
Abstract
Fatigue, experienced by patients during and following cancer treatment, is a significant clinical problem. It is a prevalent and distressing symptom yet pharmacological interventions are used little and confer limited benefit for patients. However, many cancer patients use some form of complementary and alternative medicine (CAM), and some evidence suggests it may relieve fatigue. A systematic review was conducted to appraise the effectiveness of CAM interventions in ameliorating cancer-related fatigue. Systematic searches of biomedical, nursing, and specialist CAM databases were conducted, including Medline, Embase, and AMED. Included papers described interventions classified as CAM by the National Centre of Complementary and Alternative Medicine and evaluated through randomized controlled trial (RCT) or quasi-experimental design. Twenty studies were eligible for the review, of which 15 were RCTs. Forms of CAM interventions examined included acupuncture, massage, yoga, and relaxation training. The review identified some limited evidence suggesting hypnosis and ginseng may prevent rises in cancer-related fatigue in people undergoing treatment for cancer and acupuncture and that biofield healing may reduce cancer-related fatigue following cancer treatments. Evidence to date suggests that multivitamins are ineffective at reducing cancer-related fatigue. However, trials incorporated within the review varied greatly in quality; most were methodologically weak and at high risk of bias. Consequently, there is currently insufficient evidence to conclude with certainty the effectiveness or otherwise of CAM in reducing cancer-related fatigue. The design and methods employed in future trials of CAM should be more rigorous; increasing the strength of evidence should be a priority.
Keywords
Background
Fatigue is a common and debilitating symptom of cancer and its treatment. A systematic review of 40 cancer-related fatigue studies reported prevalence rates for this symptom ranged from 46% to 96% and determined that it persisted well beyond the end of treatment in at least a quarter of patients. 1 Estimates of prevalence differed considerably between studies depending on the patient diagnostic group assessed, treatment received, and scale used to measure fatigue. A further review identified its significant impact on patients’ lives and activities of daily living and provided some evidence of the economic consequences of this symptom for both patients and their families. 2 Fatigue experienced by cancer patients before, during, and after chemotherapy seems to be higher than that experienced by healthy volunteers. 3 A consistent and key predictor of cancer-related fatigue seems to be the presence of emotional distress or mood disturbance.4,5
There are very few pharmacological options for the management of cancer-related fatigue and limited evidence regarding their effectiveness. A recent review of available research evidence determined that methylphenidate (a psycho stimulant) is more effective than placebo in reducing fatigue, as is erythropoietin in anemic patients experiencing fatigue. However, recent evidence has raised concerns about the safety of erythropoietin, suggesting it should not be used for the management of cancer-related fatigue. Finally, the review found that progestational steroids and paroxetine are no better than placebo. 6
Appraisal of nonpharmacological interventions to manage fatigue, including psychological and activity-based interventions, suggests that multimodal exercise and walking programs, restorative approaches, supportive-expressive, and cognitive-behavioral psychosocial interventions have potential to reduce cancer-related fatigue.7,8 A Cochrane review that focused on the effectiveness of psychosocial interventions found 7 studies where the intervention of choice had a significant effect on fatigue (out of 27 studies assessed); the reduction in fatigue was higher in interventions specific to this symptom (80%) than those not specifically addressing it (14%). Psychosocial interventions have been defined as influencing or changing cognitions, emotions, behaviors, or a combination of these. 9
While the role of psychosocial and activity-based interventions in the management of cancer-related fatigue is increasingly established and the role of pharmacological treatments appears limited, there are a growing number of studies that have explored the impact of complementary and alternative medicine (CAM) on cancer-related fatigue. CAM incorporates approaches outside of conventional medicine, and these interventions are being undertaken in an effort to increase the pool of options available for the management of this complex and burdensome symptom. The Oncology Nursing Society’s Putting Evidence into Practice resource reviewed and classified the effectiveness of various fatigue interventions, including some forms of CAM. 10 Their conclusion was that for the CAM interventions reviewed there was insufficient or conflicting data regarding their effectiveness for relieving cancer-related fatigue. They also determined that there was no indication they were harmful. They surmised that if their effectiveness could be determined through large well-conducted randomized controlled trials (RCTs) they could have particular benefit for palliative care populations where other effective interventions including exercise may be contraindicated. Currently, there is only one published narrative review that has explicitly appraised CAM interventions for cancer-related fatigue (21 trials assessed). 11 This suggested that acupuncture, aromatherapy, adenosine triphosphate infusions, energy conservation, activity management, healing touch, hypnosis, lectin-standardized mistletoe extract, levocarnitine, massage, mindfulness-based stress reduction, polarity therapy, relaxation, sleep promotion, support groups, and Tibetan yoga may reduce cancer-related fatigue. However, as with Mitchell et al, 10 the authors concluded that there were insufficient data to make clinical recommendations. 11 Key issues with studies they reviewed were their variable quality, lack of randomization, heterogeneous outcomes, small sample sizes, and incorporation of fatigue as a secondary outcome; all these variables render the results at high risk of bias.
