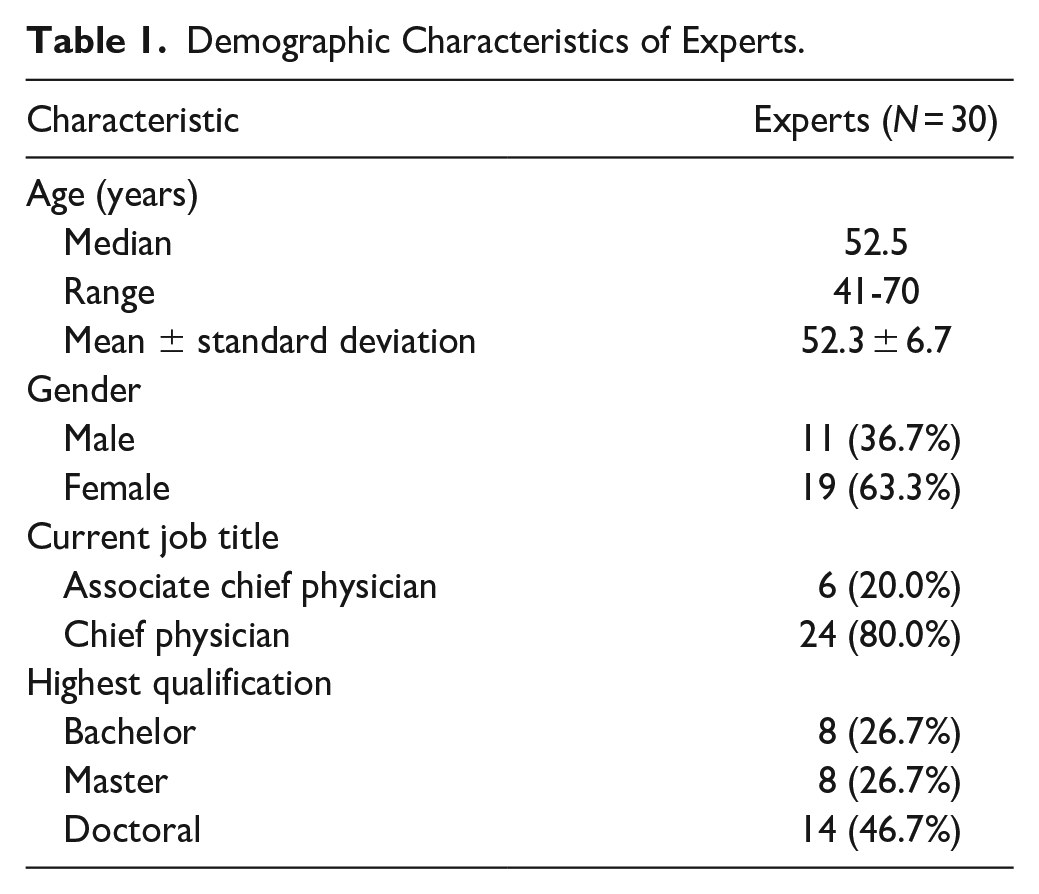
The enrolled experts were located in eastern China (Shandong, Jiangsu, Zhejiang, Fujian and Shanghai provinces), southern China (Guangdong, Guangxi and Hainan provinces), central China (Hunan, Jiangxi and Henan provinces) and northern China (Beijing city). The experts included in this Delphi study were mainly female, held the job title of chief physician and had a postgraduate qualification. The years of clinical experience of using Chinese herbal formula for patients with breast cancer ranged from 15 to 40 years, with an average of 23.5 years. The average number of patients with breast cancer admitted for a half-day outpatient visit in the previous week was 31. The demographic characteristics of the experts are shown in Table 1.
Demographic Characteristics of Experts.
First-Round Survey Results
Thirty experts completed the first-round survey (response rate of 100%) and nominated the most common syndromes in all 5 stages. For each treatment stage, 3 syndromes were rated as common by ≥50% of experts (see Table 2; Supplemental File 1). Several syndromes were considered most common for multiple treatment stages (eg, dual deficiency of qi and Blood and Spleen and Stomach disharmony were the most common syndromes in the postoperative and chemotherapy stages).
