
Abstract
Objective
To determine if iodine-125 seed implantation improved the efficacy of transarterial chemoembolization (TACE) in patients with hepatocellular carcinoma (HCC) (≤5 cm).
Methods
We retrospectively reviewed the medical records of 83 consecutive patients with HCC (≤5 cm) who underwent TACE or TACE–iodine-125 from January 2014 to July 2017. The primary endpoint was progression-free survival (PFS). The secondary endpoints were overall survival (OS) and objective response rate (ORR) at 3 months after the first TACE treatment. PFS and OS were calculated using the Kaplan–Meier method and compared using log-rank tests. Independent risk factors for PFS and OS were analyzed using a Cox proportional hazards model.
Results
Thirty-five patients received TACE–iodine-125 and 48 received TACE alone. The median OS and PFS were both significantly longer in the TACE–iodine-125 compared with the TACE-alone group (42 vs 23 months and 16 vs 8 months, respectively). The ORR was significantly higher in the TACE–iodine-125 compared with the TACE-alone group. There was no significant difference in adverse events, apart from decreased white cell count, between the two groups.
Conclusion
TACE–iodine-125 might be an effective and safe alternative treatment for patients with HCC (≤5 cm).
Keywords
Introduction
Hepatocellular carcinoma (HCC) is a major cause of overall and cancer-related mortality worldwide. 1 Liver transplantation, hepatic resection, and ablation are recommended treatments for early-stage HCC, 2 while the Barcelona Clinic Liver Cancer (BCLC) system recommends transarterial chemoembolization (TACE) as the standard treatment for intermediate HCC (BCLC B).1,3 Some studies have reported that TACE combined with radiofrequency ablation (RFA) improves survival in patients with HCC;4,5 however, some patients might not be suitable for RFA because of the heat-sink effect or the specific location of the tumor, and there is thus a need to develop selective RFA treatments. TACE combined with locoregional treatment, such as radiotherapy, is a rapidly developing treatment option for patients with unresectable HCC.6–10
Iodine-125 is a radiotherapeutic agent used for the treatment of HCC. It is a synthetic radionuclide that radiates X-rays and γ-rays that damage the tumor DNA and cause the tissue to produce free radicals, which kill the tumor cells. 11 Iodine-125 is used to treat some solid tumors and has become the first-line treatment for patients with prostate cancer. 12 Previous studies 13 , 14 reported that treatment with iodine-125 seed implantation combined with liver resection or RFA increased survival in patients with HCC. However, information on the use of TACE combined with iodine-125 implantation (TACE–iodine-125) for HCC (≤5 cm) is lacking. This study aimed to determine if the addition of iodine-125 to TACE improved the efficacy of TACE in patients with HCC (≤5 cm).
Materials and methods
Study design and patient selection
Consecutive patients with HCC (≤5 cm) who underwent treatment with TACE or TACE–iodine-125 at Union Hospital, Tongji Medical College, China, were retrospectively reviewed. Approval for this retrospective study was obtained from the Tongji Medical College ethics committee, and informed consent was obtained from each patient.
Patients with HCC BCLC stage A were recommended to undergo resection or ablation as first-line treatment. They were informed of the possible complications and offered selective treatment with iodine-125 as an alternative. Some patients rejected resection because of the high risk, and some rejected RFA because of the perceived pain, despite local anesthesia. Some patients with tumors located near major vessels or organs were considered unsuitable for RFA. The inclusion criteria for the current study were: (1) patients diagnosed with HCC according to the European Association for the Study of the Liver guidelines; 1 (2) largest tumor diameter ≤5 cm; (3) no previous or postoperative treatment for HCC, such as liver resection, RFA, or percutaneous ethanol injection; (4) Child–Pugh class A or B; (5) Eastern Cooperative Oncology Group (ECOG) score of 0 or 1; (6) platelets >40 × 109/L; and (7) patients unwilling to receive liver transplantation, hepatic resection, or ablation for their own reasons. The exclusion criteria were: (1) patients unwilling to be included in the study; (2) patients who received prior radical treatment or TACE; (3) largest tumor diameter >5 cm; (4) poor liver function (Child–Pugh class C) and physical condition (ECOG 2); and (5) tumor rupture before being included in the study.