However, although the review by Sood et al 11 provides some evidence in support of using CAM in the management of cancer-related fatigue, the review had several shortcomings. First, their search strategy was not presented; thus, the comprehensiveness of their search was unclear. Second, it lacked stringent inclusion and exclusion criteria. Finally, several new studies of CAM interventions for cancer-related fatigue have been published, with promising results, since Sood et al 11 reviewed the literature. Consequently, the current review was undertaken to provide a contemporary appraisal of the relative effectiveness of different CAM interventions in managing cancer-related fatigue.
Working Definition of CAM
For the purposes of the current review, CAM is defined according to the definition used by the Cochrane Collaboration and quoted by Zollman and Vickers. 12
Complementary and alternative medicine (CAM) is a broad domain of healing resources that encompasses all health systems, modalities, and practices and their accompanying theories and beliefs, other than those intrinsic to the politically dominant health system of a particular society or culture in a given historical period.12(p693)
As this is a broad definition and lacks specificity regarding specific CAM practices, the National Center of Complementary and Alternative Medicine’s classification of CAM practices was used to define which CAM modalities would be included in the review (see Selection Criteria).
Methods
The aim of this review was to appraise systematically the evidence for the effectiveness of CAM in the alleviation of cancer-related fatigue. A comprehensive search for clinical research was carried out. Systematic searches were conducted on a range of databases; in addition, searching was undertaken of previous literature reviews and reference lists of relevant papers.
Databases Searched
Systematic searches of major biomedical, nursing, and specialist CAM databases were carried out. We searched the Cochrane Register of Controlled Trials (June 2010), MEDLINE (1950 to June Week 2 2012), EMBASE (1980 to June Week 2 2012), British Nursing Index (1985 to June Week 2 2012), PsychINFO (1806 to June Week 2 2012), EBMR (1982 to June Week 2 2012), and AMED (1985 to June 2012).
Search Terms
Search strategies were developed to accommodate the different indexing approaches used by databases. The search strategy included a combination of terms and text words for cancer-related fatigue and different forms of CAM. The CAM search strategy was broad and covered all the therapies classified under the National Center for Complementary and Alternative Medicine (NCCAM). A MEDLINE search strategy was developed (Box 1) and adapted as appropriate for other databases. The search generated 2398 references. Of these, 78 papers appeared potentially relevant for the review and were retrieved in full; application of the inclusion and exclusion criteria identified 20 relevant papers. These were incorporated into the review (Figure 1).
Medline Search Strategy.