Syndromes and Chinese Herbal formulae for Each Treatment Stage.

n = 29.
n = 28.
Twenty-nine experts provided opinions about the Chinese herbal formulae in the preoperative and endocrine therapy stages, while 28 experts commented on the postoperative, chemotherapy and radiation therapy stages (see Table 2, Supplemental File 2). Some formulae were selected for the same syndrome in different treatment stages. For example, the formula Gui pi tang was the most common formula for dual deficiency of qi and Blood in both the postoperative and chemotherapy stages.
Second-Round Survey Results
In the second-round survey, 11 experts completed survey A and 19 experts completed survey B (100% response rate). The median rankings of the signs and symptoms were mainly above 3 (see Supplemental File 3), except for moistened tongue, which ranked 2 for dual deficiency of qi and yin in the postoperative stage. Some experts nominated additional signs and symptoms they considered common for the syndrome, such as a white and greasy tongue coat, dark tongue, distending breast pain, excess sputum, and slippery pulse for the syndrome Blood stasis with phlegm in the preoperative stage. Similarities and differences were identified in the common signs and syndromes for the same syndrome that were important in different treatment stages. Specifically, lassitude, lack of strength and speechlessness were ranked with the highest median (median 5) for dual deficiency of qi and Blood in the postoperative and chemotherapy stages. For the syndrome dual deficiency of qi and yin, the symptom tidal fever was ranked most important in the postoperative and endocrine stages and among the 3 most important symptoms in the radiation therapy stage.
Third-Round Survey Results
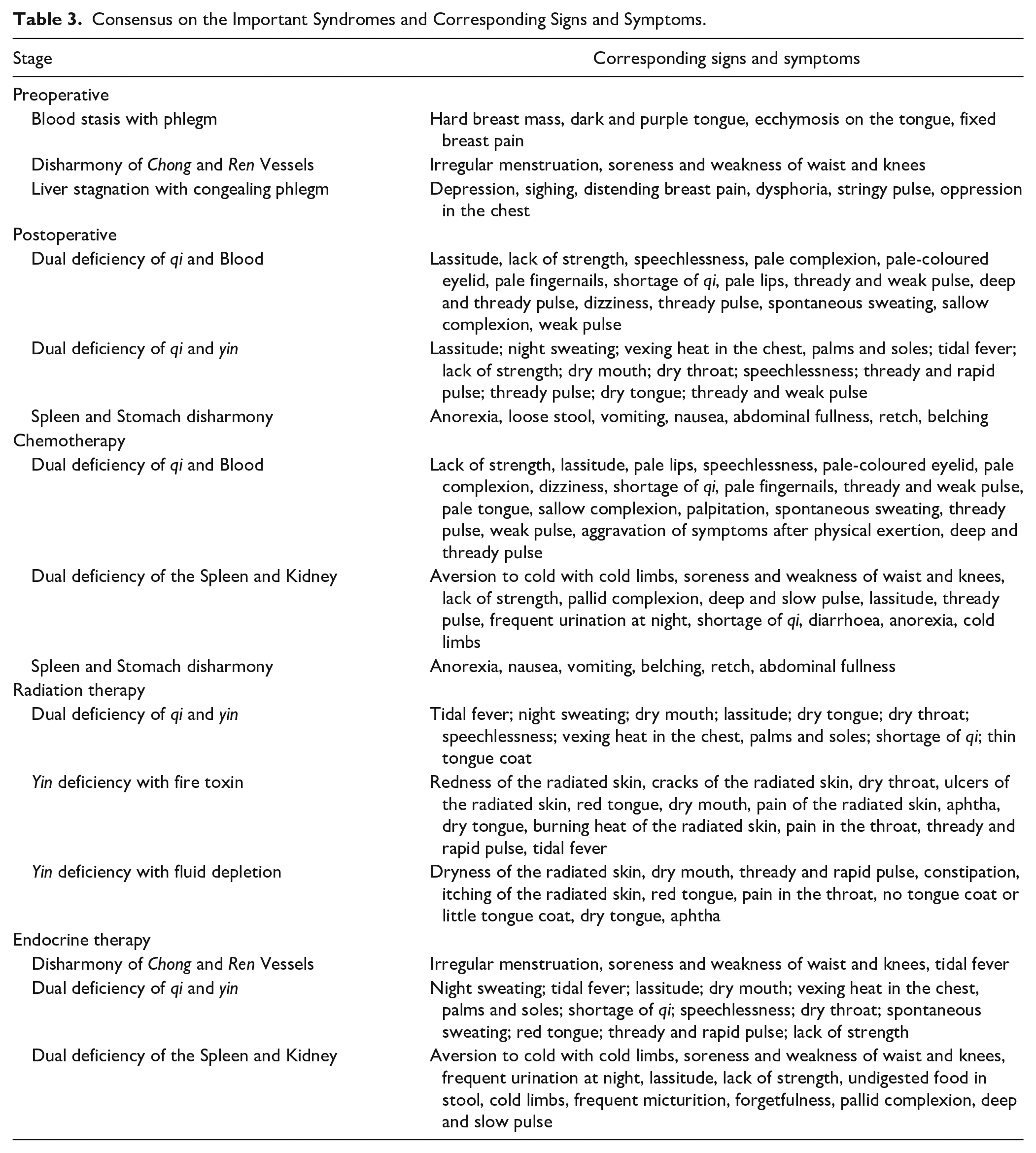
Twenty-nine experts completed the third-round survey (96.7% response rate). Consensus was reached for the signs and symptoms of each syndrome (see Table 3, Supplemental File 4) and varied from 2 to 18 symptoms. For example, only 2 symptoms reached consensus for the disharmony of Chong and Ren Vessels in the preoperative stage: irregular menstruation, and soreness and weakness of the waist and knees. However, 18 symptoms reached consensus for the syndrome dual deficiency of qi and Blood in the chemotherapy stage. As was found in the systematic review, the