TACE
TACE was performed by two operators with ≥8 and 20 years of experience in performing TACE procedures using digital subtraction angiography (Artis zee floor; Siemens, Germany). The tip of a 5-Fr catheter (Cook, Bloomington, IN, USA) or 3-Fr microcatheter (Progreat; Terumo, Tokyo, Japan) was advanced into the tumor-feeding arteries. Lipiodol (Lipiodol Ultrafluido; Guerbet, France) 5 to 10 mL was mixed with 10 to 20 mg doxorubicin hydrochloride (Hisun Pharmaceutical Co. Ltd., Zhejiang, China) to create an emulsion in a 1:2 ratio and the mixed emulsion (5–10 mL) was injected into the tumor-feeding arteries through the catheter, depending on the liver function and the tumor size. Embolization with gelatin sponge particles (300–700 µm; Alicon, Hangzhou, Zhejiang, China) was then performed until stasis of arterial flow occurred.
Iodine-125 seed implantation
Iodine-125 seeds encapsulated in NiTinol capsules (China Institute of Atomic Energy, Beijing, China) (0.8-mm diameter, 4.5-mm length) were implanted 1 to 2 weeks after TACE. One week before implantation, the patients underwent a computed tomography (CT) scan. Patients with residual tumors were evaluated by a radiologist and the decision on whether to administer RFA or iodine-125 seed implantation was discussed by doctors. The CT images were then transmitted to the treatment-planning system (TPS). The TPS software simulates the cancer tissue puncture and the placement of iodine-125 seeds, then uses 3D-printing technology to create a 3D conformal template of the surface of the cancer tissue, and directs the puncture needle into the tissue based on the template. The numbers and positions of the iodine-125 seeds were determined by the TPS according to the minimum peripheral dose prescribed to each tumor (90–165 Gy), such that the X-rays and γ-rays could cover the planning target volume, including the tumor and 0.5 to 1 cm of the adjacent non-tumor tissues. Needle (18-gauge; XinKe Pharmaceutical Ltd., Shanghai, China) placement was performed under CT scan and the seeds were implanted into the tumor via the needle at intervals of 1 to 1.5 cm.
Assessment of clinical outcomes
All patients underwent follow-up until 30 June 2018. Patients were evaluated 1 month after the initial treatment, then every 3 months with laboratory and imaging examinations, including α-fetoprotein, contrast-enhanced CT, or contrast-enhanced magnetic resonance imaging. The tumor response was evaluated by one radiologist with 3 years of experience in radiology and by one interventional radiologist with 20 years of experience in interventional radiology. The primary endpoint was progression-free survival (PFS) and the secondary endpoints were overall survival (OS) and objective response rate (ORR) at 3 months after the first TACE treatment. PFS was defined as the time to tumor progression or death according to the modified Response Evaluation Criteria in Solid Tumors (mRECIST). 15 OS was defined the time from the first TACE procedure until the last follow-up or death. The ORR was defined as the percentage of patients with a complete or partial response.
Adverse events attributed to TACE or TACE–iodine-125 treatment, including fever, right upper quadrant pain, nausea and/or vomiting, and decreased white blood cell count, were observed and recorded after the procedure.
Statistical analysis
Data analysis was performed using SPSS Statistics for Windows, version 24.0 (IBM Corp., Armonk, NY, USA). Results were compared between the groups using an independent samples t-test, Wilcoxon’s signed-rank test, Pearson’s χ2 test, and Fisher’s exact test. PFS and OS were calculated using the Kaplan–Meier method. Univariate analysis was performed using the log-rank test. Variables with a P value <0.10 in univariate analysis were entered into multivariate analysis using a Cox proportional hazards model to identify risk factors affecting OS. All statistical tests were two-sided and a value of P ≤ 0.05 was considered statistically significant.