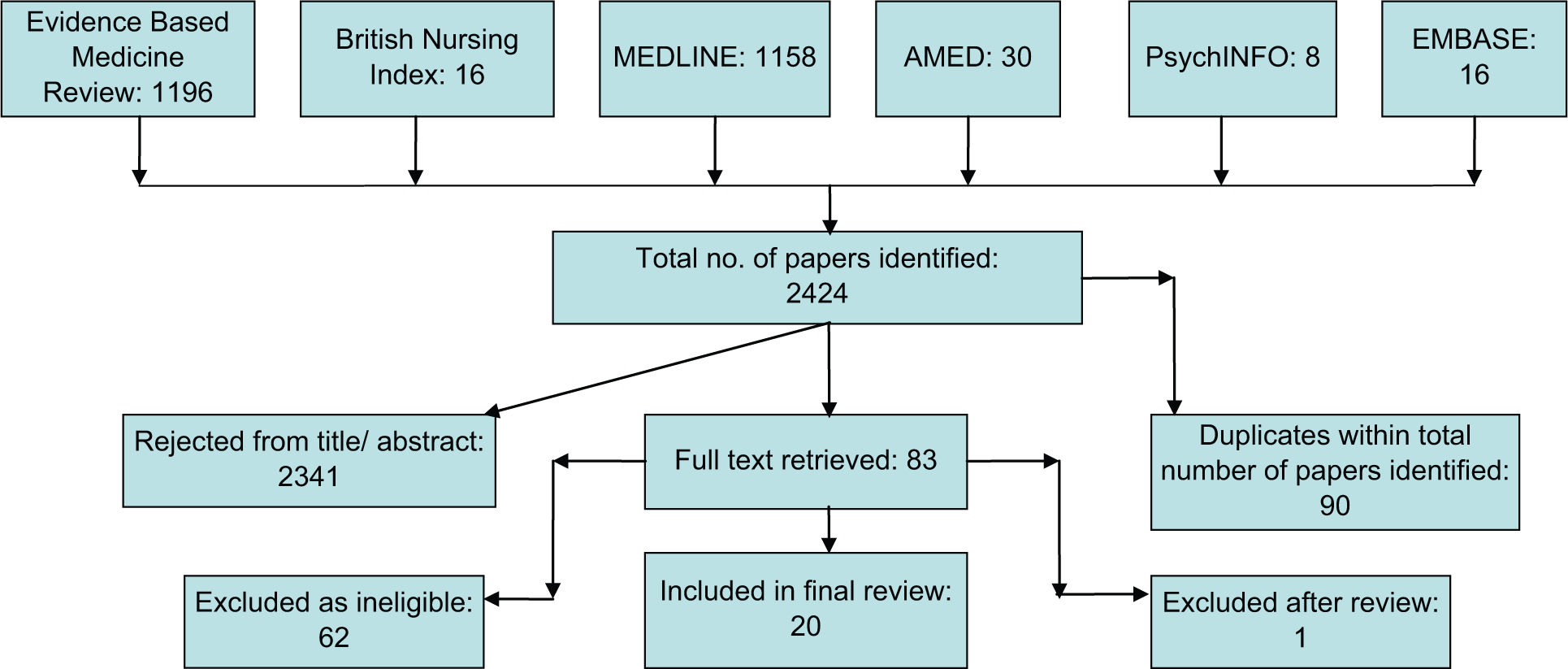
Identification and selection of articles.
Selection Criteria
To be included in the review, papers had to
Be published in English in a peer reviewed journal
Be a RCT or quasi-experiment where at least one form of CAM was tested against a control condition
Report on participants over 18 years having/having had treatment for cancer
Test at least one CAM as classified by the NCCAM as natural products, biologically based medicine, energy medicine, manipulative and body-based practices, mind–body medicine, or whole medical systems approach
Have cancer-related fatigue as a primary or secondary outcome
Measure fatigue using a single-item, multi-item, or multicomponent measure or as a dimension of a quality of life scale
Papers were excluded where interventions were not included within the NCCAM classification list. This list excludes psychosocial interventions such as cognitive–behavioral therapy.
