
Abstract
Introduction:
Young women diagnosed with cancer are at an increased risk for infertility compared to women without a cancer diagnosis. Consuming a healthful diet comprised of whole grains, fruits, vegetables, and unsaturated fats has been found to improve both fertility and cancer survivorship. Given this reason, dietary interventions tailored to support female cancer survivors with fertility challenges are of immense importance. Therefore, the aim of this study was to explore barriers and facilitators to healthful nutrition among female cancer survivors with fertility challenges, to inform the development of dietary interventions for this population.
Methods:
Using a formative research design, interview, survey, and dietary intake data were collected from 20 female cancer survivors of reproductive age. Participant-check focus group discussions were conducted to validate findings. All interviews were recorded and transcribed verbatim. Transcripts were coded and analyzed using a thematic analysis approach. Quantitative data were analyzed using means, standard deviations, ranges, frequencies, and percentages.
Results:
The average age of respondents was 31.47 ± 3.5 years and the average BMI was 24.78 ± 4.1 kg/m2. All participants were college educated, 45% identified as White, 50% as Black, and 10% as Hispanic or Latinx. Cancer diagnoses included breast, thyroid, ovarian, leukemia, and gastrointestinal cancers. The following themes were identified: (1) Lack of nutrition-related resources and detailed guidance, (2) Work-life balance, (3) Perceived rigidity of dietary guidance, (4) Treatment-related fatigue, (5) Having trust in healthcare providers, (6) Higher motivation to change nutrition behavior, and (7) Recognizing the additional benefits of nutrition.
Conclusion:
These findings indicate a sought-after yet unmet need for post-cancer treatment fertility nutrition recommendations. Interventions should be tailored to women’s needs and focus on improving their self-efficacy to make healthful dietary choices.
Background
Many young women diagnosed with cancer have a higher chance of long-term survival due to improved treatment. Up to 90% of women under the age of 45 who were diagnosed with cancer in the past decade are expected to reach their 5 year survival marker. 1 However, advances in cancer treatment are also associated with additional quality-of-life challenges including challenges related to reproductive health and fertility. 2 For example, surgery, chemotherapy, and radiation can negatively impact many biological systems by disrupting the neuroendocrine system, ovarian function, and other reproductive organs in females resulting in infertility. 2 Infertility is particularly distressing for young female cancer survivors, who have a 30% increased relative risk compared to women without a cancer diagnosis, and has been referred to by many women as an emotional roller coaster.3-5 While there have been advances in fertility treatment methods, improvements in live birth rates are still marginal and the incidence of infertility remains high. 6
Nutrition plays a critical role in female fertility.6-9 A diet rich in whole grains, unsaturated fatty acids, vegetables, fruits, and fish has been associated with improved female fertility and fecundity.7-9 Similarly, dietary patterns comprised of these foods have demonstrated beneficial effects on cancer survivorship.10,11 Dietary recommendations for healthy cancer survivorship closely parallel the evidence-based dietary recommendations to support female fertility, and most of these foods are consistent with foods recommended in the U.S. Dietary Guidelines for Americans (DGAs). Consequently, augmenting fertility treatment methods for young female cancer survivors with nutrition-related guidance is a non-drug therapeutic option that could support reproductive function, improve cancer survivorship and self-efficacy to make healthier dietary choices. Additionally, adhering to healthful dietary practices can help women maintain a healthy body weight, and this may have positive implications for both female fertility and cancer survivorship.6,12
Despite the known benefits of a healthy diet on cancer survivorship, young adult cancer survivors face several barriers and challenges that make it difficult to follow recommendations to improve their dietary intake. Up to 94% are unable to meet national recommendations for the intake of several key nutrients and many have unhealthy diets consisting of high fat and low fruit and vegetable intake. 13 Barriers to improving dietary intake among young adult cancer survivors exist at multiple levels and identifying these barriers and challenges could be a critical step to developing strategies and interventions to improve nutrition-related behaviors.14,15 However, to date, no study has investigated nutrition-related barriers of female cancer survivors experiencing fertility challenges. Therefore, the aim of this research was to characterize the perceived barriers and facilitators to healthful nutrition among female cancer survivors with fertility challenges. The results of this research are intended to inform the development of future intervention(s) that incorporate dietary guidance into fertility counseling and treatment for female cancer survivors.