Results
Study population
Eighty-three patients were included in this analysis, of whom 35 underwent TACE–iodine-125 and 48 underwent TACE alone. The baseline characteristics of the patients are shown in Table 1. There was no significant difference in baseline characteristics between the two groups.
Baseline characteristics of the patients.

TACE, transarterial chemoembolization; HBV, hepatitis B virus; AFP, α-fetoprotein; BCLC, Barcelona Clinic Liver Cancer; ECOG, Eastern Cooperative Oncology Group.
Efficacies of TACE–iodine-125 and TACE alone
A median of 18 seeds (range, 7–65 particles) were implanted in each patient in the TACE–iodine-125 group (Figure 1). The median PFS rates in the TACE–iodine-125 group and TACE-alone groups were 16 months (95% confidence interval [CI]: 11.2, 20.8) and 8 months (95%CI: 4.2, 11.8), respectively (P < 0.001) (Figure 2a). During follow-up, 14 (40.0%) patients in the TACE–iodine-125 group and 28 (58.3%) patients in the TACE-alone group died. The median OS rates in the TACE–iodine-125 and TACE-alone groups were 42 months (95%CI: 34.3, 49.7) and 23 months (95%CI: 18.9, 27.1), respectively (P = 0.005) (Figure 2b). In a subgroup analysis of patients with HCC <3 cm, median PFS and median OS were both significantly longer in patients who received TACE–iodine-125 compared with those who received TACE alone (23 months [95%CI: 8.4, 37.6] vs 8 months [95%CI: 3, 13], P = 0.038, and 44 months [95%CI: 20.1, 67.9] vs 28 months [95%CI: 10.9, 45.1], P = 0.048) (Figure 3a, b). Similar results were found for patients with tumors of 3 to 5 cm (15 months [95%CI: 6.3, 23.7] vs 8 months [95%CI: 4.1, 11.9], P = 0.009, and 42 months [95%CI: 4.3, 79.7] vs 23 months [95%CI: 19.3, 26.7] P = 0.047) (Figure 3c, d). The ORR was significantly higher in the TACE–iodine-125 group (68.6% [24/35]) compared with the TACE-alone group (50% [24/48)] (P = 0.012).
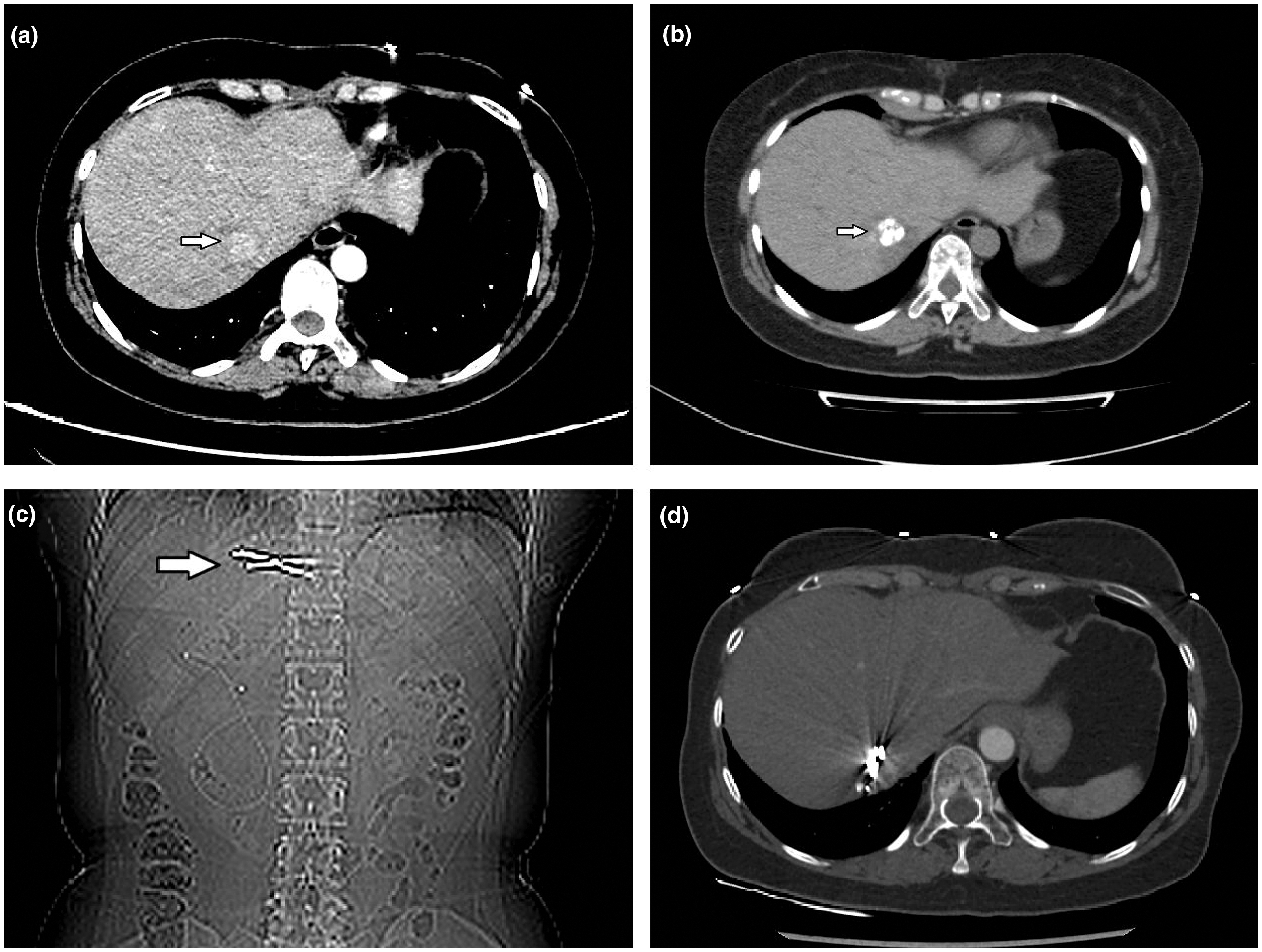
A 49-year-old female patient with one hepatocellular carcinoma nodule (2.6 cm) at the edge of the liver. (a) Contrast-enhanced computed tomography (CT) image before treatment (white arrow shows tumor). (b) CT image of lesion after transarterial chemoembolization. (c) Location of iodine-125 particles in the lesion. (d) Last reviewed image showing complete response.

Kaplan–Meier survival curves. Kaplan–Meier survival curves for (a) progression-free survival and (b) overall survival.
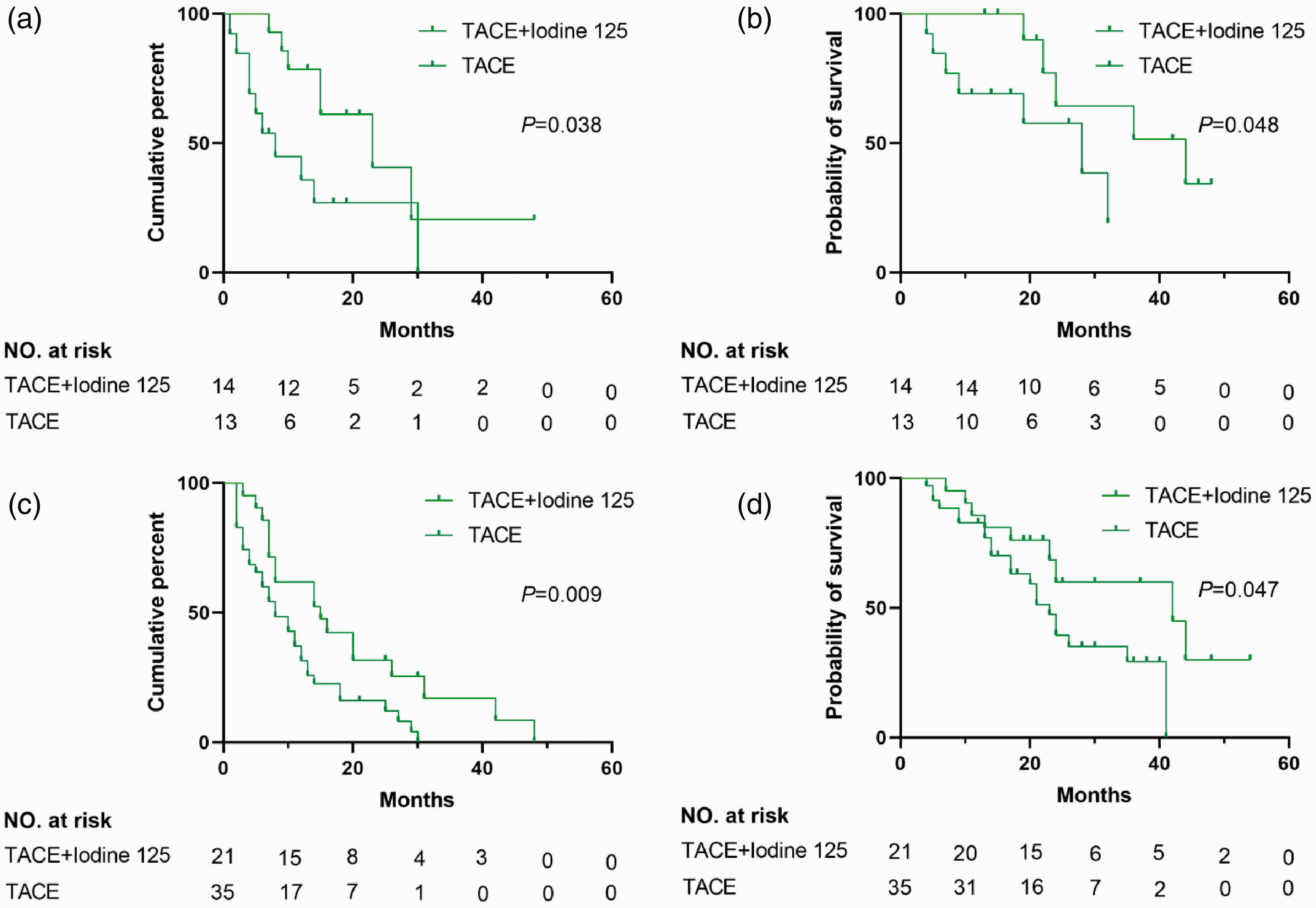
Kaplan–Meier survival curves according to tumor size. Kaplan–Meier survival curves for (a, b) progression-free (PFS) and overall survival (OS) in patients with tumors <3 cm, and (c, d) PFS and OS in patients with tumors of 3 to 5 cm.