Data Extraction and Synthesis
Data extraction forms were developed to enable pertinent details regarding the quality of the studies to be collated along with the results they generated. Data were extracted on the following: author names, journal and year of publication, location of research team, population studied, sample inclusion/exclusion criteria and characteristics, CAM intervention details, research design (including markers of quality RCTs including randomization, blinding, intention to treat analysis, control of confounding factors), outcome measures, statistical methods, study findings, and authors’ conclusions. The studies were assessed for quality using the Oxford Quality Score/Jadad score. 13 The process was undertaken by JFJ and checked independently by AR. Differences in opinion and discrepancies were resolved through discussion. Where differences of opinion remained, a third reviewer from the team was available for consultation (ER, AM). However, such arbitration was not required during the review. Thus, to enable data to be compared within and between CAM treatment modalities, and across the treatment trajectory, the pre–post changes in fatigue scores reported were standardized by presenting the change as a percentage of the original score reported by the study groups (Table 1). This was possible for all except 4 studies.14-17,23 These did not present baseline and post test scores rendering this calculation impossible. Furthermore, the difference in percentage change between the intervention and control groups was additionally calculated (Table 1). Diversity within and between treatments, when they were administered, and how fatigue was measured (Table 2) resulted in a level of heterogeneity that rendered meta analysis ill-advised. Furthermore, standard deviations were seldom presented within papers preventing calculation of effect sizes.
Details of Papers Included in the Review.

Abbreviations: CT, chemotherapy; RT, radiation therapy; RCT, randomized controlled trial; PMRT, progressive muscle relaxation training.
Complementary and Alternative Medicine Intervention Dose and Frequency.

Results
Of the 20 studies included in this review, 15 were RCTs, 3 were either phase II or counterbalanced trials, and 3 studies used a quasi-experimental design. All studies reported some form of summary fatigue score depicting either fatigue severity14-19,21,23,25,26,28-33 or a score combining fatigue severity with its interference with daily life.20,22,24,27 A few studies reported on additional domains of fatigue, for example, physical fatigue or cognitive fatigue.19,20,27,29-31
Characteristics of Participants
In total, 1560 people were evaluable in the studies. Sample sizes varied considerably across studies reviewed and ranged from 13 participants 29 to 200. 14 The median sample size was 75 (mean = 78). The majority of participants across the studies was female (80% of the total combined evaluable sample). Ten of the studies14,16-21,29,32,33 sampled solely women with breast cancer. Another study with an all female sample incorporated 26 individuals with a diagnosis of breast cancer and one woman with a diagnosis of endometrial cancer. 22 A further study sampled only women but the type of cancer was not specified, although staging details were provided. 16 Not all authors reported comprehensively on their samples. Seven studies21-25,30,31 failed to report on ethnicity. Within the papers that reported on ethnicity, 69% of the cumulative total was white. Ten of the studies also omitted details relating to educational attainment.17-19,21,22,24,25,29,31,32 The majority of studies (n = 8) were conducted in the United States; the others were undertaken in Canada, 15 Iran, 16 Turkey, 19 Brazil,20,30,32 Germany, 21 Australia, 26 the United Kingdom, 27 and Korea. 31
Study Quality
Studies reviewed varied considerably with regard to their quality (Table 1). We used the Jadad score to appraise quality. This is used to indicate the methodological quality of clinical trials based on randomization, blinding, and withdrawals and dropouts reported in a study. High scores indicated higher quality papers with low risk of bias, while low scores indicated lower quality papers and high risk of bias. 13 The majority were rated as poor, registering scores of only 0 to 2 out of 5, indicating high risk of bias.15,16,18,19,23,25,28 Studies that were ascribed a low score typically did not allocate participants between study groups randomly, provided few or no details about the method of randomization employed, or provided limited evidence of appropriate blinding of participants or study personnel to group allocation.
High-quality studies were typically randomized and the randomization process well described. Furthermore, the study designs employed enabled allocation concealment and resulted in appropriate blinding of participants and study personnel. Additionally, they provided details of study attrition. Of the studies appraised in this review, only 6 attained a Jadad score of 4 or more.17,22,24,27,29,33
Timing of Interventions
The majority of studies (n = 12) recruited patients receiving treatment—either radiotherapy or chemotherapy.14,16-20,22,23,25,28,30,32 Others sampled patients that had completed treatment,15,21,27,29,31,33 while a small number of studies included mixed samples of patients comprising people both receiving and following cancer treatments.24,26
Consequently, interventions were introduced at different points in the disease and treatment pathways. This is an important consideration: an intervention introduced during chemotherapy may not lessen the symptom but could prevent its exacerbation. This may be as clinically significant as an intervention introduced following treatment that reduces fatigue.