Materials and Methods
Study Design
Using a cross-sectional, multiple-methods study design, we conducted in-depth interviews with young female cancer survivors. We also collected demographic and personal information using a structured online survey and dietary intake information using three 24 hour dietary recalls. This study was approved by the Institutional Review Board at Drexel University. Data collection occurred between January and July of 2022.
Participants
Twenty female cancer survivors of reproductive age (18-40 years) who resided in the United States were recruited for participation in this study. Potential participants were recruited using ResearchMatch and online cancer survivorship support groups through flyer advertisements, emails, and phone calls. Participants were eligible if they had completed cancer treatment at least 6 months before the study, had resumed menstruation, had started or were considering family building, and could comply with the study procedures. Participants were excluded if they were undergoing active cancer treatment, had undergone a hysterectomy, or if they had not resumed menstruation. Participant sampling was purposive to maximize the diversity of experience among women and was informed by participant race/ethnicity, age, cancer type and fertility history. Participants were considered unable to reach if the study team received no response after contacting them at least 3 times. Women who met the inclusion criteria were enrolled in the study. The contact information of study team members, and the IRB at Drexel University, were provided to participants before they took part in any of the study activities. Eligible participants provided informed consent to take part in all study activities.
Data Collection and Analysis
All participants initially completed a structured demographics and personal characteristics survey. Descriptive data from the surveys were summarized as means, medians, range, and standard deviations for quantitative variables and frequencies and percentages for categorical variables, using SPSS v. 28.
One research team member conducted interviews virtually via HIPAA-compliant Zoom. In-depth interviews explored nutrition-related barriers and facilitators female cancer survivors experienced in their attempts to improve their health and fertility. Interviews lasted 30 to 45 minutes. Interviews were audio recorded, transcribed verbatim, and transcripts were reviewed for accuracy and consistency. Transcripts were uploaded into the NVivo qualitative software (QSR International Pty Ltd. Version 11, 2015) for data management and to facilitate coding. Transcripts were thematically analyzed using a hybrid inductive and deductive coding approach. 16 A preliminary codebook was developed and refined, and codes were operationally defined to facilitate consistency in coding. Two team members coded all transcripts and discussed emerging themes with a third team member. Themes were reviewed by other research team members to ensure that they were a true reflection of participants’ experiences.
Dietary Assessment
Dietary intake information was collected after the interviews on 3 non-consecutive days (2 weekdays and 1 weekend day) using the Automated Self-Administered 24-hour (ASA24®) Dietary Assessment Tool, which is a web-based self-administered 24 hour dietary recall system. 17 These data were used to calculate individual Healthy Eating Index-2015 (HEI-2015) scores and facilitated the comparison of responses between participants with relatively healthful dietary patterns and those with less healthful diets. The HEI-2015 score comprises 13 components that reflect different food groups and adherence to the 2015 to 2020 Dietary Guidelines for Americans.18,19 These components include adequate consumption of total fruit, whole fruit, total vegetables, greens and beans, whole grains, dairy, total protein foods, fatty acids, (the ratio of unsaturated fatty acids to saturated fatty acids), seafood and plant proteins; and moderate consumption of refined grains, sodium, added sugars and saturated fats.18,19
Establishing Validity
Participant checking was employed post-analysis as a form of establishing validity. This method ensured that participants’ own meanings and perspectives were represented and not overshadowed by the researchers’ interpretations. 20 A sample of 9 interview respondents were recruited to participate in a participant-check focus group discussion (composed of 2-5 individuals; 3 focus group discussions in total). Themes identified from the analysis of the interviews were presented to participants for feedback regarding the accuracy of the themes. 21 Data obtained during the participant-check focus group were included in data analysis and interpretation.
Results
Descriptive Characteristics
Table 1 displays participant sociodemographic and personal characteristics. Twenty female cancer survivors completed this study. The mean age was 31.47 ± 3.5 years and the mean Body Mass Index (BMI) was 24.78 ± 4.1 kg/m2. Forty-five percent identified as White, 50% identified as Black/African American, and 10% identified as Hispanic or Latinx. The majority of the women (90%) were married or living as married, 75% were college graduates and 25% were in graduate school. Regarding cancer type, 20% had survived breast cancer, 30% ovarian cancer, 20% thyroid cancer, 10% leukemia, and 20% had survived other cancers. The median number of years since cancer diagnosis was 3.5 years, ranging from 1 to 16 years. The majority of the women had undergone surgery (65%), chemotherapy (60%), or a combination of surgery and chemotherapy (30%).