signs and symptoms for a given syndrome varied depending on the treatment stage. For example, the signs and symptoms that reached consensus for the syndrome dual deficiency of qi and Blood in the chemotherapy stage are the same as for this syndrome in the postoperative stage, except for 3 additional symptoms (pale tongue, palpitation and aggravation of symptoms after physical exertion) that were selected in the chemotherapy stage. For the dual deficiency of qi and yin, the symptom shortage of qi reached consensus in the radiation therapy and endocrine therapy stage but did not reach consensus for the same syndrome in the postoperative stage.
Consensus on the Important Syndromes and Corresponding Signs and Symptoms.
Discussion
The Delphi study involved a group of geographically representative experts to reach a consensus. The 3 survey rounds achieved a high response rate (96.7%–100%). Several researchers recommend a response rate of 70% per round to maintain study rigour,24,25 which was achieved in this study. The approach of diagnosing syndromes according to different treatment stages is based on the clinical findings that patients have different CM aetiology and pathogenesis when receiving different conventional treatments. As such, syndrome differentiation according to different treatments is more aligned with clinical practice, providing clinicians with more accurate syndrome diagnosis and Chinese herbal formula use. Prescribing according to different treatment stages can better integrate CM with standard conventional treatment.
This study was conducted with an evidence-based approach to inform CM syndrome diagnosis and associated signs and symptoms during the different treatment stages of early breast cancer, which is a novel aspect in integrating conventional medical treatment into the analysis of syndrome differentiation. As mentioned, the guideline released in 2008 did not present the CM syndrome according to different treatment stages; therefore, comparison to our consensus is not possible. In the future, this consensus could be developed into a national standard according to the Regulations on the Procedure for Formulating Traditional Chinese Medicine Standards, 26 to facilitate the promotion and standardisation of CM and improve the popularity of Chinese herbal formula application in existing healthcare systems.