Effectiveness of CAM Interventions for Relieving Cancer-Related Fatigue
To reflect the diversity in studies incorporated into the review regarding when CAM interventions were introduced, findings are presented within 3 groups: during treatment, following treatment, and mixed samples of patients on and following treatment. Effectiveness of interventions has been interpreted by assessing statistical significance of the intervention with study quality (as measured by the Jadad score) in order to take into account variability of change with the reliability of the study.
Effectiveness of CAM Interventions for Fatigue During Treatment
Twelve studies evaluated the effectiveness of CAM interventions in patients undergoing cancer therapy.14,16-20,22,23,25,28,30,32 Appraisal of their findings determined that hypnosis 14 and ginseng 17 were effective at generating greatest benefits for patients with regard to fatigue in comparison to the control group.
It appeared the hypnosis intervention evaluated by Montgomery et al 14 generated significantly lower levels of fatigue in the intervention group when compared with the control (standardized mean difference 29.47 vs 54.20; difference = 24.73; 95% confidence interval = 16.4-32.8) although it was impossible due to the results presented in the published paper to determine the difference in standardized pre–post test change between the intervention and control groups (Table 1). The study was of good quality indicating reliability of the findings.
Use of massage while during treatment produced mixed results. The studies of Swedish massage 23 and therapeutic massage 28 were of poor quality, but improvements in favor of the intervention group neared significance (P = .06, P = .057, respectively). The study by Aghabati et al 16 investigating therapeutic touch in patients receiving chemotherapy reported changes both within and between groups that were consistently statistically significant. However, as this paper was also of poor quality, and of high risk of bias, drawing conclusions about the effectiveness of these interventions within this context are problematic.
Studies investigating the effectiveness of vitamins and herbs were also of mixed quality and significance. Multivitamins 20 did not improve radiation induced fatigue; instead, patients experienced significantly lower rates of fatigue from a course of placebo. This study was deemed to be of good quality with low risk of bias. The study by Barton et al 17 of the effectiveness of ginseng was of high quality and low risk of bias. The benefits of ginseng use for decreasing fatigue looked promising, nearing significance (P = .08). A subset analysis did reveal a trend for higher doses exerting greater effects on fatigue. The use of guarana, 32 an indigenous Amazonian plant, in a low-quality trial, showed significant improvements in fatigue.
In the trial of yoga undertaken by Danhauer et al, 18 the intervention group reported significant within-group improvement in fatigue unlike the control group, which remained unchanged. However, the differences between groups did not attain statistical significance. This was a poor-quality study though, so these results should be viewed with caution.
The studies testing relaxation therapy in various forms were all of poor quality, making it difficult to draw conclusions about their true effectiveness but yielded statistically significant results. Relaxation therapy 25 as an adjunct during radiotherapy reduced fatigue (P < .01). It is interesting to note that while progressive muscle relaxation training 19 appeared to prevent statistically significant (P < .05) increases in fatigue that were observed in the control, it did not actually reduce fatigue; rather, it maintained its baseline level. 18 The combination treatment of relaxation with visualization followed by acupuncture 30 produced a significant decrease in fatigue (P ≤ .05). However, the quasi-experimental design, significant biases, and assessment of fatigue as a secondary outcome with a single item from the EORTC QLQ C30 scale places less confidence in the results.
Balk et al’s 22 feasibility study of acupuncture in people undergoing radiotherapy did not generate statistically significant improvements in fatigue when compared with the sham acupuncture control. However, this is unsurprising as the study was small (n = 27) and consequently underpowered. Despite this, the study was considered to be of good quality.
Effectiveness of CAM Interventions in Patients Following Cancer Treatments
Six studies explored effectiveness of 3 different CAM therapies for reducing fatigue following cancer treatments. The Reiki intervention tested by Tsang et al 15 showed no significant difference in scores between the Reiki and control groups. This was reflected in comparisons between the intervention and control groups’ total scores; the Reiki group reported an effect size of 0.62. This was a study of poor quality. However, although the biofield healing trial 33 appeared to show comparable decreases in general fatigue, there were notable differences in effect size between biofield healing and mock healing (1.04 for biofield healing vs 0.68 for mock healing). It was also evident that mock healing generated significantly greater decreases in mental and physical fatigue when compared with the control group, indicating that these changes were not only the result of a placebo effect, particularly as “belief” (a placebo variable) did not predict fatigue in the study. This was also a good-quality study, which indicates that the results can be viewed with confidence.