Participant Demographic and Personal Characteristics.

Endometrial, liver, neuroendocrine and gastrointestinal tract cancer.
Fertility History
Sixty-five percent reported having no children at the time of data collection. Sixty percent were currently trying to conceive, 42% had been trying for 12 or more months, whereas 58% had been trying for less than 12 months. Few participants (15%) had used fertility treatment (egg retrieval, artificial insemination, and hormone therapy) for any pregnancy prior to cancer diagnosis and only a third (33%) had been successful. Thirty percent had undergone fertility preservation before cancer treatment. Similarly, few women (30%) had undergone fertility treatment after cancer, with half (50%) of them having gone through artificial insemination. The majority of participants had regular periods (80%), defined as an average cycle of 28 days, with a median duration of 4 days. The CDC defines regular periods as an average cycle length of 28 days, ranging from 21 to 35 days. 22
Dietary Quality
The median HEI-2015 score for women in this study was 57.5 out of a total of 100, with a range of 39 to 90. Using a cut-off score of 53.2, women were placed in 2 groups, those who scored <53.2 (lower dietary quality group, n = 7) and those who scored ≥53.2 (better dietary quality group, n = 13). This cut-off score was determined using the average HEI-2015 score of cancer survivors aged 20 to 44 years from the National Health and Nutrition Examination 2005 to 2016 survey data. 18
Figure 1 displays a radar plot of the comparative distribution of the HEI-2015 component scores for women with better dietary quality and women with lower dietary quality as a percentage of the maximum possible score for each component. On average, women in the better dietary quality group had better diet quality for all components of the HEI score apart from dairy and sodium. Dairy intake was low in both groups, and sodium intake was high.
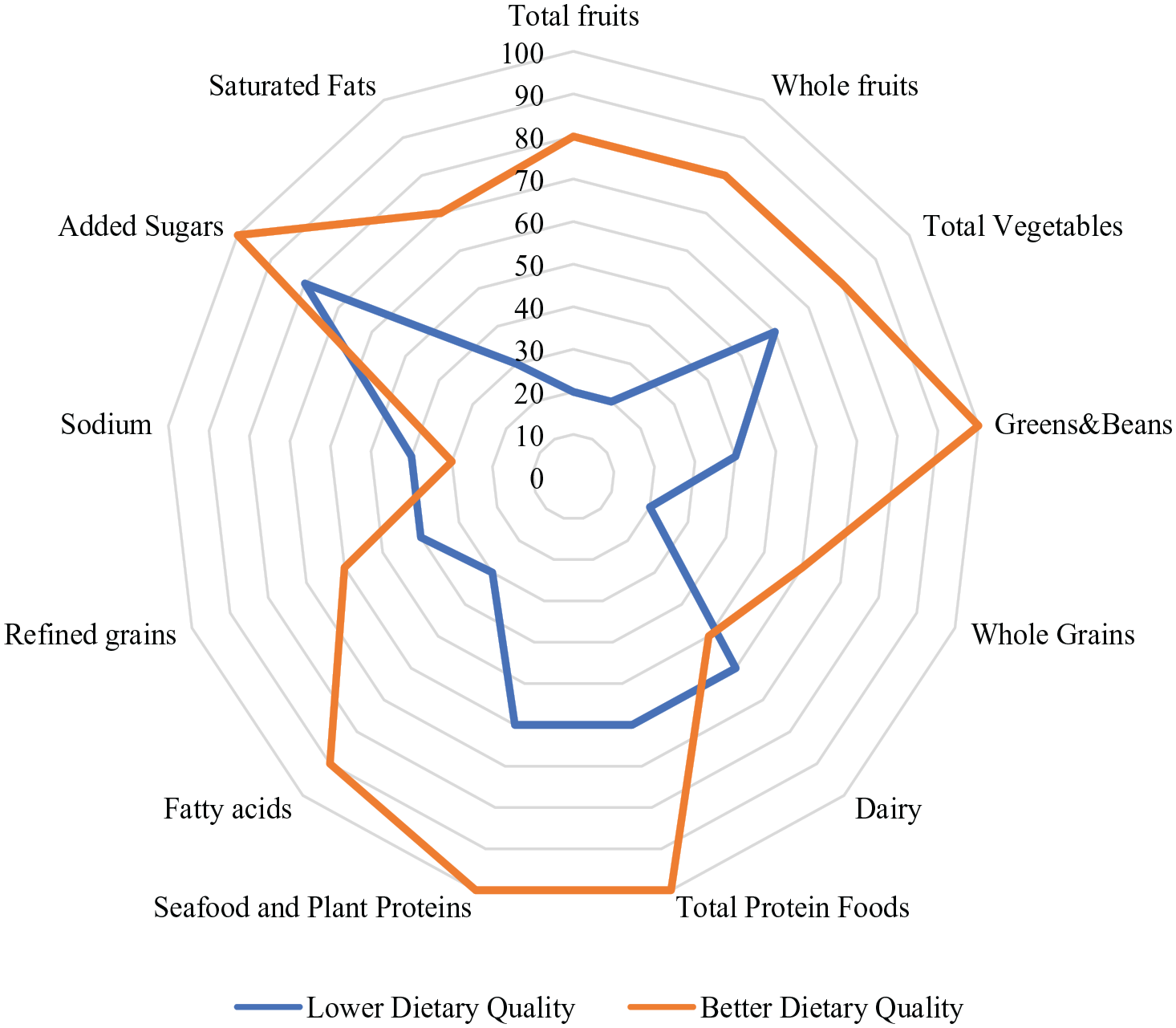
Radar plot showing the distribution of HEI-2015 component scores for women with lower and better dietary quality.
Qualitative Findings
This analysis presents the themes that emerged from in-depth interviews and participant-check focus group discussions. Four themes emerged as barriers to healthful nutrition: (1) Lack of nutrition-related resources and detailed guidance, (2) Work-life balance, (3) Perceived rigidity of dietary guidance, and (4) Treatment-related fatigue. These themes emerged predominantly among women with lower dietary quality (Supplemental Table 1). Three themes emerged as facilitators of healthful nutrition: (1) Having trust in healthcare providers, (2) Higher motivation to change nutrition behavior, and (3) Recognizing the additional benefits of nutrition. These themes emerged primarily among women with better dietary quality (Supplemental Table 1).