Univariate analysis identified number of tumors (>1), BCLC stage B/C, and treatment with TACE–iodine-125 as factors significantly associated with PFS. Among these factors, multivariate analysis identified treatment method as an independent prognostic factor for PFS (Table 2). Univariate analysis found that Child–Pugh class B and treatment with TACE–iodine-125 were correlated with OS, and both were also identified as independent risk factors for OS by multivariate analysis (Table 3).
Univariate and multivariate analyses for progression-free survival.

HR, hazard ratio; CI, confidence interval; TACE, transarterial chemoembolization; HBV, hepatitis B virus; AFP, α-fetoprotein; ECOG, Eastern Cooperative Oncology Group; BCLC, Barcelona Clinic Liver Cancer.
Univariate and multivariate analyses for overall survival.

HR, hazard ratio; CI, confidence interval; TACE, transarterial chemoembolization; HBV, hepatitis B virus; AFP, α-fetoprotein; BCLC, Barcelona Clinic Liver Cancer.
Adverse events
Adverse events relating to TACE and TACE–iodine-125 treatment, including fever, right upper quadrant pain, nausea and/or vomiting, and decreased white blood cell count, were observed and recorded after the procedures (Table 4). The incidences of low-grade fever and nausea and/or vomiting were similar in both groups (P = 0.729 and P = 0.872, respectively). However, significantly more patients in the TACE–iodine-125 group had decreased white blood cells compared with the TACE-alone group (22.9% vs. 4.2%, P = 0.01). However, these symptoms were easily controlled by symptomatic therapies and usually subsided within 1 week.