The study by Johnston et al, 29 while only a feasibility trial of 13 disease-free breast cancer patients, suggested that education about self-efficacy and self-management together with acupuncture was highly effective in reducing fatigue over a control arm of (undefined) usual care. Improvements in cognitive function were also observed. Despite its very small sample size (authors commented on recruitment difficulties), this was a well-designed trial with an intervention based on social cognitive and integrative medicine theories and merits further testing. Molassiotis et al 27 also evaluated the effectiveness of acupuncture and found it was significantly more effective at reducing fatigue (pre and post test changes) than acupressure and sham acupressure. Both were well-designed studies indicating that acupuncture may be a feasible intervention for treating fatigue posttreatment.
An improvement was also reported in the Bojungikki-tang herbal combination 31 (based on primary outcome analysis) while the control group remained unchanged. Significant improvements were also reported in all other fatigue secondary outcomes. As the study was of low quality, this outcome must be treated with caution.
Effectiveness of CAM Interventions in Heterogeneous Groups of Patients
Two studies24,26 recruited heterogeneous samples of patients that included people either receiving or having completed cancer therapies. Both these studies were of good quality. Although there were small pre–post test change scores in favor of Tibetan Yoga, the improvements in fatigue was not statistically significant. Medical Qigong 26 was effective for reducing fatigue (P < .001). These results are promising, especially as this is the first study of its kind using this intervention.
Duration of Effectiveness of CAM Postintervention
When appraising the effectiveness of interventions, it is important to consider not only their effectiveness but also to determine whether effects generated are sustained. Eleven of the studies in this review failed to incorporate a follow-up measure.14-20,23,25,26,28 Consequently, it is impossible to determine whether any reductions in fatigue, brought about by the interventions tested in these studies, were maintained.
When studies incorporated follow-up measures, there was considerable variation in their timing. The majority undertook final measurements less than 3 months following completion on the interventions.21,22,27
The study by Balk et al 22 reported that the improvement in fatigue associated with the acupuncture intervention provided during radiotherapy was maintained 4 weeks postintervention. However, these differences were not statistically significant. Whereas the effects of the Swedish massage intervention provided to women following cancer treatment were reportedly maintained (P = .048) 6 weeks following the intervention. 21 Whereas the one study that incorporated a longer follow-up (3 months) 24 failed to generate statistically significant improvements immediately following intervention delivery, and this remained the case at follow-up. The sample in this study was mixed with regard to being on or off treatment at commencement of the intervention.
Discussion
The findings from this systematic review of 20 trials are inconclusive. Some treatments appeared to show promise with regard to managing cancer-related fatigue following radiotherapy and chemotherapy yet appeared less effective at alleviating it during these treatments (eg, acupuncture). It is plausible that the physiological responses to chemotherapy and radiotherapy generating fatigue are too intense to be counteracted by the forms of CAM tested to date. However, the study evaluating acupuncture during treatment was small scale and aimed at testing feasibility. 22 Such design issues may also have prevented this intervention generating statistically significant improvements for people on treatment.
During treatment the interventions that seemed to be most effective for relieving cancer-related fatigue was hypnosis 14 while ginseng provided promising results. Massage,16,23,28 multivitamins, 20 herbs, 32 yoga, 18 relaxation therapy, and training (with acupuncture)19,25,30 were less effective. It was difficult to draw sound conclusions about the reliability of these CAM treatments due to the poor and varying quality of the studies.
Of the two29,30 studies using a combination of interventions (both including acupuncture), only the combination of education and acupuncture conferred benefit for patients. 29 Due to study quality issues, inferences cannot be made as to the effectiveness of the combination of acupuncture and relaxation/visualization. 30 It is unclear from this review whether multimodal interventions during cancer treatment are more appropriate for managing a complex symptom such as cancer-related fatigue than single interventions.