Several syndromes were considered common in multiple treatment stages. Dual deficiency of qi and Blood and Spleen and Stomach disharmony were common in the postoperative and chemotherapy stages. Surgery and chemotherapy are considered to consume qi and Blood in CM theory. The effects of surgical anaesthesia and the gastrointestinal side effects during chemotherapy are considered related to Spleen and Stomach disharmony. The important syndromes in the radiation therapy stage were not surprising since radiation therapy is considered to consume yin; the 3 most common syndromes were all related to yin deficiency. The common side effects of endocrine therapy, such as hot flushes caused by tamoxifen 27 or arthralgia caused by aromatase inhibitors, 28 are considered related to dual deficiency of qi and yin or dual deficiency of the Spleen and Kidney, 29 respectively. Some Chinese herbal formulae listed in the first-round Delphi survey were not selected by experts (see Supplemental File 2), which was not surprising since clinicians prescribed those formulae (extracted from patient records in the clinical study) according to the patient’s presentation. The formulae extracted from the systematic review were inconsistent with what experts consider common formulae in clinical practice.
Some researchers advocate including all items in the third-round survey, even those that reached consensus in the previous round. 20 The advantage of this approach is that all items have an equal chance of being assessed; however, this approach lengthens the survey, which may reduce the response rate in the third round. 20 Thus, the researcher must balance retaining a high response rate with gaining the highest level of consensus. 20 This study listed all items in the third-round survey. Each expert’s responses from the second-round survey were included to provide the chance to reconsider their own answers or indicate that their response had not changed. This approach reduced the completion time and maximised survey completion.
The other challenge for the Delphi study is the drop-out rate of the expert panel. Buck et al highlighted the importance of the panel staying involved in the Delphi process to achieve consensus. 30 A poorer response rate often happens in the final round of the Delphi process, which explains why some studies stop after 2 or 3 rounds rather than the initially planned 4 rounds. 20 This study’s response rate was relatively high (greater than 96%), indicating that experts were actively involved. Achieving consensus for all items in the second round is rare. More commonly, some items may not reach consensus after the third round. In most cases, and in this study, researchers stop the study after the third round. 20
While this study used the Delphi method, other research approaches can also achieve consensuses, such as the nominal group technique 31 or consensus conference. 20 The nominal group technique is a method that usually involves face-to-face interaction of 5 to 12 participants. 31 Participants can debate the topics and generate more robust ideas, but the results may be influenced by the dominant team member.31,32 A consensus conference of individuals or groups is used when an important agreement must be reached. 20 However, the conference can be expensive to organise, and the discussion will be directed by strong-willed individuals or groups. 20 This study used the Delphi method because of its advantages over other methods, such as the anonymous participant responses to avoid group dominance and avoiding geographic restrictions, 20 particularly since this study was conducted online during the COVID-19 pandemic.
Strengths and Limitations
This Delphi study used an online survey instead of the traditional paper-based survey to reduce the postage time and curtail survey completion and data entry errors. Compared with the previous Delphi study that did not clarify the inclusion criteria of the enrolled experts, 16 this study selected the experts according to the inclusion criteria and clinician’s experience, which minimised expert selection bias.22,23 The inclusion criteria were developed to ensure experienced experts were included, reducing the diversity in responses that might result from inexperience.
The survey was designed by incorporating key findings from a previously published systematic review 6 and a clinical study, 9 as recommended to increase Delphi study rigour and ensure efficient responses. 33 However, this approach may bias experts’ opinions if they are more inclined to select the syndromes and Chinese herbal formulae provided as a reference for the survey. Therefore, the most common syndromes and the Chinese herbal formulae were presented, but the frequency of the syndromes and formulae in each source was not listed, which reduces the likelihood of experts’ opinions being swayed by the frequencies when considering their choices. Further, the reliability of the secondary data included in the systematic review could not be verified, a problem encountered by all systematic reviews. It is possible that reporting inaccuracies in studies included in the systematic review may have influenced this study’s results. Therefore, the research team considered it vital to triangulate data from different sources (ie, using primary data from people with breast cancer through clinical study 9 and from clinicians involved in their care by this Delphi study).
This study did not seek to collect data on the specific herbal ingredients used according to the syndrome differentiation. In clinical practice, the clinician would be guided by the standard and prescribe the Chinese herbal formulae according to the patient’s situation, so herbal ingredient differences are likely to exist. However, this also reflects the combination of standardisation and personalisation of CM, which plays a mutually reinforcing relationship in clinical application.