The following section of the results presents the themes and Table 2 summarizes these themes using exemplar quotes. Names associated with the quotes are pseudonyms (Supplemental Table 1).
Themes With Exemplar Quotes.

Barriers to Healthful Nutrition
Theme 1: Lack of Nutrition-Related Resources and Detailed Guidance
Many women (n = 14) reported seeing a licensed healthcare provider including a registered dietitian, nutritionist, doctor, or naturopath (practice focuses on the body’s self-healing ability
23
) to discuss healthful eating regarding cancer treatment, survivorship, and or fertility. However, some of these women felt they were “not gaining much” or that they had received “surface information.” A smaller proportion of women (n = 6) reported not having discussed nutrition with a healthcare provider at any point during their cancer treatment, survivorship, or fertility treatment period. They attributed this to nutrition not being “well-integrated into the healthcare system” and healthcare providers being more focused on cancer treatment, stating that nutrition was “outside of their scope.” When asked if nutrition and dietary information were discussed during cancer follow-up care visits with her oncologist and endocrinologist, Monica, a 33-year-old thyroid cancer survivor shared,
Her experience was no different from Sandra, a 30-year-old breast cancer survivor who recounted she had not received any information or guidance from a healthcare provider at any point during her cancer trajectory.
In general, the majority of women (n = 13) who received nutrition information from healthcare providers had higher HEI-2015 scores indicating better dietary quality. For example, Helen, a 29-year-old ovarian cancer survivor, recounted having received specific nutrition information from her dietitian during and after cancer treatment.
“My dietitian actually stated that nutrition is key, not only to health, but my wellbeing. And he was like I should basically eat more food with high fiber and oh, such as bread, whole grains and also I should cut down [on fatty foods and take in] low fat dairy products.”
Theme 2: Work-Life Balance
Generally, many women (n = 18) indicated they tried to make healthful food choices based on their history of cancer. However, although many women desired to eat healthfully, this was not always possible due to their demanding jobs. Several women (n = 7) articulated that their busy schedules were the reason they resorted to meals that were convenient and easy to prepare. Lily, a 25-year-old leukemia survivor, stated:
“When I get extremely stressed, and I have too many things going on to manage, then like, my diet is probably one of the first things that goes out the door.”