Several studies evaluated single CAM interventions following cancer treatments; acupuncture27,29 and biofield healing 33 appeared most effective at alleviating fatigue, although both acupuncture studies had small sample sizes. The study by Jain et al 33 resulted in similar improvements in both the biofield healing and the mock healing. When compared to the control group, those receiving mock healing experienced significantly greater decreases in mental and physical fatigue. This indicated that these changes were not the result of a placebo effect. The underlying processes of biofield healing on fatigue would therefore warrant further investigation. Large multicentered trials testing its effectiveness would be necessary to confirm these early results. Neither Reiki 15 nor Swedish massage 21 appeared to confer benefit to patients. These studies were small and exploratory in nature, and of limited quality.
With regard to studies evaluating CAM in heterogeneous samples of people who were either undergoing or had completed treatment, the most favorable results were associated with medical QiGong, 26 which appeared to increase energy in patients either having or having completed treatment. The trial by Oh et al 26 is the first to evaluate the effects of this CAM modality on cancer-related fatigue to date. The utility of this form of CAM for management of cancer-related fatigue could be further tested in a larger RCT. Restorative Yoga 18 appeared to enhance energy but the sample recruited to this study was small and findings at high risk of bias. Interestingly, a further and apparently higher quality study evaluating Tibetan yoga 24 was less successful in producing a similar reduction in cancer-related fatigue.
In general, the studies in the current review were compromised through their failure to consider the possibility of therapist effect, limited power, and usage of various forms of comparative control/placebo. There are many methodological challenges that need to be overcome when designing and conducting a CAM trial. Arguably, research designs should take into account that CAM practices are holistic in nature. It has been suggested that dissecting CAM practices can lead to invalid evaluations. 35
The review has some limitations and these should be recognized when considering the conclusions drawn. The Jadad score was used to appraise the quality of included trials as it is currently the standard approach to trial assessment. Furthermore, it is an easily understood method that incorporates the most important components of methodological quality. However, it places strong emphasis on blinding and consequently may result in a somewhat harsh score in relation to CAM trials where it is often impossible to blind the patient or provider to the treatment being delivered.
Furthermore, as the data reported by published trials prevented calculation of effect sizes, future trials should report on effect sizes and provide the reader an understanding regarding magnitude of change in fatigue that is clinically meaningful.
It is recognized that fatigue is affected by disease burden. 36 However, studies in this review did not control for this confounding effect. Future studies of CAM interventions should take stage of disease into account to ensure valid conclusions are drawn. Future trials would also benefit from reporting more consistently on the statistical and clinical significance of the CAM intervention by considering effect size of interventions, or by setting a defined minimum change score before initiation of trials to ensure that statistical results are considered relative to their clinical importance. Trials in this review largely failed to measure the economic impacts of the intervention. Only one study, by Montgomery et al, 14 estimated the impact of the tested hypnosis intervention on institutional costs (surgery related costs, sedative or analgesic costs in addition to costs of intervention delivery). Such direct and indirect costs should be measured in future trials of CAM for cancer-related fatigue.
As fatigue can be chronic in nature and can continue beyond treatment, 1 duration of effect size should also be determined. Furthermore, strong placebo effects can be associated with some CAM interventions as was the case in the multivitamin study by de Souza Fede et al, 20 whereby significantly lower rates of fatigue were observed in patients who had completed the course of placebo pills when compared with patients completing a course of multivitamins. Interestingly, a study evaluating the effects of relaxation 25 during cancer treatment did not appear to confer benefit to patients. In fact, “presence,” the control condition in this trial, generated a modest improvement in fatigue, unlike the intervention, which was associated with greater fatigue. This would suggest that the placebo effect 34 could significantly contribute to improvements generated by some forms of CAM. Consequently, researchers need to debate and carefully consider the suitability of attention controls for future trials of CAM. Determination of outcomes that persist following treatment would be prudent.
Sampling is an important consideration when reviewing the evidence presented in this review. Several trials reviewed had small sample sizes, half sampled solely women, and all appeared to include mostly white, well-educated subjects. Sample characteristics can bias results and limit generalizability of findings. Some studies14,17,23-28 recruited heterogeneous samples comprising participants with different cancer diagnoses, different disease stages, had variable time since diagnosis, and presence of comorbidities. Such variability can lead to difficulties in the interpretation of the significance of findings.