Conclusion
This Delphi study reached a consensus about the most common CM syndromes, corresponding Chinese herbal formulae, and signs and symptoms for each specific syndrome among the different treatment stages of early breast cancer. Three syndromes were identified in each treatment stage, and the formulae prescribed for each syndrome and the related diagnostic signs and symptoms were summarised. This Delphi study results provided a reference for CM clinical practice that may lead to improved CM care for early breast cancer patients.
Supplemental Material
sj-docx-1-ict-10.1177_15347354231204008 – Supplemental material for A Delphi Study of Expert Consensus on Chinese Medicine Syndrome Differentiation and Herbal Use for Early Breast Cancer
Supplemental material, sj-docx-1-ict-10.1177_15347354231204008 for A Delphi Study of Expert Consensus on Chinese Medicine Syndrome Differentiation and Herbal Use for Early Breast Cancer by Qianqian Guo, Anthony Lin Zhang, Charlie Changli Xue, Meaghan E. Coyle and Qianjun Chen in Integrative Cancer Therapies
Supplemental Material
sj-docx-2-ict-10.1177_15347354231204008 – Supplemental material for A Delphi Study of Expert Consensus on Chinese Medicine Syndrome Differentiation and Herbal Use for Early Breast Cancer
Supplemental material, sj-docx-2-ict-10.1177_15347354231204008 for A Delphi Study of Expert Consensus on Chinese Medicine Syndrome Differentiation and Herbal Use for Early Breast Cancer by Qianqian Guo, Anthony Lin Zhang, Charlie Changli Xue, Meaghan E. Coyle and Qianjun Chen in Integrative Cancer Therapies
Supplemental Material
sj-docx-3-ict-10.1177_15347354231204008 – Supplemental material for A Delphi Study of Expert Consensus on Chinese Medicine Syndrome Differentiation and Herbal Use for Early Breast Cancer
Supplemental material, sj-docx-3-ict-10.1177_15347354231204008 for A Delphi Study of Expert Consensus on Chinese Medicine Syndrome Differentiation and Herbal Use for Early Breast Cancer by Qianqian Guo, Anthony Lin Zhang, Charlie Changli Xue, Meaghan E. Coyle and Qianjun Chen in Integrative Cancer Therapies
Supplemental Material
sj-docx-4-ict-10.1177_15347354231204008 – Supplemental material for A Delphi Study of Expert Consensus on Chinese Medicine Syndrome Differentiation and Herbal Use for Early Breast Cancer
Supplemental material, sj-docx-4-ict-10.1177_15347354231204008 for A Delphi Study of Expert Consensus on Chinese Medicine Syndrome Differentiation and Herbal Use for Early Breast Cancer by Qianqian Guo, Anthony Lin Zhang, Charlie Changli Xue, Meaghan E. Coyle and Qianjun Chen in Integrative Cancer Therapies
Footnotes
Acknowledgements
The authors wish to acknowledge Prof Xiaobo Yang, Dr Qian Li, Dr Xiuli Xie for their guidance of the Delphi study, and Yan Dai and the other colleagues from the Guangdong Provincial Hospital of Chinese Medicine for their help during this study. Finally, we would like to express our thanks to the experts who actively participated in this study and provided their professional comments.
Authors’ Contributions
QQG developed the study protocol, conducted the Delphi study, acquired and analysed the data, and wrote and edited the manuscript. ALZ and CCX commented on the study design and contributed to data interpretation and manuscript revision. MEC provided comments on the survey design and the study process, analysed and interpreted the results, and critically edited the manuscript. QJC provided comments on the study design and conduct, contributed to the interpretation of the study results, and revised the manuscript. All authors are accountable for all aspects of the work and approve the final version of the manuscript accepted for publication.
Data Availability
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Traditional Chinese Medicine Bureau of Guangdong Province (no. 20212079), and the School of Health and Biomedical Sciences (RMIT University) that provided the PhD scholarship to the first author.
Ethics Approval and Consent to Participate
Ethics approval was obtained from the Ethics Committee of Guangdong Provincial Hospital of Chinese Medicine (approval no. ZE2020-048-04) and was registered with the RMIT Human Research Ethics Committee (registration no. 23259). The requirement for written informed consent was waived for the anonymous online survey—experts’ completion of the survey indicated their agreement to participate.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.