Adverse events in patients treated with transarterial chemoembolization (TACE)-iodine-125 and TACE alone.

TACE, transarterial chemoembolization.
Discussion
Radiation therapy has been widely used for the treatment of tumors,16,17 and stereotactic ablative body radiosurgery, yttrium 90 radioembolization, and iodine-125 seed implantation have all shown encouraging results for the treatment of some solid tumors.12,18,19 Iodine-125 seed implantation has been used to treat HCC with encouraging efficacy. 20 The advantage of using iodine-125 seed implantation for tumor treatment is that it minimizes damage to the surrounding normal tissues because of their limited radiation distance. In the present study, we recruited patients with HCC (≤5 cm) to determine if the addition of iodine-125 could improve the efficacy of TACE in patients with HCC (≤5 cm).
Previous studies reported that TACE conferred significant survival benefits or reduced tumor growth in patients with HCC,21,22 with a notable effect on 2-year survival. 23 A meta-analysis 24 of nine studies reported significantly higher 1-year OS (odds ratio [OR]: 4.72, 95%CI: 2.63, 8.47, P < 0.001) and 2-year OS (OR: 4.72, 95%CI: 2.63, 8.47, P < 0.001) in patients treated with TACE–iodine-125 compared with TACE alone. The results of the current study similarly showed that patients with HCC (≤5 cm) treated with TACE–iodine-125 particle implantation had longer median PFS (16 months vs 8 months, P < 0.001) and OS (42 months vs 23 months, P = 0.005) than those treated with TACE alone. Cui et al. 25 enrolled 62 patients with HCC (2–8 cm), including 32 treated with RFA and 30 with RFA plus cellular immunotherapy. PFS in the RFA group was 12 months, which was shorter than in the current study. However, although their study included 38 patients with tumors <3 cm in diameter, they did not specifically compare the treatment efficacies in this subgroup. In contrast, the current study compared the efficacy of TACE combined with iodine 125 with TACE alone in patients with HCC <3 cm, and found better results with the combination treatment. Li et al. 26 reported that the median OS among patients with HCC (maximum diameter 3–5 cm) treated with TACE–iodine-125 was higher than that in the TACE-alone group (30 months vs 18 months, P < 0.001). The median OS of the combined treatment and TACE-alone groups in the current study were higher than in the previous study because the previous study recruited more BCLC C stage patients and the current study included more patients with HCC <3 cm. In this study, the ORR was significantly higher in the TACE–iodine-125 group (77.1%) compared with the TACE-alone group (50%) (P = 0.012). Zhou et al. 27 recruited 99 patients with HCC (mean largest diameter 4.3 cm) treated with TACE using drug-eluting CalliSpheres® beads, and showed an ORR and complete response of 75.8% and 16.2%, respectively. The ORR at 3 months after treatment was lower than in the current study, possibly because of patient heterogeneity. However, the results for local tumor response need to be confirmed with longer follow-up in future research. Multivariate analysis identified combined treatment as an independent factor affecting median PFS (P < 0.001) and OS (P = 0.003), suggesting that TACE combined with iodine-125 particle implantation was more effective for the treatment of HCC than TACE alone.
The most common adverse events of TACE–iodine-125 were fever and right upper quadrant pain. Although a decreased white blood cell count was significantly more common in the TACE–iodine-125 group compared with the TACE-alone group, the incidences of other adverse events were similar in both groups. All patients with decreased white blood cell counts in the current study recovered after the corresponding treatment, indicating that iodine-125 was a safe treatment for HCC.
This study showed encouraging results, but there were several limitations. First, this was a retrospective study and might therefore have had inherent selection bias. Second, the data came from a single center, and an adequately powered, prospective, randomized trial of TACE–iodine-125 in patients with HCC (≤5 cm) is necessary to confirm our findings.
In summary, TACE–iodine-125 might be an effective and safe alternative treatment method for patients with HCC (≤5 cm) who are unwilling to receive or who are unsuitable for TACE-RFA or surgical treatment.
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China [grant no. 81873919].