The presence of other corelated symptoms to fatigue (such as sleep disturbance or depression) may also compromise the effectiveness of an intervention and needs to be considered in some way within the trial design. Several trials used fatigue only as a secondary outcome, and future research should employ fatigue as the primary outcome, measured with well-validated, reliable, sensitive, and responsive scales. Recommendations for the measurement of fatigue do exist and should be used as a guide. 37
Quality assurance processes and measures to ensure intervention integrity are important in the conduct of trials. However, these were not described in the reviewed trials and this is another area for improvement in future work. Protocol integrity should be assessed and reported as should methods for both training and monitoring of therapists delivering the CAM intervention.
The “dose” of an intervention (techniques used, frequency of application, and length of course) is an important determinant of outcome. Among the studies incorporated in this review, the “dose” was often not well reported; frequently little rationale was offered to support that prescribed. Dose-finding studies (that determine the optimal techniques, scheduling, and length of course) are required and the “optimal” dose considered against adherence to protocol. Practicalities, including travel required for treatments, may significantly influence attendance/treatment. The most appropriate time to deliver an intervention may also need consideration. For example, it may be acceptable and beneficial for patients to be provided the CAM treatment when attending clinics for cancer treatment or follow-up. The case of herbal medications and their effects on fatigue is a promising area of further research work. In the pilot study by Barton et al, 17 no significant changes were found in fatigue; however, it was a dose-finding study, and it did identify a dose that may be associated with fatigue improvements. This dose was tested subsequently to a large sample of 364 patients and showed that the dose of 2000 mg of ginseng led to significant improvements in fatigue after 8 weeks of treatment, and the results of this trial were recently presented at a conference. 41 This is a good example of developing early-stage dose-finding studies before progressing to phase III trials. Furthermore, the guarana trial 32 also showed significant effect at a dose of 100 mg/day, while a similar trial in radiotherapy patients using 75 mg of guarana showed no significant effect, 42 demonstrating the importance of conducting dose-finding trials with any herbal/plant preparations.
Furthermore, the reporting of many of the reviewed trials was poor. It is recommended that researchers use established frameworks for reporting acupuncture 38 or other CAM trials (CONSORT statement).39,40 This is crucial for enhancing the quality of CAM trials. Unfortunately, most trials incorporated into this systematic review were methodologically weak and at high risk of bias; the majority were feasibility studies where blinding was not indicated or incorporated. However, it should be recognized that it is desirable to conduct a feasibility study before a large trial of a complementary therapy. The feasibility trial of acupuncture 27 was recently followed-up by a large, multisite pragmatic RCT, the first of its kind using this intervention. The study by Molassiotis et al 43 focused on the effectiveness of acupuncture in breast cancer patients. The findings from 302 women, posttreatment, were positive, indicating that acupuncture was both statistically and clinically significant for improving physical and mental fatigue as well as physical and functional quality of life.
In conclusion, currently there appears a limited role for complementary therapies to significantly contribute to improvements in the management of cancer-related fatigue. Evidence generated by trials to date is not sufficiently robust to support the use of any one of the apparently promising approaches over the others. Early preliminary findings identified in this review need replication through larger well-conducted multicentered trials. Complementary therapies could be delivered alongside other established effective interventions for fatigue (such as exercise or psychosocial programs). It is difficult to determine whether combinations of interventions might work together to achieve a greater effect than interventions used independently. This hypothesis could be tested in future trials of interventions for cancer-related fatigue.
While patients are often interested in the use of complementary therapies, currently many CAM therapies for the management of cancer-related fatigue do not have a strong level of evidence for their effectiveness. This limits their utilization outside the context of clinical trials. The results of this systematic review combined with indications of other potentially promising interventions reviewed by Sood et al 11 can constitute the future fatigue research “road map.” The future of complementary therapies for the management of fatigue may look tenuous, but increasing the strength of evidence should be a priority.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.