Similar to Lily, Monica, a 33-year-old thyroid cancer survivor, reiterated how work-related time constraints had her skipping multiple meals a day.
“That is pretty frequent. I often don’t have breakfast just because I feel too busy in the morning.”
Theme 3: Perceived Rigidity of Dietary Guidance
For some women (n = 7), overly rigid diet plans left them unable to follow through with these plans. Some of these women felt they were “ordered to follow” and had to “restrict” themselves. Women in families also had challenges preparing separate meals for themselves and their children. Trina, a 30-year-old ovarian cancer survivor, reported seeing a dietitian after cancer treatment. For her, starting a meal plan was tough because she had to search for specific ingredients and her recommended meal plan involved following a monotonous dietary pattern.
“It was difficult to follow. You know at first I wasn’t used to eating in that kind of way. Like, I don’t really like cooking that much, so sometimes I just go with the easy foods to make and the rest. And it was difficult because, you have to get this, you have to get that, you have to make sure the ingredients are complete. . . And then it was just crazy because you have to follow one pattern of eating.”
Tina, a 28-year-old ovarian cancer survivor, also recounted receiving dietary advice from a dietitian, which she describes as having to “abide by the rules.” For Tyra, a 35-year-old, breast cancer survivor, her dietitian had provided nutrition guidance during and after cancer treatment, which she also found difficult to follow because her family was eating differently from her, causing her son to voice concerns about her diet.
“I look at them [husband and son] eating, and I look at what I’m eating, I would want to eat, what they are eating. Sometimes my son [will say] ‘Oh mommy the food isn’t the same, why are you eating different? Are you going to die?’”
Theme 4: Treatment-Related Fatigue
During the participant-check focus group discussions, a new theme emerged about lingering symptoms and side effects, termed treatment–related fatigue or “exhaustion.” Although all participants were 6 months or more out of treatment, some (n = 6) complained about intermittent feelings of exhaustion post-cancer treatment. While not all participants who mentioned this barrier had low dietary quality, this barrier is worth mentioning since it was pervasive among participants during the focus group discussions. Some of these women recounted days when they were exhausted and could not perform activities like preparing their own meals. These instances of treatment-related fatigue were often “unpredictable.” Due to this, some women either relied on their spouses to cook or resorted to preparing what was “convenient” but not necessarily healthy. Ann, a 37-year-old leukemia survivor, recounted her experience with treatment-related fatigue and how she resorted to getting takeout sometimes or prioritized house chores over her nutrition based on her energy levels.
“I’d say, for me, sometimes it’s just pure exhaustion. . . So, I’ll go eat a can of soup or get fast—or not necessarily fast food but takeout. And sometimes I just don’t feel like doing that, or I have to prioritize the little bit of energy that I have. That’s going to be, “Go to do the laundry,” because that really needs to be done, [laughter] and I have no clean clothes up. I can heat something up, easier than I can have someone else do my laundry.”
Monica, a 33-year-old thyroid cancer survivor, reiterated Ann’s point about treatment-related fatigue and went ahead to elaborate on how her husband takes over the role of grocery shopping and cooking during this period, although they have different preferences in food.
“So, I’m similar, just exhaustion . . . And I live with my husband, who helps out a lot. But we don’t necessarily have the same taste in food. So, I would say if he’s the one grocery shopping or cooking, it might be different than something that I might want to have. We compromise. Sometimes he eats what he [laughter] doesn’t want it either. But I think that’s also a challenge, like having something that we’re both happy to have as a meal.”
Facilitators of Healthful Nutrition
Theme 1: Having Trust in Healthcare Providers
When asked about trust in their source of nutrition information, some women (n = 6) with better dietary quality reported trusting their healthcare providers to provide them with adequate nutrition information. Tina, a 28-year-old ovarian cancer survivor, who was referred to a dietitian by her primary care physician early on during cancer treatment, described feelings of trust in the nutrition information she had received because she felt her dietitian knew what he was doing.
“I feel it [nutrition information] was enough because my dietitian was someone that was actually recommended by my family doctor. . . I feel that he knows what he’s actually doing, very professional.”
Like Tina, Ruth, a 30-year-old ovarian cancer survivor who had received nutrition advice from her primary care physician during cancer treatment and survivorship, articulated trust in the information she had received because of the longstanding relationship she had with her healthcare provider.
“So, I kind of trust the whole information he [primary care physician] was giving me because I’ve known him for a very long time. . . I kind of trust whatever he told me about.”
Theme 2: Higher Motivation To Change Nutrition Behavior
Women who showed higher motivation to change their nutrition behavior also had high HEI-2015 scores. Maribel, a 33-year-old gastrointestinal cancer survivor, and a registered dietitian, who was pregnant at the time of the study described her motivation for healthful eating as not wanting to “play games” with herself.
“It [cancer] helped me to realize how like important was diet and I don’t—Like I don’t want to play games with myself.”
Similar to Maribel, Helen, a 29-year-old ovarian cancer survivor also reported being ready to do what is necessary for her health as long as she reaps the benefits.
“What I have to do, I just have to do it. As long as it’s gonna be beneficial for me.”
Theme 3: Recognizing the Additional Benefits of Nutrition
For Trina, a 30-year-old ovarian cancer survivor, recognizing the additional benefits of healthful nutrition such as weight maintenance was an important motivator for her to eat healthy.
“Because when I followed the whole diet plan that was given to me, I felt that’s—like it wasn’t just working on just my cancer treatment alone, like it was actually helping me with my weight. . . Like killing two birds with one stone.”
Kristen, a 31-year-old cancer survivor also reported having heard from some healthcare providers the possibility of using nutrition to manage lingering symptoms post-cancer treatment.
“Because I felt a little bit lingering symptoms and I have had some of them [healthcare providers] talk to me about nutrition as being a potential treatment option, in terms of diet as a way of treating yourself.”
Discussion
This study explored the barriers and facilitators to improving nutrition-related behaviors among female cancer survivors with fertility challenges. Our findings suggest that female cancer survivors face multiple level barriers (lack of nutrition-related resources and detailed guidance, work-life balance, perceived rigidity of diet plans, and treatment-related fatigue) to improving their nutrition. Whether or not women reported receiving nutrition information during general cancer survivorship or fertility treatment, these barriers were pervasive and are in tandem with previous research regarding cancer survivors of similar age as our population.14,15
Lack of Nutrition-Related Resources and Detailed Guidance
Female cancer survivors like other cancer survivors often report unmet information needs that prevent them from engaging in healthful behaviors, including healthful eating.24-26 For example, Halbach et al conducted a prospective cohort study in Germany that investigated the level of unmet information needs among female breast cancer survivors. Their study found persistent unmet information needs including health promotion (nutrition and self-help) needs among this population during their cancer trajectory, however, this need was slightly decreased post-treatment. 27 Though the authors attributed this reduction to rehabilitation programs for cancer survivors that incorporated nutrition and other self-help information, they emphasized the need for additional strategies to reduce unmet information needs among breast cancer survivors. 27 Likewise, in a qualitative study in Australia by James-Martin et al that assessed the information needs of adult cancer survivors, participants reported a general lack of information about diet, weight, and exercise. 28
Perceived Rigidity of Dietary Guidance
Many women in our study who reported receiving guidance commented about the rigidity of the guidance they received. It can be challenging for female cancer survivors to consistently follow the strict diets suggested by healthcare providers. These diets often require specific quantities, qualities, and timings of meals, which can lead to a cycle of strict adherence followed by non-adherence. 29 Additionally, the term “diet” can sometimes have negative connotations and suggest a departure from one’s usual eating habits. 30
To help female cancer survivors follow dietary recommendations that promote healthy cancer survivorship and fertility, one effective strategy is to combine evidence-based dietary patterns with effective nutrition counseling strategies such as motivational interviewing, self-monitoring, social support, goal setting, group counseling and cognitive restructuring. 31 Most often, multiple nutrition counseling strategies would need to be integrated to achieve results. For example, a study by Zuniga et al found that a nutrition intervention, which combined motivational interviewing, goal setting, group workshops and culinary instruction led to an increased adherence to the Mediterranean dietary pattern among breast cancer survivors in the U.S. 32 Similarly, health behavior interventions involving nutrition, in a randomized controlled trial study by Park et al among breast cancer survivors in the U.S. that employed behavioral goal setting, recipe modifications, and accountability, increased participants’ fruit and vegetable intake and physical activity levels. 33 By combining evidence-based dietary patterns with nutrition counseling strategies, women’s self-efficacy to adhere to these recommendations will improve, which will make them more confident in their own abilities to change their dietary behaviors.
Work-Life Balance
Several women in this study reported work-related barriers to healthful dietary intake, particularly the lack of time and stress associated with their jobs. This finding is in line with other studies that have found work demands to be among the most common barriers to healthful lifestyle behaviors among young adults.34,35 For example, a U.S. population-based cohort study that investigated time-related beliefs and behaviors regarding healthful eating and dietary intake among young adults found that young adult females who worked >40 hours a week or reported longer part-time hours (20-39 hours) experienced time-related barriers to healthful eating. These included not having time to think about eating healthfully, eating on the run, and being too busy to eat healthfully. 36 Similarly, a review article by Munt et al involving 34 original peer-reviewed studies, found that young adults lacked the time to plan, shop and prepare healthy foods due to their demanding jobs and academic pursuits. 37 Providing practical solutions for healthier eating habits is crucial for young adults, particularly female cancer survivors. This could include the provision of convenient food delivery services, meal kits, and meal plans that can seamlessly fit into their demanding work schedules.38-40
Treatment-Related Fatigue
Women in this study reported treatment-related fatigue to be a barrier to healthful dietary intake. Being too tired to prepare healthful meals was often the consequence of this fatigue and many had to rely on spouses or partners to cook. This echoes the findings of several other studies about the impact of treatment-related fatigue on healthful lifestyle behaviors among cancer survivors.41-44 For example, a qualitative study among female breast cancer survivors in Australia that explored survivors’ perceptions of dietary habit changes found many survivors had made dietary changes to reflect current recommendations. Participants also reported barriers to making healthful dietary changes such as feeling too tired to plan or prepare meals as they would before cancer. 45 Interventions to help women prepare and eat healthful meals should be developed such as those that promote quick recipes and easy-to-prepare foods, since these interventions have the potential to increase self-efficacy. A pilot mixed-method study among cancer survivors with cancer-related fatigue in Canada, investigating the feasibility, acceptability, and effectiveness of a culinary intervention, found improvement in fatigue management and confidence in culinary skills among participants. 46 In a recent systematic review that included nearly 400 original peer-reviewed research articles, authors examined the influence of cooking interventions (meal planning and shopping, cooking recipes, and cooking skills) on psychosocial outcomes and also found improvements in self-esteem and self-confidence, reduced anxiety, and improved quality of life among healthy adults and adults with chronic diseases including cancer. 47 Encouraging social support from spouses, family, friends, and other community networks is also crucial in helping women maintain healthful dietary habits. This assertion is in line with a survey-based study in the U.S., which examined factors associated with fruit and vegetable intake and physical activity among cancer survivors, that found social support from family, friends, and partners to be the single most important factor associated with fruit and vegetable intake and physical activity among this population. 48 Likewise, a quasi-experimental study in the U.S. among middle aged healthy adults that investigated the impact of a behavioral nutrition intervention on dietary intake found increased social support among participants who had significant improvements in their dietary intake. 49
Facilitators of Healthful Nutrition
Facilitators of healthful dietary behavior identified among women in this study with better dietary quality included having trust in their healthcare providers (registered dietitian, primary care physician, and oncologist), having a higher motivation to change nutrition behavior, and recognizing the additional benefits of nutrition. Studies have found that receiving guidance and clear recommendations from trusted sources, such as healthcare providers, positively influences cancer survivors’ motivation to change their nutrition behavior.50-52 For example, a qualitative study in the UK by Beeken et al among adult cancer survivors exploring their beliefs about dietary quality and cancer found participants to be skeptical about nutrition information from sources other than healthcare providers. 51 Similarly, in another study that investigated the influence of nutritional information on dietary behaviors among Dutch cancer survivors, respondents indicated that they preferred to receive nutrition information from healthcare professionals (oncology nurses, registered dietitians, and doctors). Further, participants who received nutrition information from these preferred sources reported changing their dietary behaviors. 52 Moreover, having additional reasons to engage in healthful nutrition including weight loss and chronic disease prevention, have been found to be facilitators for healthful eating among several cancer survivorship populations including prostate cancer survivors 53 and young adult cancer survivors. 15
Strengths and Limitations
The primary strength of this study is that it addresses an important yet unmet need. To date, no other study has explored nutrition-related barriers and challenges among female cancer survivors with fertility challenges. This is important because interventions that seek to augment fertility treatment can be optimized by considering and addressing barriers and facilitators during the development stage. An additional strength was the use of multiple data sources (structured survey, dietary assessment, in-depth interviews, and participant-check focus group discussions) to achieve the study results. Data were explored concurrently and iteratively to provide a deeper interpretation of findings.
A limitation of this study is that the majority of women had higher education and generally higher socioeconomic status. Future studies may need to investigate if these findings are similar for women with diverse educational and socioeconomic backgrounds. Additionally, the majority of study participants had not experienced fertility preservation or treatment. Moreover, this current study involved women with a mean of BMI: 24.78 ± 4.1 kg/m2, and 70% reported healthy body weight (18.5-24.9 kg/m2). Most studies in the U.S. have reported higher mean BMI among young adult cancer survivors compared to our study.54-56 Therefore, a future study involving a more representative BMI sample of women is needed to compare and contrast this study’s findings and to determine if female cancer survivors’ nutrition-related challenges and needs differ in relation to their body weight. Future studies could also further investigate nutrition-related challenges among female survivors of different racial and ethnic backgrounds, different cancer types, and treatments.
Conclusion
The results of this study have several implications for nutrition interventions that aim to support fertility treatments for female cancer survivors. Nutrition programs and interventions intended for female cancer survivors should be presented using tools such as motivational interviewing, self-monitoring, social support, and other evidence-based strategies. Healthcare professionals should deliver these programs in a clear and actionable manner to improve motivation, adherence, and self-efficacy among this population. Additionally, future studies should test the impact of integrating effective nutrition counseling strategies into dietary interventions through mobile apps, social media platforms and informative websites. This could improve adherence to dietary recommendations that promote healthy cancer survivorship and successful fertility treatment outcomes. These interventions could be tailored to accommodate women’s work schedules to improve adherence. Culinary education could also be integrated into interventions to help improve survivors’ cooking self-efficacy, motivation, and fatigue management. 46 Moreover, future interventions for this population should be evidence-based, include engagement with multiple stakeholders (female cancer survivors, healthcare providers, and policymakers), and follow a structured pathway for development. 57 Therefore, we intend to continue exploring and refining our study findings using validated intervention development framework(s).
Supplemental Material
sj-docx-1-ict-10.1177_15347354231191984 – Supplemental material for Optimizing Fertility Treatment With Nutrition Guidance: Exploring Barriers and Facilitators to Healthful Nutrition Among Female Cancer Survivors With Fertility Challenges
Supplemental material, sj-docx-1-ict-10.1177_15347354231191984 for Optimizing Fertility Treatment With Nutrition Guidance: Exploring Barriers and Facilitators to Healthful Nutrition Among Female Cancer Survivors With Fertility Challenges by Cynthia Klobodu, Jonathan Deutsch, Mara Z. Vitolins, Kathleen Fisher, Jennifer A. Nasser, Dahlia Stott and Brandy-Joe Milliron in Integrative Cancer Therapies
Supplemental Material
sj-docx-2-ict-10.1177_15347354231191984 – Supplemental material for Optimizing Fertility Treatment With Nutrition Guidance: Exploring Barriers and Facilitators to Healthful Nutrition Among Female Cancer Survivors With Fertility Challenges
Supplemental material, sj-docx-2-ict-10.1177_15347354231191984 for Optimizing Fertility Treatment With Nutrition Guidance: Exploring Barriers and Facilitators to Healthful Nutrition Among Female Cancer Survivors With Fertility Challenges by Cynthia Klobodu, Jonathan Deutsch, Mara Z. Vitolins, Kathleen Fisher, Jennifer A. Nasser, Dahlia Stott and Brandy-Joe Milliron in Integrative Cancer Therapies
Footnotes
Author Contributions
The authors’ contributions to the manuscript are as follows: BJM, CK and JN conceptualized and designed the study. CK collected the data. CK, BJM and DS analyzed the data. CK and BJM had responsibility for the final content. All authors contributed to the synthesis and refining of themes, writing of the paper, reading and approval of the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the American Society for Nutrition Foundation (ASNF) Predoctoral Fellowship Award and the Drexel University College of Nursing and Health Professions Dean’s PhD Student Research Award.
Data Sharing
Data will be made available upon request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.